
Abstract
Objective
Minimally invasive mitral valve repair has been increasingly adopted. Right minithoracotomy (RT) and lower hemisternotomy (HS) have each been associated with improved short-term outcomes; however, these approaches have not been directly compared to each other. The aim of this study was to compare long-term survival and durability of 2 minimally invasive approaches to mitral repair.
Methods
We retrospectively identified all isolated mitral repairs performed via RT or HS between October 1997 and June 2018; 100 RT cases and 719 HS cases were included. Outcomes of interest were postoperative complications, long-term survival, and freedom from mitral reoperation. A Cox proportional hazard model was used to compare RT and HS to a reference cohort of full-sternotomy cases. Total observation time was 9,901 patient-years and mean follow-up time was 12.2 years.
Results
Mean age was 58±12 years in the RT group and 56±13 years in the HS group (P = 0.2). The RT group had longer bypass (143 minutes vs. 112 minutes; P < 0.001) and cross-clamp times (99 minutes vs. 78 minutes; P < 0.001) compared with the HS group. There were no differences in operative mortality or 30-day outcomes. Survival at 5, 10, and 15 years was 99% (96-100), 92% (85-100), and 69% (30-100) in the RT group and 98% (97-99), 92% (90-94), and 89% (86-92) for HS (P < 0.9). There were no differences in risk-adjusted survival between RT, HS and full sternotomy. No long-term mitral reoperations occurred in the RT group and 8 (1%) occurred in the HS group (P < 0.50).
Conclusions
Minimally invasive mitral valve repair can be performed safely through RT or HS with excellent survival and durability at 15 years.
Central Message
Minimally invasive mitral valve repair can be performed via right minithoracotomy and lower hemisternotomy with excellent and comparable long-term survival and durability. Surgeon experience and patient-specific factors should be taken into consideration when choosing minimally invasive approaches to the mitral valve.
Introduction
Minimally invasive (MIS) approaches to the mitral valve have been increasingly adopted over the past 2 decades. 1 The primary goal of MIS mitral surgery is to perform a procedure that is technically equivalent to what can be delivered through full sternotomy, while avoiding pitfalls inherent to the traditional incision. 2,3 Several studies have highlighted benefits of MIS mitral surgery compared with full sternotomy in terms of pain, reduced transfusion, improved cosmesis and shorter hospital stay in select patients. 4 -9 Furthermore, long-term studies have shown excellent survival and durability. 10,11
Various MIS approaches to the mitral valve have been described, including parasternal incision, hemisternotomy (HS), robotic surgery, and right minithoracotomy (RT), which has become the preferred method in most centers. 12 -14 When studying MIS mitral surgery, comparisons are generally made to full sternotomy, and MIS approaches have not previously been compared directly to each other. 15 -18 In the absence of direct head-to-head data, the choice of MIS approach is, therefore, based primarily on surgeon preference. The purpose of this study was to compare short-term outcomes, as well as long-term survival and durability in patients undergoing MIS mitral valve repair via RT versus lower-HS approaches.
Methods
Patient Selection
This retrospective, observational review identified all adult patients who underwent MIS mitral valve repair between October 1, 1997 and June 1, 2018 at a single institution. Mitral valve replacement and concomitant procedures, other than atrial fibrillation-related procedures, were excluded to reduce confounding due to case complexity or patient risk. This research was approved by our institutional review board with waived patient consent.
Data Sources and Variables of Interest
Patient demographics, laboratory values, operative details, and in-hospital outcomes were obtained from the patients’ electronic medical records (EMR). Data on long-term outcomes were collected through routine patient or clinic follow-up, our internal research data repository, or by query of our institution’s Healthcare Research Patient Data Repository, which can access EMR for all patients seen at our institution since 1989, as well as National Death Index data. 19 Additional follow-up data were obtained from our state’s Registry of Vital Statistics and search of publicly available obituaries. There was 99% follow-up for patient survival. Follow-up time was calculated in months from the date of surgery to either date of death or December 2018. For patients lost to follow-up, observation time was censored at the point of last known clinical contact. All variables collected were coded according to STS Adult Cardiac Surgery Database version 2.52 specifications unless otherwise noted. Operative mortality included any death occurring in-house or within 30 days of surgery, if discharged alive. In cases of missing echocardiographic data, the severity of disease is reported as “Unknown.”
The main outcomes of interest were survival and freedom from mitral reoperation. Secondary outcomes included postoperative length of stay, return to the operating room, permanent stroke, rate of new-onset atrial fibrillation, and renal failure. For comparative purposes on long-term survival, a reference cohort (N = 851) was selected from the pool of contemporaneous patients who underwent full-sternotomy isolated mitral valve repair with similar demographic characteristics.
Surgical Techniques
MIS mitral valve repair was performed through RT or lower HS (Fig. 1). 20 Our institutional techniques have been described in detail previously. 10 Briefly, lower HS is carried out through a 6-cm skin incision with sternotomy extending from the xyphoid process into the right second intercostal space. Central aortic cannulation is generally performed with venous drainage accomplished through the femoral vein under transesophageal echo guidance.
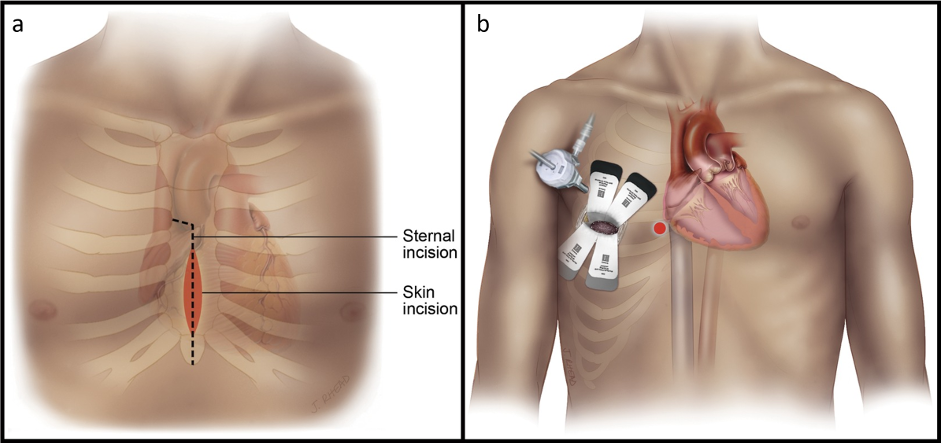
(a) Standard hemisternotomy, and (b) right minithoracotomy incisions for minimally invasive mitral valve surgery. Images from Wolfe et al. 2016,20 distributed as open access under a CCBY-NC-ND license with no permission to reproduce required.
RT is carried out through the fourth intercostal space either just below the nipple or within the inframammary crease. Cardiopulmonary bypass (CPB) is initiated through the femoral artery and vein. Percutaneous venous drainage of the superior vena cava is also used to assist drainage in select cases. There were no major differences in de-airing techniques between the RT or lower-HS procedures.
In both approaches the mitral valve is accessed primarily through the interatrial groove and antegrade cardioplegia is delivered through the ascending aorta in the standard fashion, unless contraindicated.
Statistical Analysis
Continuous variables are expressed as a mean and SD and were compared using Student’s t-test with Levene’s test for homogeneity of variance or as median and interquartile range (IQR) and were evaluated using Mann–Whitney U tests, as appropriate to their distribution. Categorical variables are presented as number and percentages and were compared using Fisher’s exact tests. Time-to-events were estimated using Kaplan–Meier analysis. Adjusted survival was evaluated by a forward-stepwise Cox proportional hazards model with inverse probability weighting for the probability of undergoing full sternotomy. Variables chosen for entry into the model included those significantly associated with mortality on exploratory univariable analysis, variables known to be confounders or predictors of the outcomes of interest and those deemed clinically meaningful. Continuous variables included age (years) and preoperative creatinine. Categorical values included gender, indication for procedure, chronic kidney disease, peripheral vascular disease, cerebrovascular disease, congestive heart failure, and reoperative status. All analyses were conducted using IBM SPSS Statistics version 23.0 (IBM Corporation, Armonk, NY, USA) with P < 0.05 as the criterion for significance.
Results
Overall, 819 patients undergoing MIS mitral valve repair met study criteria. RT approach was performed in 100 patients and 719 underwent lower HS. Baseline demographics are presented in Table 1. Mean age was 58 ± 12 years in the RT group and 56 ± 13 years in the HS group (P = 0.2). There was an increased rate of congestive heart failure in the RT group compared with HS (40% vs. 19%, P < 0.001); however, this difference in clinical diagnosis was not reflected in baseline ejection fraction measured echocardiographically. There were no significant differences in other baseline characteristics, degree of mitral regurgitation, or Society of Thoracic Surgeons–predicted mortality score. Furthermore, there were no significant differences in the etiology of mitral disease.
Preoperative Characteristics of Patients Undergoing Minimally Invasive Mitral Valve Repair via RT and HS Approaches.
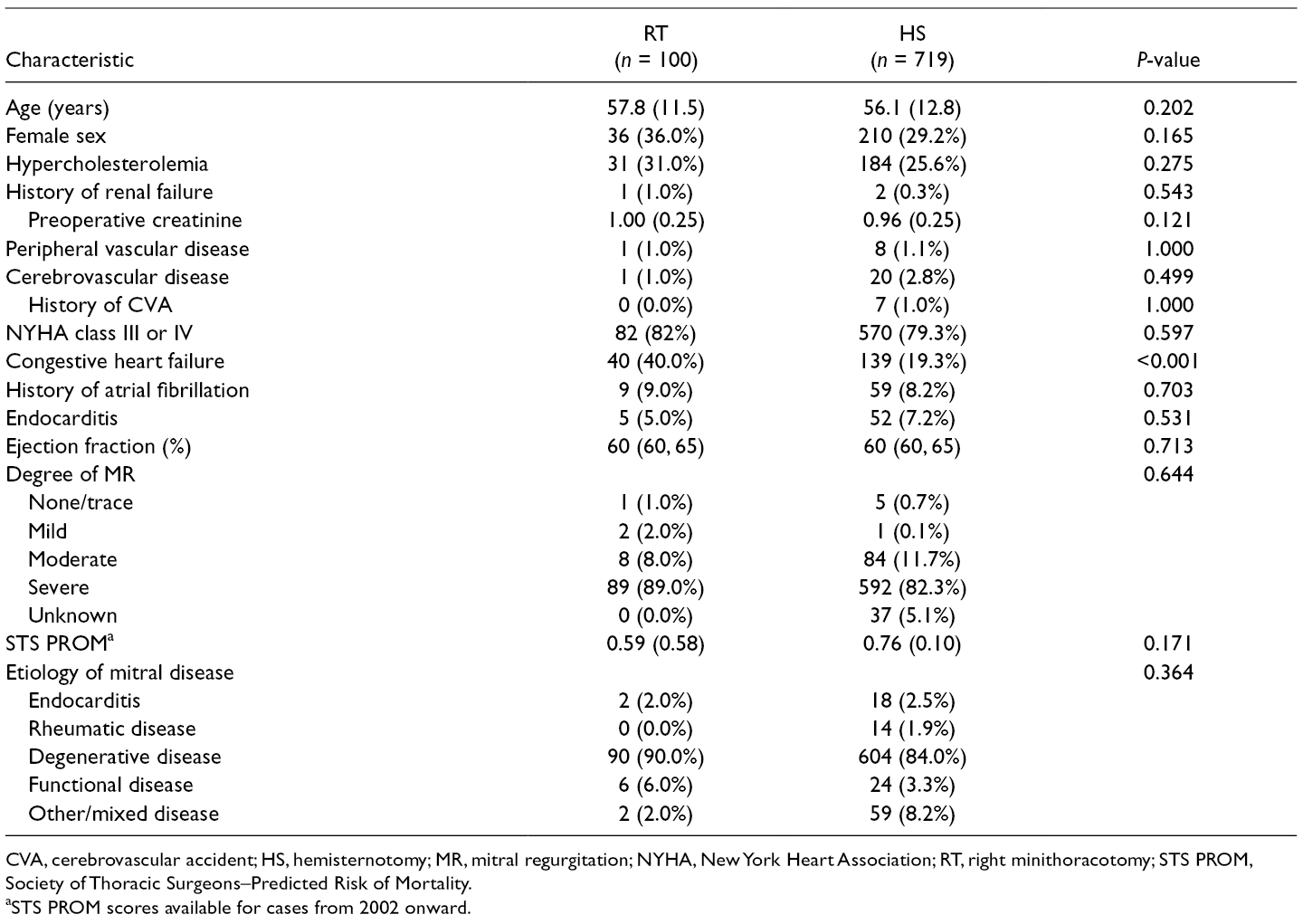
CVA, cerebrovascular accident; HS, hemisternotomy; MR, mitral regurgitation; NYHA, New York Heart Association; RT, right minithoracotomy; STS PROM, Society of Thoracic Surgeons–Predicted Risk of Mortality.
aSTS PROM scores available for cases from 2002 onward.
Both CPB (143 minutes vs. 112 minutes) and aortic cross-clamp times (99 minutes vs. 78 minutes) were longer in the RT group compared with the HS group (P < 0.001 for both), as shown in Table 2. Data on cannulation site were available in 67 RT patients and 475 HS patients. In this group, femoral arterial cannulation with retrograde perfusion was used in 61 (91%) of RT patients and 19 (4.0%) of HS patients. One patient in the HS group had right axillary cannulation, otherwise all were cannulated centrally. The use of annuloplasty ring in mitral repair was reviewed in a subset of cases. Annuloplasty ring was implanted in 97%, 98%, and 98% of RT, HS, and full-sternotomy cases, respectively.
Operative Characteristics of Patients Undergoing Minimally Invasive Mitral Valve Repair via RT and HS Approaches.
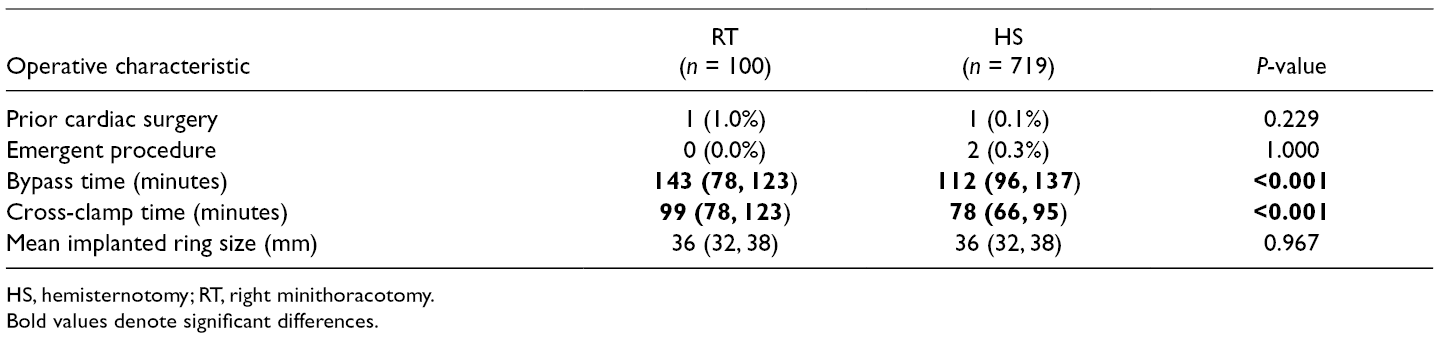
HS, hemisternotomy; RT, right minithoracotomy.
Bold values denote significant differences.
Retrograde cardioplegia was not used in any of the RT cases but was used in 12 (1.6%) HS cases. A lidocaine containing “modified Del Nido” cardioplegia solution was used in 6 (6.0%) of RT cases and 1 (0.1%) HS case. 21 All other cases were performed with intermittent whole-blood cardioplegia.
Hospital Outcomes
In-hospital and 30-day outcomes are presented in Table 3. There were no cases of 30-day mortality in the RT group and 5 (0.7%) in the HS group (P = 1.000). Postoperative intensive care unit stay (29 hours vs. 28 hours, P = 0.855) and hospital stay (5 days vs. 5 days, P = 0.370) were also similar between RT and HS groups, respectively. There were no significant differences in rates of other important short-term outcomes including stroke, new-onset atrial fibrillation, reoperation, or hospital readmission.
Short-Term Postoperative Outcomes of Patients Undergoing Minimally Invasive Mitral Valve Repair via RT and HS Approaches.
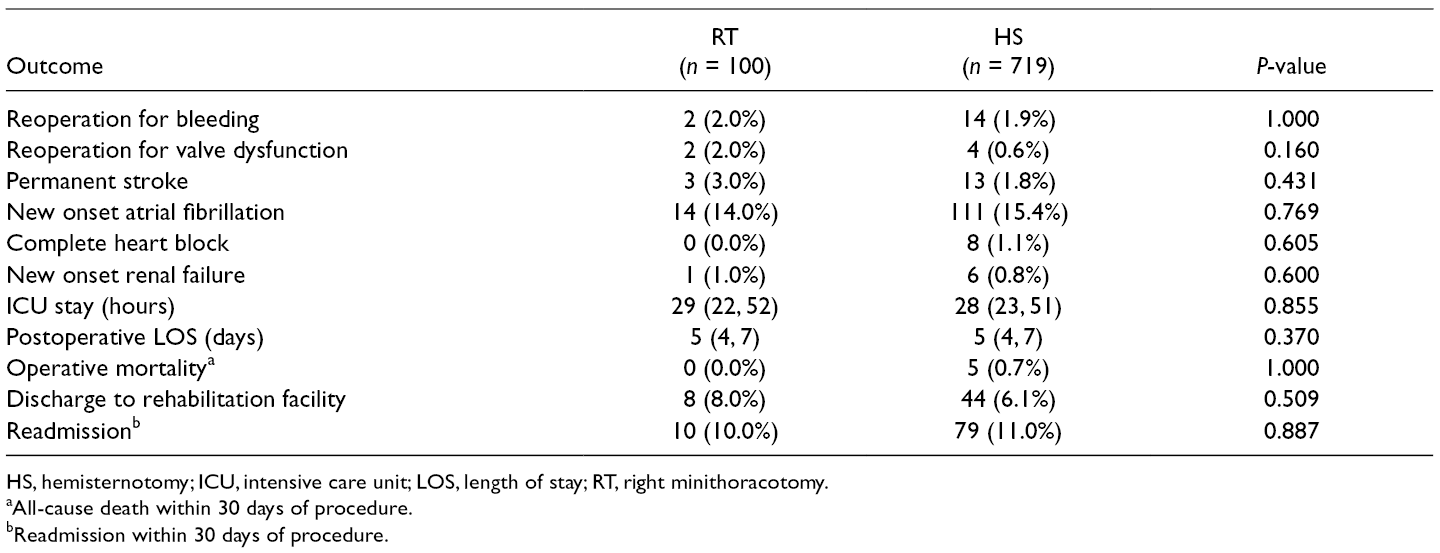
HS, hemisternotomy; ICU, intensive care unit; LOS, length of stay; RT, right minithoracotomy.
aAll-cause death within 30 days of procedure.
bReadmission within 30 days of procedure.
Long-Term Survival
The median observation time was 12.2 years [IQR 8.2 to 15.8] for a total of 9,901 patient-years, with 2 patients (0.2%) lost to follow-up. Long-term survival curves are shown in Fig. 2. Unadjusted survival at 5, 10, and 15 years was 99% (96, 100), 92% (85, 100), and 69% (30, 100) in the RT group and 98% (97, 99), 92% (90, 94), and 89% (86, 92) in the HS group (P < 0.9).
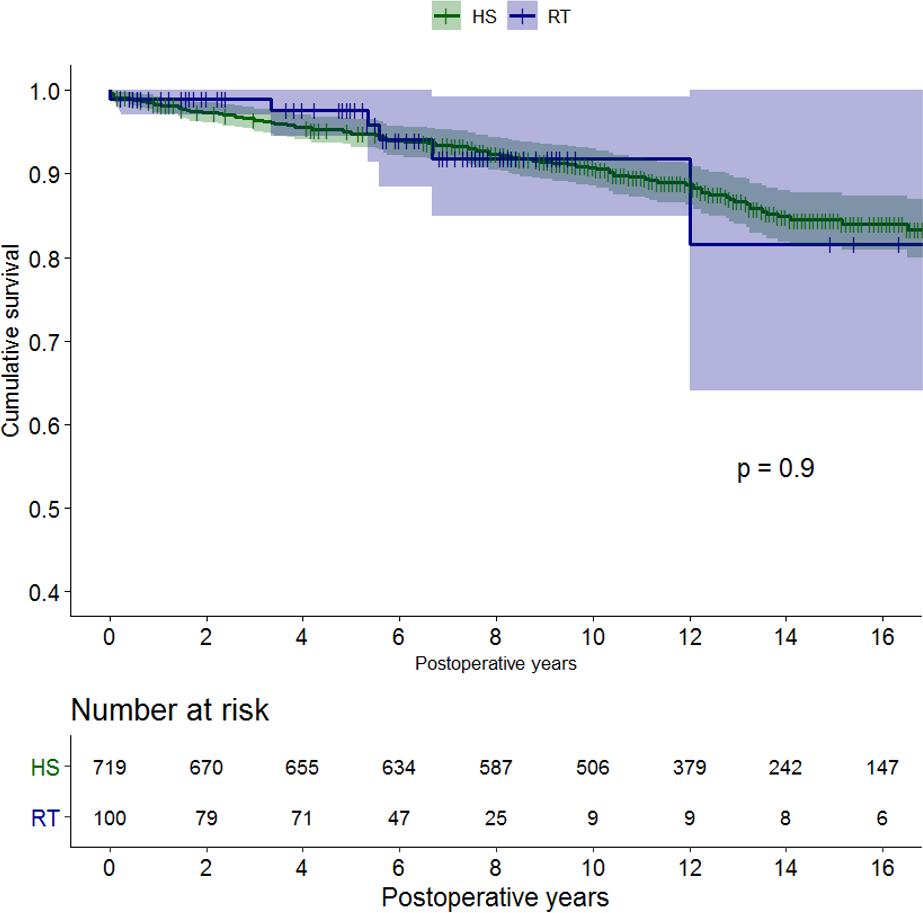
Kaplan–Meier curve showing long-term cumulative survival following minimally invasive mitral valve repair via right minithoracotomy (RT) and lower hemisternotomy (HS).
On Cox-adjusted survival analysis there was no significant difference in long-term survival between RT, HS, and a comparable group of full-sternotomy patients, matched using inverse probability weighting (Fig. 3).
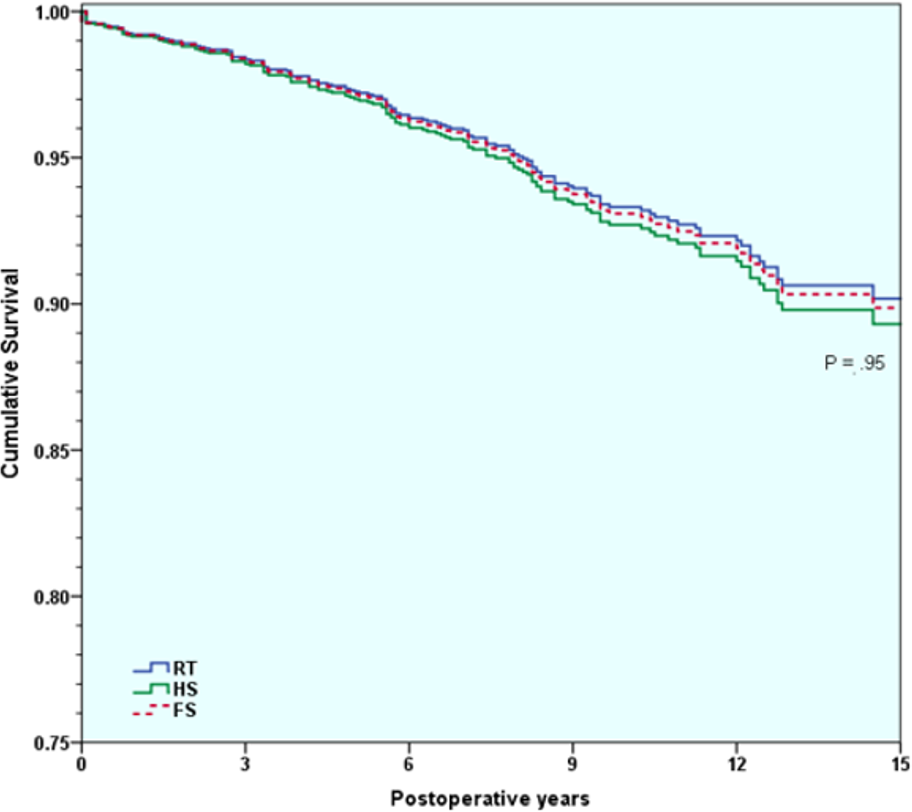
Cox proportional hazards model-adjusted survival following minimally invasive mitral valve repair via right minithoracotomy (RT) and lower hemisternotomy (HS). A full-sternotomy (FS) cohort, matched by inverse probability weighting, is included for reference.
Freedom From Mitral Reoperation
Kaplan–Meier freedom from long-term mitral reoperation curves are presented in Fig. 4. Over the entire 15-year period, there were no mitral reoperations required in the RT group and 8 (1%) in the HS group. This difference did not reach statistical significance, with P < 0.50. Operative details of cases requiring mitral reoperation are presented in Supplemental Table 1.
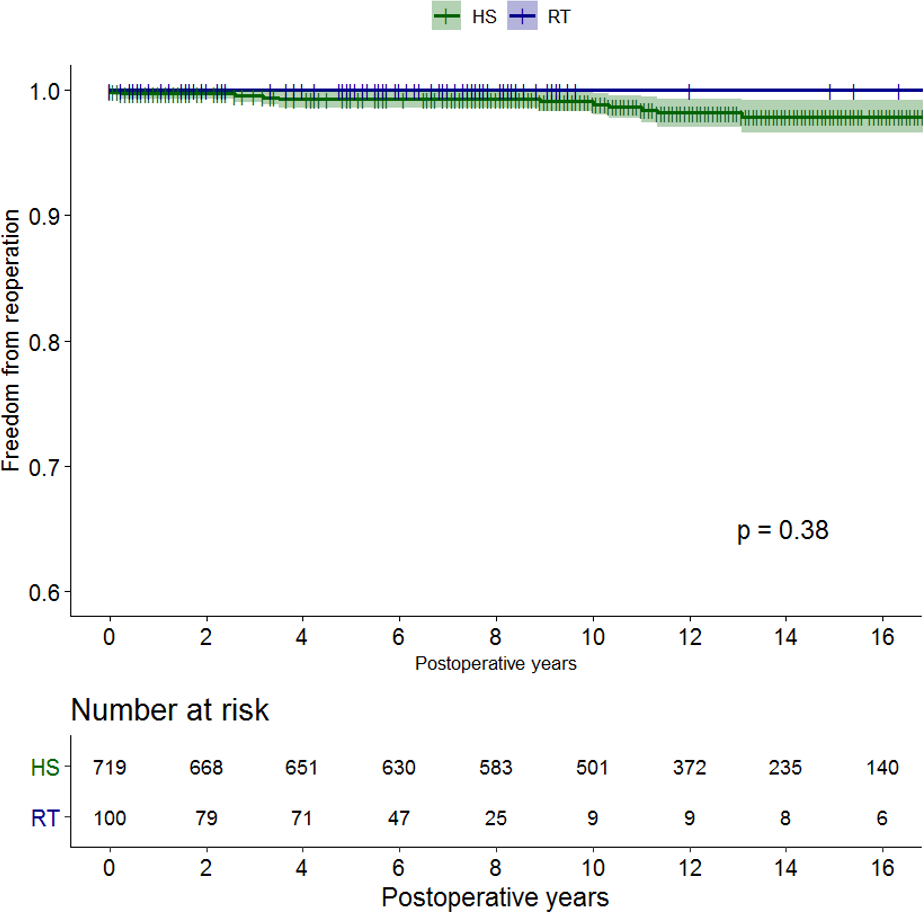
Kaplan–Meier curve showing long-term freedom from reoperation following minimally invasive mitral valve repair via right minithoracotomy (RT) and lower hemisternotomy (HS).
Discussion
The primary goal of any minimally invasive technique is to deliver a safe and durable operation while avoiding the morbidity associated with a traditional full sternotomy. MIS approaches to the mitral valve have achieved this goal, having previously shown reduced pain and postoperative stay, among other patient-centered outcomes. 4 -9 While RT has become the most widely used approach, a comparison of its safety and durability in relation to other MIS techniques has not been previously performed. In this single-center analysis, we have shown similar short-term outcomes, as well as long-term survival and durability of mitral valve repairs performed through RT and HS. Furthermore, following a risk-adjusted analysis we found 15-year survival to be similar in both groups and not significantly different from a reference full-sternotomy cohort.
The only significant differences between the RT and HS groups were longer total CPB time and aortic cross-clamp times in the thoracotomy arm. This is perhaps unsurprising, given that surgical techniques involved in the HS procedure more closely mirror those of a traditional full sternotomy. Several publications have noted longer operative times for RT in comparison to full sternotomy. 16 -18 A well-described learning curve exists within the RT literature and this may be another contributing factor, given that our center has more experience with the HS approach. 22 Nonetheless, these differences in operative time did not translate into worse long-term survival or rates of reoperation. These results indicate that excellent long-term outcomes can be attained through both minimally invasive methods. Surgeon preference and experience, provided suitable patient-level features, should remain the most important factor in determining MIS approach.
In recent years we have seen the emergence of several novel approaches to less-invasive mitral repair, including technologies for off-pump transapical chordal replacement. 23,24 Furthermore, there has been significant investment from industry examining new transcatheter options for degenerative mitral valve repair. 25 This is a dynamic and promising space with the potential to further decrease surgical trauma. Our results, in the context of the larger MIS mitral repair literature, should serve as a benchmark for development of these technologies.
There have been concerns regarding the neurologic consequences of retrograde systemic perfusion, given previous reports of increased stroke rates following the RT approach. 26,27 In particular, advanced age and increased atherosclerotic burden have been associated with significantly increased odds of neurologic complications in these patients. 28 We do not have adequate power in the current study to comment on specific risk factors for peripheral cannulation. Nonetheless, we found no significant difference in the rate of permanent stroke between the RT group, perfused primarily (91%) with a retrograde technique, and the HS group, who underwent standard central aortic cannulation in over 95% of cases.
Our results are reassuring in the context of long-term traditional hard endpoints. Long-term survival and freedom from valve-specific reoperation are extremely important metrics in judging the safety and reliability of any procedural advance. To measure the true value of MIS cardiac surgery, however, more patient-centered outcomes such as pain, satisfaction, return to work, and function must be evaluated. While an assessment of these patient-reported outcomes was beyond the scope of the present study, we believe that outcome measures such as pain and return to normal activity will have increasing value and should be pursued in future MIS research. 29
This research is subject to the inherent limitations of a single-center, retrospective study design. Given that the choice of approach was primarily a surgeon-specific decision, it was not possible to fully eliminate patient selection bias. Although we did not find any differences in outcomes between operating surgeons, our small numbers limited a more thorough analysis of this point. Apart from the traditional risk factors included in our model, it was also not possible to control for specific anatomic or physiologic factors that would influence choice of approach. While Cox-adjusted analysis was used to control for differences between groups, the relatively small number of patients in the RT group did limit the use of more sophisticated matching techniques. We were also unable to identify cases of conversion from RT or HS to full sternotomy, or from mitral repair to replacement; thus, our population represents an “as-treated” analysis. Furthermore, given limitations of our database for the earliest portion of this series, we are unable to report on specific repair techniques, atrial fibrillation lesion sets, or other postoperative complications. These issues limit the generalizability of our research and our findings should be interpreted in this context.
Conclusions
MIS mitral valve repair performed through RT or HS yields excellent long-term results. In this experience, no significant differences in 15-year survival or durability were found between RT or HS approaches. Following risk-adjusted analysis, survival was similar to that of a comparable reference full-sternotomy group. Surgeons should continue to offer MIS approaches based on expertise, training, and patient-level factors. Further research is needed to establish comparisons of MIS approaches with respect to patient-centered outcomes.
Supplemental Material
Supplementary material - Supplemental material for Long-Term Outcomes of Right Minithoracotomy Versus Hemisternotomy for Mitral Valve Repair
Supplemental material, Supplementary material, for Long-Term Outcomes of Right Minithoracotomy Versus Hemisternotomy for Mitral Valve Repair by Edward Percy, Sameer A. Hirji, Farhang Yazdchi, Siobhan McGurk, Spencer Kiehm, Richard Cook, Tsuyoshi Kaneko, Prem Shekar and Marc P. Pelletier in Innovations: Technology and Techniques in Cardiothoracic and Vascular Surgery
Footnotes
*
Presented at the 2019 International Society for Minimally Invasive Cardiothoracic Surgery Annual Scientific Meeting, New York, NY, May 29th-June 1st, 2019.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Percy received funding from the University of British Columbia Clinician Investigator Program.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.