
Abstract

Introduction
Coronavirus disease 2019 (COVID-19) is a pandemic that has affected more than 5,400,000 people in over 180 countries worldwide with more than 40,000 reported deaths. 1,2 Typical presentation of severe forms of COVID-19 is bilateral pneumonia and, in some patients, an acute hypoxemic respiratory failure that can represent a significant therapeutic challenge for physicians. 3 -8 In these severe patients with profound hypoxemia and a near-normal respiratory system compliance, at least in the very early phase, 9 different clinical scenarios can be observed, ranging from normal breathing (i.e., “silent” hypoxemia) to bilateral patchy ground-glass opacities requiring oxygen supply. Gattinoni et al. suggested that the different COVID-19 patterns are related to the interaction of many factors, including the viral load, the host response, the physiological reserve and existing comorbidities, time between the onset of the disease and the presentation to the hospital, as well as provided therapies. 10 Whether the interactions between these factors can really result in 2 different phenotypes of respiratory failure (i.e., the “L type,” characterized by low elastance, low ventilation-to-perfusion ratio, and low recruitability and the “H type,” characterized by high elastance, high right-to-left shunt, and high recruitability) remains to be demonstrated. 11,12 Nevertheless, in some patients, the use of mechanical ventilation, even if adjusted on patient’s phenotype, fails to provide an adequate systemic oxygenation and rescue therapies might be needed.
Role of Extracorporeal Membrane Oxygenation in COVID-19
Although it remains unclear which factors determine the progression of COVID-19-related acute respiratory failure to refractory hypoxemia to the “lung-protective” strategies (i.e., severity of the disease itself; negative intrathoracic pressure during spontaneous breathing; interstitial lung edema secondary to the increased lung permeability due to inflammation; loss of lung perfusion regulation due to the microvascular thrombosis; hypoxic vasoconstriction), the institution of extracorporeal membrane oxygenation (ECMO) can be a valuable strategy to avoid lung damages caused by aggressive mechanical ventilation (i.e., ventilator-induced lung injury) or inappropriate triggering (i.e., patient self-induced lung injury) and to promote pulmonary healing. Indeed, during the ECMO run, ventilatory settings may include the lowest positive end-expiratory pressure, the lowest tidal volume to reduce plateau airway and driving pressures, and the lowest respiratory rate, all reducing the mechanical power. 13
The initial reports on the use of ECMO in COVID-19 patients has been associated with very limited cohorts and poor outcomes. 14,15 Despite this discouraging start, the extracorporeal support in COVID-19 respiratory failure had shown a worldwide spread. 16 -18 In particular, the Extracorporeal Life Support Organization (ELSO, Ann Arbor, MI, USA) 19 and the American Society for Artificial Internal Organs (Beverly, MA, USA) 20 recently published guidelines about the role of ECMO in this specific patient population. Also, the World Health Organization interim guidelines for the management of severe COVID-19 and the Surviving Sepsis Campaign guidelines both suggested the use of venovenous (V-V) ECMO in patients with persisting hypoxemia despite conventional treatments. 21,22 Nevertheless, no large report on the effectiveness of such strategy has been reported so far, and indication, optimal management, and potential complications of ECMO therapy in COVID-19 patients are actually poorly defined. Moreover, when compared to the previous outbreaks of emerging viral disease such as H1N1, 23 Severe Acute Respiratory Syndrome (SARS), and Middle East Respiratory Syndrome (MERS) coronavirus related to Acute Respiratory Distress Syndrome (ARDS), 24 COVID-19 has been associated with an increased incidence of cardiovascular complications, such as “acute cardiac injury” (i.e., increased troponin values) and/or pulmonary embolism.
ECMO and Inflammatory Burden in COVID-19
As it is well known, COVID-19 is also characterized by a hyperinflammatory state with an increase of markers of inflammation like interleukin 6 and ferritin directly linked with high mortality. The underlying pathophysiology of this inflammatory disease could be strictly related with an endothelial injury and dysfunction that induce a vascular barrier breach with consequent tissue edema, activation of coagulation pathways, and consequent thrombosis that deregulated inflammatory cell infiltration (severe endothelial distress syndrome). At the same time, ECMO per se, with its large and continuous surface, causes a systemic activation of coagulation and inflammation pathways by the increasing shear stress and the interactions between the foreign material and blood components. 25 The interplay between ECMO and COVID-19 inflammatory state is an unbalance from procoagulant/hypercoagulant state and anticoagulant conditions related to the necessary administration of unfractioned heparin required for the ECMO run. 26
While several authors have reported a relevant reduction in mortality with higher dosage of heparin in COVID-19, it is too early to gather definitive conclusions, and extreme attention to the coagulation profile during ECMO should be instituted in this particular clinical condition.
Infection triggers a complex host response and the inflammatory activation may lead also to a hyperpermeability of vasculature, which can ultimately induce vasoplegic shock.
In this scenario, the administered fluid is rapidly redistributed into the extravascular compartment leading to only transient improvement in hemodynamic parameters such as cardiac output and increasing adverse consequences in patients with already diminished respiratory reserve due to pulmonary infiltrates.
A restricted or “preventing” overload strategy might be advantageous, or the earlier application of renal replacement therapy (RRT), especially in those patients with more severe volume overload, progressive alkalosis, suboptimal diuretic response or diuretic refractoriness, and development of acute kidney injury, might be considered for optimization of volume status.
In the most severe form of COVID-19, a cytokine storm could be present and hemoadsorption therapy may be used to decrease cytokine levels and to control the pro-inflammatory response by the maintenance of the vascular barrier function. 27
Hemoadsorption or RRT could be used alone or in combination with extracorporeal circuit, and even if there is no recommendation for clinical use in the actual guidelines for management of sepsis and septic shock, it could represent a promising approach.
The multifaced presentation of COVID-19 poses a challenge not only in the indications of ECMO but also in its management.
Cardiovascular Complications in COVID-19
Up to one-third of COVID-19 patients who are admitted to the intensive care unit will develop cardiogenic shock, acute cardiac injury, arrhythmias, and/or acute cardiomyopathy. The mechanisms of these cardiac complications remain poorly understood in clinical practice and these phenomena are probably multifactorial. Some authors suggested an acute myocarditis (i.e., viral invasion of myocardial cells), in particular for young patients, while others a form of stress cardiomyopathy (i.e., cytokine-mediated with microvascular dysfunction). 28 Another important cause of cardiogenic shock could be acute pulmonary embolism with acute right ventricular (RV) failure, which could result either in low cardiac output or sudden death. 29 All of these conditions are enhanced by preexisting cardiovascular diseases. 30
In these cases, the benefits of V-V ECMO to confer lung protection are not sufficient to support the failing heart and concomitant tissue hypoxia and might need a shifting mode to venoarterial (V-A) ECMO support or of a hybrid veno-arterovenous (V-VA) ECMO. In the literature, there are currently no reported case series on the use of V-A ECMO in coronavirus outbreaks.
Has V-A ECMO Been Underused in COVID Pandemic?
Whereas the mortality of the majority of COVID-19 patients appears to be related to the development of multiorgan failure, complicating acute hypoxemic respiratory failure, or superimposed bacterial infections with sepsis, V-V ECMO remains the most frequently applied extracorporeal strategy, being used in 91% of the cases. Indeed, the preliminary data provided by the ELSO and European ELSO ongoing registries showed that less than 5% of the ECMO runs in COVID-19 patients were treated with V-A configuration. 31,32 Moreover, ECMO-assisted cardiopulmonary resuscitation (ECPR) was used in only 1% of COVID-19 cases in the ELSO registry; ECPR can be considered in carefully selected cardiac arrest patients who fail to obtain return of spontaneous circulation during conventional CPR and have a high likelihood of survival in case of restored circulation. However, because of the very poor outcomes being reported in severe COVID-19 patients and the considerable risk of infection transmission to responding staff, most of the centers interrupted their ECPR program and deprived these patients from a potential life-saving intervention. 12
Considering the frequent occurrence of cardiovascular complications in COVID-19 patients and the challenging discrimination between a cardiac and a respiratory etiology of hypoxemia in this setting, it is critical to recognize whether cardiac and pulmonary involvement coexists in these patients and provide the most effective ECMO configuration accordingly. In particular, cardiovascular ECMO support should be considered in 2 main scenarios:
Persistent hypoxemia that may evolve into RV dysfunction or failure (i.e., due to hypercapnia, acidosis, pulmonary hyperinflation, airway resistance, hypoxia, and thrombosis).
Cardiogenic shock of different origin with the coexistence of respiratory failure.
Importantly, cardiovascular ECMO support may include some hybrid configuration, such as V-AV mode (i.e., extra return cannula is inserted to improve the oxygenation in case of moderate cardiac dysfunction with high peripheral metabolic requirement and severe lung injury) or VV-A mode (i.e., an extra drainage cannula would provide an optimal biventricular unloading with concomitant high-flow ECMO, which would be effective in case of severe hypoxemia and high cardiac output; Fig. 1). 33
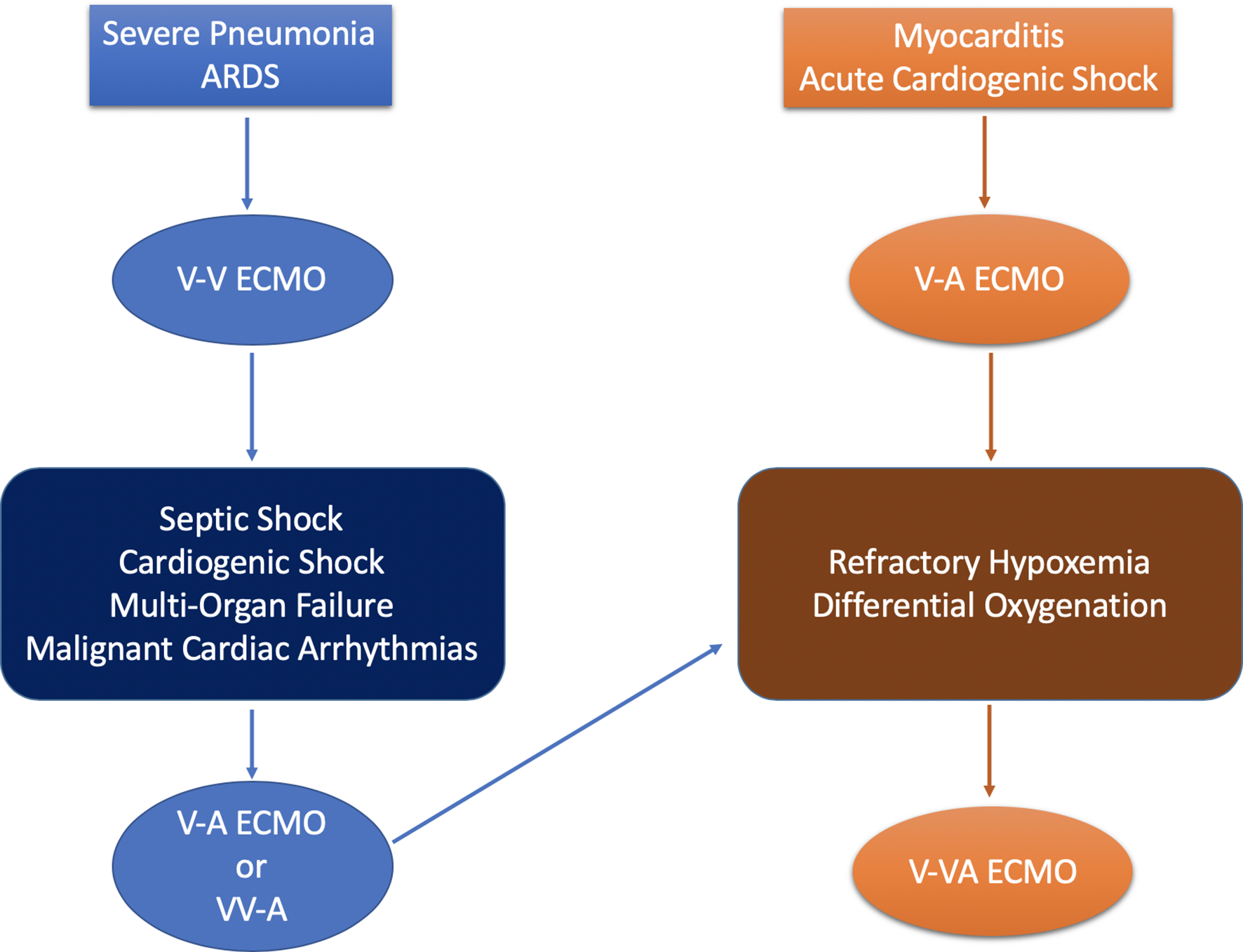
Different ECMO configurations in COVID-19 according to initial presentation or progress of the disease. ARDS, acute respiratory syndrome; ECMO, extracorporeal membrane oxygenation; V-A, venoarterial; V-V, venovenous; V-VA: veno-venoarterial; VV-A, venovenous-arterial.
From the available data reported until now, we can only postulate a possible underuse of the V-A modalities (i.e., 5%) when compared to the high incidence of cardiovascular complications (i.e., 20% to 30%). The reasons for this lower application of V-A configuration are related to the complexity of an arterial cannulation, the requirement of a backup from cardiovascular surgeons, the lack of experience in low-volume centers with V-A use, and the lack of recognition of cardiac dysfunction in this setting. The rate of conversion from V-V to V-A modes in COVID-19 has been only 3%, but it could have been much higher if a more accurate hemodynamic evaluation of these patients would have been done. We encourage international registries to analyze the cardiac function in COVID-19 ECMO patients to better define the potential role of V-A mode in this disease.
Conclusions
The overall impact of the COVID-19 pandemic on potential ECMO use is currently unclear and an urgent need exists to enhance our understanding of the role of ECMO in management of severely ill patients.
Some have advocated restricting mechanical support to V-V rather than V-A ECMO. Each patient must be considered on a case-by-case basis, with great attention regarding candidacy in the context of advanced age, and those comorbidities that portend to a reasonable poor prognosis.
More data are coming from the 2 large multicenter studies on the use of ECMO in COVID-19 patients promoted by ELSO and the European Group of ELSO which is leading to redefinition and reassessment of the real actual global ECMO capacity and capability. 31,32
Outbreaks of emerging infectious disease, such as COVID-19, represent an important step to improve our knowledge in ARDS and its different phenotypes in order to provide a better indication about the type of ECMO, target populations, as well as optimal time of implant.
Finally, the need for a multidisciplinary approach to this delicate population together with a more flexible and dynamic reassessment is essential. 34
This outbreak of infectious disease could enable an improved understanding of ARDS and a more precise use of therapeutics as ECMO and different configurations with a tailor-made treatment.
Take-Home Messages
Infectious outbreaks such as coronavirus disease 2019 (COVID-19) have been an unprecedented challenge in the treatment of virus-based pandemic due to the high rate of patients with severe compromised respiratory and cardiovascular systems.
The ethical and organizational circumstances, particularly the limited resources available during such an outbreak, have highlighted several shortcomings in the hospital network and patient management, including personnel availability and protection.
Despite initial skepticism, extracorporeal membrane oxygenation (ECMO), either veno-venous (V-V), or with a reduced use, venoarterial (V-A), has been increasingly applied in COVID-19 patients.
ECMO, however, remains a resource-intensive form of respiratory and circulatory support, which should be considered in special circumstances, with indications and selection criteria, which may vary according to the above mentioned shortcomings.
V-A ECMO represents, so far, a marginal quote (<5%) of extracorporeal support, apparently indicating a low incidence of cardiocirculatory compromise in COVID-19 patients. However, based on patient outcome and cause of deaths, doubts about an underutilization remain.
Several features of COVID-19 patients undergoing ECMO have also been increasingly appreciated and peculiar of this virus-induced patient compromise.
The main features and characteristics of ECMO in COVID-19 are need of high-flow V-V ECMO, awareness of those V-V cases with a rapid deterioration which may require conversion to an associated circulatory support (V-A, VV-A), need of prolonged support particularly to enhance lung recovery, and the need of enhanced anticoagulation due to the hypercoagulative state.
Several other configurations for cardiorespiratory support, “tailored” ECMO, have been utilized, but in a very limited rate (<1% to 2%).
In many ECMO centers, these procedures have been limited due to the lack of beds, dedicated personnel, lack of equipment or supply of disposables due to quick consumption, and an unexpectedly high number of patients potentially requiring such a treatment.
For the future, dedicated centers should receive adequate empowerment and resources and be better organized to improve the treatment of the severely ill requiring ECMO, including patient transport. Sicker patients should be centralized to allow access to such treatments, not excluding a full use of a patient-tailored algorithm for best support.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: F.S. Taccone, M. Belliato, M.M. Malfertheiner, and M.L. Broman received honoraria from EUROSETS. R. Lorusso is consultant for Medtronic and LivaNova, and Medical Advisory Board Member of EUROSETS and PulseCath.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.