
Abstract

Introduction
Recent trends demonstrate an increase in the proportion of bioprosthetic surgical valves in aortic valve replacement, instead of mechanical valves. One study evaluating 767,375 valves implanted in the United States has found that the proportion of bioprostheses increased from 37.7% in 1998-2001 to 63.6% in 2007-2011. 1 Other studies presented similar findings. 2 While advantageous for not requiring anticoagulation, bioprosthetic valves are prone for structural degeneration. Several devices may demonstrate as much as 40% rate of reintervention at long-term follow-up. 3 Failure rates may be even higher when considering echocardiographic degeneration, as a significant number of patients may be denied surgery due to severe comorbid burden. 4
Aortic valve-in-valve (ViV) may offer a less-invasive alternative for these high-risk patients, with a mounting global experience and excellent results. 5 However, the procedure has a learning curve and offers some important pitfalls that may even lead to life-threatening complications. In this editorial, we aim to share some of this experience, with the objective of discussing important risk factors for complications, how to appropriately plan for the procedure, and what operators should be looking for when evaluating their results. We summarize these tenets in the Ten Commandments of Aortic ViV.
1. Know Your Patient (and Their Valve)!
To obtain a successful result, knowing the anatomy of the patient is absolutely paramount. In the case of aortic ViV, much of this knowledge is concentrated on the specific failing bioprosthetic valve that the patient has. Dozens of bioprosthetic valves have been described in the ViV literature. 6 A meaningful stratification is that of stented versus stentless surgical valves. Stented surgical valves have rigid struts that support the porcine (older) or bovine pericardial (more recent) leaflets. Stentless valves, on the other hand, lack the structural support of stented valves, as its designers aimed to provide hemodynamics closer to the native valve. 7
Commonly, information about the model of the surgical valve and its size should be available in the original index operative report. However, considering that the original surgical aortic valve replacement may have taken place over 10 years ago, it is possible that this documentation will be lost. If that is the case, operators may obtain the size of the device through computed tomography (CT) evaluation. 8 Additionally, surgical valves have specific appearances, especially in the case of stented surgical valves that generally have typical fluoroscopic markers. An atlas of fluoroscopic images of surgical valves is freely available and may aid in preoperative planning. 9 Some novel surgical valves, such as the Inspiris (Edwards Lifesciences, Irvine, CA, USA), have the size of the surgical valve marked in the fluoroscopic frame.
As we will discuss in the next paragraphs, the type of surgical valve will have an important impact in outcomes, from residual elevated gradients to coronary obstruction, among other issues. It is highly relevant that the aortic ViV operator will be well-acquainted with these devices. The differences between ViV procedures in stented versus stentless valves have been extensively studied. In an analysis of 1,598 patients of the Valve-in-Valve International Data (VIVID) Registry, researchers have compared the clinical outcomes of 291 stentless surgical valves versus 1,307 stented surgical valves after aortic ViV with several differences found. 7 First, stentless surgical valves fail differently than stented surgical valves. Over 50% of patients in the stentless arm failed by aortic regurgitation as compared to 20% of patients in the stented arm. As a consequence, patients with stented valves have smaller effective orifice areas and higher gradients. 7
Second, operators oversized more in patients with stentless valves, especially in cases failed by regurgitation (8%, 3% in stented valves), aiming therefore to obtain a better seal of the transcatheter heart valve and avoid residual regurgitation. Third, severe complications were more frequent in stentless surgical valves. Namely, stentless valves had a higher rate of malpositioning, need for a second transcatheter heart valve, coronary obstruction, and paravalvular regurgitation ≥mild. 7 Malpositioning and need for a second valve are likely related to the lack of fluoroscopic markers to guide positioning. 10 This complication is associated with an increased need for reoperation in long-term follow-up. 11 Coronary obstruction will be discussed in the further sections. As advantages of stentless valves, we may enumerate a lower tendency for residual stenosis and prosthesis–patient mismatch. Although the complication rate was higher, no survival difference between stented and stentless valves was identified. 7 Sutureless valves can also degenerate and their ViV outcomes have been studied in detail. 12 In summary, it is essential to be fully prepared for whichever type of surgical valve that requires an aortic ViV procedure and to be aware of the pitfalls that may appear in that specific design.
2. Evaluate for Pre-ViV Prosthesis–Patient Mismatch
One of the most common adverse events with aortic ViV is residual stenosis. Gradients reflect a plethora of preprocedural, intraprocedural, and postprocedural parameters. One of the most relevant preprocedural factors is the presence of pre-existing prosthesis–patient mismatch of the surgical valve. Prosthesis–patient mismatch consists in a surgical or transcatheter valve that is inadequately sized for a patient (i.e., not a match), limiting forward flow and, therefore, incompletely relieving the original obstruction caused by degenerative aortic stenosis disease. Current echocardiographic guidelines define severe prosthesis–patient mismatch as indexed effective orifice area ≤0.65 cm2/m2 for nonobese patients (body mass index <30 kg/m2) and indexed EOA ≤0.60 cm2/m2 for obese patients (body mass index ≥30 kg/m2). 13
A large analysis from the VIVID Registry evaluated the outcomes in aortic ViV patients with pre-existing prosthesis–patient mismatch. 14 Mismatch was calculated by utilizing reference tables with effective orifice area values for each surgical valve model and size, 15 and then dividing the obtained values by the patient’s body surface area. Among 1,168 aortic ViV patients, 7.6% had pre-existing severe prosthesis–patient mismatch. 14 Unadjusted 1-year survival was significantly worse in patients with pre-existing prosthesis–patient mismatch (28.6%, 11.9% no/moderate mismatch, P < 0.001), and this difference persisted after multivariable adjustment (19.3%, 10.9% no/moderate mismatch; P = 0.03). Pre-existing prosthesis–patient mismatch was an independent predictor of 1-year mortality (hazard ratio 1.88; 95% confidence interval 1.07 to 3.28). Additionally, pre-existing prosthesis–patient mismatch was significantly associated with a higher incidence of elevated postprocedural mean gradients (78.3% of ViV patients with a balloon-expandable valve and severe mismatch having residual gradients ≥20 mmHg). Figure 1 shows the rates of elevated gradients, 30-day mortality, and 1-year mortality stratified by the presence of mismatch.
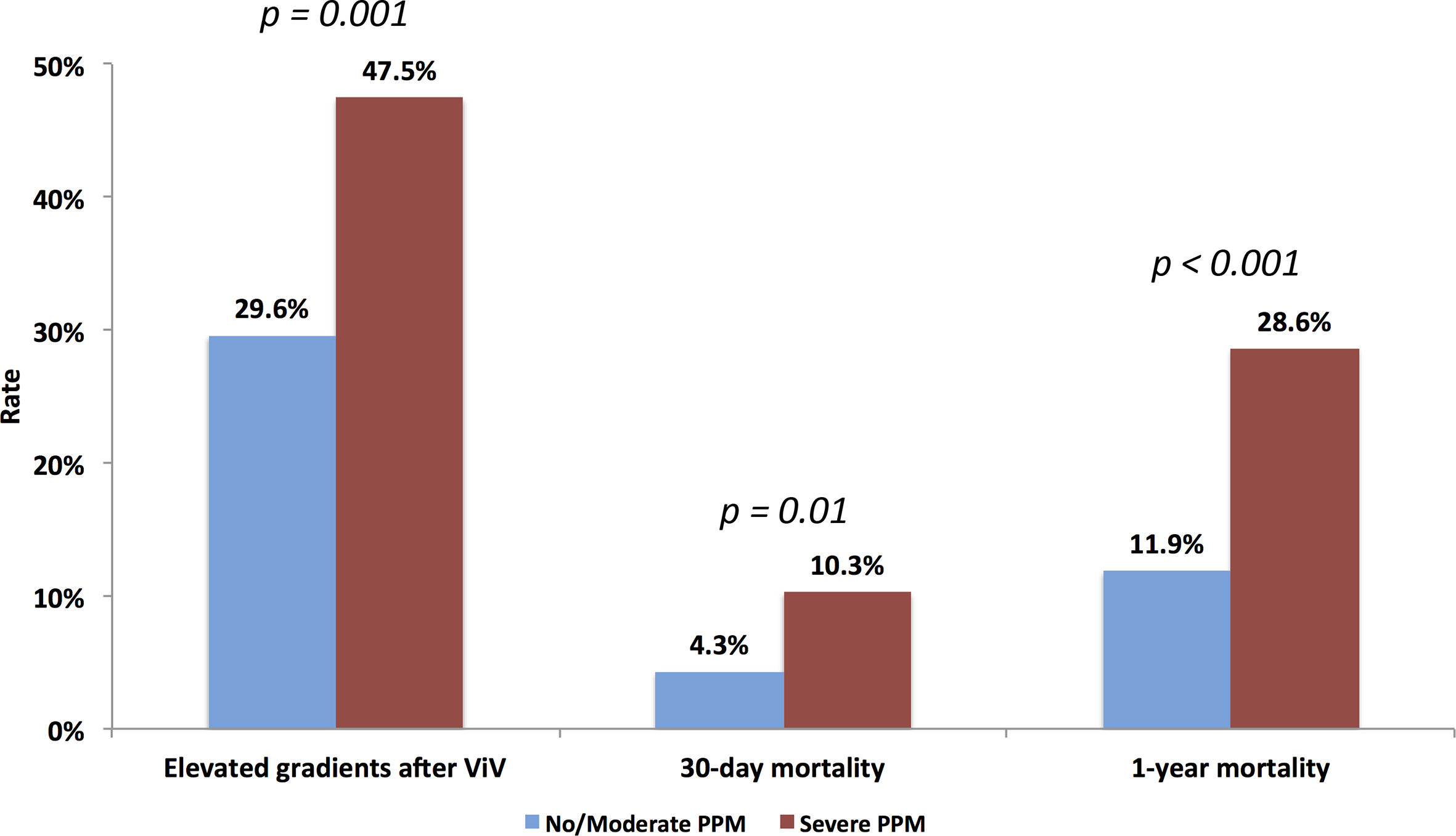
Rates of elevated gradients, 30-day mortality and 1-year mortality stratified by the presence of severe pre-existing prosthesis–patient mismatch. Reprinted with permission from Pibarot et al. 14
It has also been confirmed that pre-existing prosthesis–patient mismatch impacts long-term outcomes after aortic ViV. In a cohort of 1,006 aortic ViV patients with 8-year clinical follow-up, researchers identified that for every 1 mm decrease in the size of the failed surgical valve, there was a 7% increase in long-term mortality. 11 In the same analysis, pre-existing prosthesis–patient mismatch of the surgical valve was associated with a 4-fold rate of reintervention after ViV in a multivariable analysis controlled for competing risk of mortality (Fig. 2a). Mismatch increases turbulence and mechanical stress on leaflets, 16 which in turn place an undue pressure toward tissue degeneration. 17 This leads to decreased durability of both the index surgical valve 14 and the transcatheter heart valve if ViV is performed. 11
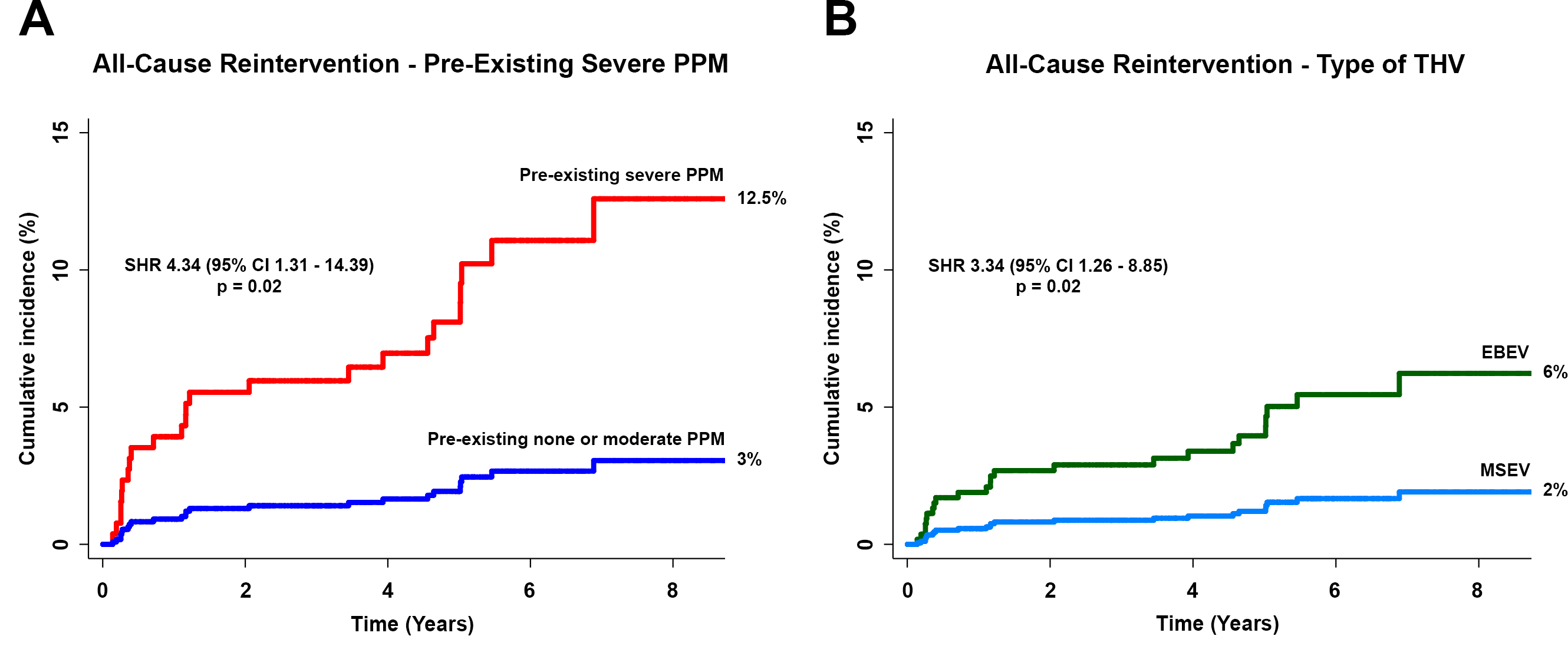
Independent predictors of the need for reintervention over 8-year follow-up in aortic ViV. Reprinted with permission from Bleiziffer et al. 11 CI, confidence interval; EBEV, Edwards balloon-expandable valve; MSEV, Medtronic self-expandable valve; PPM, prosthesis–patient mismatch; SHR, subhazard ratio; THV, transcatheter heart valve; ViV, valve-in-valve.
The operator may prepare by evaluating the indexed effective orifice area of the patient’s failed surgical valve during procedural planning. Calculators are available online for this purpose, such as the freely available VIVID app in the Apple App Store and Google Play Store. If the evaluated patient has pre-existing prosthesis–patient mismatch, this may preclude an effective aortic ViV procedure. However, alternatives, including bioprosthetic valve fracturing, may be considered.
3. Identify Cases at Risk for Coronary Obstruction
Coronary obstruction is a life-threatening complication of aortic ViV. The largest analysis on this topic evaluated 37 cases of this complication, among a total of 1,612 patients. 18 Total 30-day mortality among coronary obstruction cases was 48.6%, compared to only 3.7% in the control group (P < 0.001). Percutaneous coronary interventions (PCI) were attempted in 77.8% of patients and were successful in only 64.3% of them. In the failed PCI cases, 80% of patients died. Therefore, it is of paramount importance to identify the cases at highest risk for coronary obstruction, as there are interventions that may potentially protect the patient and that treatment after the obstruction has taken place may fail.
The anatomy of the patient is the most important factor in predicting the risk for coronary obstruction. Operators must take into consideration characteristics of the surgical valve, the width and height of coronary sinuses, and the relationship of all of these components to the coronary ostia. The main driver of coronary obstruction is the leaflet of the failed bioprosthetic valve. When the transcatheter heart valve is expanded, the leaflet of the failed bioprosthetic valve is deflected toward the coronary ostium and this may obstruct flow. Occasionally, the leaflet of the failed bioprosthetic valve may also block flow at the level of the sinotubular junction.
Surgical valves with leaflets mounted on the outside of stent posts (Mitroflow, LivaNova, London, UK; Trifecta, Abbott Laboratories, Abbott Park, IL, USA) and stentless valves may be at increased risk for coronary obstruction. However, it must also be noted that the risk of coronary obstruction when the coronary ostium position is above the stent post is minimal. Another aspect that must be taken into consideration is the horizontal distance between the valve and the coronaries, also known as the virtual transcatheter to coronary distance (VTC). A core-lab analysis of the VIVID Registry has shown that a VTC value ≤4 mm is a relatively accurate tool for assessing that risk, with an area under the curve of 0.943 for prediction coronary obstruction. 18
There have been attempts to standardize the classification of anatomical risk factors, with the development of a VIVID classification. 19 Patients with coronary arteries above the level of the highest deflection of the leaflets have type I anatomy, considered very low risk. In cases with leaflets deflected below the level of the sinotubular junction but above the coronaries (type II anatomy), the sinus width becomes of major importance, and cases with small VTC are considered at high risk of obstruction. Finally, patients with type III anatomy are those with leaflets that may deflect above the sinotubular junction, and these have, at least theoretically, the highest risk of obstruction. Figure 3 demonstrates the VIVID classification. This guidance is helpful for operators planning ViV procedures.

Valve-in-Valve International Data Registry anatomical classification for identification of coronary obstruction risk. STJ, sinotubular junction.
4. Exclude Cases With Possible Endocarditis, Thrombosis, or Predominant Paravalvular Regurgitation
Endocarditis after transcatheter aortic valve replacement (TAVR) is associated with poor outcomes. In 1 multicenter registry, two-thirds of endocarditis patients after TAVR died at 1 year. 20 In cases of surgical valve endocarditis, patients should not undergo ViV. Instead, surgical aortic valve replacement should be performed with appropriate debridement of infected tissue. Recently, a new role for functional imaging has been described. Researchers reported in a case series the use of positron-emission tomography-computed tomography (PET-CT) for the identification of endocarditis, particularly in situations where the Duke criteria are indeterminate. 21 The addition of PET-CT in selected cases to the ViV workup could be informative, but prospective studies on the topic would be needed. This may be utilized in cases with possible occult infection of a failing bioprosthetic valve.
In the same line, ViV is not optimal for cases of valve thrombosis or predominant paravalvular regurgitation of the bioprosthetic valve. In cases of thrombosis, the use of anticoagulation should be considered, with echocardiographic evaluation for gradient resolution and clinical evaluation for symptom improvement, before reintervention is planned. In addition, cases of predominant paravalvular regurgitation are not appropriately treated by ViV. In these situations, the most appropriate transcatheter intervention may include the implantation of a vascular plug.
5. Select Optimal Transcatheter Heart Valve for Your Particular Case
While several different transcatheter heart valves are currently available in the market, 22,23 the most widely used are the balloon-expandable SAPIEN 3 (Edwards Lifesciences) and the self-expandable Evolut (Medtronic Inc., Minneapolis, MN, USA). Each of these devices have specific advantages and disadvantages, and to date, no head-to-head prospective comparison in ViV has ever been performed. Operators must consider the degree of experience they have with each device. We recommend that operators utilize the device they are most acquainted with, until at least a comparable experience with both has been achieved. If the operator is proficient with both, then other considerations may come into play.
The hemodynamics of the SAPIEN family of devices has been consistently shown to be inferior to the self-expandable competitor in the context of ViV. 5 The SAPIEN is an intra-annular device, meaning that its leaflets are positioned at the level of annulus, an area with significant compression. The Evolut, on the other hand, is supra-annular when implanted high, which may lead to better expansion of the valve, with consequently larger effective orifice area and lower gradients. Considering that the majority of ViV cases are in stented valves, it is of essential importance to obtain the best transcatheter heart valve expansion possible as these stented valves do not offer much malleability. The concerns about the relationship of gradients and durability were related to studies assessing increased stress levels in transcatheter heart valves when compared to conventional surgical valves. 24 Up until recently, this concern was largely theoretical. However, in the evaluation of long-term outcomes of aortic ViV, the use of balloon-expandable valves has been identified, through multivariable analyses controlling for competing risk of mortality, as an independent predictor of need for redo aortic valve replacement. 11 Figure 2b demonstrates the rates of reintervention among patients with balloon-expandable valves and self-expandable valves. While the transcatheter heart valves utilized in these analyses were of older generations, which do not have the same leaflet technology of the current one, many of the original issues, such as those related to elevated gradients, were not resolved according to matched comparisons of ViV cases with the older SAPIEN XT (Edwards Lifesciences) and the SAPIEN 3, 22 especially when implanted inside small failed bioprosthetic valves.
Another important issue that must be considered is that of transcatheter heart valve sizing in relation to the failed surgical valve, as this may also impact hemodynamic results. In an in vitro study, Azadani and colleagues tested the implantation of different sizes of 23 and 26 mm Evolut devices in 21, 23, and 25 mm Hancock II (Medtronic Inc.) bioprostheses, with variations in the implantation depth. 25 In this analysis, the authors conclude that Evolut 26 mm will be superior to 23 mm for true ID above 17.5 mm. Therefore, sizing selection is key and operators may utilize references, such as the VIVID app, to obtain optimal recommendations.
6. Position the Transcatheter Heart Valve Optimally
Although the importance of gradients and residual hemodynamics is known, what tools are available for operators aiming to obtain optimal results? One of the most well-studied approaches is the depth of implantation. As we previously discussed, transcatheter heart valves may be divided into intra-annular and supra-annular. However, if a supra-annular valve is positioned excessively deep, it is possible to “intra-annularize” its leaflets, and therefore not obtain the advantages of improved expansion. Conversely, it would also be possible to position an intra-annular valve in a position with less critical constriction.
In a bench study, investigators studying the implantation of Evolut, SAPIEN XT, and the Portico valve (Abbott Laboratories) positioned these devices at varying depths in small surgical valves (label size 19 mm), aiming to simulate stenotic conditions. 26 Significant relationships were obtained in polynomial regressions for the depth of implantation of all these devices and the variables of interest, mean gradients, and effective orifice areas. Transcatheter valves positioned high had lower mean gradients and larger effective orifice areas. In addition, leaflet coaptation was superior in valves implanted higher, 26 which may influence long-term durability.
These findings were later confirmed with a multicenter core-lab study, in which investigators evaluated the implantation depth of 292 consecutive aortic ViV patients (157 Evolut, 135 SAPIEN XT). 27 An Evolut implantation of 0 to 5 mm below the surgical valve ring, and an XT implantation of 0 to 2 mm below the surgical valve ring were defined as optimal after receiver operating characteristic curve analysis. Patients with high implantation had a significantly lower rate of postprocedural mean gradients ≥20 mmHg (Evolut: 15% vs 34.2% deep implantation, P = 0.03; SAPIEN XT: 18.5% vs 43.5%, P = 0.03). The importance of implantation depth was confirmed in a multivariable analysis controlling for relevant confounders, including the transcatheter heart valve model and the mechanism of failure of the surgical valve. 27 Similar findings were obtained in a dedicated analysis of aortic ViV and SAPIEN 3 implantation, with optimal final depth of 20% and central marker positioning 3 to 6 mm above the surgical valve ring. 28 It is important that ViV operators will be well acquainted with positioning techniques to obtain the best-possible hemodynamic result, particularly so in cases at high risk for elevated gradients (e.g., preprocedural prosthesis–patient mismatch, small true internal diameter, stenosis as the mechanism of failure, among others).
7. Consider Bioprosthetic Valve Fracture
Bioprosthetic valve fracture consists in the modification of the surgical valve ring with a noncompliant balloon inflated at high pressure. While the rings are visible in fluoroscopy, they are not typically made of metal, but are actually a plastic structure, which is, therefore, pliable with sufficient pressure and even breakable. The technique was first described in 2015, 29 but only recently gained traction with larger worldwide experience. 30,31
The largest study on the topic reported on the 75-patient experience of 21 centers. 30 As expected, patients had small surgical valves, with a mean true internal diameter of 18.3 mm. The majority of cases had fracturing performed after transcatheter valve deployment (88%, 12% fracturing before). Fracturing was successful in 100% of patients, with a 30-day mortality of 2.7%. In terms of complications, there were no coronary obstruction, annular rupture, or pacemaker events, although these adverse events have been described anecdotally after this procedure. In 2 cases included in this analysis there was new onset of severe aortic regurgitation after balloon fracturing, which resolved with a second transcatheter valve implantation. In terms of gradients, there was a significant decrease in mean gradients after fracturing. However, this decrease was more pronounced in patients who underwent bioprosthetic valve fracturing after implantation of the transcatheter heart valve.
While promising, only limited clinical follow-up beyond 30 days is available. Additionally, no large head-to-head comparison between patients undergoing bioprosthetic valve fracturing versus conventional aortic ViV has been done. However, the rate of severe complications appears to be low and the gradient reduction is substantial. Further studies on the topic are ongoing.
There are important advantages and disadvantages related to the timing of bioprosthetic valve fracture. When performing bioprosthetic valve fracture first, there is no possibility of damaging the new leaflets of the transcatheter heart valve. Balloon pressures range from 8 to 27 atmospheres 32 and the effects of such a stressor over the long term, particularly on durability, are still unknown. On the other hand, advantages of performing fracturing after the ViV procedure include the knowledge of the prefracturing hemodynamic result, as the operator cannot be sure of the true necessity of fracturing when performing it prior to transcatheter heart valve deployment. We suggest that operators have transcatheter heart valves close to readiness for new implantation in the, albeit rare, case of acute decompensation.
Situations that should highlight a potential need of bioprosthetic valve fracture are those related to prosthesis–patient mismatch: small surgical valves, stenosis as the mechanism of failure of the surgical valve, intra-annular transcatheter heart valves, stented surgical valve, and excessively deep valve positioning. When considering the possibility of bioprosthetic valve fracture, operators must also keep in mind that not all surgical valves are amenable to fracturing. Several utilized valves, such as the Hancock (Medtronic Inc.) and the Trifecta (Abbott Laboratories), cannot be conventionally fractured. For the valves that can be fractured, bench studies have established the thresholds of balloon inflation for fracturing and these should be consulted before attempting the procedure. 32 High-quality procedural planning is always essential, but especially so when considering bioprosthetic valve fracture. Longer-term studies on the effectiveness of this technique are certainly warranted.
8. Plan for BASILICA or Chimney/Snorkel Techniques in Appropriate Cases
As previously discussed, coronary obstruction is a feared complication of aortic ViV. Two techniques are part of the therapeutic arsenal against coronary obstruction. BASILICA is the acronym for “Bioprosthetic or Native Aortic Scallop Intentional Laceration to Prevent Coronary Artery Obstruction,” a technique first described in 2018 after in vitro and in vivo testing, with also the first-in-human cases. 33 The procedure essentially consists in the electrification of a 0.014-inch guidewire, which is used to perforate the failed surgical valve leaflet. After initial perforation, the free end of the wire is snared and the wire is pulled with simultaneous electrification. This procedure cuts the leaflet, allowing it to splay after ViV, effectively permitting blood flow through the stent frame of the transcatheter heart valve.
Evidence for BASILICA is mounting. In a prospective study with 30 patients at high risk for coronary obstruction, there was 100% freedom from coronary obstruction and reintervention in BASILICA patients. 34 Hemodynamic compromise, a theoretical complication given sudden laceration of the leaflet, which could lead to regurgitation-induced acute heart failure, was present in 7% of patients and subsided with TAVR. 34 Other independent series have shown similar results. 35 BASILICA does require extensive planning prior to the procedure and has a steep learning curve. 36,37 In terms of the implantation itself, while step-by-step guides are available in the literature, close proctoring is considered essential for a successful procedure. 37
As an alternative to BASILICA, the chimney/snorkel technique consists in the deployment of a coronary stent extending from the coronary ostium to a cranial direction, parallel to the transcatheter heart valve leaflet. 38 While it was typically performed as a bailout strategy for coronary obstruction cases, prophylactic use for high-risk cases has become more common. 38 Data on the chimney technique are relatively limited. A multicenter registry reported on 60 cases of chimney stenting, the majority of which were ViV. 38 The investigators found that stenting of an established coronary obstruction was associated with poor results, including high rates of myocardial infarction (52%, 0% nonestablished, P < 0.01). The sole predictor of myocardial infarction, cardiogenic shock, and death in a multivariable analysis was the absence of coronary protection (i.e., wiring of the coronary prior to transcatheter heart valve deployment). One potential drawback of chimney stenting is that coronary stents are not designed for implantation outside of a coronary artery. Therefore, the risk of incomplete closure or thrombosis needs to be considered. Longer-term follow-up will be needed. We would recommend that, for operators interested in using this technique, preemptive coronary protection should be performed, instead of reactive access of the coronary ostia after transcatheter valve deployment, which can be very challenging.
9. Consider Anticoagulation Therapy
Hypoattenuated leaflet thickening of the transcatheter heart valve has been recognized as a potential complication of TAVR. 39 Thrombotic material accumulation in the leaflets may lead to increased gradients, which could lead to acute heart failure. Thrombosis may also present asymptomatically, with a gradient increase found on follow-up transthoracic echocardiography. Prior series on native TAVR had lower incidences between 0.6% and 2.2%. 40,41 ViV procedures have previously been identified as a risk factor for development of thrombosis, 40,42 with 1 analysis showing almost 6-fold risk increase. 40
A specific analysis of aortic ViV thrombosis has been performed utilizing the VIVID Registry. 43 Investigators identified 23 cases of ViV thrombosis among 300 procedures, with an estimated incidence of 7.6%. 43 The median time to development of thrombosis was 101 days after the procedure. Approximately two-thirds presented symptomatically, and 91% had an increase in mean gradients. Median mean gradient at diagnosis was 39 mmHg. Some key risk factors were identified for the development of ViV thrombosis. Patients with small surgical valves and large body surface area, a surrogate for mismatch, had an increased risk of thrombosis. Additionally, patients with Mosaic and Hancock II surgical valves (Medtronic Inc.) had a 4-fold increase in thrombosis risk. 43 For patients with these valves and not on anticoagulation, thrombosis rate approached a quarter of cases.
Use of anticoagulation was highly protective against thrombosis, with a 93% reduction in the risk of development. Anticoagulation was also effective in the treatment of ViV thrombosis, with a reduction of median mean gradients from 39 to 17.5 mmHg. Many proposed mechanisms for the thrombosis risk increase in ViV exist. Computational studies suggest that ViV procedures are associated with a decrease in flow and shear stress, leading to greater flow stasis. 44 Other studies have proposed that an increase in blood residence time in the leaflets may be part of the explanation. 45 In the specific case of Hancock II and Mosaic valves, one of the potential explanations for the increased risk is that these surgical valves have a rail in the sinus portions that may lead to local blood stasis. 46
The question of whether to anticoagulate TAVR, and more specifically ViV, patients is a relevant one. Only 1 randomized study has evaluated this question in patients without a prior indication for anticoagulation (e.g., atrial fibrillation), the GALILEO study, which randomized patients to rivaroxaban or antiplatelet therapy and included few ViV patients (5.5%). 47 In this study, there was a significant increase in mortality in the rivaroxaban cohort. 47 However, in the core-lab CT evaluation of this trial, investigators found a decrease in subclinical leaflet motion abnormalities in the rivaroxaban group. 48 Therefore, it is clear that while anticoagulation may be effective for prevention of thrombosis, it should not be used indiscriminately. While no prospective studies specific to the ViV population are available, we believe that anticoagulation may be employed in selected patients at high risk for thrombosis (e.g., Hancock II/Mosaic, severe prosthesis–patient mismatch) and at low risk for bleeding for a period of 3 to 6 months, with close clinical follow-up for bleeding events. Even if the operator decides to not anticoagulate, it is reassuring that thrombosis cases tend to resolve after a course of this medication.
10. Meticulously Follow Your Patient With Echocardiography
Close follow-up is one of the main determinants of a successful result in ViV. The ViV population is a highly comorbid population, requiring close care. It is also known that bioprosthetic valves will eventually fail. It is, therefore, recommended to follow ViV patients with echocardiography. Our recommendation is that operators obtain direct hemodynamic measurements after the implantation of the transcatheter heart valve. Afterwards, an echocardiogram should be obtained at discharge, another at 30 days, and then annually. The transcatheter heart valve should be evaluated according to current recommendations. 4,49 If signs of degeneration appear (e.g., new onset of stenosis, regurgitation), the frequency of echocardiography can be increased to every 3 to 6 months. Care should be taken to distinguish causes of poor hemodynamics, including the possibility of postprocedural mismatch. 50 In cases of suspected thrombosis, reintervention should be avoided until a therapeutic trial of anticoagulation has been performed, unless contraindicated. In symptomatic patients with severe degeneration, reintervention should be considered. 51
Conclusions
Aortic ViV is a fascinating but potentially complex procedure that may be safely used to treat patients with bioprosthetic valves at high risk for conventional redo surgical aortic valve replacement. Operators should devote sufficient care to the preprocedural planning stage and employ strategies delineated in this review in order to obtain optimal results. We invite centers interested in the procedure to participate in the investigator-initiated VIVID Registry, which aims to improve outcomes of these procedures for the benefit of our patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Dvir is a consultant to Edwards Lifesciences, Medtronic Inc., JenaValve, and Abbott.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.