
Abstract

Introduction
The introduction of hybrid arch repair techniques as an alternative to purely open approaches has greatly facilitated the management of aortic arch and proximal descending thoracic aortic disease. Surgery on these aortic segments is challenging to address through either a sternotomy or thoracotomy alone, and so was traditionally often tackled in separate stages. In 1983, Borst et al. introduced the elephant trunk (ET) technique, where through a median sternotomy, a 10-cm section of Dacron graft is left distal to the site of distal anastomosis in the arch. 1 The second stage is then carried out through the left chest where the proximal anastomosis is now simplified by the ET. Inter-stage mortality remains a concern with this approach. 2,3
The frozen elephant trunk (FET) procedure was first described by Kato et al. in 1996, and it evolved through adoption of thoracic endovascular aortic repair (TEVAR) techniques. 4 Stent-graft technology has been a revolutionary advance, converting surgeries with large morbid incisions into minimal-access procedures. Having a stent-supported ET affords several benefits that we will review, including the optimization of subsequent aortic interventions in the contemporary era of endovascular intervention, and elimination of the second-stage repair in some patients. It has also been an important addition to the armamentarium in the treatment of acute type A dissections. 5,6
Endovascular arch repair that avoids cardiopulmonary bypass and a median sternotomy altogether remains fraught with stroke risk and technical challenges related to arch angulations and inadequate proximal fixation. These techniques are in fact usually hybrid in that they tend to incorporate varying degrees of open arch vessel debranching. New developments in this area and a comparison of various hybrid arch techniques are explored.
Patient Selection
There are 3 predominant scenarios for use of hybrid arch repair: (1) distal arch/proximal descending thoracic aneurysms (DTAs); (2) extensive aneurysms involving the arch and descending thoracic or thoracoabdominal aortic aneurysms (TAAA); and (3) acute type A aortic dissections (ATAAD). While many options exist for the treatment of each of these aortic conditions, certain factors may make the hybrid arch a particularly attractive option.
Distal Arch/Proximal DTAs
Distal arch and proximal DTAs are located in a challenging anatomical location. From a median sternotomy, it may not be possible to safely and proficiently perform the distal anastomosis in zones 3 or 4, deep posteriorly in the patient’s chest. The more morbid hemi-clamshell or full clamshell approach may be necessary for proper anterior exposure to the most distal aspect of these aneurysms. Alternatively, a thoracotomy may be performed, but this approach is associated with more tissue dissection, pain, and pulmonary dysfunction. 7 Access to the ascending aorta and proximal arch is more limited through the left chest if the proximal aorta or arch branch vessels are involved. If circulatory arrest is necessary, cerebral perfusion is more challenging through a thoracotomy.
A recent retrospective review of surgical approaches to these types of aneurysms found that median sternotomy resulted in less death (3.1% vs 11.9%), stroke (3.1% vs 13.1%), and superior long-term survival (82.8% vs 61.0%) at 10 years, compared to thoracotomy. 8 The hybrid arch/FET strategy facilitates a median sternotomy approach to these aneurysms by allowing the distal anastomosis to be moved more proximally to zone 2 (or even more proximally as required). The FET then seals off the aneurysm at the distal landing zone in the descending thoracic aorta (Fig. 1). In the setting of chronic distal dissections, the FET may delay or avoid the need for a distal aortic repair (Fig. 2).
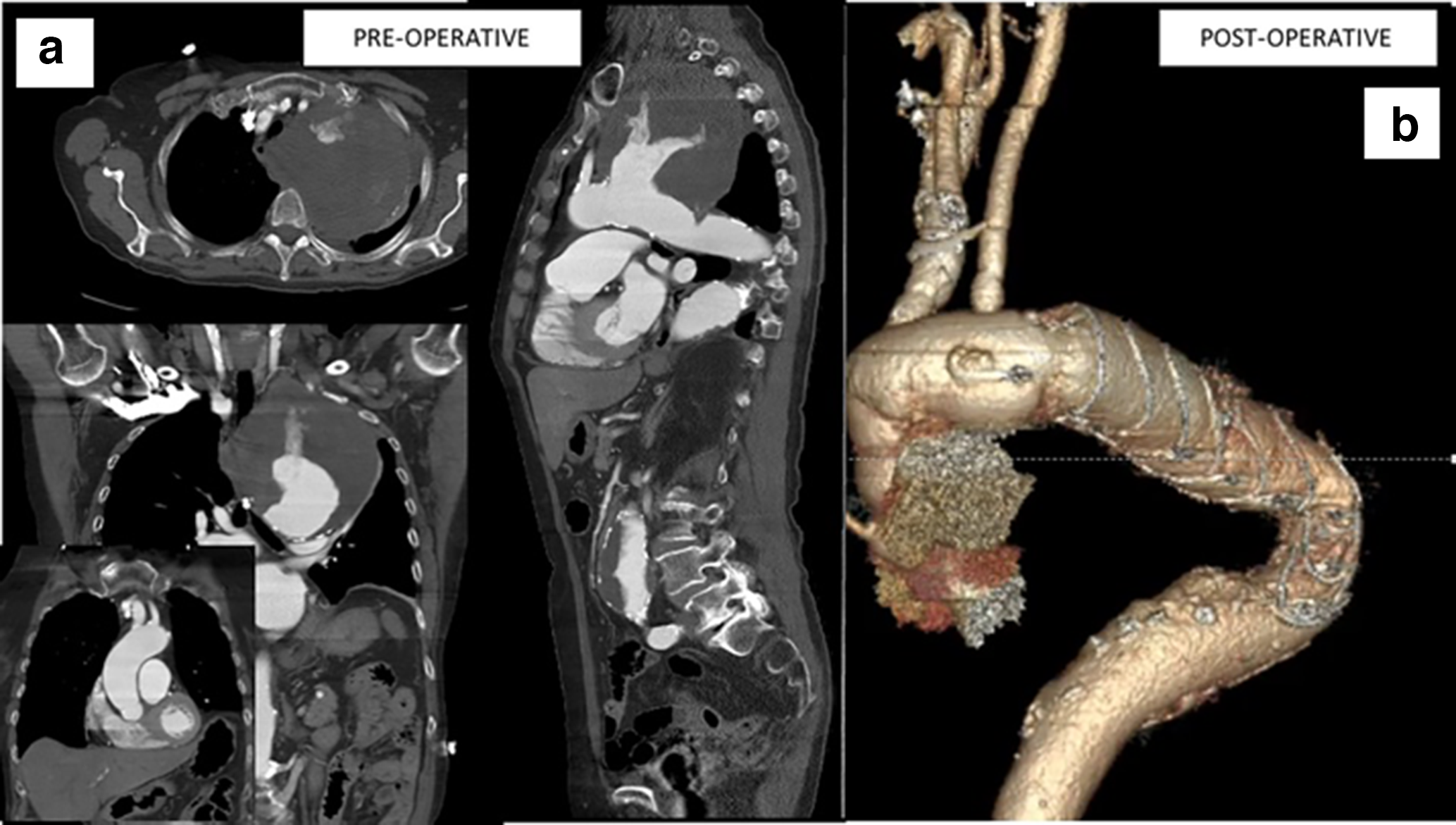
Distal arch aneurysm treated with hybrid arch/frozen elephant trunk repair. (a) Selected preoperative images showing large distal arch aneurysm. (b) Postoperative 3-dimensional reconstruction following repair with Thoraflex plexus device.
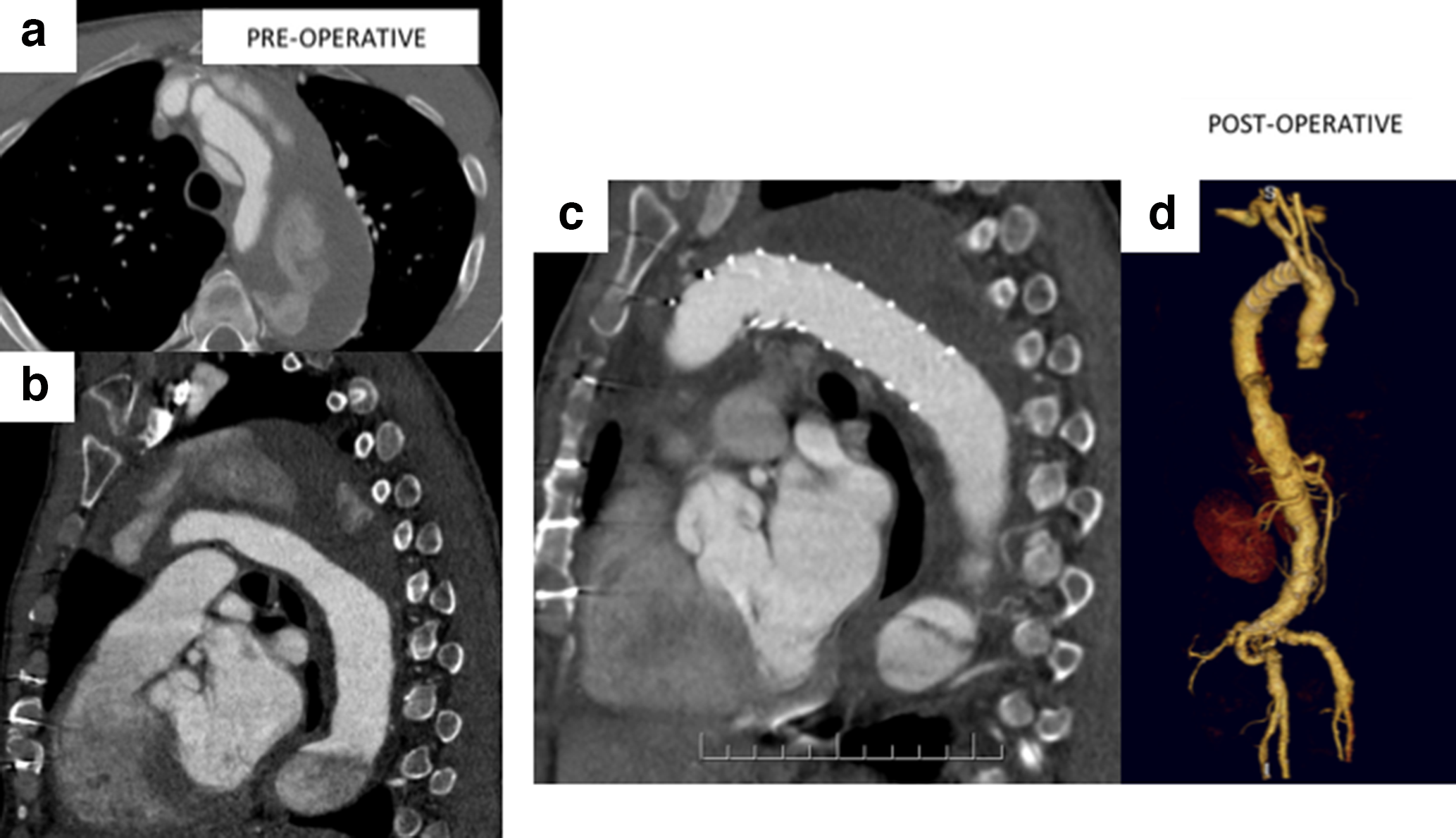
Hybrid arch/frozen elephant trunk repair for chronic distal dissection. (a,b) Selected preoperative images showing chronic distal dissection in patients with previous type A dissection repair. (c,d) Postoperative sagittal and 3-dimensional reconstruction following repair with Thoraflex Anteflo device.
Hybrid techniques that involve arch vessel debranching and subsequent TEVAR are another possibility in select patients with distal arch/proximal DTAs. Variations of this approach and total endovascular arch repair techniques tout the advantage of avoiding an open anastomosis and cardiopulmonary bypass. However, they are less versatile than the hybrid arch/FET technique and are hampered by anatomical constraints. These include the need for adequate access and landing zones that are not aneurysmal and without excessive curvature. 9 Patients with heavy thrombus burden in the arch should also be avoided. There are size restrictions for the ascending aorta as rates of retrograde type A dissection increase with ascending aortic diameters greater than 40 mm. 10 Patients with connective tissue disorders are poor candidates for these techniques. 11 A recent meta-analysis demonstrates that although technical success rate is high (93%), there are significant risks of stroke (7.6%), endoleaks (16.6%, majority type I), and retrograde type A dissection (4.5%). 12 Reintervention rates are also higher than with open repair. 13 To whom this category of hybrid arch repair should be offered remains controversial. We reserve its use in patients with hostile resternotomies and severe comorbidities such as advanced cardiopulmonary disease. As a second-line approach, a small proportion of arch patients will be candidates given the limitations listed above.
Extensive Aneurysms Involving the Arch and Descending Thoracic or TAAA
Borst and colleagues initially envisioned the ET technique to set up subsequent open aortic surgery through left thoracotomy for extensive DTA/TAAA that extend beyond the arch. Having an appropriate-length ET enables clamping of the ET during the second-stage repair, and avoidance of circulatory arrest for the proximal anastomosis. Anastomosis to a synthetic graft is also very straightforward and eliminates concerns about tissue quality and bleeding. Practical limitations have included the at-times harrowing experience of grabbing a floppy and short ET. Other complications that have been described include ET kinking in overly long and improperly deployed ETs. On the other hand, the shape and length of FETs positioned in the distal thoracic aorta are entirely predictable. There is little stress involved in controlling and clamping a FET upon opening the DTA/TAAA.
In addition, in the current era, the subsequent treatment of DTA/TAAA after arch surgery is often endovascular. Guidewire cannulation of traditional ETs, although possible, is technically challenging as the graft may accordion onto itself and may not serve as an adequate landing zone. Several adjunctive techniques have been developed, many of which require forethought during the initial ET deployment. In contrast, guidewire cannulation of the FET is very simple, and the FET serves as a stable and optimal landing zone.
Acute Type A Aortic Dissection
Sun and colleagues have popularized the routine use of the hybrid arch/FET technique in treatment of ATAAD. 6 The group reported a staggering 94.2% false lumen thrombosis rate around the FET with an impressive in-hospital mortality rate of 3%. By extending the repair beyond the usual hemiarch replacement, this technique promotes true lumen expansion and resolution of malperfusion. 5,14 In certain hands, extended arch repair during ATAAD does not appear to increase operative mortality in registry and retrospective studies. 15,16 These results have been replicated in other groups, who also report 93% 10-year freedom from thoracic aortic reoperation, presumably from positive aortic remodeling secondary to the FET. 5 The International Registry of Aortic Dissection found similar 5-year rates of freedom from death, aortic rupture, and reoperation between those undergoing standard versus extended arch repairs. 17 It is possible that the group undergoing extended arch repairs would have had worse outcomes had the patients undergone standard repairs, but the long-term benefits of using extended arch repair techniques such as the hybrid arch/FET for ATAAD are still debatable. The Canadian position statement on open and endovascular surgery for thoracic aortic disease recommends considering extended arch repairs in the setting of intimal entry tear in the arch or descending thoracic aorta, or significant aneurysmal disease of the arch. 18
A variant on FET in ATAAD is the Ascyrus Medical Dissection Stent (Cryolife Inc., Atlanta, GA, USA), a novel hybrid arch prosthesis with an uncovered nitinol stent and a proximal felt cuff. This uncovered stent with low radial force is deployed antegrade during the open distal anastomosis of ATAAD repair. As it is uncovered, it may be deployed across the arch branch vessels. Early experience with this novel graft is promising with positive aortic remodeling in 100% of cases, and 95% resolution of vessel malperfusion. 19 Unlike with FET, spinal cord ischemia does not appear to be a concern.
Other Indications for Hybrid Arch Repair
There are other less-common scenarios where hybrid arch techniques can be helpful. In cases of type 1A endoleak after TEVAR, arch debranching and proximal TEVAR extension may resolve the endoleak. In patients with challenging arch anatomies or further aneurysmal degeneration of the proximal landing zone, however, further proximal extension with a TEVAR may not be an option. The hybrid arch/FET technique is a very effective solution. 20 For open surgical candidates, an FET hybrid device landed within the previously placed TEVAR may provide a more secure and definitive solution than a simple suture line onto the previously placed TEVAR.
Some groups have experience using the hybrid arch/FET technique for the treatment of acute complicated type B dissections. 21 -23 Clearly, TEVAR has transformed the management of acute complicated type B dissections and it has largely supplanted open repair. However, if no proximal landing zone is available, the patient has a moderately dilated arch or the patient has a connective tissue disease and is at elevated risk of retrograde type A dissection, hybrid arch/FET should be considered. A large case series has shown success in true lumen expansion and false lumen regression with minimal morbidity and mortality. 23 This solution may be preferred to open distal aortic repair in acute type B dissections, which is associated with high morbidity and mortality.
Surgical Technique
In the University of Pennsylvania classification system of hybrid arch repair, techniques that avoid circulatory arrest are termed type 1. 24 Arch vessels are debranched and moved proximally to lengthen the proximal landing zone for subsequent TEVAR. Type 2 repairs involve replacement of the ascending aorta and hemiarch replacement to create an adequate landing zone for TEVAR after arch vessel debranching in the setting of a dilated ascending aorta. In our opinion, type 2 repairs are more or less obsolete in the era of specifically designed hybrid total arch/FET grafts, which fall under the category of type 3 repairs. Type 3 hybrid arch repair is generally our preferred technique for its versatility and is described in detail below.
Hybrid Arch/FET Repair
Although several variations exist, the general conduct of the hybrid arch/FET repair is similar in setup to traditional arch replacement techniques. Strategies for cannulation, cerebral perfusion, and arch vessel reconstruction are largely unchanged. One unique consideration is sizing of the prosthesis. If the goal is to seal the aneurysm with the FET, the size of the stent graft would be dependent on the distal landing zone. Generally, 15% to 20% oversizing with 3 to 4 cm length of landing zone should suffice for most devices; however, prosthesis-specific IFU should be reviewed. In cases of acute or chronic dissections, minimal oversizing should be applied in order to prevent stent-induced new entry tears. 25 This well-described phenomenon results in persistent false-lumen perfusion and consequent negative aortic remodeling. Additional sizing considerations arise when subsequent endovascular repairs are planned. The anticipated size of the subsequent endoprosthesis would dictate sizing of the FET.
Once in the operating room, to prepare for deployment of the FET device, a wire is introduced from the femoral artery into the aortic arch after systemic heparinization. Its positioning should be confirmed by fluoroscopy, transesophageal echocardiography, or intravascular ultrasound. For cases of aortic dissection, it is imperative to confirm that the wire is correctly positioned in the true lumen of the thoracic aorta. Then, under circulatory arrest, the wire is retrieved from the aortic arch and the FET device is introduced antegrade over the wire and deployed. Alternatively, some FET devices are designed for direct antegrade positioning without a wire. The advantage is that in the case of dissection, true lumen identification is simple and advanced imaging to ensure accurate placement of the wire in the correct lumen is unnecessary. The pitfall of this seemingly simpler approach is the potential for catastrophic aortic rupture in the descending thoracic aorta if the prosthesis is not smoothly delivered, or deployment in the false lumen if the device crosses through a large reentry tear.
Position of the arch anastomosis of the FET may be in any aortic zone. In fact, proximalization of the anastomosis is one of the major advantages of the FET technique. For many patients, zones 3 and 4 are far more posterior in the chest than zone 2 and repair in these zones risks injury to the left recurrent laryngeal nerve. Sewing the distal anastomosis in zone 2 is more convenient, and the stent-graft is used to effectively and significantly extend the repair beyond this anastomosis. Thoughtful planning for head vessel reconstruction is necessary, particularly in the case of difficult-to-reach left subclavian arteries. 26 Once positioned, the device is released from the delivery system. The delivery system is retrieved and the guidewire is withdrawn. Some hybrid FET devices such as the Thoraflex are designed with a sewing cuff to facilitate the anastomosis, as illustrated in the Supplemental Video. The proximal repair, including management of the arch branch vessels, may be carried out as with any traditional arch operation.
Hybrid Arch Without Open Anastomosis
To allow for arch TEVAR, arch debranching may be performed through extra-anatomic bypasses in the neck, most commonly with carotid–subclavian bypass (and proximal ligation) or transposition. Carotid–carotid bypass in addition to the carotid–subclavian bypass, debranches the arch vessels further, moving the proximal TEVAR landing zone to zone 1. To achieve zone 0 stenting, arch vessels may be debranched off the proximal ascending aorta using a side-biting clamp. Oftentimes, a radio-opaque marker is left around this anastomosis to facilitate the endovascular component of the procedure. TEVAR is carried out in the usual manner, except that cardiac output is usually tightly controlled during endograft deployment using rapid ventricular pacing, pharmacological means, or inferior vena cava balloon occlusion.
Meta-analyses and propensity-score-matched data suggest that these type 1 hybrid techniques are associated with higher rates of stroke and reintervention, when compared to open arch repair. 13,27,28 These increased complication rates may be related to the required increased intravascular manipulation as well as the characteristically unstable zone 0 landing zone. Therefore, we believe that these techniques are most suitable when contraindications for cardiopulmonary bypass and an open anastomosis are present, such as in the event of an extreme-risk resternotomy or patient comorbidities.
Alternatively, a modular approach to endovascular repair of the aortic arch with branches and fenestrations may be considered in patients with relatively normal or previously replaced ascending aortas. When used to provide zone 0 and 1 coverage, these grafts are usually combined with arch debranching in a hybrid repair strategy. A selection of available devices is described below with their associated early outcome data. These are technically challenging cases and experience with these devices is very limited and isolated to centers with experienced in advanced EVAR.
Techniques involving chimneys and snorkels have unacceptably high rates of gutter leaks and are generally reserved as bail-out strategies. 29
Outcomes of Current Devices
Homemade Hybrid Total Arch FET
The initial case series by Kato et al. reported 10 patients who received homemade hybrid arch grafts. These homemade devices have largely been supplanted by off-the-shelf hybrid FET devices, although cost and availability have led to their ongoing use. Depending on how they are constructed, these homemade devices may be accompanied by higher rates of type IA endoleaks.
Off-the-Shelf Hybrid FET Devices
There are several devices on the market designed for open deployment of hybrid arch grafts (Fig. 3). There is a stent-graft FET section of nitinol-supported Dacron. The nitinol design varies, ranging from individual hoops (Thoraflex Hybrid), z-stents (E-vita, Cook hybrid graft, Cronus open), to a single knitted wire (Frozenix). 30 -32 The stent-graft section seamlessly connects to an unsupported Dacron section for the proximal repair and the sections may not be uniform in size. Presence of a collar at the junction between the 2 sections can be helpful with the anastomosis of a large arch. Additional features that may be selected for in the proximal Dacron section include having a side branch for reinstituting systemic cardiopulmonary bypass, and individual branches for arch vessel anastomoses.
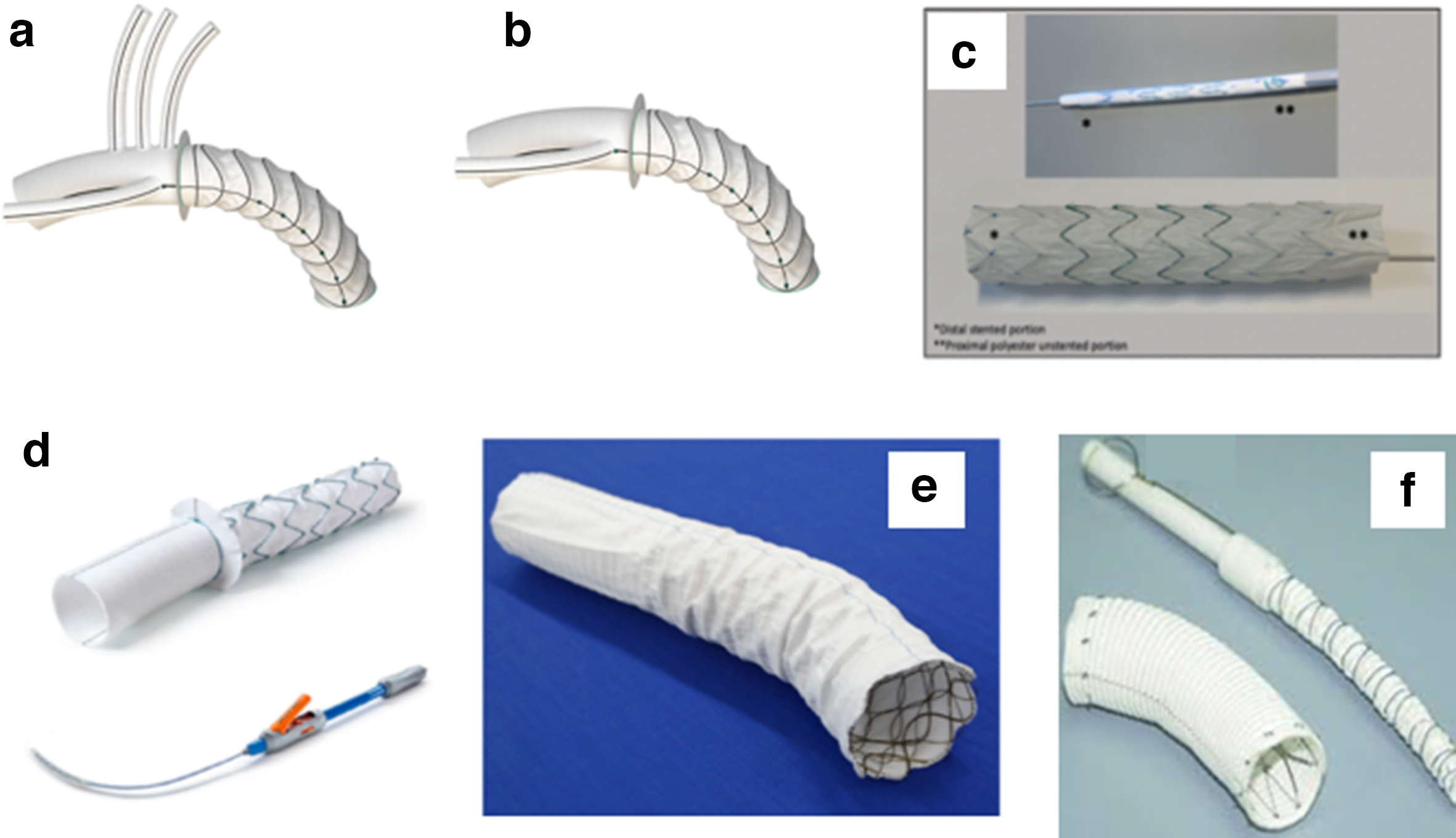
Selection of available hybrid arch/frozen elephant trunk devices. (a) Thoraflex hybrid plexus device; (b) Thoraflex ante-flo device; (c) Cook hybrid stent-graft; (d) e-Vita open plus device; (e) Frozenix device; (f) Cronus device.
A recent review conducted by the Vascular Domain of the European Association of Cardio-Thoracic Surgery did not identify significant outcome differences between the devices, but a wide range of complication rates have been reported by large single-center series. 33 In aggregate, the in-hospital mortality rate was 1.8% to 17.2%, stroke rate was 2.5% to 20%, and spinal cord ischemia rate was 0% to 21%. The Canadian experience with hybrid arch repair (the majority of which involved off-the-shelf hybrid FET devices) included 167 patients with a mean age of 65 ± 13 years, 30% of whom underwent urgent or emergent surgery. 34 In this cohort, there was an 8% in-hospital mortality and 13% stroke rate. Permanent spinal cord ischemia occurred in 1.8% of patients. Renal failure requiring dialysis occurred in 8% of patients. Among elective patients, the in-hospital mortality rate was 3.5%, while the stroke rate was 12%.
In a systematic review that compared hybrid FET with traditional open arch repair, FET was associated with lower mortality (7.7% vs 14.5%, odds ratio [OR] 0.55) and equivalent stroke rate (6.5% vs 9.7%). 35 The Achilles’ heel of the FET technique is the higher spinal cord ischemia rate given the more extended coverage (5.0% vs 2.6%, OR 2.20). This can be mitigated by using shorter stents and setting the arch anastomosis more proximally (zone 2). 36
Endovascular Arch Grafts
Despite the growing success of endovascular TAAA, endovascular arch repair with branched and fenestrated grafts remains mostly investigational. The proximal aorta is notable for the extreme curvature across the arch, translational movement associated with cardiac motion, and significant size changes through the cardiac cycle. These hostile conditions increase the risk of device fracture, migration, and endoleaks, and have thus far made total endovascular approaches to the arch foreboding. Yet, several branch and fenestrated endograft systems have been specifically designed for the aortic arch (Fig. 4).
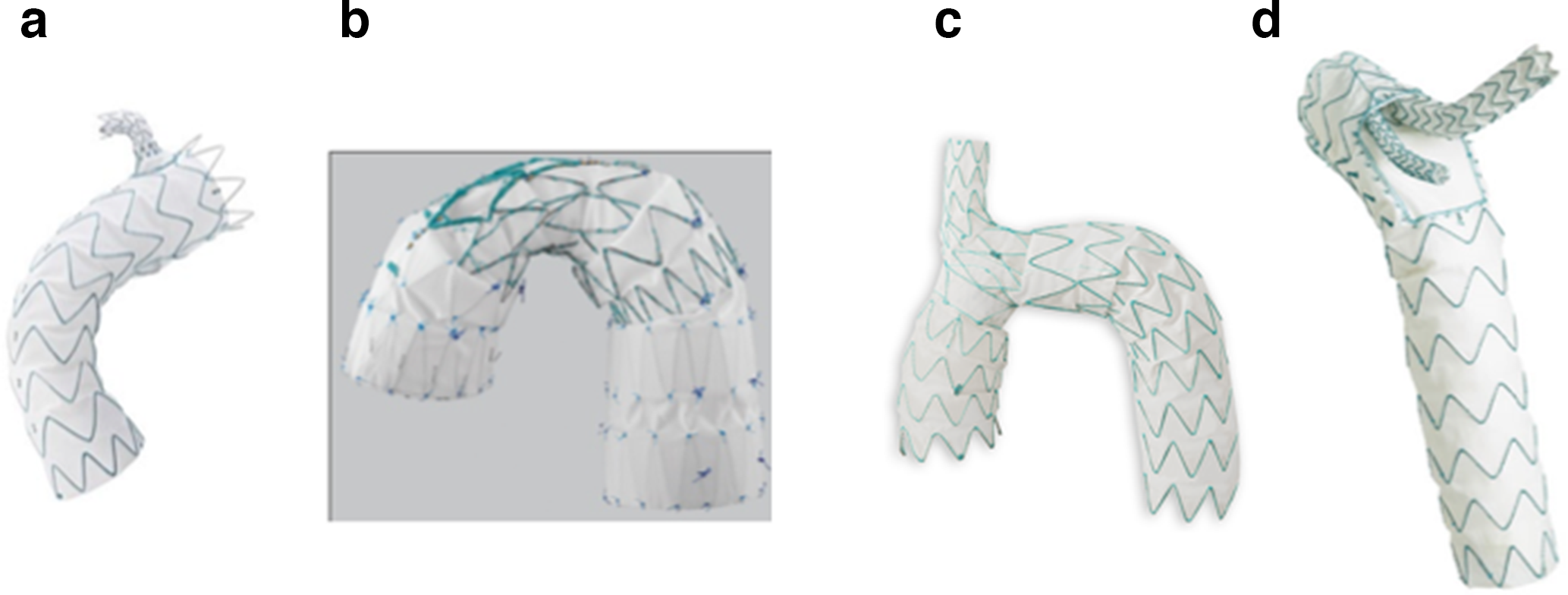
Selection of available endovascular arch devices. (a) Medtronic Valiant LSA branch thoracic device. (b) Cook arch branched stent graft. (c) Endospan NEXUS arch graft. (d) Terumo relay branch device.
The Valiant Mona LSA (Medtronic) system was designed for zone 2 deployment. It includes a main-body nitinol-supported polyester fabric graft and has a proximal bare stent and a single-side cuff with radiopaque markers. A 10 to 14 mm branch graft for the left subclavian artery then docks into this side cuff. Initial experience with 9 patients was reported. 37 Four of 9 patients developed endoleaks and 4 strokes occurred within 30 days.
Several devices are designed for zone 0 deployment. The A-branch custom-made arch endograft (Cook Medical, Bloomington, IN, USA) includes 2 internal branches and requires left subclavian artery revascularization. A 3-branch total endovascular design has recently been made available. Initial experience with the Cook custom-made devices for the arch was reported by Abraham and colleagues. 38 Of 6 high-risk patients, 2 suffered stroke, 1 developed a type 1 endoleak, and another had unsuccessful innominate branch cannulation. A global registry of 38 patients reported a 30-day mortality rate of 13%, technical success rate of 84%, and stroke in 15.8% of patients. 39 The delay in manufacturing of custom-made devices is a limitation for urgent cases.
The learning curve effect has been significant, but progress has been made in both technique and patient selection. Data from the multi-institutional registry on use of the A-branch in patients with chronic arch dissection post-type A dissection repair were recently published. 40 The results were tremendous; perioperative mortality was 2.9%, perioperative stroke rate was 2.9%, and there was no spinal cord ischemia. Avoiding degenerative atherosclerotic aneurysms and landing in surgical graft material contributed to the good results. The drawback was the high reintervention rates in the early and late periods. It should be noted that all centers involved in this study had to demonstrate tremendous experience with branched and fenestrated endograft repair of TAAA and some experience already with the A-branch device. Thus, whether wide adoption of this technique will be possible is unclear.
Successful use of the similar custom-made Relay (Bolton) system with 2 internal branches has also been reported. 41 There is a pre-curved self-orienting mechanism to the delivery system that allows for better positioning of the internal branches along the outer curve of the aorta. The branches are cannulated in a retrograde fashion and branch grafts deployed.
The NEXUS (Endospan) modular arch endograft system is approved for investigational use. It uses a through-and-through wire from the femoral artery to the right axillary to deliver the main body. This positions the brachiocephalic branch and it is the ascending aorta module that is then delivered to seal off the aneurysm. Left subclavian artery revascularization is necessary. The left carotid artery may be debranched off the right carotid artery, or an additional branch graft may be docked to the main body.
Future Directions
We are currently in the development phase of arch stent-graft technologies. Stroke, endoleaks, and anatomical inflexibility remain significant hurdles. Nevertheless, in Brazil, the first-in-human endo-Bentall has now been reported. 42 The aortic annulus, which has been the main fixation point for transcatheter aortic valve prostheses, appears to offer more stability than the ascending aorta. However, overcoming the increased forces on the aortic root and ascending aorta, along with the challenge of maintaining coronary flow remain daunting challenges. Improvements in stent-graft design will likely improve the conformability to unique aortic arch shapes and reduce rates of significant bird-break formation. Real-time customizable stent-graft technology could potentially allow patient-specific arch branch cannulations without manufacturing delays. Widespread use of computed tomography fusion imaging protocols could allow more accurate graft deployment, minimize arch manipulation, while reducing radiation to the implanting team.
Hybrid arch/FET repair will also likely evolve further. We look forward to anastomotic technologies to shorten circulatory arrest times further by facilitating quick and hemostatic arch and head vessel anastomoses. Intraoperative imaging such as angioscopy, and real-time adaption of the FET can optimize distal seal and reduce spinal cord ischemia.
In adopting these newer technologies, patient safety must remain the guiding principle. Many centers report outstanding results with hybrid arch/FET techniques and it is against this bar that novel approaches must be compared. Meanwhile, hybrid arch repair techniques have become commonplace and familiarity with the gamut of hybrid options is a must for all current specialized aortic surgeons.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Michael WA Chu: Speakers honoraria from Medtronic, Edwards Lifesciences, Boston Scientific, Abbott Vascular, Terumo Aortic. Maral Ouzounian: consulting agreement with Medtronic Inc, Ascyrus Medical, Gore Medical.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.