
Abstract
Objective
There is an increasing amount of evidence supporting use of transcatheter aortic valve replacement (TAVR) for treatment of aortic stenosis in patients at low or intermediate risk for surgical aortic valve replacement (SAVR). TAVR is now approved for use in all patient cohorts. Despite this, there remains debate about the relative efficacy of TAVR compared with SAVR in lower-risk cohorts and various subgroups of patients. We performed a systematic review and meta-analysis of randomized controlled trials (RCTs) and propensity-matched trials to guide a consensus among expert cardiologists and surgeons.
Methods
Studies comparing TAVR and SAVR in low- and intermediate-risk patients were identified by a thorough search of the major databases. Mortality, stroke, and other perioperative outcomes were assessed at 30 days and 1 year.
Results
Early mortality was lower in TAVR compared to SAVR in RCTs, but not propensity-matched studies in low-risk cohorts (0.66% vs 1.5%; odds ratio [OR] = 0.44, 95% confidence interval [CI] 0.20 to 0.98, I2 = 0%). No difference in mortality between TAVR and SAVR was identified in intermediate-risk patients at early or later time points. Incidence of perioperative stroke in 3 low-risk RCTs was significantly lower in TAVR (0.4%) than SAVR (1.4%; OR = 0.33, 95% CI 0.13 to 0.81, I2 = 0%). There was no difference in stroke for intermediate-risk patients between TAVR and SAVR. The expert panel of cardiologists and cardiac surgeons provided recommendations for TAVR and SAVR in various clinical scenarios.
Conclusions
In RCTs comparing TAVR and SAVR in low-risk patients, early mortality and stroke were lower in TAVR, but did not differ at 1 year. There was no difference in mortality and stroke in intermediate-risk patients. The Multidisciplinary Heart Team must consider individual patient characteristics and preferences when recommending TAVR or SAVR. The decision must consider the long-term management of each patient’s aortic valve disease.
Keywords
Introduction
Transcatheter aortic valve replacement (TAVR) has become an established treatment option for patients with significant risk for surgical aortic valve replacement (SAVR) for severe aortic stenosis (AS). While some randomized trials have shown lower early and 1-year mortality and stroke for TAVR compared to SAVR in high-, intermediate- and low-risk patients, others have shown no difference in these 2 most important outcomes. 1 -6 Consistently, mortality and stroke have in large part been better with TAVR in early time points; however, they are similar between TAVR and SAVR at 5 years. Transcatheter valve replacement has led to a few other potential early benefits compared to SAVR, including lower rates of new postoperative atrial fibrillation, acute kidney injury (AKI), bleeding, and resource utilization (other than the cost of the device). However, TAVR has had higher rates of permanent pacemaker (PPM) implantation and left bundle branch block for certain prosthesis (mainly mechanical and self-expanding [SE]) and higher rates of mild or greater paravalvular regurgitation (PVR) compared to surgery. The impact of these complications in younger patients and patients with life expectancy longer than a decade remains to be seen and active and accurate follow-up investigation is required.
Three randomized trials have compared TAVR with SAVR in generally elderly low-risk patients. 7 -9 Two recently published trials included patients with mean ages of 73 and 74 years with follow-up to 1 year. 8,9 These trials demonstrated excellent results for both treatments, but lower rates of the composite of death and disabling stroke in TAVR at 30 days. Compared to SAVR, balloon-expandable (BE) valves had a significantly lower composite endpoint of mortality, stroke, and rehospitalization at 1 year, while the SE valve was noninferior for the composite rates of death and disabling strokes at 2 years using a Bayesian analysis. Recovery was initially faster after TAVR, but the quality of life did not differ at 12 months. SE valves required more pacemakers and both SE and BE valves had a greater degree of mild PVR compared with SAVR. While patients undergoing surgery had better hemodynamics compared to TAVR in BE valves, this was the opposite for the SE valves.
In the United States, TAVR has been approved for use in extreme-, high-, intermediate-, and now low-risk patients as assessed by a multidisciplinary heart team, while worldwide, there remains a discrepancy between approval categories. For instance, in Japan, TAVR is only approved for high-risk patients (as compared to those “non high risk”), while in Germany, it is approved for all risk categories. With the approval of low-risk patients in the United States in August 2019 by the Food and Drug Administration, an entirely new patient population of patients with severe AS will be offered TAVR. Currently, in the United States, low-risk patients (as determined by the Society of Thoracic Surgeons [STS] predicted risk score) compromised ~80% of those undergoing SAVR. 10
There remains a discussion on the comparative outcomes between TAVR and SAVR for intermediate- and low-risk patients. Therefore, we performed a systematic review of all available randomized controlled trials (RCTs) and propensity-matched (PM) studies, including intermediate- and low-risk patients to determine whether an advantage exists between TAVR and SAVR. We used this meta-analysis to guide clinical scenarios from a group of expert cardiologists and cardiac surgeons.
Methods
A literature search was undertaken in May 2019 to locate each study that compared TAVR and SAVR within low-risk and/or intermediate-risk patients and crossed with 3 co-authors (VHT, JJE, SDH). The search terms
Evaluated Study Characteristics.
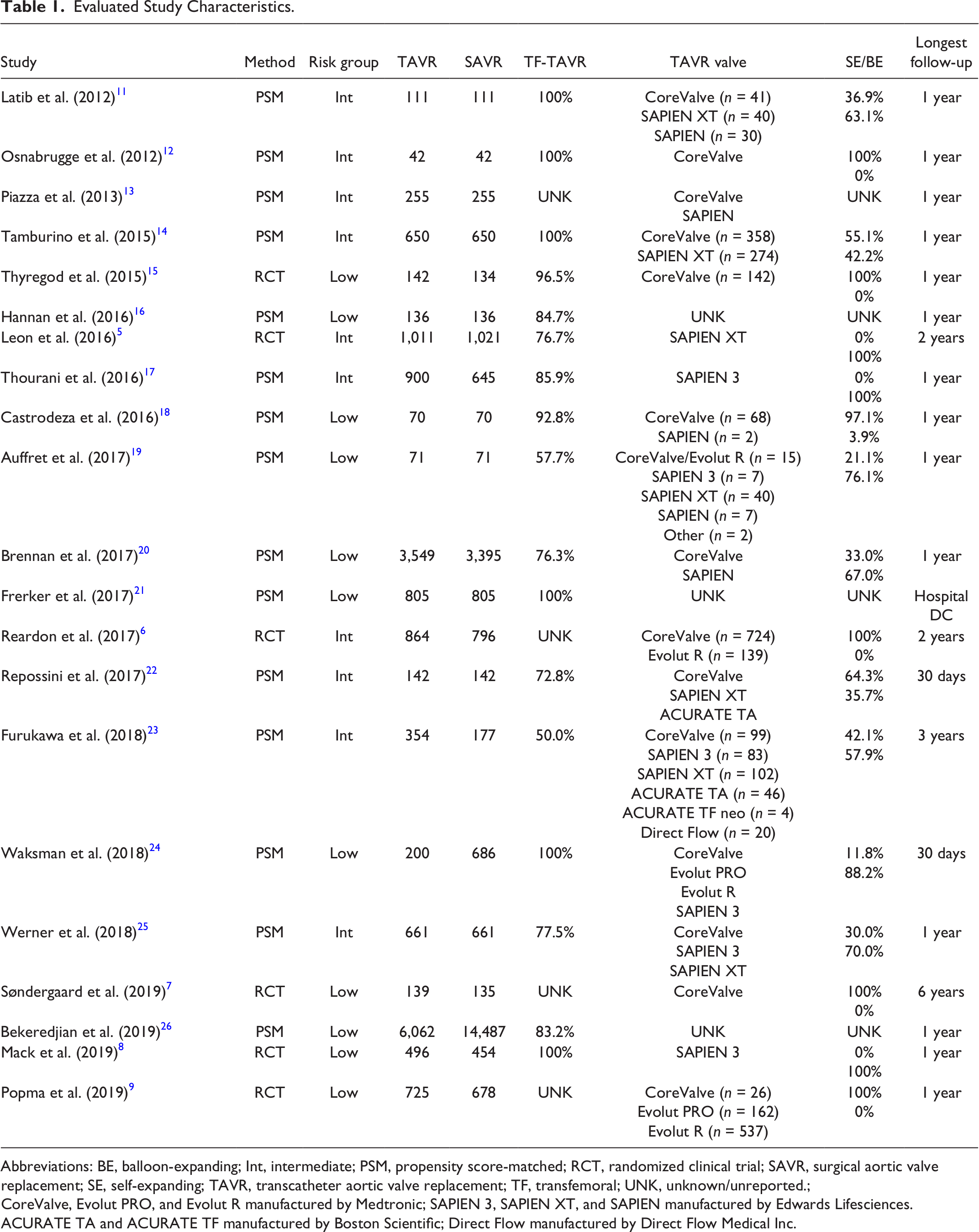
Abbreviations: BE, balloon-expanding; Int, intermediate; PSM, propensity score-matched; RCT, randomized clinical trial; SAVR, surgical aortic valve replacement; SE, self-expanding; TAVR, transcatheter aortic valve replacement; TF, transfemoral; UNK, unknown/unreported.;
CoreValve, Evolut PRO, and Evolut R manufactured by Medtronic; SAPIEN 3, SAPIEN XT, and SAPIEN manufactured by Edwards Lifesciences.
ACURATE TA and ACURATE TF manufactured by Boston Scientific; Direct Flow manufactured by Direct Flow Medical Inc.
All-cause mortality was assessed at 30-day (16 studies), 1-year (15 studies), and long-term (>1 year; 4 studies) time points. Stroke was analyzed separately for disabling strokes and all neurological events, both perioperatively (13 and 8 studies, respectively) and during follow-up (9 and 6 studies, respectively). Vascular complications, both major (12 studies) and minor (3 studies), were assessed in the perioperative period. New PPM implantation and aortic valve (AV) reintervention were examined as perioperative complications (15 and 7 studies, respectively), and during follow-up (5 and 6 studies, respectively). Mild aortic regurgitation and moderate-severe regurgitation were assessed both within 30 days (6 and 9 studies, respectively) and during follow-up (5 and 6 studies, respectively). The AV mean gradient as a continuous measure was assessed within 30 days (8 studies) and during follow-up (5 studies). Perioperative AKI was defined using the Valve Academic Research Consortium (VARC)-2 criteria stage 2 to 3 (9 studies) and AKI requiring transient or permanent dialysis (4 studies). 27 Major bleeding (or greater severity) and new or worsening atrial fibrillation were examined as perioperative complications (11 and 7 studies, respectively) and during follow-up (3 and 4 studies, respectively). Unless otherwise noted (i.e., mortality), perioperative outcomes included any studies with the relevant events during hospital admission and follow-up outcomes included any studies with the relevant event reported beyond 30 days. There were some instances when perioperative outcomes were reported within 30 days of surgery even after hospital discharge while others were reported within the hospital admission. For example, 6 studies reported in-hospital disabling stroke, whereas 7 studies reported a 30-day incidence. The longest follow-up included for each study was primarily at 1 year after surgery (Table 1). When a single study reported events at multiple long-term time points, the incidence at the longest follow-up time point was used in meta-analyses.
Data were extracted from each study for the applicable outcomes and entered into Review Manager Version 5.3 for meta-analysis. 28 Random effects models and 95% confidence intervals were used for all outcomes. All outcomes, except for mean AV gradient, were dichotomous variables presented as an odds ratio (OR) obtained using the Mantel–Haenszel statistical method. Results for AV gradient are presented as mean differences and used the Inverse Variance statistical method. Forest plots were constructed for each research question and funnel plots to examine publication bias were constructed for 30-day mortality, 30-day disabling stroke, follow-up moderate-severe aortic regurgitation, and follow-up AV mean gradient. For mortality and stroke, which were reported in the greatest number of studies, analyses were conducted separately for low versus intermediate risk and RCT versus PM methodology. Studies with both low- and intermediate-risk patients were grouped into the low-risk subgroup for analyses. Data for baseline characteristics of the 2 groups were extracted when available for PM groups and from the full RCT samples and were compared using the same meta-analytic strategy as the primary outcome variables described above.
Results
Results of the literature search strategy are shown in the Supplemental Figure. Twenty-one studies, including 39,795 patients (TAVR = 15,789, SAVR = 24,006), fulfilled the search criteria and were included in the analysis (Table 1). Baseline characteristics of the TAVR and SAVR groups were comparable (Supplemental Table), including age, gender, risk scores, and preoperative comorbidities.
Intermediate-risk patients had a mean age of 80.8 years for TAVR and 80.6 years for SAVR, while the low-risk patients had a mean age of 75.5 years for TAVR and 74.6 years for SAVR. Mean STS Predicted Risk of Mortality score for TAVR and SAVR patients was 5.3% and 5.3% for the intermediate-risk group and 2.2% and 2.1% for the low-risk group, respectively.
Mortality
For 3,692 intermediate-risk patients (TAVR n = 1,875 and SAVR n = 1,817) in 2 RCTs, there was no difference in operative mortality between TAVR and SAVR (3.0% vs 2.8%; OR = 1.10, 95% CI 0.71 to 1.71, I 2 = 14%; Fig. 1). Similarly, in 2,931 intermediate-risk patients (TAVR n = 1,554 and SAVR n = 1,377) included in PM studies, TAVR mortality at 30 days (4.1%) did not differ from SAVR mortality (3.9%; OR = 1.08, 95% CI 0.74 to 1.58, I 2 = 0%). The incidence of operative mortality in the 3 low-risk RCTs, including 2,629 patients (TAVR n = 1,363 and SAVR n = 1,266), was significantly lower in TAVR (0.66%) compared with SAVR (1.5%; OR = 0.44, 95% CI 0.20 to 0.98, I 2 = 0%). In contrast, in 23,327 low-risk patients included in PM studies (TAVR n = 7,208 and SAVR n = 16,119), TAVR mortality (1.9%) did not differ from SAVR mortality (2.8%; OR = 0.75, 95% CI 0.49 to 1.15, I 2 = 14%).
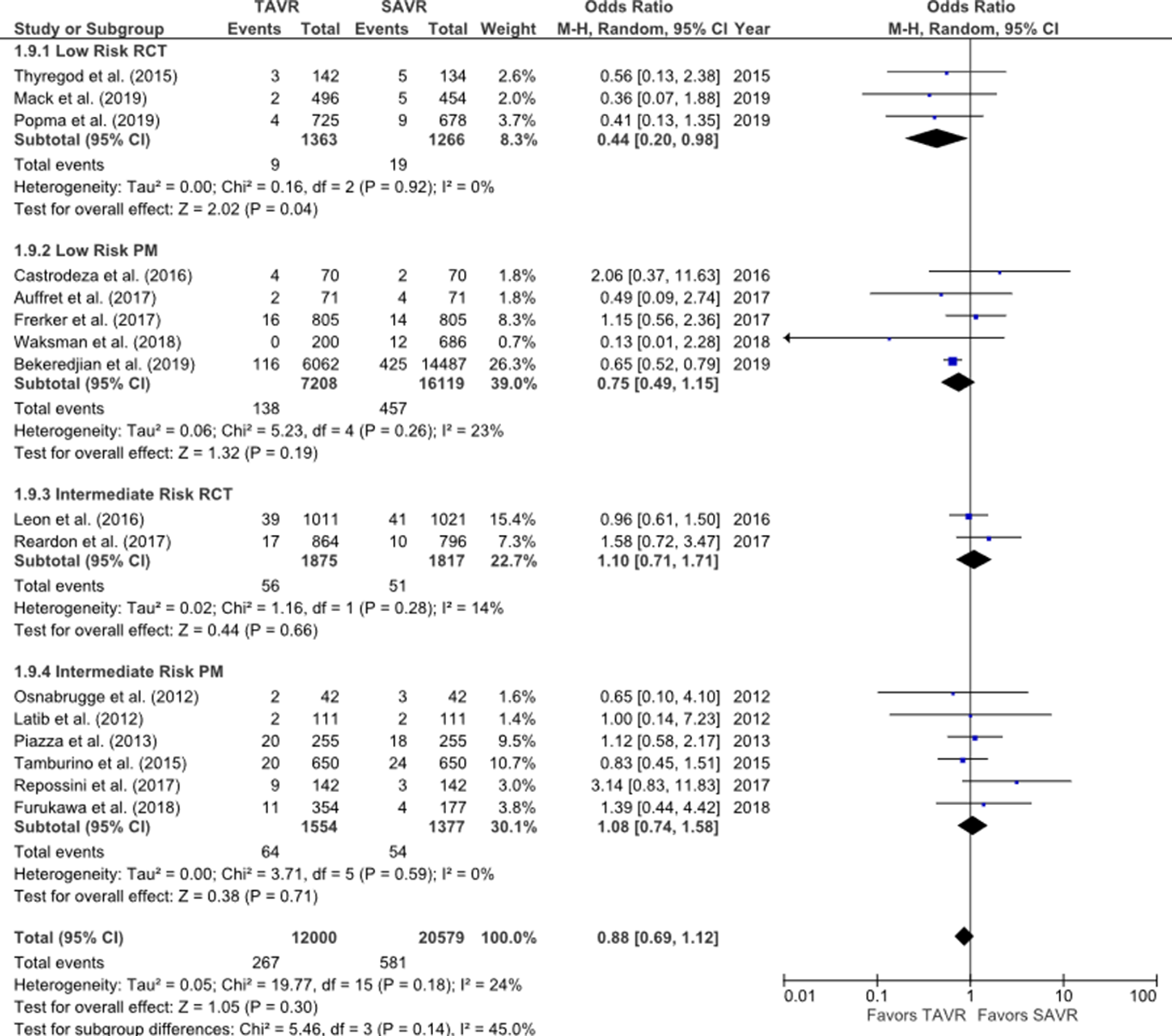
Forest plot for 30-day mortality by risk group and study type.
There was no difference in the 2 RCTs reporting 1-year mortality in intermediate-risk patients (TAVR 9.8% vs SAVR 9.8%, OR = 1.01, 95% CI 0.81 to 1.26, I 2 = 0%; Fig. 2). Similarly, in 6 PM studies for intermediate-risk patients, TAVR mortality (13.8%) did not differ from SAVR mortality (12.7%; OR = 1.10, 95% CI 0.90 to 1.34, I 2 = 0%). In 3 RCTs reporting 1-year mortality in low-risk patients, there was no difference between TAVR (2.1%) and SAVR (3.2%; OR = 0.66, 95% CI 0.40 to 1.07, I 2 = 0%). In 28,047 low-risk patients included in the PM studies, TAVR mortality (11.4%) was higher than SAVR (9.7%; OR = 1.11, 95% CI 1.03 to 1.21, I 2 = 0%). Of note, mortality rates at 1 year for the RCTs for both TAVR and SAVR were dramatically lower than for the PM, questioning the low-risk nature of patients in the PM trials. Moreover, in the nonrandomized studies, the operators decided without randomization that the patient should undergo TAVR or SAVR, potentially leading to significant selection bias in the PM studies.
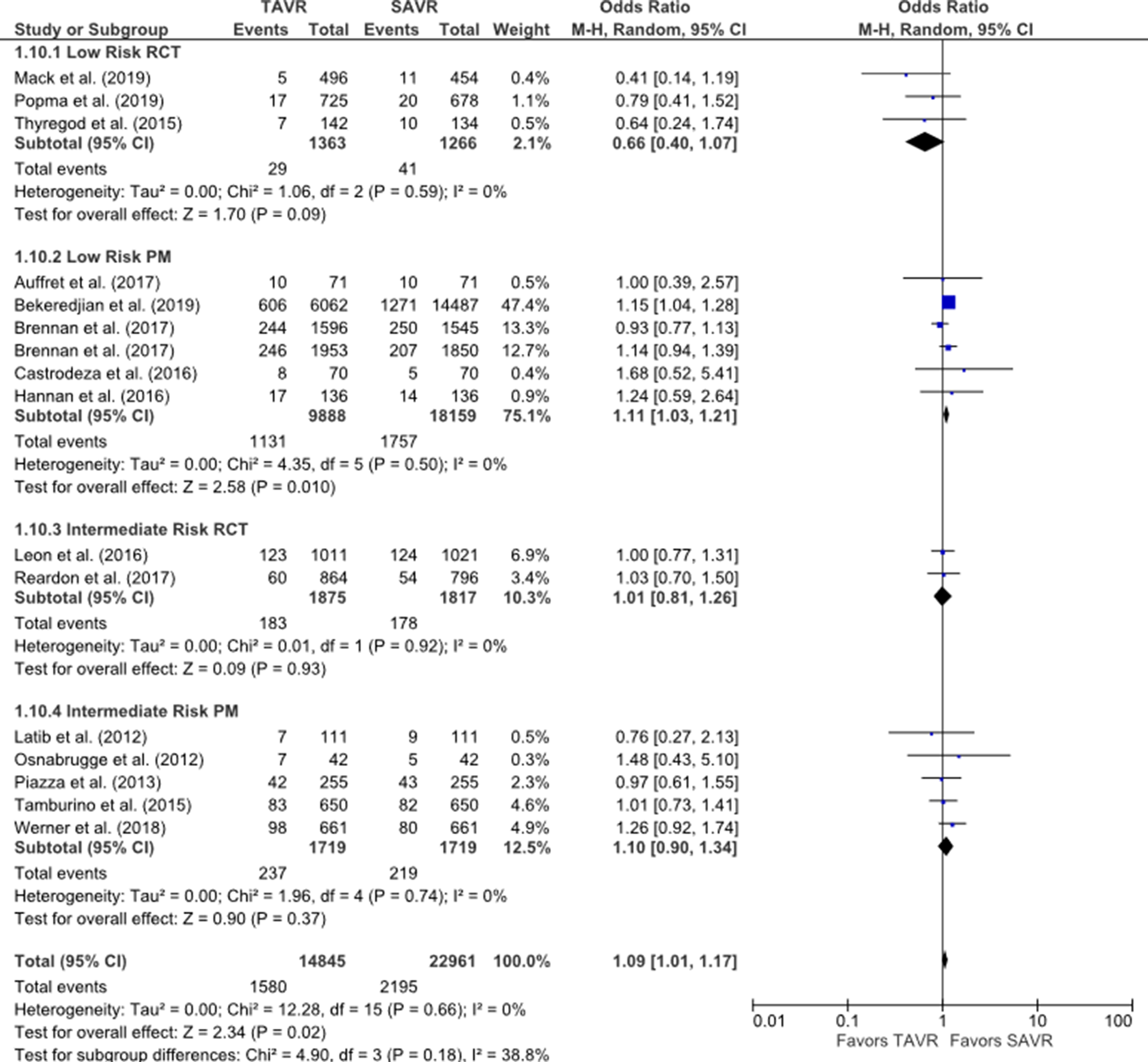
Forest plot for 1-year mortality by risk group and study type.
Stroke
In 2 RCTs of intermediate-risk patients, the rate of stroke in TAVR (2.2%) trended lower than SAVR (3.3%; OR = 0.67, 95% CI 0.45 to 1.00, I 2 = 0%; Fig. 3). There was no difference in stroke rates for intermediate-risk patients in PM between TAVR (1.6%) and SAVR (1.9%; OR = 0.88, 95% CI 0.45 to 1.72, I 2 = 2%). The incidence of perioperative stroke in 3 low-risk RCTs was significantly lower in TAVR (0.4%) than SAVR (1.4%; OR = 0.33, 95% CI 0.13 to 0.81, I 2 = 0%). There was no difference in the rate of stroke in PM studies including low-risk patients (OR = 0.55, 95% CI 0.12 to 2.12, I 2 = 0%).
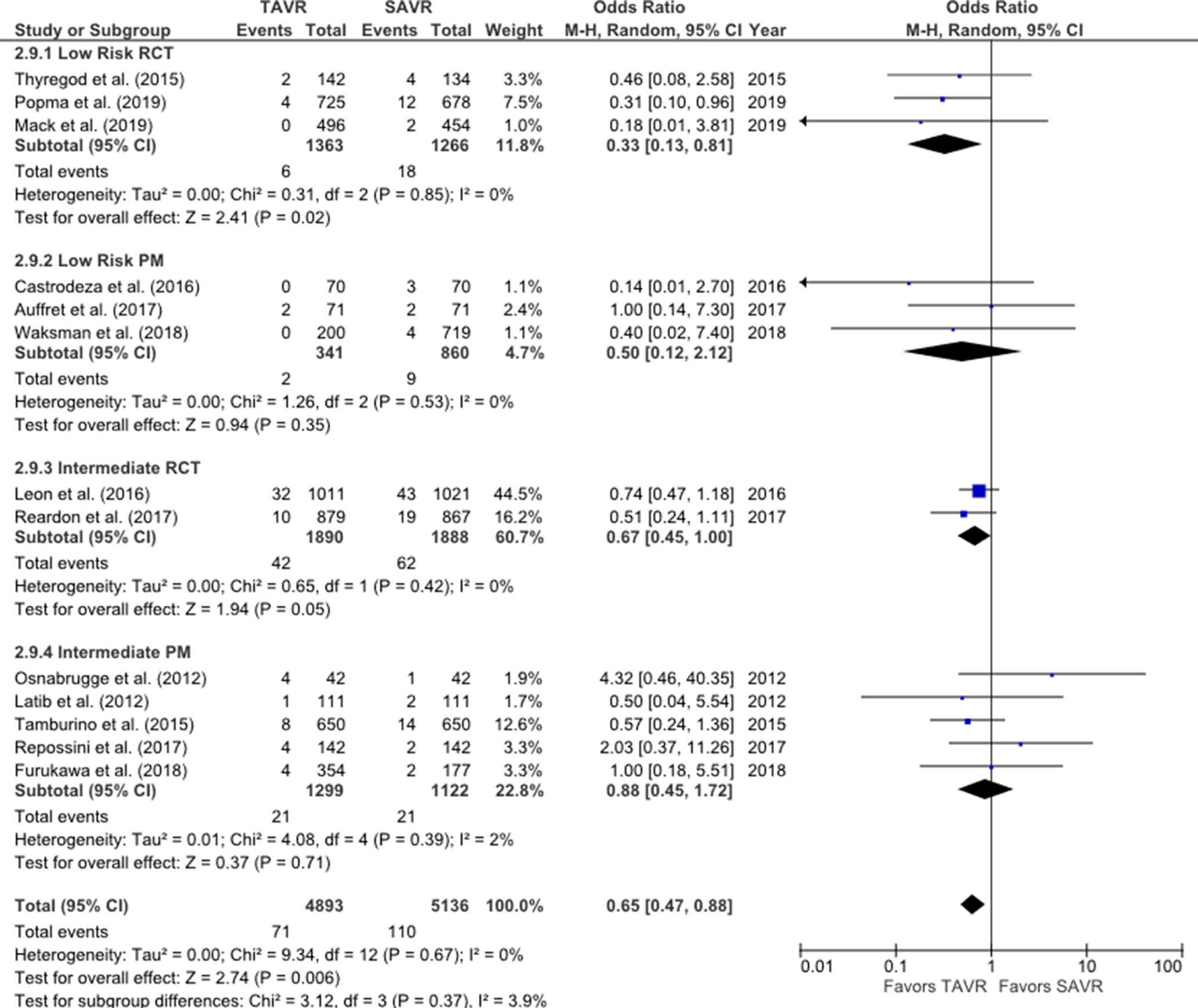
Forest plot for perioperative stroke by risk group and study type.
Procedural Complications
Meta-analysis was performed on other procedural complications, including vascular complications, need for a new PPM, perioperative AKI, and new atrial fibrillation. Heterogeneity of data for each complication was too high (>60%) to permit interpretation of the results allocated separately within randomized or PM studies. Moderate-severe aortic regurgitation data were available in 9 studies within 30 days (N = 28,147). Greater than moderate aortic regurgitation was higher in TAVR (3.8%) compared with SAVR (0.5%; OR = 6.45, 95% CI 5.13 to 8.12, I 2 = 0%).
Assessment of Bias
Since 1 study accounted for a large portion of sample size in the PM analysis, 26 we undertook sensitivity analyses on each of the outcomes by removing this study. Analyses of 1-year mortality in the low-risk PM group, after removal of the study by Bekeredijan et al., 26 found that the lower 1-year mortality in the surgical group became nonsignificant. This finding may suggest that those in the SAVR arm of that study were actually at lower risk than those in the TAVR arm despite attempts at matching. It should be noted that the point estimates for the majority of the remaining low-risk PM studies were in the same direction as the excluded study.
Expert Consensus Opinion in Areas of Uncertainty
The ISMICS TAVR/SAVR Committee, consisting of cardiac surgeons and interventional cardiologists, formed a Multidisciplinary Heart Team to form a consensus in the areas of uncertainty, which are summarized in Table 2.
Multidisciplinary Heart Team Consensus in Areas of Uncertainty.
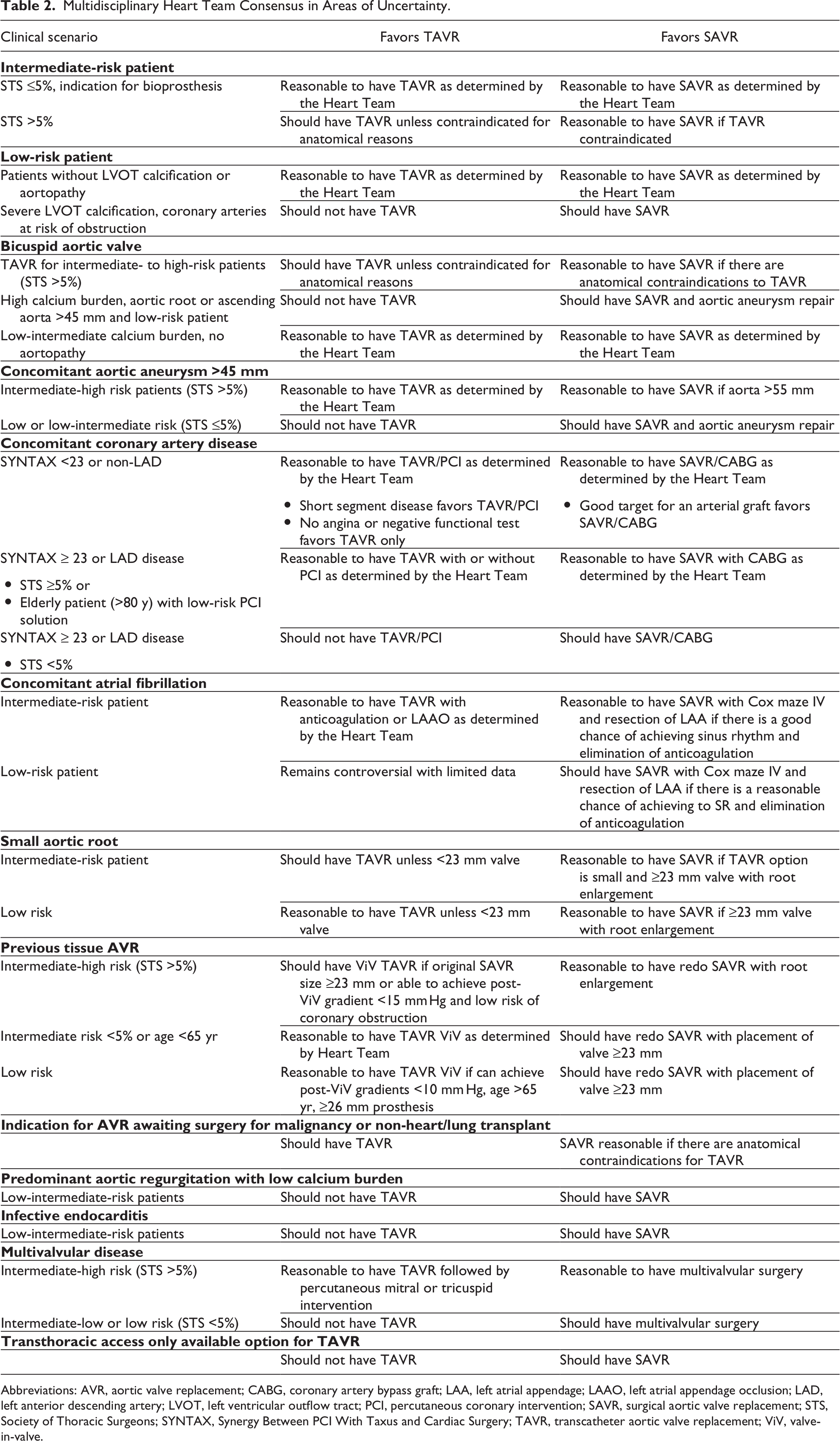
Abbreviations: AVR, aortic valve replacement; CABG, coronary artery bypass graft; LAA, left atrial appendage; LAAO, left atrial appendage occlusion; LAD, left anterior descending artery; LVOT, left ventricular outflow tract; PCI, percutaneous coronary intervention; SAVR, surgical aortic valve replacement; STS, Society of Thoracic Surgeons; SYNTAX, Synergy Between PCI With Taxus and Cardiac Surgery; TAVR, transcatheter aortic valve replacement; ViV, valve-in-valve.
Discussion
In this meta-analysis comparing TAVR and SAVR in low- and intermediate-risk patients, 30-day mortality in RCTs was lower in TAVR patients, but did not differ in intermediate-risk patients. There was no difference in either group in studies with PM outcomes at 30 days. The incidence of 30-day stroke was lower after TAVR in RCTs, but did not differ in the PM analyses. One-year mortality was similar for TAVR and SAVR patients in the RCTs, but was higher in TAVR in the PM studies. After removal of the GARY PM study by Bekeredijan et al., 26 the lower 1-year mortality in the surgical group became nonsignificant. There was no difference in 1-year mortality for the intermediate-risk studies in the RCT or PM studies. Furthermore, there was no difference between TAVR and SAVR on incidence of stroke at 1 year. These results are similar to other recently published meta-analyses. 29 -32 From our analysis, we note the tremendous advances to the treatment of AS with the advent of TAVR. The similar outcomes of TAVR and SAVR at 5 years in data from 2 randomized trials of low- and intermediate-risk patients is reassuring for the efficacy of TAVR in mid-term follow-up. 33,34 However, in these younger patient cohorts, long-term follow-up is necessary and maintenance of a dedicated multidisciplinary valve team is required for the lifetime management of these complex patients.
Mortality
Early mortality has generally always favored less invasive transcatheter techniques compared to traditional surgical approaches. Similarly, 30-day mortality in RCTs was lowest in the TAVR group compared to SAVR in low-risk patients (PARTNER 3 study: TAVR 0.4% and surgery 1.1%; CoreValve LR study: TAVR 0.5% and surgery 0.8%). 8,9 Interestingly, early mortality in intermediate-risk patients did not follow these patterns. In the SURTAVI trial using the CoreValve prosthesis, all-cause mortality was lower in the surgery group (1.3% vs 2.0%), while in the PARTNER 2A trial with the SAPIEN XT prosthesis, surgery had a higher early mortality (4.0% vs 3.4%). 1,6 The reason for this difference in low-risk, but not intermediate-risk groups is unclear. It is plausible that in the low-risk RCTs, TAVR utilized the most recent TAVR valves (SAPIEN3 in the PARTNER 3 study and the majority Evolut R in the Evolut LR trial), which are associated with lower rates of complications. 17 Increased operator experience and better sizing using computed tomography (CT; rather than transthoracic echocardiogram) may also be a contributing factor in favor of TAVR.
At 1-year, all-cause mortality in low-risk patients was not significantly different between TAVR and SAVR in the RCTs, but was higher with the addition of the PM registries. There remain differences between RCTs for 1-year mortality. In the PARTNER 3 trial, there was a significantly lower 1-year mortality in the TAVR group compared to surgery (1.0% vs 2.5%), while in the CoreValve LR trial, there was no difference (TAVR: 2.4% vs surgery: 2.9%). 8,9 In the PARTNER 2 intermediate-risk RCT, death from any cause was 11.8% in TAVR and 13.0% in surgery. 5 While in the SURTAVI trial, TAVR had a mortality of 7.0% compared to surgery at 6.8%. 6 No randomized trials have demonstrated a survival advantage for SAVR at any time point, but longer follow-up is limited to high-risk patients, 1 intermediate-risk and 1 low-risk trial. 3,4,33,34 The NOTION trial has reported outcomes beyond 5 years in low-risk patients. 33 It found no difference in its primary outcome of the composite of mortality, stroke, or myocardial infarction at 5 years nor in cardiovascular mortality. The PARTNER 2 RCT of intermediate-risk patients reported no significant difference in mortality and stroke at 5 years (5-year mortality TAVR 47.9% vs SAVR 43.4%, P = 0.21). However, in the transthoracic cohort, the 5-year mortality was lower in SAVR patients. 34 In PM studies, there is a major concern that a selection bias may account for the survival advantage in SAVR since poor prognostic factors such as frailty may not have been accounted for in matching.
Stroke
One of the most devastating complications after TAVR or SAVR remains a stroke. While the incidence of stroke after SAVR has remained stable over time, the rate of stroke following TAVR has dramatically improved. In earlier studies comparing TAVR and SAVR in high-risk patients, there was a significantly higher stroke rate in those undergoing TAVR. 35 With improvements in valve technology, less frequent need for pre-TAVR balloon valvuloplasty and post-deployment dilation, and higher incidence of transfemoral access, the stroke rates for TAVR have significantly improved. 36,37 The rate of stroke in the recently reported RCTs in low-risk patients was similarly low in both SAVR and TAVR, but favored TAVR. 8,9 It is important to note that very low numbers of neuroprotection devices were used in any of the low- or intermediate-risk RCTs for the SAVR or TAVR procedures. However, there is a possibility that some adjunct neuroprotective devices were used in the TAVR patients of the PM studies. A mechanism for strokes following TAVR or SAVR has been linked to bioprosthetic leaflet thrombosis. The RESOLVE and SAVORY registries, each representing cases from a single center, reported a relatively common rate of reduced leaflet motion after TAVR (13%) and SAVR (4%), from multidetector CT performed at median 83 days postoperatively. 38 Subclinical leaflet thrombosis, defined as reduced leaflet motion with hypoattenuating lesions on CT, was associated with an increased rate of transient ischemic attacks, but not stroke. The relationship with leaflet thrombosis at longer-term follow-up is under active investigation. 39,40 The role of anticoagulation following SAVR or TAVR remains unclear and requires careful evaluation.
Paravalvular Regurgitation
The rate of paravalvular aortic regurgitation has significantly been lower after SAVR than TAVR. While the rate of moderate or severe AR was low after TAVR (3.8%), it was more than 6 times more frequent than after SAVR. Moderate or greater AR has been consistently associated with a higher rate of mortality at follow-up. 3,5 At 2 years in the PARTNER 2 trial, patients with moderate or greater AR at 30 days had nearly 3 times greater mortality than those with mild or less. 5 In this meta-analysis, nearly 33% of patients who underwent TAVR, yet only 8.5% after SAVR, had mild AR at 30 days. Historically, mild AR was associated with increased mortality in high-risk patients at 5-year follow-up in 2 RCTs, and in a meta-analysis, 3,4,41 but this may be due to the lack of appropriate echocardiography standards during that study time period. Mild AR did not influence mortality or rehospitalization in secondary analyses of RCTs in intermediate-risk patients at 2 years. 5,6 While the natural history of mild AR of the native AV is benign, the influence of mild paravalvular prosthetic AR on mortality in younger, low-risk patients who have greater life-expectancy is unclear and will require longer follow-up of existing studies. 42
Other Outcomes
Heterogeneity in procedural complications associated with TAVR and SAVR may be a result of improving outcomes over time. For example, the rate of PPM and moderate or greater aortic regurgitation in the intermediate-risk trial (8.5% to 25.9% and 3.7% to 5.3%, respectively) improved in the low-risk trials (6.6% to 17.4% and 0.8% to 3.5%, respectively). 5,6,8,9 While the pattern of these short-term complications has been well documented, the long-term impact of them, however, remains unclear. After TAVR, the need for PPM has been associated with an increase in heart failure rehospitalization but not mortality; but no data are available with follow-up beyond 5 years. 43,44 Furthermore, there remain stark differences in pacemaker rates in those undergoing BE, SE, or mechanically expandable TAVR prosthesis. The effect of pacemakers in younger patients undergoing TAVR remains unknown. It has been documented that pacing-induced cardiomyopathy is related to pacing burden and can be as high as 40%. 45 The consequences for younger patients and need for pacemaker are unknown and may lead to significant clinical ramifications.
Areas of Uncertainty and Consensus Discussion
The mean age of patients treated in this meta-analysis was 75 years in the low-risk group and 81 years in the intermediate-risk group. The RCTs including low-risk patients had mean age of ~73 to 79 years. 8,9,33 The Society recommends that a more robust conversation with a Heart Team is needed when offering a TAVR to young patients (≤65 years) who may require a repeat valve procedure in the future, and in whom it is likely beneficial to avoid PPM and PVR. In the current low-risk trials, there were very few patients (<10%) who were under the age of 65 years. Very young patients (≤50 years) eligible for a mechanical prosthesis should have SAVR. When performing SAVR, effort should be made (including root enlargement or replacing procedures) to place a valve of size large enough to prevent prosthesis–patient mismatch and (if a bioprosthesis is placed) to prepare for valve-in-valve (ViV) TAVR. There is little short or long-term data on the use of TAVR in patients younger than 70, who can be expected to outlive a bioprostheses, and no data for the outcomes of surgical explant of TAVR valves. Only limited data are available for TAVR-in-TAVR procedures, but the procedure appears to be relatively safe. 46 Data for TAVR ViV (TAVR-in-SAVR) procedures are accumulating, and ViV appears to be safer than redo-SAVR in matched registry data; the long-term results are not clear. 47 -49
The major randomized trials comparing TAVR and SAVR have excluded patients with bicuspid aortic valve disease (BAV). Patients with BAV typically present with aortic valve disease at a younger age and commonly have an associated aortopathy that may benefit from prophylactic replacement. Asymmetry of both the annulus and calcified valve leaflets (which varies by Sievers classification type) theoretically makes placement of a TAVR valve more challenging than in a tricuspid valve. However, data are accumulating on the use of TAVR in patients with BAV. Current-generation BE TAVR valves in select patients with BAV are associated with similar mortality (30-day and 1-year), PVR, and gradients compared with tricuspid valves; but stroke was higher in the BAV group. 50 The STS/American College of Cardiology Transcatheter Valve Therapy Registry found a small decrease in device success, with increase in PVR (4.7% vs 3.5%) in patients undergoing TAVR for BAV compared to tricuspid aortic valves. 51 We encourage a randomized trial comparing TAVR or SAVR to determine the best treatment algorithm for those with BAV stenosis.
There are no adjudicated core laboratory data beyond 5 years for the durability of TAVR valves. Available data do not show any concerning signals for early valvular degeneration, but include only elderly patients not expected to outlive their surgical prosthesis. 52 There are limitations also for the data of SAVR bioprosthesis durability, mainly a paucity of prospective, protocolized echocardiographic follow-up. The best durability data may emerge from the planned 10-year follow-up of the low- and intermediate-risk randomized trials comparing TAVR and SAVR.
The management of concomitant coronary artery disease (CAD) remains unclear; the rate of concomitant CABG in SAVR was twice as common as percutaneous coronary intervention (PCI) in TAVR in the low-risk randomized trials. In a retrospective cohort, the presence of concomitant CAD (SYNTAX >22) and incomplete revascularization (residual SYNTAX >8) were associated with higher mortality at 2-year follow-up, compared with patients with no residual (SYNTAX <8) or no CAD. 53 While this result most likely increased the perioperative risk of SAVR + CABG patients, further work is required to clarify the long-term influence of concomitant revascularization. There is similar concern about the ability to access the coronary arteries after the placement of TAVR valves. In the absence of data, the Consensus was to follow the published Guidelines for Myocardial Revascularization, which supports using the SYNTAX score and other anatomical features to guide a decision between PCI and CABG. 54,55
The key factors that impact on the choice of TAVR versus AVR for individual patients need to be understood and are in addition to the factor previously discussed of CAD stratified by SYNTAX score. The level of evidence comparing TAVR and SAVR is highest with the RCT, but patients were excluded who had contraindications for either form of AVR.
Additional factors influence the recommendation of SAVR versus TAVR and include patient-specific characteristics, often anatomical, and inherent differences between TAVR and SAVR. Left ventricular outflow track calcification has a small, but serious risk of annular rupture from BE TAVR and may increase the differential value of SAVR. Porcelain aorta leads to strong preference for TAVR. Small aortic annulus would create preference for SAVR with annular enlargement in a younger patient, but in an elderly patient with increased surgical risk would increase the value of TAVR with a supra-annular valve orifice. SAVR has the upper hand in low- and intermediate-risk patients with risk factors for TAVR-related acute coronary obstruction, that is, long and bulky leaflets, low takeoff of coronary ostia, and dimensions of the sinuses of Valsalva minimally greater than annular and sinotubular junction dimensions. On the other hand, an adjunctive technique reduces the risk of coronary obstruction from TAVR, specifically native leaflet laceration techniques.
The final factor in the SAVR versus TAVR discussion is patient preference that should be incorporated in the process of shared decision-making. While there is often a preference for the less burdensome form of AVR with more rapid recovery (i.e., TAVR), some patients may be influenced by uncertainties of remaining with TAVR (or SAVR) such as long-term leaflet durability, the emerging problem of early leaflet thickening from thrombus, and restricted valve opening requiring full anticoagulation. As previously mentioned, patients likely to “out-live their valve” have the additional issue of how their choice of valves for their first AVR may impact the second AVR. 56 While nearly one quarter of SAVR patients in the PARTNER 3 RCT were performed using minimally invasive techniques, to date there is no good quality evidence comparing minimally invasive SAVR with TAVR. 8 Minimally invasive SAVR, performed via upper hemisternotomy or right anterior thoracotomy, may reduce postoperative pain length of stay, and improve patient cosmesis compared to SAVR via median sternotomy, with similar rates of mortality and stroke. 57
Therefore, the SAVR versus TAVR comparison, in the broad sense, comes from the clinical trials as summarized in this review. The SAVR versus TAVR team recommendation for the individual patient, and the subsequent patient choice, has multiple dimensions. Discussions with some patients will need to go into these details with the caveat that new evidence may impact on these discussions. The heart team approach will take on a new importance in forming recommendations from a thorough review of important patient-specific factors followed by a discussion of SAVR and TAVR current data from trials. A similar multidisciplinary approach is needed for discussions with patients who must make an informed decision incorporating their preference, fears, and integration of pertinent areas of clinical uncertainty.
A myriad of patient scenarios has emerged and the 2017 Appropriate Use Criteria for the Treatment of Patients with Severe Aortic utilizes voting by leading clinicians of the SAVR versus TAVR choice, as well as palliative medical therapy and balloon valvuloplasty. 58 An update is needed for these guidelines with the dynamic nature of the field.
Limitations
This meta-analysis has a number of limitations. First, the study was not a patient-level meta-analysis, and the inclusion of PM studies with RCTs introduces the potential for selection bias. The randomized trials represent the highest level of science, but were performed in highly select sites, for which the outcomes may not be generalizable to other sites. Moreover, RCTs apply only to the population tested. For example, those with bicuspid valves or significant CAD were not allowed for participation in the trial leading to a 14.8% to 34% rejection rate by the case adjudication committees for the CoreValve Low Risk and PARTNER 3 trials, respectively. Similarly, the higher rate of concomitant procedures (e.g., CABG) with SAVR in the RCTs may have influenced perioperative outcomes. In the PM studies, concomitant CABG represented a small minority (<10%) of included patients.
Of course, the opposite is true in the PM studies where the operators selected which group to put the patient in likely leading to the SAVR having better-risk patients no matter how you attempt to match the patients. Therefore, a major shortcoming of PM trials is that there is no case review committee to reliably note the patient’s risk status. This leads the “low- and intermediate-risk” populations to possibly be a heterogenous group of patients in PM studies. Therefore, we have separated RCTs from PM studies to minimize this bias. Despite the large number of patients included in this analysis, there was a high degree of heterogeneity in some outcomes, which limits interpretation of the results—thus we chose to focus on only mortality and stroke, which had low levels of heterogeneity. To date, there are no reliable 10-year data available to satisfactorily assess the true efficacy of TAVR in low- and intermediate-risk patients. Finally, some data from presentations not included in this submission may highlight longer-term outcomes in intermediate-risk patients and 2-year outcomes in low-risk patients.
Conclusions
In RCTs comparing low-risk cohorts, early mortality was lower in TAVR compared to SAVR, but did not differ at 1 year. No difference in mortality between TAVR and SAVR was identified in intermediate-risk patients at early or later time points. The Society recommends that low-risk and intermediate-risk patients with severe, symptomatic AS be discussed by a multidisciplinary Heart Team, which includes (but is not limited to) interventional cardiologist, cardiac surgeon, an imaging specialist well versed in echocardiography and CT, valve team coordinators, and a noninvasive cardiologist. The decision of whether to offer TAVR or SAVR should be in consultation with the patient, who should have the opportunity to meet both a cardiologist and surgeon, preferably at the same visit. In the absence of more data to clarify areas of uncertainty, the Heart Team approach ensures a balanced discussion of the relative merits of each therapy and how they apply to an individual patient with emphasis on the long-term management of AS.
Supplemental Material
Figure S1 - Supplemental material for The International Society for Minimally Invasive Cardiothoracic Surgery Expert Consensus Statement on Transcatheter and Surgical Aortic Valve Replacement in Low- and Intermediate-Risk Patients: A Meta-Analysis of Randomized and Propensity-Matched Studies
Supplemental material, Figure S1, for The International Society for Minimally Invasive Cardiothoracic Surgery Expert Consensus Statement on Transcatheter and Surgical Aortic Valve Replacement in Low- and Intermediate-Risk Patients: A Meta-Analysis of Randomized and Propensity-Matched Studies by Vinod H. Thourani, J. James Edelman, Sari D. Holmes, Tom C. Nguyen, John Carroll, Michael J. Mack, Samir Kapadia, Gilbert H. L. Tang, Susheel Kodali, Tsuyoshi Kaneko, Christopher U. Meduri, Jessica Forcillo, Francis D. Ferdinand, Gregory Fontana, Piotr Suwalski, Bob Kiaii, Husam Balkhy, Joerg Kempfert, Anson Cheung, Michael A. Borger, Michael Reardon, Martin B. Leon, Jeffrey J. Popma and Niv Ad in Innovations: Technology and Techniques in Cardiothoracic and Vascular Surgery
Supplemental Material
Table S1 - Supplemental material for The International Society for Minimally Invasive Cardiothoracic Surgery Expert Consensus Statement on Transcatheter and Surgical Aortic Valve Replacement in Low- and Intermediate-Risk Patients: A Meta-Analysis of Randomized and Propensity-Matched Studies
Supplemental material, Table S1, for The International Society for Minimally Invasive Cardiothoracic Surgery Expert Consensus Statement on Transcatheter and Surgical Aortic Valve Replacement in Low- and Intermediate-Risk Patients: A Meta-Analysis of Randomized and Propensity-Matched Studies by Vinod H. Thourani, J. James Edelman, Sari D. Holmes, Tom C. Nguyen, John Carroll, Michael J. Mack, Samir Kapadia, Gilbert H. L. Tang, Susheel Kodali, Tsuyoshi Kaneko, Christopher U. Meduri, Jessica Forcillo, Francis D. Ferdinand, Gregory Fontana, Piotr Suwalski, Bob Kiaii, Husam Balkhy, Joerg Kempfert, Anson Cheung, Michael A. Borger, Michael Reardon, Martin B. Leon, Jeffrey J. Popma and Niv Ad in Innovations: Technology and Techniques in Cardiothoracic and Vascular Surgery
Supplemental Material
Presentation 1 - Supplemental material for The International Society for Minimally Invasive Cardiothoracic Surgery Expert Consensus Statement on Transcatheter and Surgical Aortic Valve Replacement in Low- and Intermediate-Risk Patients: A Meta-Analysis of Randomized and Propensity-Matched Studies
Supplemental material, Presentation 1, for The International Society for Minimally Invasive Cardiothoracic Surgery Expert Consensus Statement on Transcatheter and Surgical Aortic Valve Replacement in Low- and Intermediate-Risk Patients: A Meta-Analysis of Randomized and Propensity-Matched Studies by Vinod H. Thourani, J. James Edelman, Sari D. Holmes, Tom C. Nguyen, John Carroll, Michael J. Mack, Samir Kapadia, Gilbert H. L. Tang, Susheel Kodali, Tsuyoshi Kaneko, Christopher U. Meduri, Jessica Forcillo, Francis D. Ferdinand, Gregory Fontana, Piotr Suwalski, Bob Kiaii, Husam Balkhy, Joerg Kempfert, Anson Cheung, Michael A. Borger, Michael Reardon, Martin B. Leon, Jeffrey J. Popma and Niv Ad in Innovations: Technology and Techniques in Cardiothoracic and Vascular Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Thourani has been an advisor to or received research grants from Abbott Vascular, Boston Scientific, Edwards Lifesciences, Gore Vascular, and JenaValve. Dr Carroll is a local investigator in clinical trials sponsored by Edwards Lifesciences, Medtronic, and Abbott and receives consulting fees from Abbott. Dr Mack is Trial Co-PI for Abbott, Trial Co-PI for Edwards Lifesciences, and Trial Study Chair for Medtronic, all uncompensated with travel expenses paid for trial-related meetings. Dr Tang is a physician proctor for Medtronic and a consultant for Medtronic, Abbott Structural Heart, and W. L. Gore & Associates. Dr Kodali reports research funding from Edwards Lifesciences, Abbott Vascular, Medtronic, Boston Scientific, JenaValve; consultant honoraria from Admedus, Tricares, Meril Lifesciences; SAB (equity) from Thubrikar Aortic Valve Inc, Dura Biotech, Supira, Microinterventional Devices, TriFlo Medical. Dr Kaneko is a consultant for Edwards Lifesciences, Medtronic, 4C Medical, Cook Medical, and CardioMech and a speaker for Baylis and Abbott. Dr Forcillo is a consultant for Medtronic, Edwards Lifesciences and Boston Scientific and received research funding from Edwards Lifesciences. Dr Fontana is a consultant for and has received proctoring fees from Abbott, Medtronic, and LivaNova; is a Structural Heart Advisory Board Member for Abbott; and is a principal investigator for Abbott and Medtronic. Dr Kiaii is a consultant with Medtronic, Boston Scientific, Johnson and Johnson, and Abbott. Dr Balkhy is a proctor for Intuitive, AtriCure, and Edwards. Dr Kempfert receives speaker fees from Edwards, Medtronic, LivaNova, CryoLife, LSI, and Abbott, is on the Proctoring/Advisory Board for Edwards and Abbott, and receives research grants from Edwards and LivaNova. Dr Cheung is a consultant to Medtronic and Abbott Vascular. Dr Borger’s hospital receives speaker’s honoraria and/or consulting fees on his behalf from Edwards Lifesciences, Medtronic, Abbott, and CryoLife. Dr Reardon is a consultant for Medtronic, Boston Scientific, Abbott, and Gore Medical with all fees directly to his department. Dr Leon reports institutional support for clinical research from Abbott, BSC, Edwards Lifescience, and Medtronic and is an advisory board member (non-paid) for Abbott, BSC, Edwards Lifescience, Gore, and Medtronic. Dr Popma reports grants from Medtronic, Boston Scientific, and Abbott, and grants and personal fees from Edwards. Dr Ad discloses a financial relationship with Medtronic, AtriCure, LivaNova, Nido Surgical, and Left Atrial Appendage Occlusion, LLC. All other authors declared no potential conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for completion of this Consensus Statement was provided by the International Society for Minimally Invasive Cardiothoracic Surgery.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.