
Abstract
Objective
Plication of the diaphragm is a life-changing procedure for patients affected by diaphragm paralysis. Traditionally, this procedure is performed through a thoracotomy. Access to the diaphragm via this incision is poor and the indications for surgery are limited to patients who can actually sustain such an invasive approach and associated morbidities. A minimally invasive approach was developed to improve the surgical management of diaphragm paralysis.
Methods
Patients underwent minimally invasive diaphragm plication either by video-assisted or robotic surgery through a 3-port technique with CO2 insufflation. Patients were followed at the routine 6-week clinic and also by telephone consultation 6 to 12 months postoperatively. Data were collected on postoperative complications, postoperative pain or numbness, symptomatic improvement, and change to quality of life following surgery.
Results
Forty-eight patients underwent 49 minimally invasive diaphragm plication. Median postoperative length of hospital stay was 4 days (range: 2 to 34 days) and there were no cases of mortality. Mean reduction in Medical Research Council dyspnea score per patient was 2.2 points (mode: 3 points). Twenty-eight patients (77.8%) reported a significant symptomatic improvement enabling improvements in quality of life, and 97.2% (n = 35) were satisfied with the surgical outcome.
Conclusions
Minimally invasive diaphragm plication is a safe procedure associated with prompt postoperative recovery. It is effective at reducing debilitating dyspnea and improving quality of life.
Central Message
Minimally invasive diaphragm plication is a safe and effective treatment for patients who have symptomatic diaphragmatic paralysis, with improvements in dyspnea and quality of life. Our study suggests that indications for this surgical approach could be expanded.
Introduction
Pathophysiology of Diaphragmatic Paralysis
The diaphragm is the main respiratory muscle, accounting for more than 70% of respiratory effort, and is the only muscle providing ventilation when asleep and at rest. It is supplied by the phrenic nerve from spinal roots C3, C4, and C5.
Paralysis of the diaphragm is a debilitating condition, causing severe dyspnea resulting in significant limitations on quality of life. It most often results from phrenic nerve palsy, which itself has several causes, though damage could occur at any level of the neuromuscular tract. 1 This subsequently leads to atrophy of the diaphragm, which eventually stretches under the positive pressure of abdominal viscera. As a result, the diaphragm is pushed upwards into the pleural cavity, reducing pulmonary volume. Importantly, it assumes a paradoxical movement, moving further upwards into the pleural cavity with inspiration due to increased intra-abdominal pressure. 2
Most cases of phrenic nerve palsy are idiopathic with no identifiable cause, though in some cases there may be a preceding trigger or viral infection. Other common causes include trauma, malignancy, motor neuron disease, and neuropathies (of several etiologies). 3 Another important cause is iatrogenic injury, usually from thyroid, neck, or cardiac surgery. Cardiac protection with ice water, or division of the pericardiophrenic artery during internal mammary artery harvesting may underlie some of the mechanisms of paralysis after cardiac surgery, which may occur in up to 30% of patients postoperatively. 4
Clinical Presentation and Diagnosis
Unilateral paralysis in an otherwise healthy individual may be asymptomatic and remain undiagnosed. The classical presentation of unilateral paralysis is shortness of breath on bending forward or lying supine, when the increased abdominal pressure further pushes the diaphragm upwards, reducing the pulmonary volume. Although the accessory muscles can compensate better in the upright position, some patients are dyspneic at rest or during conversation.
However, unilateral paralysis in patients with significant cardiopulmonary disease often leads to severe impairment of exercise tolerance and exertional dyspnea. 3 Bilateral paralysis is rarer but may present more acutely due to the severity of dyspnea. 5 Paralysis may be a temporary phenomenon due to nerve apraxia instead of permanent injury, and some patients may report recovery.
Chest x-rays will demonstrate a raised hemidiaphragm, and together with a suggestive clinical presentation, should warrant a diaphragm fluoroscopy test, also known as a “Sniff Test.” This involves images taken during inspiration with rapid “sniffs” and will reveal paradoxical movements of the hemidiaphragm. The affected side rises during inspiration while the normal side moves downward. 6 Pulmonary function tests are usually worse when supine and may be normal when standing. 1
Patients with diaphragmatic paralysis can be misdiagnosed with chronic obstructive pulmonary disease (COPD), especially with a smoking history. It is therefore likely that this condition is more common than clinically diagnosed and a number of individuals who suffer exertional dyspnea may have undiagnosed diaphragmatic paralysis. 1
Management Strategies
Even with accurate diagnosis, patients are often managed without treatment or chest physiotherapy alone. 7,8 Despite optimum conservative management, a proportion of patients remain profoundly dyspneic and are severely limited in their daily activities. 9
The principle of surgery is to increase the volume in which the lung can expand during inspiration by minimizing paradoxical diaphragmatic movement. Therefore, accessory muscles of respiration can compensate and provide adequate inspiratory effort provided the diaphragm does not move upwards. From our experience, few patients are referred for surgical intervention. Several factors could account for low rates of surgery for diaphragmatic paralysis, despite the severity of symptoms. These include limited knowledge of surgical options among both patients and primary care physicians. Secondly, diaphragm plication has traditionally been undertaken via thoracotomy. Open surgery can have high postoperative complication rates and minimally invasive diaphragm plication surgery is yet to be widely adopted.
Aims
Our aims are to describe a minimally invasive technique for diaphragm plication and report on safety of the procedure, as well as symptomatic benefit. The video-assisted (VATS) procedure described below was conceived by Dr Joel Dunning and adopted at James Cook University Hospital since 2014. Minimally invasive plication of the diaphragm is carried out either via standard VATS approach or with the da Vinci Si robot. The benefits of minimally invasive surgery are maximized in this procedure as there is no specimen to be delivered, thereby not requiring extension of VATS ports. This augments the need to keep the ports as small as possible, reducing injury to the intercostal nerves and minimizing consequent neuropathic pain or paresthesia.
Methods
Indication for Surgery
Patients with suspected diaphragm plication should undergo routine blood tests, lying and standing pulmonary function tests, and the Fluoroscopy Sniff Test. Prior to becoming eligible for surgery, patients are followed for at least a 12-month period to ensure there is no late recovery of the phrenic nerve. Patients are only offered surgery if fluoroscopy demonstrates paradoxical movement of the hemidiaphragm. Surgical plication would minimize the paradoxical movement and improve pulmonary volumes. Other indications for surgery include life-limiting dyspnea, pulmonary atelectasis, recurrent infections, and ventilation dependency. Computed tomography (CT) scans are not routinely undertaken preoperatively but may be performed if intrathoracic pathology is suspected. CT scan is also performed when diaphragmatic rupture or hernias are differential diagnoses.
Patient Preparation
The patient is selectively intubated and positioned in lateral decubitus. The table is tilted 30° reverse Trendelenburg to move the abdominal viscera as low as possible. The table is also flexed above the hip to widen the intercostal spaces. For left-sided procedures, a nasogastric tube is recommended to empty the stomach. The surgeon and the assistant stand posterior to the patient as this facilitates an optimal view of the diaphragm and improved ability to plicate it down as the dome is higher anteriorly and may limit the surgical field when standing anteriorly.
Port Placement
Adequate placement of ports is vital to the procedure’s success (Fig. 1). On single-lung ventilation, two 5 mm and one 12 mm trocars are introduced. The first port is performed with a closed technique. A small 5 mm incision is made 2 cm behind the inferior angle of the scapula and over the fourth or fifth intercostal space. A 5 mm camera is placed inside a Kii Fios First Entry port (Applied Medical, Rancho Santa Margarita, CA, USA). This has a plastic trocar with 2 lateral holes, for CO2 insufflation, just below the blunt tip. CO2 insufflation is commenced at 6 mm Hg pressure with a flow rate of 6 L per minute. The tip of the trocar is pushed through the subcutaneous tissue and the intercostal muscles. Once the parietal pleura is breached, the CO2 will immediately create a pneumothorax and prevent injury to the lung parenchyma. The pleural cavity is then assessed, and the next two ports are placed under direct vision. The first port is generally used as the camera port, hosting a 5 mm optic. The second port is anterior to the first port, and located in the mid axillary line, in the same intercostal space or one below. The second port is larger, at 12 mm, to allow use of the Endo Stich (Medtronic, Minneapolis, MN, USA). The third port is a 5 mm port and positioned lower and posterior to the other two ports in the eighth or ninth intercostal space and is used for a 5 mm grasper. It is important not to exceed the diameter of the trocars with the skin incision in order to maintain a sealed CO2 insufflation circuit and therefore push the diaphragm down to enhance the surgical field.
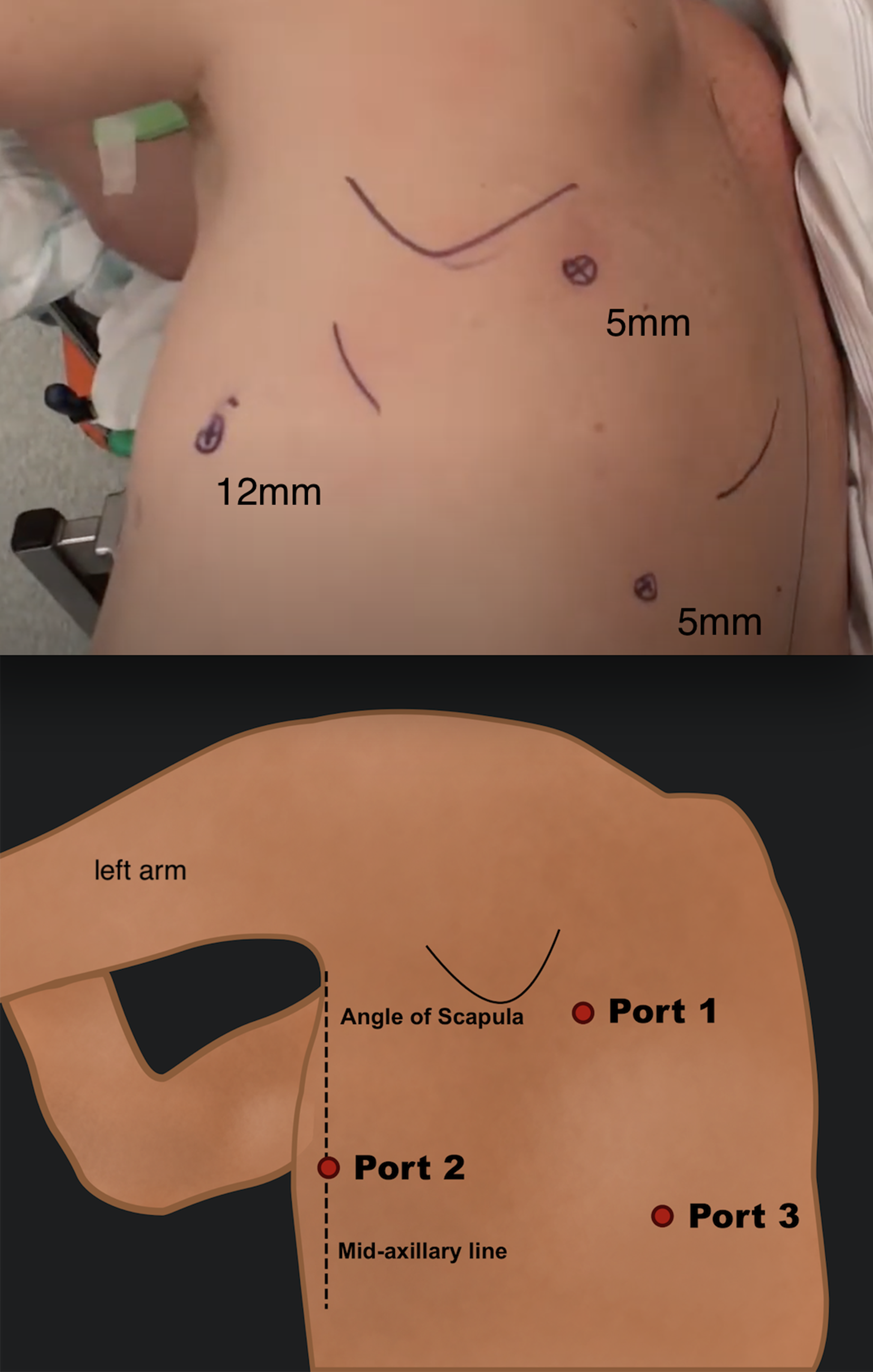
Port placement for a video-assisted approach to diaphragm plication. The first 5 mm port is placed just below the inferior angle of the scapula in the fourth or fifth intercostal space. The second and third ports are created under camera guidance with the second port located anterior to the first port in the mid-axillary line in the fourth intercostal space (12 mm port) and the third 5 mm port posteriorly in the eighth or ninth intercostal space.
VATS Plication
The hemidiaphragm is first assessed for severity of the relaxation and tissue quality of the muscle, to estimate the degree of invagination required. CO2 insufflation may be increased up to 10 mm Hg to facilitate stitching, provided the patient is hemodynamically stable.
Horizontal mattress sutures are placed with 2 braided nonabsorbable sutures (Ticron) with pledgets. The number of sutures varies depending on patient size and grade of relaxation but ranges between 8 and 16 horizontal mattress stitches (Fig. 2). Use of pledgets may prevent the suture material cutting through thinner areas of muscle. However, some reports suggest use of pledgets may contribute to reactive pleural effusion postoperatively. The first suture (Fig. 3) is placed and is of fundamental importance as it provides tension and guides the following stiches. The first stitch is placed in the middle of the fibrous part of the diaphragm. When placing the first stitch, it is important to lift up the diaphragm and stitch on either side of the grasper to prevent injury to underlying viscera. The plication continues in an oblique fashion, on a posterolateral to anteromedial line, starting beside the first stitch. The invagination of the diaphragm will lie under the suture line. Sutures should be tight as under-tightening can lead to a poor result with minimal improvement in symptoms and recurrence. Over-tightening is less likely to cause injury or tearing. The plicated hemidiaphragm is then reassessed and additional stitches can be considered. A video of the procedure with details on plication technique was previously published. 10
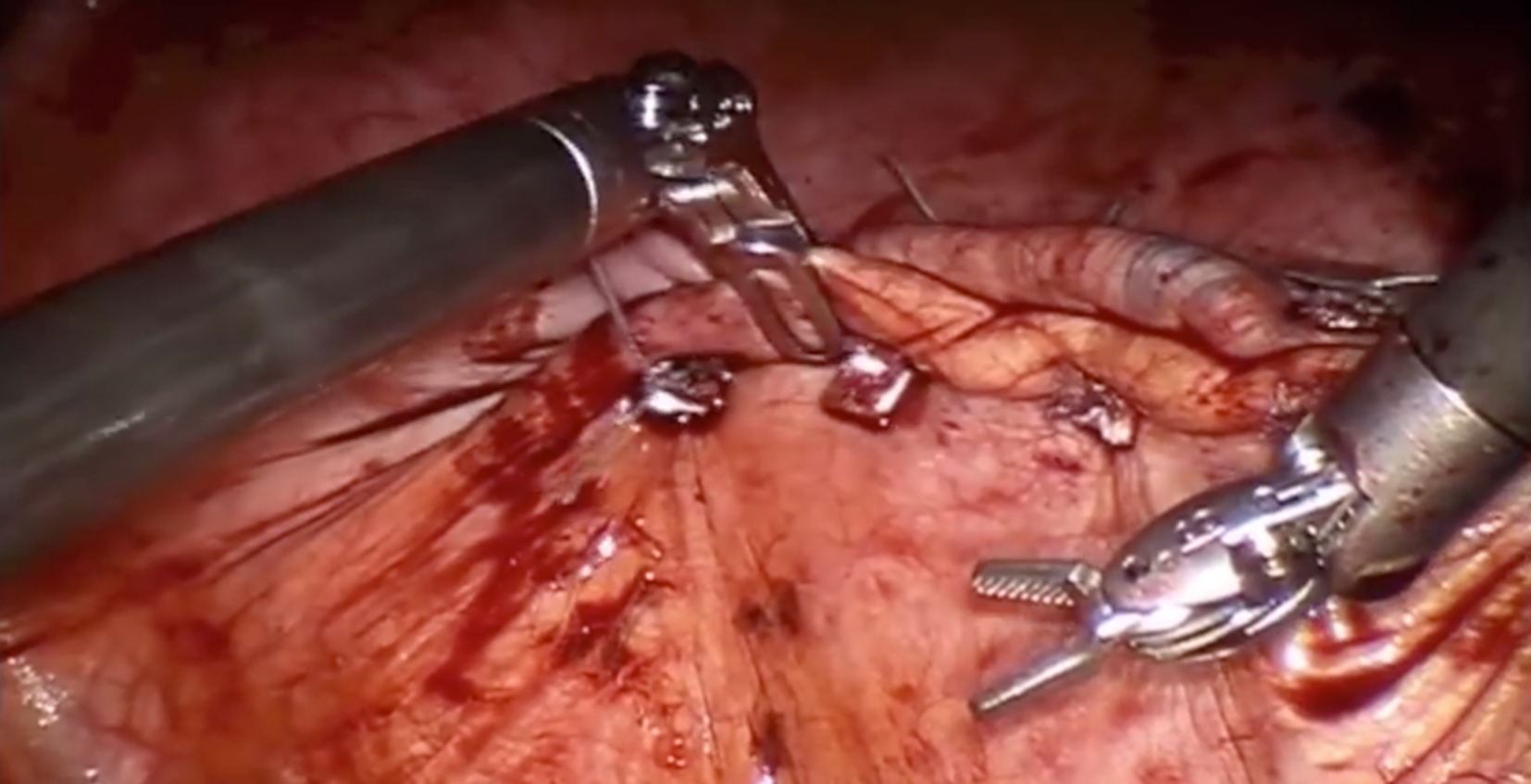
Placement of horizontal mattress sutures on the diaphragm. The number of sutures ranges between 8 and 16 depending on patient size and grade of diaphragm relaxation. Pledgets are also used to prevent sutures cutting through the thinner parts of the muscle.

The endostitcher, on the top right of the screen, placing the first stitch. Lifting up the diaphragm (grasper on the left) prevents visceral injuries.
The most common postoperative complication is pleural effusion. In order to prevent this, we opted for a basal drain. At the beginning of the experience, we adopted one apical and one basal drain but we now abandoned the apical drain. An epipleural catheter is placed for postoperative analgesia. The chest drain is left in situ until drain output is less than 50 ml over 24 hr.
Robotic Plication
The robot is particularly advantageous for diaphragm plication as it provides 360° articulation of the needle holder and other instruments as well as a 3D image of the surgical field. This improves the manual dexterity and depth perception required for stitching and reduces the learning curve for suturing compared to VATS. While dissection of tissues is more challenging in robotic surgery due to loss of pressure sensation, dissection is not typically required for diaphragm plication, making it particularly suitable for a robotic approach. Port placement is similar to VATS but requires a 10 cm distance between ports to prevent impingement of the robotic arms. An additional fourth port is also created anteriorly and lower as assistant port. The remainder of the procedure is similar to VATS.
Prevention of Late Recurrence
Despite surgical plication, there is a risk that the diaphragm may continue to stretch further with time and rise into the chest cavity, causing recurrence of symptoms. This risk may be minimized by reinforcing the suture line and anchoring it to the chest wall. A nylon suture is passed around the ninth rib, creating a ring approximately 3 cm in diameter. The suture line is overrun with a continuous line starting medially, running toward the chest wall, anchoring to the ring, then passing back to the starting point and then secured. This anchors the original suture line to the chest wall and prevents the diaphragm rising above the ninth rib.
Some authors suggested a Prolene mesh may be applied over the diaphragmatic plicated surface. This could be anchored to the ribs or to the outer surface of the diaphragm itself. In this series the mesh was adopted in 1 patient who had associated diaphragmatic Morgagni hernia.
Follow-Up and Data Collection
Data were extracted from the Thoracic Database on patient demographics, operation details, and postoperative management. Occurrence of postoperative complications, length of stay, and time to drain removal were extracted from clinical notes. All patients were followed routinely in clinic at 6 weeks postoperatively and data were collected on any further complications, symptomatic benefit, and clinical improvement. Patients were subsequently followed via telephone consultation for 6 to 12 months postoperatively with a questionnaire. Patients were asked a series of 6 questions relating to degree of breathlessness as defined by the Medical Research Council (MRC) dyspnea score, current pain, ongoing numbness, their satisfaction with the surgical results, and improvement, if any, in their day-to-day life (Supplemental Table).
{kind=link}
Statistical Analysis
Data were analyzed using quantitative and qualitative methodologies. Data are presented as means ± standard error of the mean, where applicable. Student’s t-test was used to determine statistical significance of the difference between preoperative and postoperative MRC dyspnea score. Thematic analysis was performed on free-text answers. Recurring themes were identified, and each comment was then classified into one or more themes.
Results
Forty-eight patients underwent 49 diaphragm plications during a 4-year period between August 2014 and October 2018. The mean age of patients was 60.6 years (range: 26.6 to 75.7 years). There were 67.3% (n = 33) male patients. Average body mass index was 31.8 kg/m2 with a range of 22.2 to 47.4 kg/m2. Sixteen patients had a diagnosis of COPD and 24 patients had a smoking history with an average of 21 pack-years. Data from routine 6-week clinic follow-up were obtained on 48 patients. Thirty-six patients were also followed via telephone consultation a minimum of 6 months postoperatively.
The majority of cases of phrenic nerve palsy were idiopathic (n = 29, 59.1%), though the second most common cause was trauma (n = 7, 14.3%). Iatrogenic injury accounted for 6 cases (12.2%), of which 4 cases were following cardiac surgery and 2 cases were following neck tumor excision. Other causes included cervical radiculopathy (n = 2), neuropathy (n = 3) and malignancy (n = 2; Fig 4).
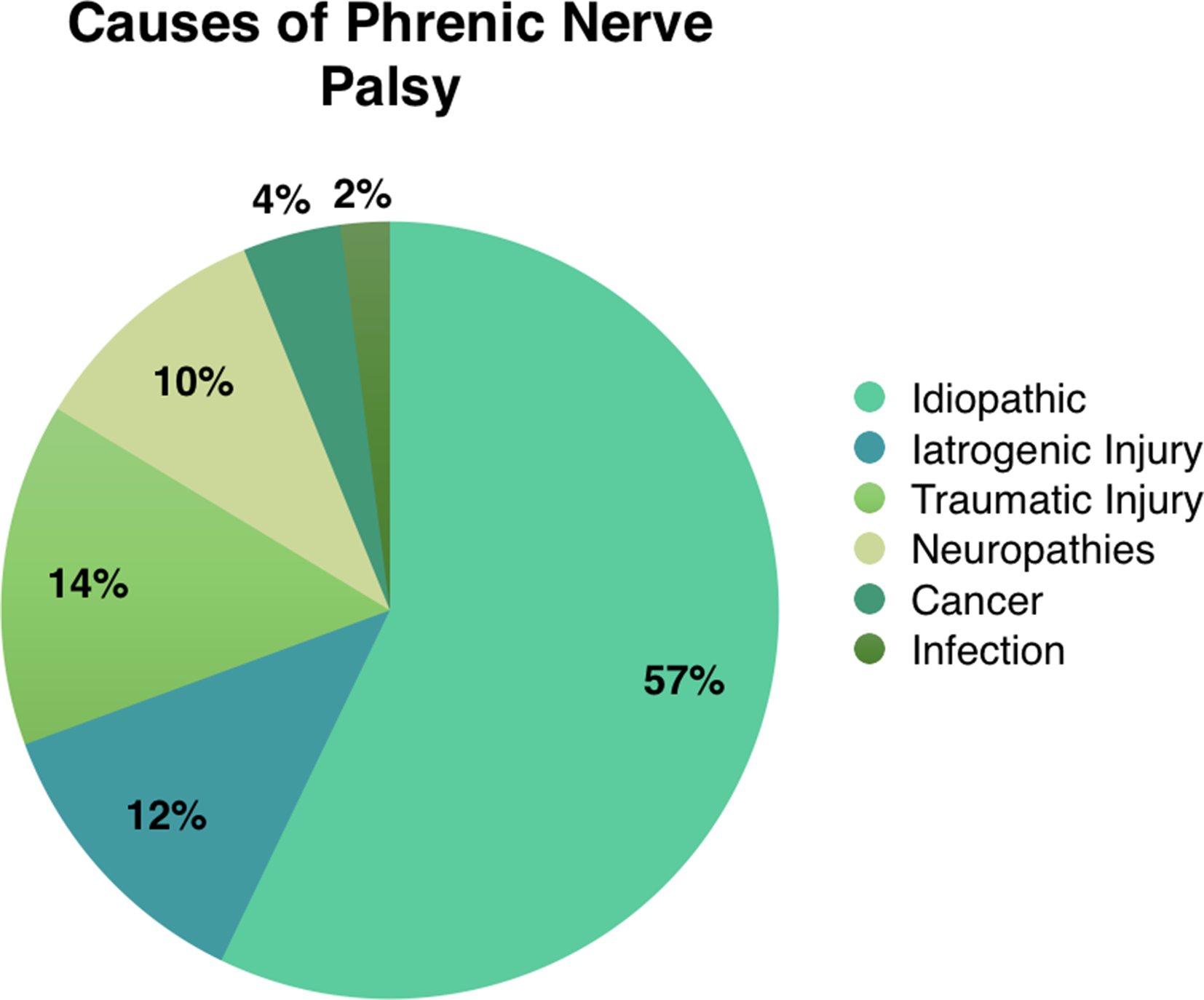
Causes of phrenic nerve palsy in patients undergoing video-assisted diaphragm plication. The most common cause of phrenic nerve palsy resulting in diaphragm paralysis was idiopathic followed by traumatic and iatrogenic injuries.
Of 49 plication procedures, 25 were left-sided and 22 were right-sided, 1 patient had bilateral sequential procedure. Thirty-five (71.4%) were undertaken via a standard VATS approach as described above. Two of these 35 were redo cases. Fourteen cases were carried out with the robot. An average of 10 sutures were placed (range: 4 to 16 sutures). The majority of patients (n = 28) had a single chest drain postoperatively. Eighteen patients had a single basal chest drain overlying the suture line whilst 10 had only an apical drain. The remaining 21 patients had both an apical and basal drain. Drains were on average removed a median of 3 days postoperatively (range: 1 to 22 days). Mean postoperative length of stay was 5.9 days with a median of 4 days (range: 2 to 34 days).
The most common postoperative complications were pleural effusions (n = 6) and pain. Two patients required admission to intensive care postoperatively, 1 of whom required a tracheostomy due to respiratory failure. This patient had bilateral paralysis and required prolonged intensive care admission with slow weaning from ventilation after both the first (left) and second procedure. There were no mortalities.
On 6-month follow-up, 7 (19%) patients reported ongoing pain related to the surgery, though average pain score among these 7 patients was 3.6 points on a Likert scale from 1 to 10, 10 being the most severe (range: 1 to 7 points). Six (17%) patients reported some degree of numbness at the operation site, and 2 of these also had chronic pain from the surgery.
The mean preoperative MRC dyspnea score was 3.8 ± 0.13 (out of 5) which reduced to an average of 1.8 ± 0.17 postoperatively (P < 0.05). The mean reduction in MRC score was 2.2 points (Fig. 5a), with the greatest number of patients reporting an improvement in MRC score by 3 points (Fig. 5b). Twenty-eight patients (77.8%) reported a significant symptomatic improvement enabling improvements in quality of life, and 97.2% (n = 35) reported satisfaction with the outcome.
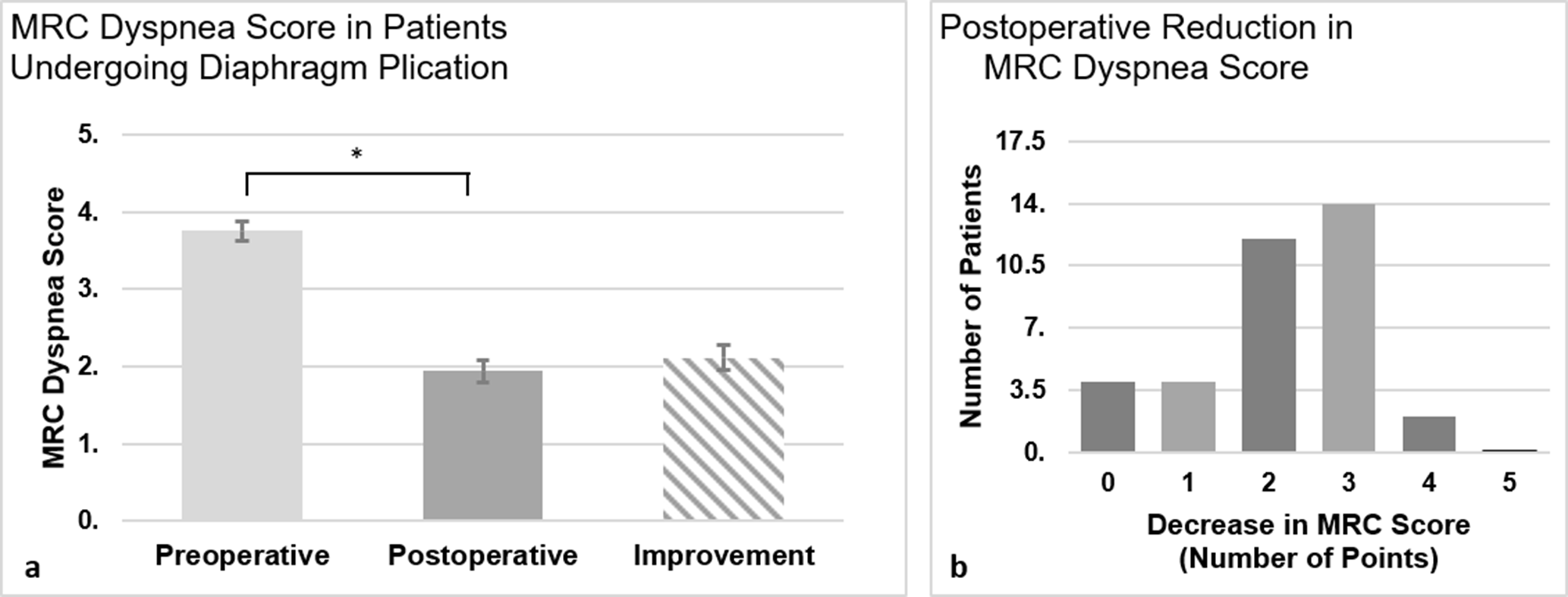
Improvement in MRC dyspnea score following diaphragm plication surgery. (
Three main themes were identified during thematic analysis: increased exercise tolerance and mobility, return to previous hobbies, and improved independence with activities of daily living. Twenty patients reported a remarkable improvement in exercise tolerance and mobility, while 19 patients described an increased ability to commence hobbies such as swimming and gardening, thus improving quality of life. Nineteen patients could undertake actions they were previously unable to, such as having conversations or lying flat.
Discussion
This paper, to date, remains the largest series published on minimally invasive diaphragm plication. Though the current literature in this field is in the form of case series and cohort studies, there is accepted evidence that surgical plication provides better outcomes than conservative management in patients with diaphragmatic paralysis, especially when symptoms begin to impact on day-to-day activities.
We suggest that only a small fraction of the patients who are diagnosed with diaphragm paralysis are referred for surgery. In this subgroup of patients with diaphragm paralysis, those who underwent surgery reported a radical improvement in their dyspnea and significant benefit to their quality of life.
The principles of surgery are to reduce the surface of the diaphragm creating an infold. This brings the muscle back to the normal anatomical position. Although this will not regenerate lost neurological function, it will re-establish a larger pleural cavity and stop the paradoxical movement. This allows for re-expansion of the pulmonary parenchyma, facilitated by accessory respiratory muscles, and prevents recurrent infections of the previously atelectatic segments.
Current Evidence for Surgery
Several studies evaluating open diaphragm plication have since been undertaken with evidence of good outcomes and improvement in symptoms. 9,11 -13 Furthermore, the effect of surgery is lasting with maintained improvement of symptoms at long-term follow-up of at least 5 years postoperatively. 11,12,14 However, open procedures via thoracotomy may be associated with significant risk of morbidity and long-term pain due to intercostal nerve injury compared to thoracoscopic procedures. 15
With the progress of minimally invasive surgery, a number of endoscopic techniques have been reported, significantly reducing the burden of morbidity while showing similar or superior results. 16 -21 The benefit of a minimally invasive approach is maximized in diaphragm plication surgery as there is no tissue resection and the incisions do not need to be enlarged for specimen delivery. Gharagozloo was the first to report a minimally invasive approach by VATS in 1995. 19 Mouroux’s technique, published in 1996, was more reproducible and widely accepted. 18 It consists of 2 small ports in the fifth intercostal space and a 5 cm minithoracotomy over the diaphragm, which is used for the needle holder and to create the invagination. 18
In our cohort, patients experienced dramatic improvement in their quality of life and significant amelioration of dyspnea. In line with our study, previous studies also clearly demonstrate symptomatic improvement, increase in pulmonary function, and return to premorbid levels of functional status with surgery.
Mouroux and colleagues reported significant improvements in symptoms and lung function tests, which persisted at long-term follow-up. The principles described in that pioneer paper remain valid. Prior to our study, Freeman and colleagues report the largest case series of diaphragm plication, consisting of 41 patients of which 30 were thoracoscopic, and demonstrated improvement in symptoms, spirometry values, and functional status following surgery. 16 In a small series of 4 patients, Kim and colleagues proposed a similar technique with the use of CO2 insufflation and three 5 mm ports employing a completely endoscopic approach. 17 They also achieved marked symptomatic improvement in their patients with no recurrence at 6-month follow-up. Yalcinkaya and colleagues more recently described a uniportal VATS approach to diaphragm plication and also demonstrated effectiveness of the procedure with good symptomatic relief. 21
There is increasingly strong evidence that diaphragm plication can improve quality of life and symptoms. However, in our experience, many patients and general practitioners were not aware of a surgical option and were therefore not referred to a thoracic service. We are now receiving an increasing number of referrals.
Reported Complications
Complication rates are minimal with only 2 patients requiring intensive care postoperatively and no injuries to viscera are reported at our institution with VATS or a robotic approach. Other studies providing data on minimally invasive diaphragm plication also reported minimal complications with no mortalities as a result of the procedure or conversion to thoracotomy. 16 -20,21,21 Length of stay was also shorter with minimally invasive surgery than expected with an open approach. 19 As reported by other authors, in patients with bilateral paralysis the recovery is complicated by initial respiratory failure.
Other Treatment Options and Approaches
Abdominal procedures are more difficult, especially on the right due to the presence of the liver and should be restricted to a small group of patients who have undergone previous chest surgery, in whom dense adhesions may be anticipated. 22 Higher risk of iatrogenic organ damage is also a complication of an abdominal approach. 23
There is some evidence for the role of pacing in diaphragmatic paralysis, particularly bilateral cases due to spinal cord injury or amyotrophic lateral sclerosis (ALS). 24,25 However, a randomized trial on diaphragm pacing in patients with ALS indicated higher mortality in those who underwent pacing of the diaphragm. 26 Further studies are required in order to establish the safety of pacing or electrical stimulation devices.
There is also some evidence for conservative management or a “watch and wait” approach in patients with iatrogenic phrenic nerve palsy presenting with mild symptoms and unilateral paralysis. This is most commonly due to cardiac surgery, particularly from usage of ice water to cool the myocardium, resulting in phrenic nerve damage. 4 There is some evidence for recovery of the phrenic nerve during mid-term follow-up following cardiac surgery. 7,27 Mehta and colleagues report success with management of symptoms with chest physiotherapy alone. However, Katz and colleagues report significant persistence of symptoms, requiring readmission to hospital and decrease in quality of life, suggesting a role for earlier surgical intervention. 28
Limitations
This is a noncomparative prospective case series on a small subgroup of patients with diaphragm paralysis, who have been selected by other medical practitioners as candidates for surgical referral, leading to selection bias. These patients may have more symptomatic or moderate to severe forms of diaphragmatic paralysis, and therefore the impact of surgical intervention on mild diaphragmatic paralysis is not entirely characterized in this study. Similarly, patients referred for surgery may also be those perceived to be good surgical candidates. Consequently, this case series may only describe lower-risk patients and exclude high-risk patients who did not have an opportunity to undergo surgery due to non-referral. However, in this subgroup of patients we have demonstrated a significant benefit conferred from surgery, and further studies are required to characterize the presence of similar benefit in other groups. Another limitation is that for logistic issues we could not have postoperative pulmonary function tests in all the patients and therefore these data were not analyzed.
Conclusions
Minimally invasive plication of the diaphragm is safe, and it is a life-changing procedure for dyspneic patients affected by diaphragm paralysis of different etiologies. However, patients with diaphragm paralysis likely represent an “under-treated” group of patients who may benefit from a relatively low risk procedure via a minimally invasive technique. The development of this approach, which is associated with low complication rates and rapid recovery, may suggest that the indications for surgery should be widened to higher-risk patients.
Supplemental Material
Table S1 - Supplemental material for Minimally Invasive Plication of the Diaphragm: A Single-Center Prospective Study
Supplemental material, Table S1, for Minimally Invasive Plication of the Diaphragm: A Single-Center Prospective Study by Marco Nardini, Shruti Jayakumar, Marcello Migliore, Mario Nosotti, Ian Paul and Joel Dunning in Innovations: Technology and Techniques in Cardiothoracic and Vascular Surgery
Supplemental Material
Presentation S1 - Supplemental material for Minimally Invasive Plication of the Diaphragm: A Single-Center Prospective Study
Supplemental material, Presentation S1, for Minimally Invasive Plication of the Diaphragm: A Single-Center Prospective Study by Marco Nardini, Shruti Jayakumar, Marcello Migliore, Mario Nosotti, Ian Paul and Joel Dunning in Innovations: Technology and Techniques in Cardiothoracic and Vascular Surgery
Footnotes
Acknowledgments
The authors would like to thank all the professionals at James Cook University Hospital (Middlesbrough, UK) who were involved in the care of the patient cohort described.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.