
Abstract

We have read with great interest the article of Kaleda et al. 1 entitled “Simple Technique for Central Venous Cannulation with Cannula-Free Wound in Minimally Invasive Aortic Valve Surgery.” First of all, we congratulate the authors for their invaluable contribution to the literature.
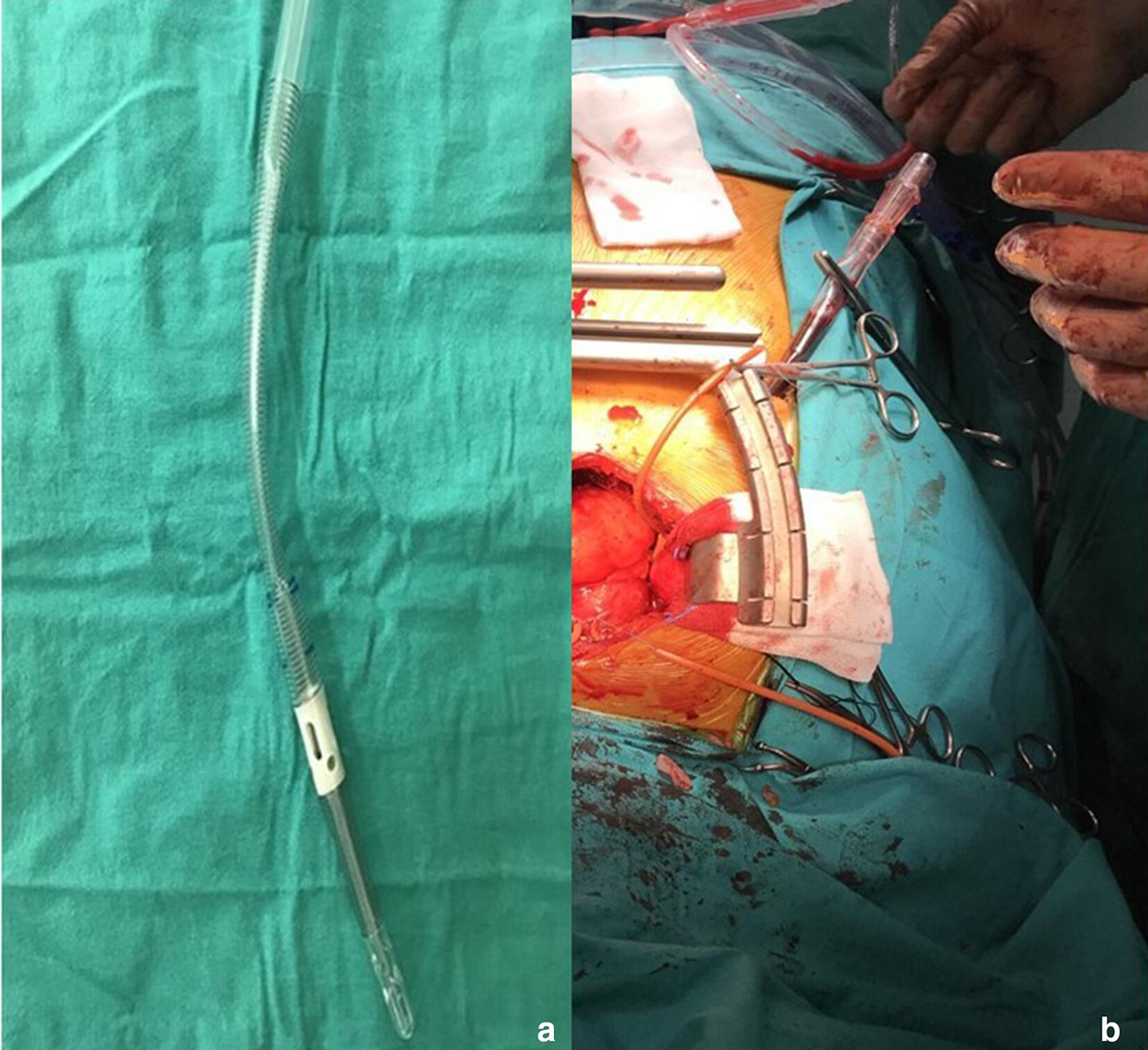
The authors have described a technique for central venous cannulation during minimally invasive aortic surgery using a novel device. However, we have been using this technique in our clinic since 2017. Also, our technique was presented as poster (Poster-244, page 215 in poster book) at the 15th Congress of the Turkish Society of Cardiovascular Surgery, October 26-29, 2018, Antalya, Turkey. 2 In our technique, unlike the authors, we did not use an additional instrument (like their novel device) for venous cannula and we still do not use any device. We use a flat venous (low body profile) two-stage venous cannula (Fig. 1a).We perform a 1 cm incision under the breast (fifth or sixth intercostal space) and open the right pleura. Using a surgical clamp, venous cannula is externalized from the chest (Fig. 1b). During this procedure, subcutaneous fatty tissues may contaminate the venous cannula. For this reason, we first pass the cannula and then wash the cannula with saline. We have been using this technique in our clinic since 2017 and we have not encountered any complications related to this method. Also, skin incision in the chest wall is used for postoperative tube thoracostomy.
(
In recent years, minimally invasive methods are widely used in heart operations, as in many areas of medicine. Various surgical equipment is needed in order to provide adequate exposure in minimal surgical methods. 3 Pfeiffer et al. described a novel technique in minimally invasive aortic surgery in 2015. In this technique, after ministernotomy, a 29-Fr Optiflow venous cannula (LivaNova PLC, London, UK) was placed through a purse suture in the superior vena cava by retracting the ascending aorta to the left. 4 Aortic surgery with partial sternotomy is a safe and effective strategy, and this method requires additional surgical equipment. Thanks to our technique, surgical interventions for the aortic root can be successfully performed using standard surgical equipment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.