
Abstract
Objective
We investigated health and healthcare disparities in the treatment of aortic stenosis with transcatheter aortic valve replacement (TAVR) and how they affect resource utilization and costs.
Methods
We retrospectively reviewed all patients who were discharged alive after TAVR between 2012 and 2017 from the National Inpatient Sample. Patients were stratified by race and outcomes investigated were in-hospital complications, total procedural costs, and resource utilization. High resource utilization (HRU) was defined as length of stay (LOS) ≥7 days or discharge to a nonhome location. Multivariable regression models were used to identify predictors of HRU.
Results
TAVR patients (N = 29,464) were stratified into Caucasians (n = 25,691), others (n = 1,274), Hispanics (n = 1,267), and African Americans (AA, n = 1,232). More AA and Hispanics had TAVR at urban teaching centers (P = 0.003) and were less likely to be Medicare beneficiaries (P < 0.001). Distribution of TAVR patients in the lowest income quartile showed AA (50%) versus Caucasian (20%) versus Hispanic (33%, P < 0.001). In-hospital complications were higher among Hispanics and AA than Caucasians with prolonged LOS, procedural costs, and HRU. On multivariable analysis, independent predictors of HRU were TAVR year (P < 0.001), advanced age (P < 0.001), female sex (P < 0.001), non-Caucasian race (P = 0.038), history of coronary artery bypass grafting (P < 0.001), smoking (P < 0.001), chronic lung disease (P = 0.003), stroke (P < 0.001), and lowest income quartile (P = 0.002).
Conclusions
There exist significant healthcare and health disparities among patients undergoing TAVR in the United States. Consequently, this unequal access to care and determinants of heath translate into higher resource utilization and costs.
Keywords
Central Message
Data from a national registry found that significant healthcare and health disparities exist among patients undergoing TAVR in the United States. Consequently, unequal access to care and determinants of heath translate into higher resource utilization and costs.
Introduction
Transcatheter aortic valve replacement (TAVR) has revolutionized the treatment of aortic stenosis (AS) over the past decade. It is the mainstay of treatment in AS patients who are deemed high-risk for surgical aortic valve replacement (SAVR), and its indication has expanded rapidly to lower risk profiles in recent years. 1 As such, the use of TAVR for management of AS in a broader patient population is expected in the future. Racial disparities in the access to TAVR have been described in the literature with disproportionately lower rates of minorities documented among patients who undergo TAVR in the United States. 2
Previous studies have shown the possible impact of race on long-term outcomes and resource utilization after SAVR. 3 While comparable adjusted outcomes in different races have been demonstrated after TAVR, the effect of race on resource use has not been well established. In this study, we focus on the racial disparities among AS patients treated with TAVR and seek to identify if these racial variations lead to differences in high resource utilization (HRU), defined as length of stay (LOS) ≥7 days or discharge to a location other than home. The implications of this study are important especially in the current era of value-based healthcare delivery.
Methods
The National Inpatient Sample (NIS) database was queried for patient information between 2012 and 2017. The records identify hospital stay and include information on primary and secondary discharge diagnoses and procedures, demographics, hospital characteristics, expected payment source, total charges, discharge status, LOS, and comorbidity measures.
The International Classification of Diseases, Ninth Edition, Clinical Modification (ICD-9-CM) procedure codes was used to identify all patients aged ≥18 years undergoing TAVR (procedures codes 35.05, 35.06, 02RF37H, 02RF37Z, 02RF38H, 02RF38Z, 02RF3JH, 02RF3JZ, 02RF3KH, and 02RF3KZ) from January 2012 to December 2017. Records with missing data on any of the baseline characteristics were excluded from analysis. The final study population was divided into 4 groups according to race/ethnicity: Caucasian, African American (AA), Hispanic, and other race. Patients were classified as other race if they were Asian, Pacific Islander, or Native American.
The following baseline patient and hospital characteristics were used in our study: age, sex, weight status, history of relevant comorbidities (diabetes mellitus, hypertension, smoking history, coronary artery disease [CAD], chronic heart failure [CHF], chronic lung disease [CLD], chronic liver disease, and chronic renal failure [CRF]), history of relevant procedures (percutaneous coronary intervention [PCI], coronary artery bypass grafting [CABG], implantable cardioverter defibrillator [ICD] insertion), insurance status, income status, TAVR approach, urgency of TAVR, TAVR center volume, hospital bed size, hospital location, and hospital region. Centers were classified as high, medium, or low volume if they performed >100, 50 to 100, or <50 TAVR cases annually, respectively.
Our primary endpoint was HRU, a variable defined as the composite of LOS ≥7 days or discharge to a location other than home. Our secondary endpoints were comprehensive cost of procedure, in-hospital mortality, LOS, discharge location, presence of complications such as acute kidney injury (AKI), acute myocardial infarction, cardiac arrest, cardiogenic shock, combination, hemorrhage, respiratory complications, stroke, vascular complications, blood transfusion, pacemaker placement, postoperative sepsis, postoperative pneumonia, AKI requiring dialysis, and acute respiratory failure.
Statistical Analysis
Differences in patient baseline and hospital characteristics and patient outcomes were assessed within each racial group using descriptive statistics and analyzed using Pearson Chi-Squared tests. Multivariable logistic regression models were used to identify predictors of HRU and to estimate odds ratios (OR). Variables considered for the regression model included age, sex, weight status, history of relevant comorbidities (diabetes mellitus, hypertension, smoking history, CAD, CHF, CLD, chronic liver disease, and CRF), history of relevant procedures (PCI, CABG, ICD insertion), insurance status, income status, TAVR approach, urgency of TAVR, TAVR center volume, hospital bed size, hospital location, and hospital region. Variables were chosen a priori according to clinical relevance or included in the final model if they were deemed significant after backward selection using the minimum Akaike information criterion at a P value <0.05. Statistical analyses were performed using Stata Statistical Software: Release 15 (StataCorp, College Station, TX, USA) and P values <0.05 were considered statistically significant.
Results
A total of 29,464 patients who underwent TAVR between 2012 and 2017 were included in the study. These included 25,691 Caucasians (87.2%), 1,274 others (4.3%), 1,267 Hispanics (4.3%), and 1,232 AA (4.2%). Compared with Caucasians, the minority groups were significantly younger. Gender stratification of the groups demonstrated that only AA and Hispanics groups had a female majority (57.7%) whereas Caucasians (45.8%), Hispanics (51.3%), and others (47.0%) did not (P < 0.001). There was a heterogenous distribution of comorbidity burden among the groups according to the different races. Of note, significant differences across race were found in the percent of patients with a history of diabetes mellitus (P < 0.001), obesity (P < 0.001), smoking (P < 0.001), CRF (P < 0.001), and in income status (P < 0.001), number of elective TAVR procedures (P < 0.001), and the distribution of procedures at low-volume centers (P < 0.001).
Hispanic patients had the highest representation of patients with a history of diabetes mellitus (44.2%), with procedures in low volume-centers (28.0%), and with Medicaid insurers (4.7%). They also had notable percentage of patients in the lowest income quartile (32.6%) and patients who underwent nonelective TAVRs (27.2%). AAs had the highest representation of patients with CRF (47.3%), obesity (19.0%), with incomes in the lowest quartile (50.5%), and with nonelective TAVR procedures (28.0%) and had a secondary emphasis on Medicaid insurers (2.5%). Caucasians had the highest representation of patients with a history of smoking (25.9%) and the lowest number of patients with diabetes mellitus (33.8%), with CRF (31.1%), with Medicaid insurance (0.8%), and with nonelective TAVRs (19.3%). No significant interracial differences were detected for a prior history of hypertension, CHF, and chronic liver disease (Table 1).
Baseline Demographic and Clinical Characteristics of TAVR Patients in the United States Stratified by Race.
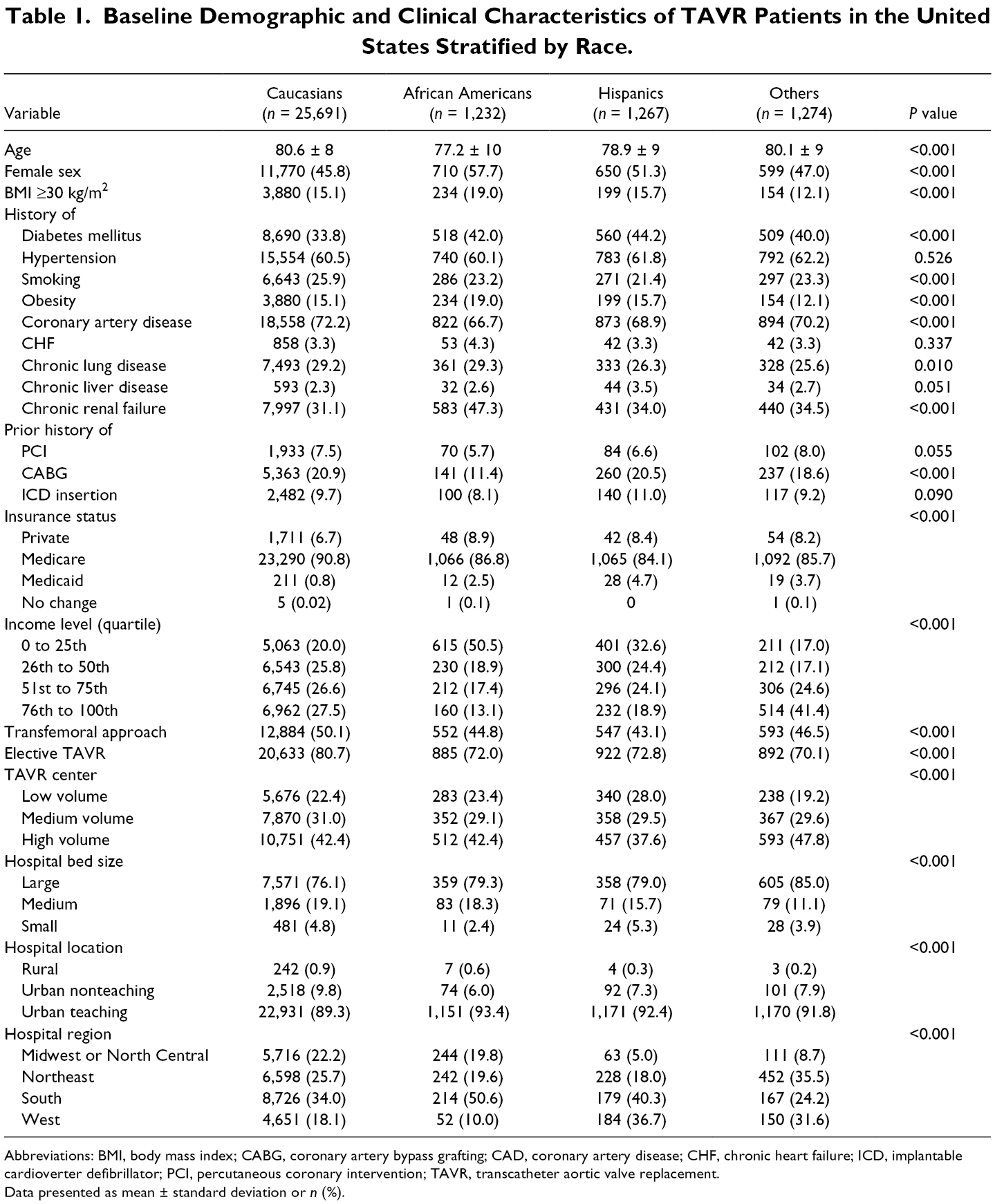
Abbreviations: BMI, body mass index; CABG, coronary artery bypass grafting; CAD, coronary artery disease; CHF, chronic heart failure; ICD, implantable cardioverter defibrillator; PCI, percutaneous coronary intervention; TAVR, transcatheter aortic valve replacement.
Data presented as mean ± standard deviation or n (%).
AA and Hispanics had a greater percentage of patients undergoing TAVR at urban teaching hospitals (93.4% and 92.4%, respectively) compared with Caucasians (89.3%) and others (91.8%). Hospital region was heterogeneously distributed among the groups. Caucasians were focused in the South (34.0%) and Northeast (25.7%), while AA and Hispanics were more likely to present for TAVR in the South (50.6% and 40.3%, respectively; Table 1).
HRU was different (P = 0.047) among Caucasians (32.6%), AA (33.8%), Hispanics (30.5%), and others (32.3%). Our secondary endpoints demonstrated significant differences in LOS (P < 0.001), comprehensive operation cost (P < 0.001), blood transfusions (P < 0.001), AKI (P < 0.001), AKI requiring dialysis (P < 0.001), pulmonary complications (P < 0.001), and postoperative sepsis (P = 0.01). Hispanics and AA had longer LOS (6.6 ± 7 days) and higher total procedural costs ($54,237 ± $33,631 and $54,717 ± $31,486, respectively), when compared with Caucasians. The following outcomes were not different among the groups: stroke (P = 0.348), vascular complications (P = 0.149), and pacemaker implantation (P = 0.090; Table 2).
In-Hospital Outcomes of Study Population Stratified by Race.
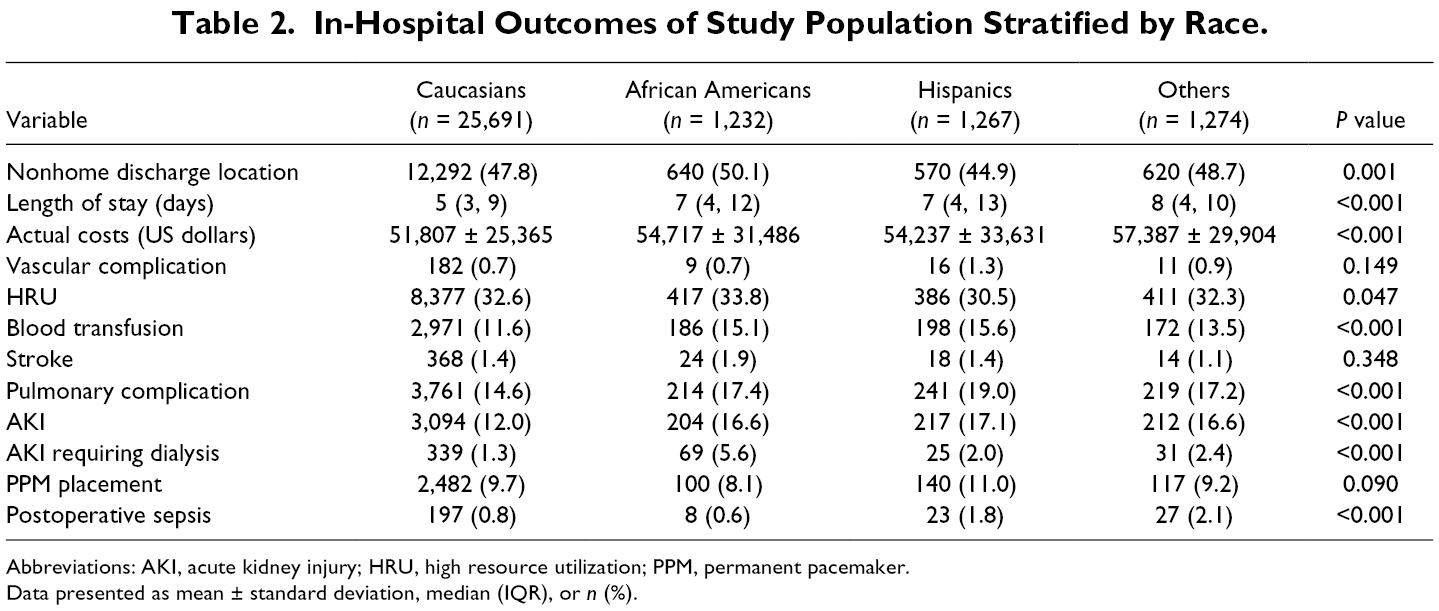
Abbreviations: AKI, acute kidney injury; HRU, high resource utilization; PPM, permanent pacemaker.
Data presented as mean ± standard deviation, median (IQR), or n (%).
On multivariable logistic regression, the following variables were independently associated with HRU after TAVR: year (2012 vs 2017), sex, race (Non-Caucasian vs Caucasian), income status (25th to 50th vs 76th to 100th percentile), and history of CAD, CHF, CLD, hypertension, stroke, and CRF. TAVR year (OR: 1.84 [1.55 to 2.16]), presence of CRF (OR: 1.71 [1.54 to 1.88]), and history of CHF (OR: 1.58 [1.29 to 1.94]) were the strongest predictors of HRU after TAVR. An independent association between the Hispanic race and HRU was noted (OR: 1.31 [1.02 to 1.67]; Fig. 1).
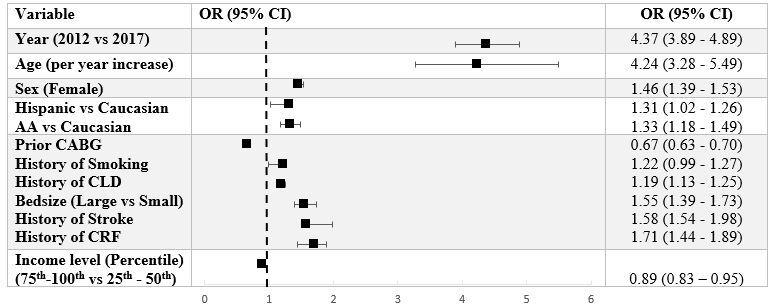
Forest plot of independent predictors of high resource utilization among a national cohort of TAVR patients. AA, African American; CABG, coronary artery bypass graft; CI, confidence interval; CLD, chronic lung disease; CRF, chronic renal failure; OR, odds ratio.
Discussion
The present study showed that healthcare disparities exist among AS patients who had TAVR in the United States. Compared with Caucasians, minority populations reported higher rates of post-procedure complications which resulted in higher costs and resource utilization.
There was a disproportionately lower number of minority patients who underwent TAVR for the management of AS. Healthcare disparities in access to novel technologies for the management of structural heart diseases has been described by previous authors. 2,4 -6 Although the prevalence of these diseases was high in Caucasians, the rates of utilization of novel technologies per affected subjects remained significantly low in minority populations. 2 AA and Hispanic patients were less likely to receive common interventions for structural heart diseases than their Caucasian counterparts. We demonstrated a similar trend in our study with real-world data from a national registry. Minority groups were younger with a higher incidence of baseline chronic diseases such as diabetes mellitus, CAD, and CRF than Caucasians, which may suggest worse access to care for chronic conditions. This translated into a greater proportion of emergent TAVR in minorities, raising the notion that TAVR in most of these patients was performed as a bailout procedure rather than part of a treatment protocol. Moreover, considering the higher incidence of comorbidities in minority populations as shown with the present analysis, it will be prudent to state that they will benefit more from TAVR as their overall estimated surgical mortality risk may be higher than that of nonminority populations.
We demonstrated worse post-procedure complication rates in minority groups than Caucasians and this was associated with a disproportionate increase in HRU and procedural costs. These findings are supported with a recent report by the American Heart Association, which predicted that the total costs of cardiovascular diseases in both AA and Hispanics are expected to surpass those of Caucasians in the next two decades. 7 Many of these healthcare costs can be avoided with an increased focus on curtailing the development of diseases rather than managing chronic diseases and their complications. Although some racial disparities are influenced by genetic differences, particularly CRF, other differences, like low income status, can be abated with better access to healthcare and early management of diseases. 8
In an analysis of the TVT registry, Alkhouli et al. described comparable 30-day and 1-year mortality rates in minority patients and Caucasians. Another study of Medicare patients who had either SAVR or TAVR, showed that race had no effect on mortality rates during similar time points. 2 A single-center experience by Minha et al. observed the same findings although it was limited by a smaller sample size. 9 Nevertheless, none of these studies evaluated the net effect on resource utilization in achieving comparable mortality outcomes. Our findings suggest that the current healthcare system may achieve these mortality benefits at the expense of disproportionately high healthcare costs. This is the first study to characterize the impact of race on resource utilization after TAVR. Additionally, it adds clinically relevant information in how comprehensive TAVR costs are achieved in minority populations.
However, as with all observational studies, the data analyzed in this study are limited by measured variables. Therefore, unmeasured or confounding variables may account for some of the associations found. Secondly, the Society of Thoracic Surgeons scores and other essential prognostic information could not be computed as this information is not available in the database. Furthermore, due to the large number of variables included in the NIS database, coding and documentation errors across hospitals may bias the study, although this is unlikely as the magnitude of the dataset would dilute such errors. Finally, the database provides no information on long-term outcomes as NIS is a time-discrete database.
Conclusions
In conclusion, with data from a national registry, we showed that among patients undergoing TAVR, racial minorities have worse comorbidities at baseline and are under-represented. These differences resulted in worse postoperative complication rates and HRU. As the United States healthcare system aims for a value-based approach, these shortcomings warrant further scrutiny and re-evaluation. Better access to healthcare and early management of diseases will help abate the progression of this medically demanding diseases.
Supplemental Material
Visual Abstract - Supplemental material for Health and Healthcare Disparities: Impact on Resource Utilization and Costs After Transcatheter Aortic Valve Replacement
Supplemental material, Visual Abstract, for Health and Healthcare Disparities: Impact on Resource Utilization and Costs After Transcatheter Aortic Valve Replacement by Alexis K. Okoh, Nehal Dhaduk, Aakash M. Shah, Justin Gold, Setri Fugar, John Kassotis, Chunguang Chen, Leonard Y. Lee, and Mark J. Russo in Innovations: Technology and Techniques in Cardiothoracic and Vascular Surgery
Footnotes
*
Presented at the Eastern Cardiothoracic Surgical Society 57th Annual Meeting, October 2019, Naples, FL.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.