
Abstract

In cardiac surgery, venodilation occurs shortly after the institution of cardiopulmonary bypass (CPB), necessitating fluid or vasoconstrictor administration to maintain adequate oxygen delivery. 1 This phenomenon is highlighted in conventional CPB by the presence of the venous reservoir, which allows for the visualization of the dynamic volume during cardiac surgery procedures and to visually perceive the venodilation phenomenon. The literature provides some consideration of central venous pressure (CVP); in particular, any given CVP value will not accurately predict whether a patient will respond to fluids. This is true for all variables, including cardiac output, capillary refill time, central venous oxygen saturation, urine output, and blood lactate level. Nevertheless, when the CVP is low, there is a greater chance of an increase in cardiac output in response to fluids. 2 In this context, we found some analogies of fluid management in relation to CVP during minimally invasive extracorporeal circulation (MIECC) techniques in particular for closed systems without the dynamic vision of venous volume in a hardshell or softshell reservoir. This aspect is connected not only to the types of circuit, hardware, and safety systems of the console but also to the “tricks” and strategies of the perfusion operator and anesthetist during the procedures.
At our institution, 50 adults were scheduled for isolated elective coronary artery bypass grafting with MIECC volume management (type III). Baseline characteristics are reported in Table 1. Patients analyzed in this context were not critical, did not have endocarditis or septic shock, and reported good preoperatory hemodynamical stability without the use of diuretics and Swan-Ganz catheter. Anesthesia was induced with intravenous sufentanil (0.5 to 1 μg/kg) and midazolam (0.08 to 0.2 mg/kg), and tracheal intubation was facilitated with intravenous rocuronium (0.6 to 1 mg/kg). 1 Anesthesia was maintained with propofol (2 to 5 mg/kg) and sufentanil (0.5 to 2.0 μg/kg), and the depth of anesthesia was monitored using bispectral index (BIS) values (BIS XP, Aspect Medical System, Newton, MA, USA). The dosage of propofol was titrated to maintain BIS values between 40 and 45. Normothermic blood cardioplegia (St Thomas solution) was used in all cases and repeated every 20 min. Oxygen delivery was calculated as follows: cardiac output × arterial oxygen concentration × 10. During the cross-clamp time, we observed and collected the CVP values and correlations for various situations for including blood flow, inlet of pump pressure, cardiac cavities (stretched or empty), and mean arterial pressure with solutions correlation and volume management strategies for ideal CVP (3 to 5 mm Hg). We share our approach for volume management (Table 2). During MIECC type III, we used a central cannulation with a single atriocaval cannula 32/40 Fr for the right atrium and 22 to 24 Fr arterial cannula for the ascending aorta (Fig. 1). 3 Nevertheless, in the literature, there are no clear CVP nadirs on MIECC for volume management. 4 Table 2 describes our approach to volume management in relation to CVP. Nevertheless, further studies are needed to support the CVP nadirs during the MIECC approach.
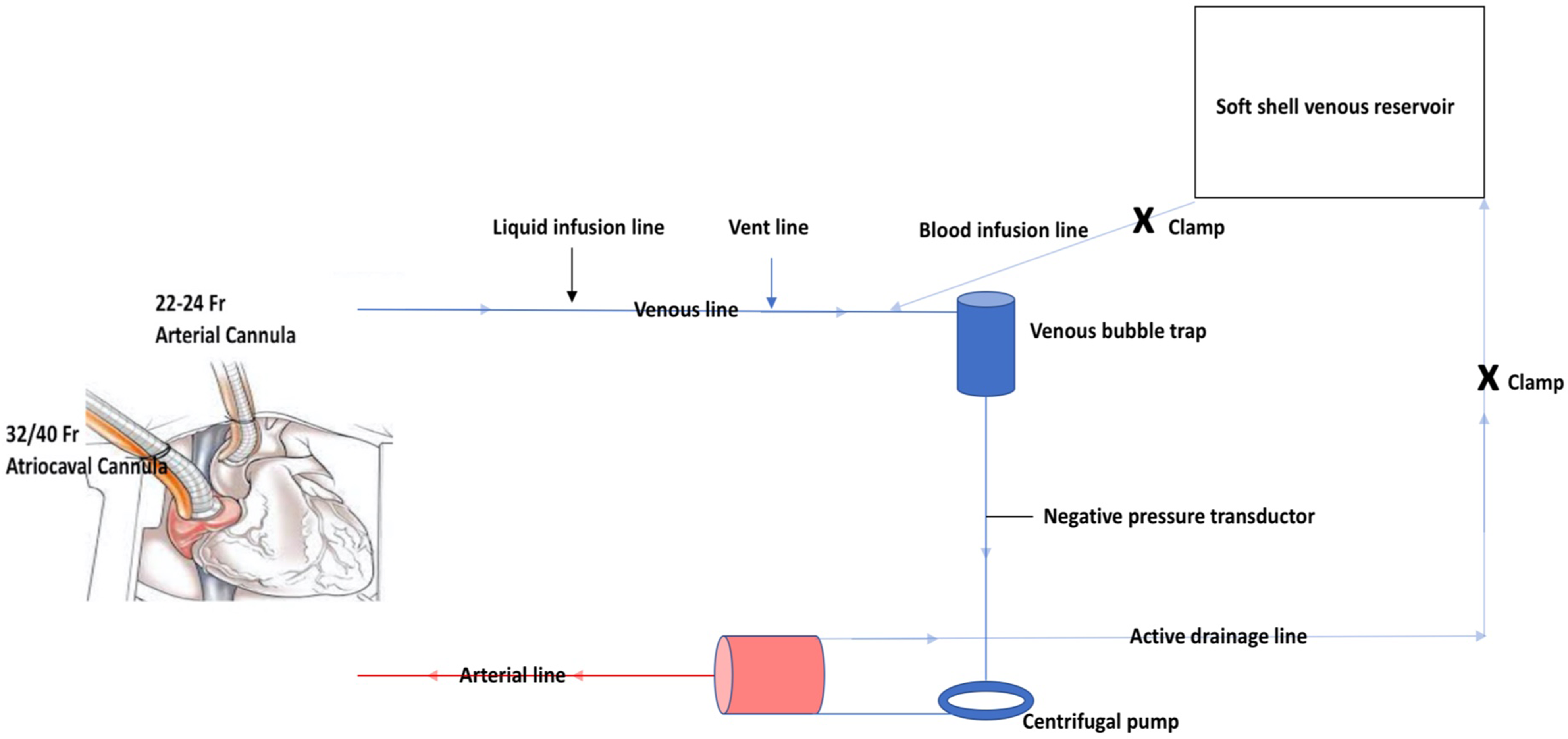
Minimally invasive extracorporeal circulation type III sketch.
Clinical Characteristics of the Study Group.
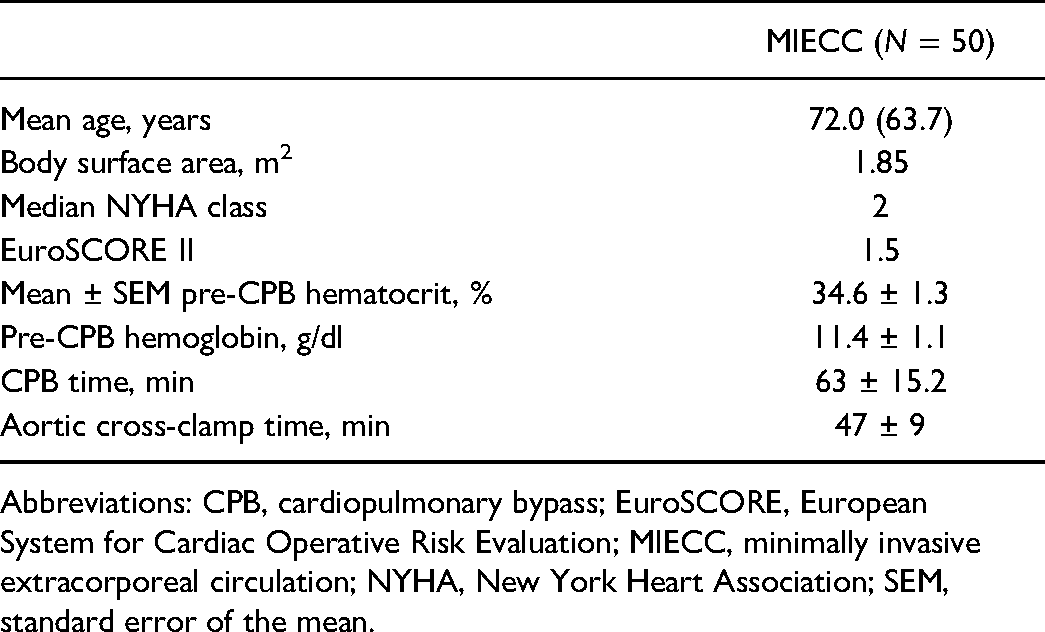
Abbreviations: CPB, cardiopulmonary bypass; EuroSCORE, European System for Cardiac Operative Risk Evaluation; MIECC, minimally invasive extracorporeal circulation; NYHA, New York Heart Association; SEM, standard error of the mean.
Situations and Solutions for Volume Management During MIECC Technologies.
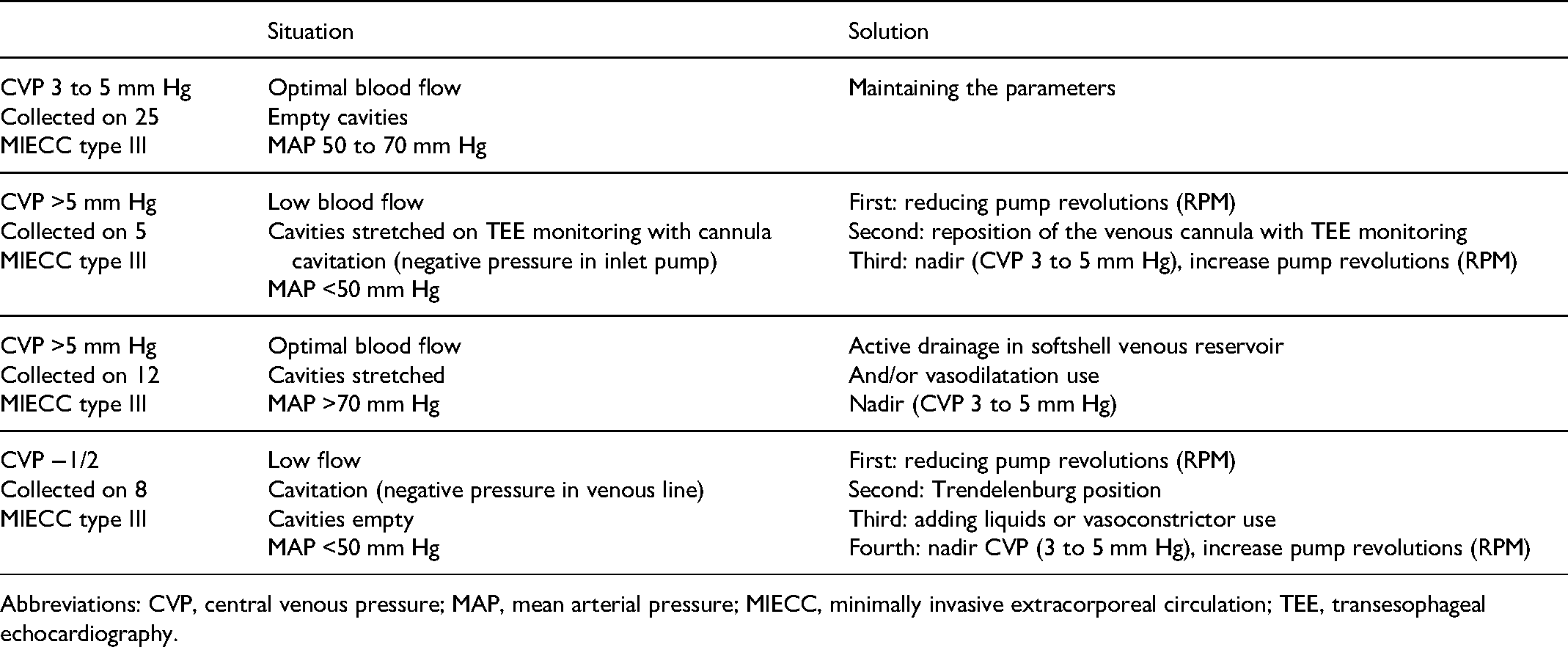
Abbreviations: CVP, central venous pressure; MAP, mean arterial pressure; MIECC, minimally invasive extracorporeal circulation; TEE, transesophageal echocardiography.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.