
Abstract
Keywords
Manipulation in a narrow surgical field and risks of femoral arterial complications are difficulties when applying totally endoscopic surgery for congenital heart disease in small children. We provide technical solutions to overcome these difficulties and follow-up with a long enough time to assess safety.Central Message
Introduction
In the treatment of atrial septal defect (ASD) in young children, transcatheter closure is still the first choice. However, the rate of early and late complications of device closure is higher in children ≤15 kg (including pericardial effusion, atrioventricular block, and mitral valve regurgitation), 1 and some ASDs are unsuitable for intervention (insufficient rims or ASD combined with anomalous pulmonary vein return [APVR]), which has posed a real need for the development of minimally invasive cardiac surgery in small children. However, there are very few reports on the application of minimally invasive approaches in this population, namely, minithoracotomy,2–4 midaxillary approach, 5 and 3 reports on totally endoscopic surgery.6–8
The risk of femoral arterial (FA) complications (compartment syndrome, iliac–femoral artery stenosis or obstruction) and the difficulty of endoscopic manipulation in a narrow surgical field are reasons for the limited use of totally endoscopic surgery in small children. Smaller FA size (due to low weight or young age) increases the risk of FA complications. 8 Meanwhile, the follow-up time in published studies was short (3 to 6 months), so it is possible to miss late FA complications. In this report, we provide technical solutions to overcome the above difficulties and follow-up with a long enough time to assess the feasibility of the technique.
Methods
The ethical committee of our hospital approved the study. Before surgery, all patients and their families were informed about the advantages, disadvantages, and possible complications of the operation. All patients agreed to participate in the study and allowed the use of information as well as images and videos during surgery for scientific purposes.
Patient Selection
Criteria for patient selection included secundum ASDs unsuitable for transcatheter closure and weight ranging from 13 to 20 kg. Excluded from the study were cases with other congenital heart diseases requiring surgery (i.e., right ventricular outflow tract obstruction, ventricular septal defect).
From July 2016 to July 2021, 14 patients who matched the inclusion criteria and did not have any exclusion criteria underwent totally endoscopic surgery for repairing ASD. Preoperative demographic indices (i.e., age, weight, skin area, defect size) and characteristics of pathophysiology are presented in Table 1.
Preoperative Patient Characteristics.
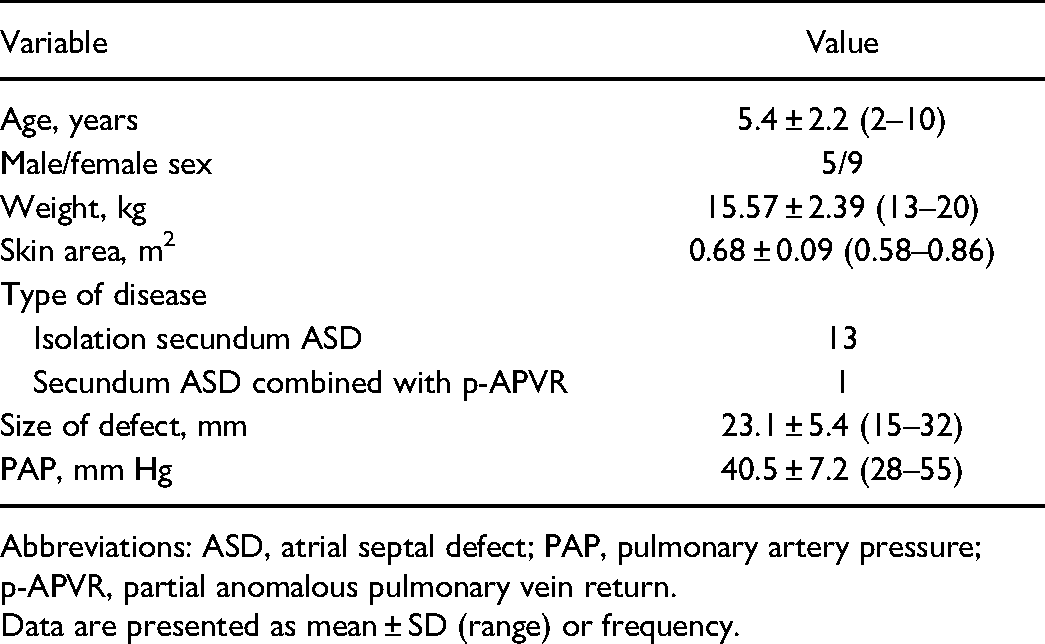
Abbreviations: ASD, atrial septal defect; PAP, pulmonary artery pressure; p-APVR, partial anomalous pulmonary vein return.
Data are presented as mean ± SD (range) or frequency.
Features of Establishing Peripheral Cardiopulmonary Bypass.
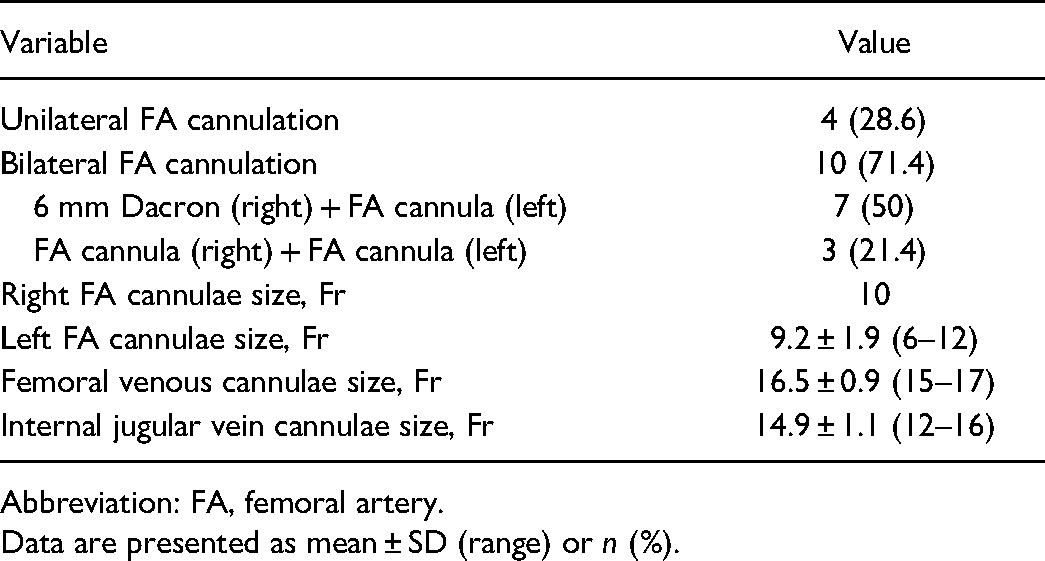
Abbreviation: FA, femoral artery.
Data are presented as mean ± SD (range) or n (%).
Perioperative and Postoperative Parameters.
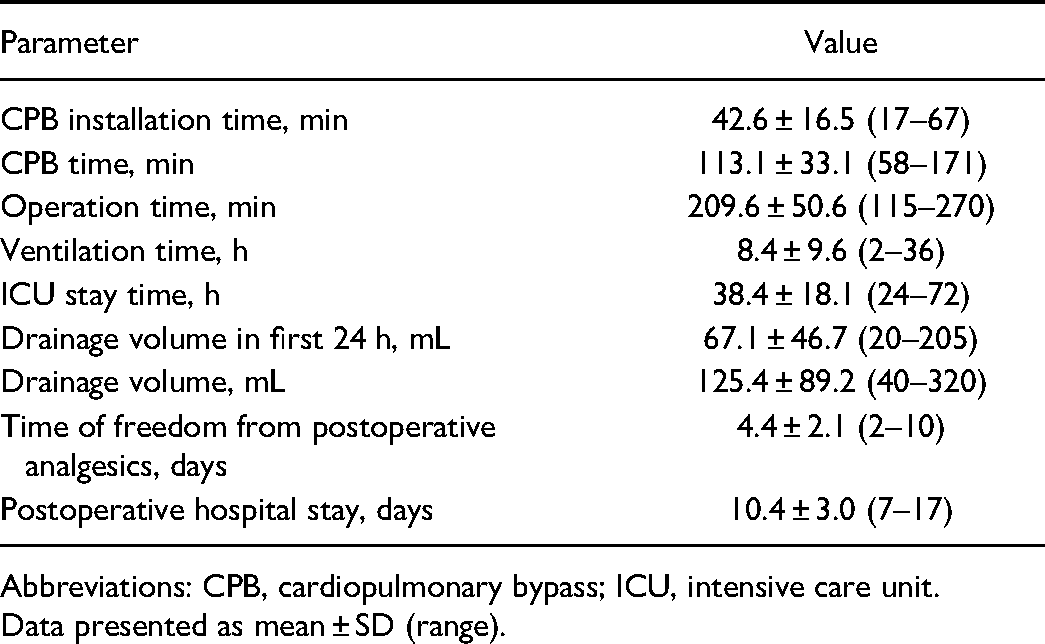
Abbreviations: CPB, cardiopulmonary bypass; ICU, intensive care unit.
Data presented as mean ± SD (range).
Early and Late Complications.
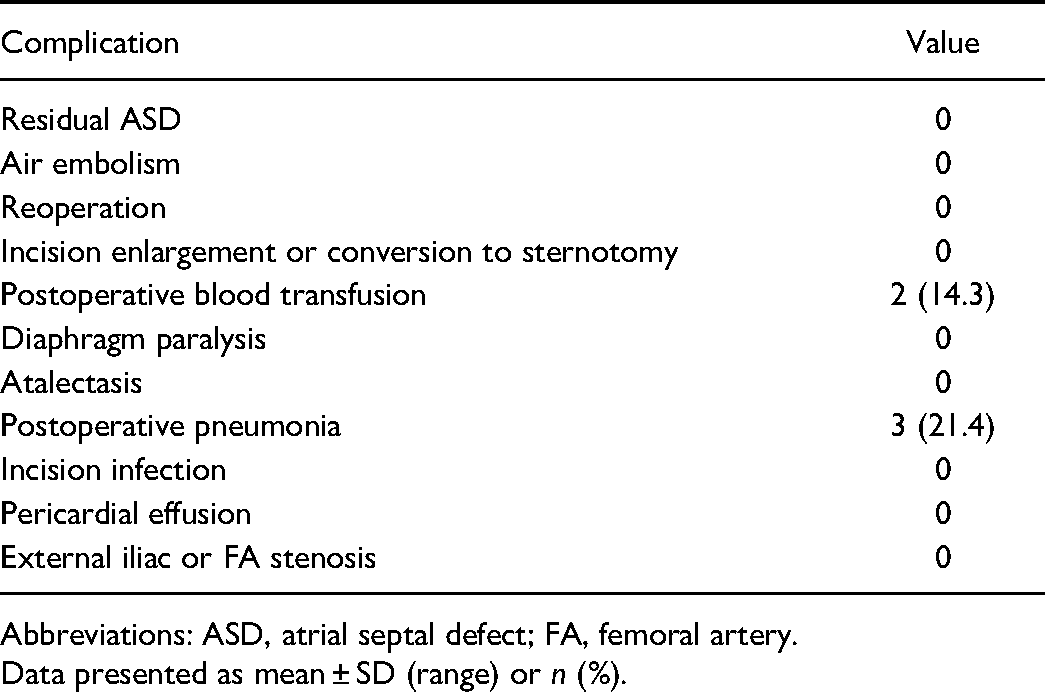
Abbreviations: ASD, atrial septal defect; FA, femoral artery.
Data presented as mean ± SD (range) or n (%).
Operative Technique
All patients were operated on by the same surgeon using an identical surgical protocol.
Anesthesia and patient position
The patient was placed in a supine position with the right side of the body elevated to 30°. The patient’s 2 arms were placed alongside the body, and the patient was administered general anesthesia using a single-lumen endotracheal tube. A central venous catheter was placed through the left internal jugular vein and, a needle for superior vena cava (SVC) guidewire introduction was inserted into the right internal jugular vein.
Peripheral cardiopulmonary bypass cannulation
CAPIOX FX15 Advance Oxygenator with integrated arterial filter (Terumo Cardiovascular, Ann Arbor, MI, USA) was used. We created a 2 cm horizontal incision on the right inguinal fold, revealing the common FA and femoral vein. SVC and inferior vena cava (IVC) cannulae were placed through the right internal jugular vein and femoral vein, respectively, using the Seldinger technique.
For patients weighing ≥15 kg, an arterial cannula was set up indirectly in the right common FA through a 6 mm knitted Dacron graft (Uni-Graft K DV; B. Braun, Tuttlingen, Germany). Before trocar placement, we tested the arterial line by trial running the bypass machine. If the arterial pressure was higher than 240 mm Hg, an additional FA cannula was placed on the left side with a cannula 2 to 4 Fr smaller than the predicted size based on the patient's weight (Fig. 1a). For patients weighing <15 kg, we placed the cannulae directly on both sides, using cannulae 2 to 4 Fr smaller than the predicted size based on the patient's weight (Fig. 1b).
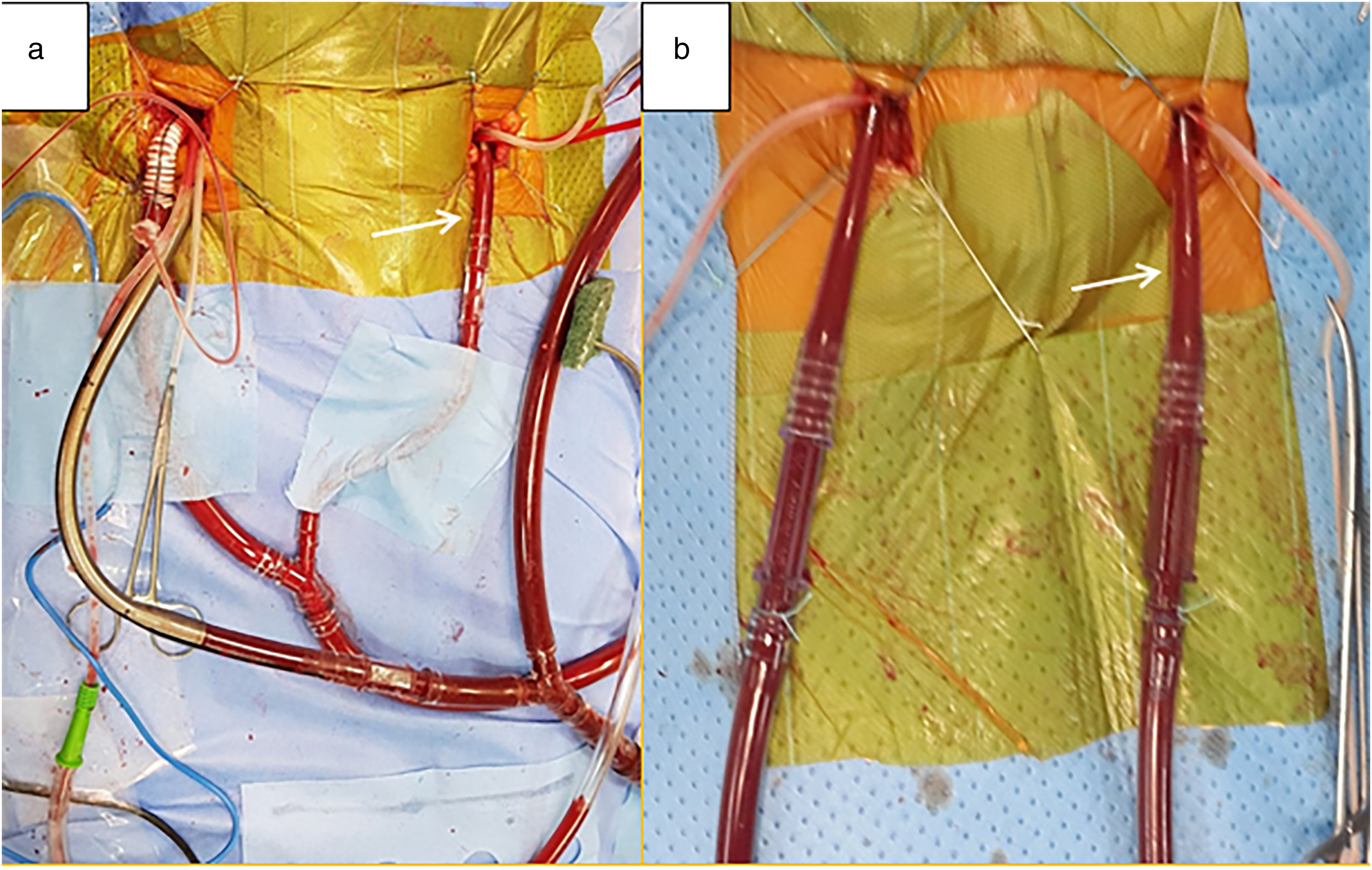
FA cannulation in small children. (a) Establishing bilateral FA cannulation in children weighing ≥15 kg. (b) Establishing bilateral FA cannulation in children weighing from 13 to 15 kg. The white arrow indicates the arterial cannula directly inserted into the left FA in case of increasing arterial pressure. FA, femoral artery.
Totally endoscopic surgery for repairing ASD
Port and trocars on the right chest included the following: (1) a 12 mm main working port at the fifth intercostal space (ICS) on the anterior axillary line, exposure achieved by the smallest size wound protector (SurgiSleeve Wound Protector Extra Small Incision size 2 to 4 cm; Medtronic, Dublin, Ireland), without the use of a rib retractor; (2) a 5.5 mm trocar (Thoracoport 5.5 mm, Medtronic) at the fourth ICS on the midaxillary line for the left-hand instruments; (3) a 5 mm trocar (VersaOne Optical Trocar, Medtronic) at the fifth ICS on the midaxillary line for the endoscopic camera and CO2 insufflation; and (4) another 5.5 mm trocar at the sixth ICS on the midaxillary line for the right heart suction tube (Fig. 2). Right after port/trocars installation, the pleural and pericardial spaces were filled with CO2 at a rate of 2 L/min. The pericardium was opened parallel to and 1 to 1.5 cm away from the anterior chest wall, then along the diaphragm to 1 cm from the diaphragmatic nerve. Afterward, the pericardium was sutured and pulled out through trocars.
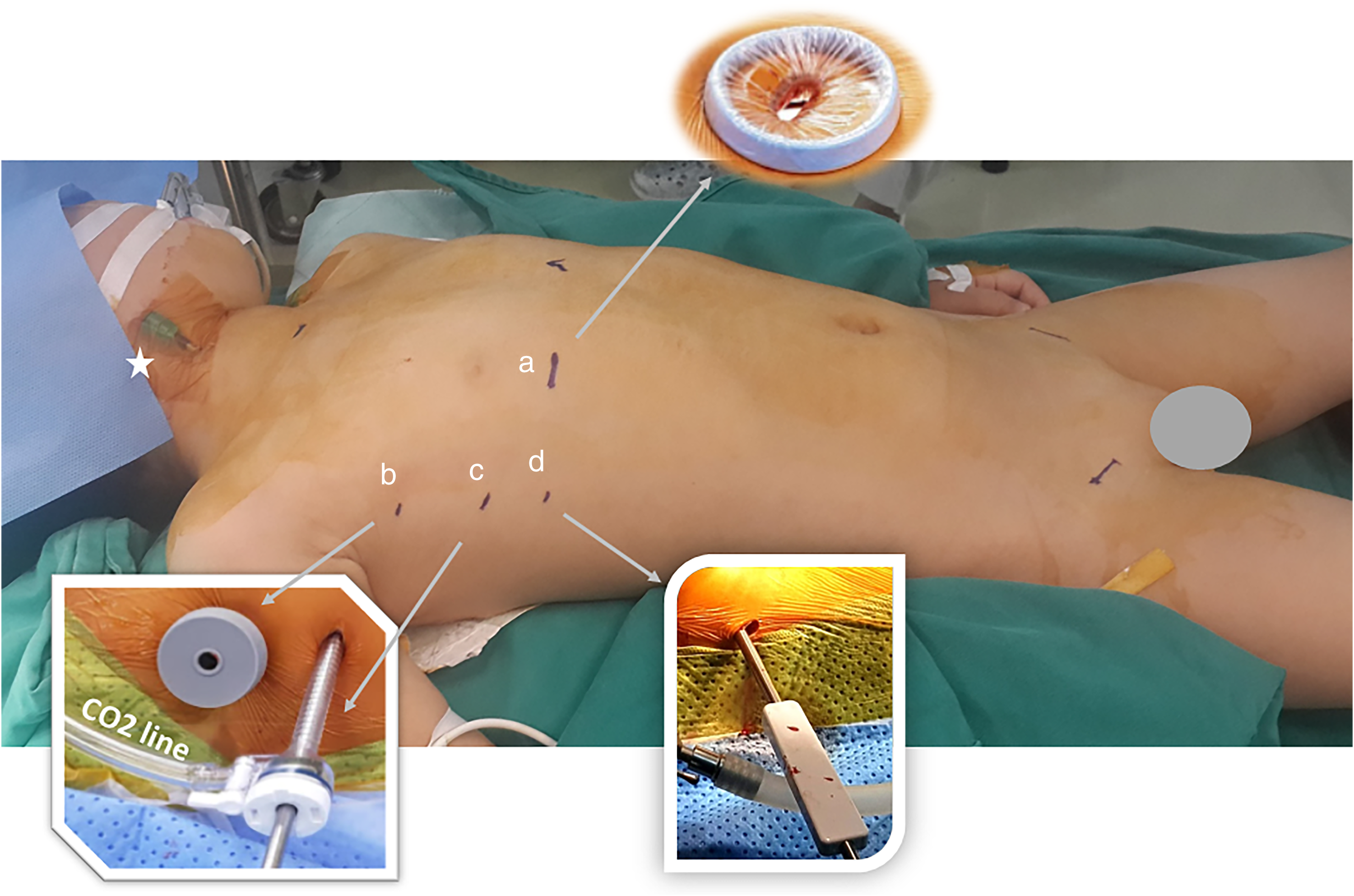
Trocars and port installation. (a) Main working port using the smallest size SurgiSleeve Wound Protector. (b) A 5.5 mm trocar for left-hand instruments. (c) A 5 mm trocar for camera and CO2 line. (d) Last trocar for the right heart suction tube. The white star is the needle for the superior vena cava cannulation.
The patient was placed in the Trendelenburg position, and arterial pressure was maintained at >50 mm Hg. After snaring the SVC (the snare was inserted into the thorax toward the apex of the lung; Supplemental Video 1), the right atrium (RA) was opened and sutured to the pericardium (Supplemental Video 2). The ASD, IVC, coronary sinus position, partial APVR (if present), and tricuspid valve were examined (Supplemental Video 3). The ASD was closed using an artificial patch (Neuro-Patch, B. Braun) by continuous suture (Supplemental Video 4). The left atrium was always kept full of blood during the closing operation. At the end of the ASD closing progress, we still filled the left heart passively through lung expansion to make sure no microemboli were in the left atrium. Posterior annuloplasty was used in cases of moderate or severe tricuspid regurgitation. Blood from the partial APVR (if present) was returned to the left atrium through the ASD by an intracardiac baffle.
The operation time was the duration from skin to skin. The surgery was completed after suturing the RA (Supplemental Video 5), closing the pericardium, and placing 3 drains (14 Fr Covidien suction tubing, Medtronic; 1 pericardial drain and 2 pleural drains).
Postoperative Management
Patients were monitored in the intensive care unit after surgery. Bedside chest x-ray and echocardiography were performed to identify postoperative respiratory complications (atelectasis, pleural effusion) as well as pericardial and pleural hematomas. Complications of postoperative bleeding and air embolism were closely monitored.
Patients were extubated as soon as possible and could be transferred to the normal ward the day after if no special monitoring was required. Analgesia by opioids was used on the first day (morphine) and by oral nonsteroid analgesics on the following days. Patients and their parents were encouraged to stop analgesics as soon as possible. All patients underwent postoperative transthoracic echocardiography and vascular Doppler ultrasound before discharge.
Follow-Up
Follow-up appointments were scheduled at 1 month, 3 months, 6 months, 1 year, and every year after surgery. Surgeons checked and accessed scars, the symmetry between the 2 breasts, paraesthesia around the incision area in the chest and the groin, and the satisfaction of families and patients regarding the location and size of the surgical scars. Patients were examined using transthoracic echocardiography and vascular Doppler ultrasound. The mean follow-up time was 37.9 ± 12.5 months (range, 3–48 months).
Data Analysis
Continuous variables were expressed as mean ± SD and categorical variables as a percentage. Comparisons between groups were performed using t tests for continuous variables and chi-square test or Fisher's exact test for categorical variables. Regression models with logarithmic curve fit were used for learning curve analysis. The results were statistically significant with a P value of <0.05. Data were processed with IBM SPSS Statistics, Version 22.0 (IBM Corp., Armonk, NY, USA).
Results
Bilateral FA cannulation was found in 71.4% of patients. The average size of the cannulae for decompression purposes was 9.2 ± 1.9 Fr (range, 6 to 12 Fr). A 17 Fr femoral venous cannula and a 15 Fr or 16 Fr right internal jugular vein cannula were commonly used (Table 2). Patch closure was used in 13 patients, and direct suture was used in 1 patient. A 10-year-old female patient with preoperative severe tricuspid regurgitation underwent posterior angioplasty. A 4-year-old female patient with ASD combined with right lower APVR underwent repair with an intracardiac baffle.
Cardiopulmonary bypass (CPB) time and operative time appeared to have statistically significant learning curve patterns, which were (ymin = 163.6–28.1ln(x); r2 = 0.433, P = 0.011; Fig. 3) and (ymin = 275.1–36.4ln(x); r2 = 0.309, P = 0.039; Fig. 4), respectively. The patients were on mechanical ventilation for an average of 8 h, stayed in the intensive care unit for 1.5 days, and were discharged after 10 days. Patients did not need analgesics on day 4 or 5 after surgery (Table 3). Pneumonia that prolonged the postoperative treatment time was seen in 3 patients, and postoperative blood transfusion was seen in 2 patients. No severe complications, including FA stenosis or obstruction, were recorded during the follow-up time (Table 4). All parents of the patients were satisfied with the surgical results and the cosmetic value of the scars (Fig. 5).
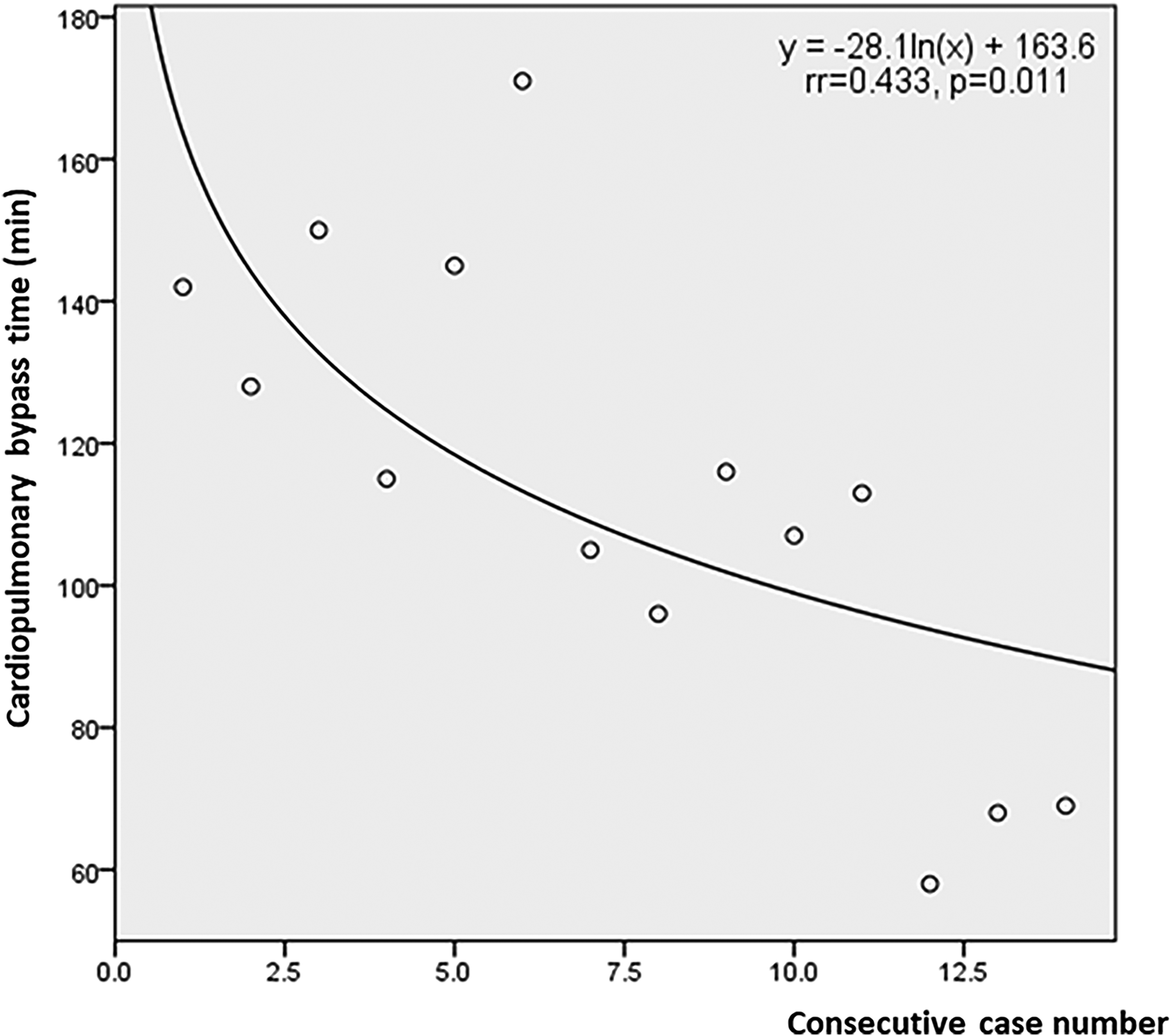
Learning curve for cardiopulmonary bypass time.
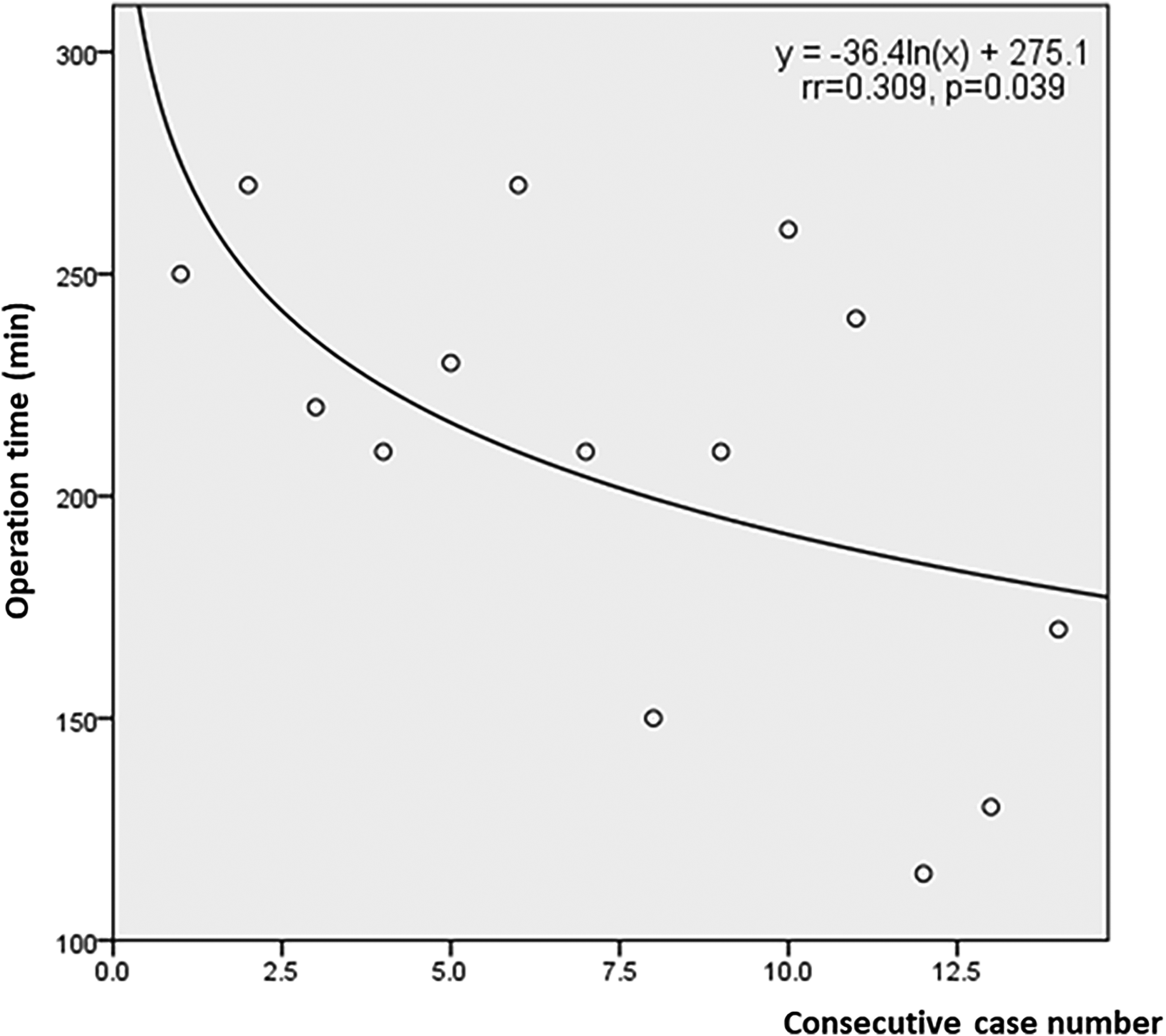
Learning curve for operation time.
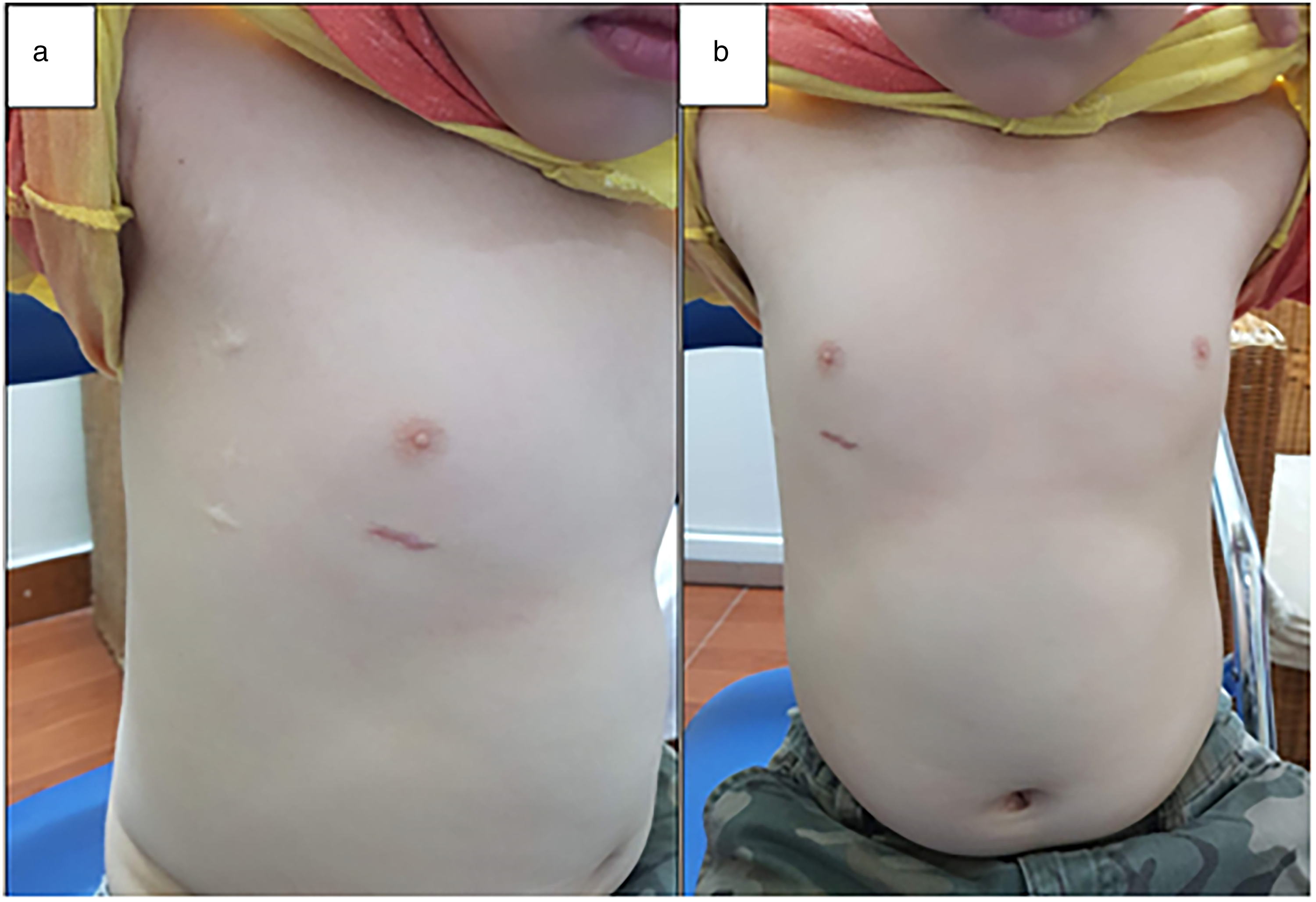
Scars of a 6-year-old boy at 3 years of follow-up.
Discussion
Totally endoscopic ASD closure in small children presents 2 major difficulties, including manipulation in a narrow surgical field and how to safely set up the arterial cannulation for CPB. The surgical field is narrow for some reasons, such as the narrow ICS, 9 small thoracic cavity,7,10 and required transthoracic aortic clamping for myocardial protection due to the inability to use an intra-aortic balloon. 11 Our operative manipulation was favorable thanks to the following technical changes: (1) not using the transthoracic aortic clamp, (2) not using the aortic root needle, (3) not snaring the IVC, (4) the SVC snare was inserted into the thorax toward the apex of the lung so as not to obstruct the surgical field, and (5) not using the 2-stage femoral venous cannula.
In totally endoscopic ASD closure in small children, it is ideal to insert the arterial cannula directly into the ascending aorta through the chest wall. 8 However, this technique is difficult and not suitable for routine application. Direct FA cannulation was applied in the remaining reports;6,7 the size of the cannula chosen was dependent on patient weight. In ASD patients, the FAs are often small, making it difficult to insert the cannula and leading to risks of local complications, including FA dissection, 12 compartment syndrome, 13 and FA pseudoaneurysm. 14 This phenomenon is most often recorded in young women and small children, who often have small FAs associated with a strong spasm reflex of the vascular smooth muscle. 15 The weight limit was ≥13.5 kg, 7 ≥15 kg, 16 or >20 kg 17 depending on the studies.
Direct FA cannulation has an arterial complication rate of 1% to 10% depending on the studies.18–20 These complications may appear immediately during and after surgery or appear late after a period of follow-up. According to Lamelas et al., direct FA cannulation in adults has a 0.07% incidence of compartment syndrome. 21 Although there are no published studies, this rate is likely to be higher in small children. Lower extremity ischemia can be eliminated when arterial blood is bidirectional. 22 The increasing pressure of the arterial line through a Dacron graft connected to the FA, which is caused by small arteries or arterial spasms, can lead to red blood cell rupture or leg edema and hemorrhage in case of prolonged CPB time. An additional arterial cannula inserted into the left FA helped to significantly reduce the arterial pressure, which should be maintained at 224 ± 43 mm Hg according to Nakajima et al. 23 or no more than 250 mm Hg according to Jeanmart et al. 20 and Iino et al. 24 With the maintenance of arterial pressure ≤240 mm Hg, we did not record complications due to increased arterial pressure. The rate of bilateral FA cannulation in adults in our unpublished research was 18.7%—a statistically significant difference compared with the rate of 71.4% in small children patients in this study (P < 0.001).
External iliac or FA stenosis, which is a late complication due to injury of the arterial endothelium during direct FA cannulation, is always recorded from the fifth month postoperatively. 25 Wang et al. did not record this complication with a 3-month follow-up. 7 In this study, for direct arterial cannulation, we chose an arterial cannula that was 2 to 4 Fr smaller than the predicted size to minimize the possibility of endothelial damage during manipulation. The smallest arterial cannula used was 6 Fr. We did not record any late arterial complications during an average follow-up time of 37.9 ± 12.5 months.
To exclude transthoracic aortic clamp Chitwood, ventricular fibrillation (either by hypothermia or electrical fibrillator) and beating heart are good options, among which beating heart is more common. Regarding measures to prevent air embolism, CO2 has a specific gravity that is 1.5 times heavier than air, so in a closed volume, CO2 tends to sink and take the place of air. According to Svenarud et al., in the case of clamping aorta, CO2 significantly reduces the number of microemboli in the left heart chambers (left atrium, left ventricle, and proximal ascending aorta) in comparison with traditional de-airing methods. 26 Moreover, the number of microemboli also decreases and disappears faster (within 3 to 5 min) in the CO2 group than in the conventional de-airing group, because CO2 is ≥25 times more soluble in blood and tissue than in air. 26 According to Martens et al., the minithoracotomy required CO2 injection at a flow of 2 L/min to achieve a CO2 concentration of 92% ± 6%. 27 Increasing the CO2 flow did not increase but conversely decreased CO2 concentrations in the surgical field.27–29 On the other hand, limiting the use of suction devices in the surgical field 28 and keeping the negative pressure for IVC drainage ≤40 mm Hg also contributes to maintaining CO2 concentrations. In this study, we always kept the left atrium full of blood, which eliminated the trapped air in the pulmonary veins. In addition, maintaining a high arterial pressure during the ASD closure phase played an important role in keeping the aortic valve closed. At the end of the ASD-closing progress, we still filled the left heart passively through lung expansion to make sure no microemboli were in the left atrium. With the above measures, no cases of air embolism were recorded in this study.
In this study, we recognized that the preoperative weight of the patients influenced the operation times. However, because of the small number of patients, we were unable to divide the patients into groups to demonstrate this. Therefore, we stopped at only the most basic analysis of the learning curve. The postoperative hospital stay time in our study was long for 2 reasons: (1) our hospital does not allow patients to be discharged on weekends (Saturday and Sunday) and (2) postoperative respiratory tract infections. In this study, we recorded 3 patients with postoperative pneumonia, and most of the other patients had upper respiratory tract infections that required antibiotic treatment. The prolonged postoperative hospital stay time of totally endoscopic surgery for ASD closure in small children was not only found in our study. Wang et al. also noted that the postoperative hospital stay time ranged from 6 to 10 days for subjects weighing 13.5 to 22 kg. 7
We found some advantages of totally endoscopic surgery in our study, including less pain and less blood loss. The amount of blood drained in the first 24 h was 67 mL in our research compared with 400 to 600 mL in studies using sternotomy approach.30,31 Regarding analgesia, our patients did not need analgesics on day 4 or 5 after surgery. Meanwhile, Ma et al. reported that 62.5% of patients in the sternotomy group suffered moderate to severe pain at the time of discharge (mean 6.9 days after surgery). 32
Conclusions
By optimizing the surgical field and setting the FA cannula correctly, totally endoscopic surgery for ASD closure is feasible in small children weighing between 13 and 20 kg.
Supplemental Material
Visual abstract - Supplemental material for Intermediate-Term Outcomes of Totally Endoscopic Atrial Septal Defect Repair on Beating Heart in Small Children
Supplemental material, sj-pptx-1-inv-10.1177_15569845221102179 for Intermediate-Term Outcomes of Totally Endoscopic Atrial Septal Defect Repair on Beating Heart in Small Children by Uoc H. Nguyen, Huy Q. Dang, Huu C. Nguyen and Thanh N. Le in Innovations: Technology and Techniques in Cardiothoracic and Vascular Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.