
Abstract
A 76-year-old male patient was referred to our institution with moderate-to-severe aortic and mitral insufficiency. The patient underwent totally endoscopic robot-assisted aortic valve replacement and mitral valve repair. In this article, we present our lateral approach to the robotic double valve surgery.
Introduction
The safety and efficacy of robotic mitral valve repair (rMVr) have been well-established. 1 Yet, robotic aortic valve replacement (rAVR) remains a nascent frontier in minimally invasive cardiac surgery (MICS). A recent case series demonstrated successful rAVR with conventional prostheses using a lateral approach. 2 However, previous reports were limited to small rAVR case series using sutureless valves via an anterior–medial approach3,4 or isolated MV or AV procedures. Concomitant rAVR and rMVr remains an infrequent procedure, although it has been previously described. Here, we demonstrate our lateral approach to totally endoscopic robot-assisted AVR and MVr.
Case Report
A 76-year-old man with symptomatic aortic and mitral insufficiency was referred to our institution. Echocardiography revealed moderate-to-severe aortic and mitral regurgitation with maintained left ventricular function (ejection fraction = 58%). Cardiac catheterization showed nonobstructive coronary artery disease (CAD). Computed tomography (CT) angiography demonstrated the absence of mitral annular calcification, aortic atherosclerosis, and pleural/diaphragmatic abnormality. Arterial anatomy was favorable for femoral cannulation. The patient expressed interest in robotic double valve surgery. Normal chest wall anatomy and body mass index were amenable for rAVR with rMVr.
General anesthesia was initiated in standard fashion with right lung isolation. A single-lumen central line was placed in the right internal jugular (IJ) catheter for use during bicaval cannulation. The right chest was elevated and draped. Figure 1 depicts our port placement. An 8-mm camera port was placed in the right fourth intercostal space (ICS) along the anterior axillary line. An 8-mm retractor port was placed medial to the camera port. Two 8-mm arm ports were placed in the third and sixth ICS at the midclavicular line. The 30-mm working port was placed in the fourth ICS 2 cm lateral to the camera port for AV placement into the chest.
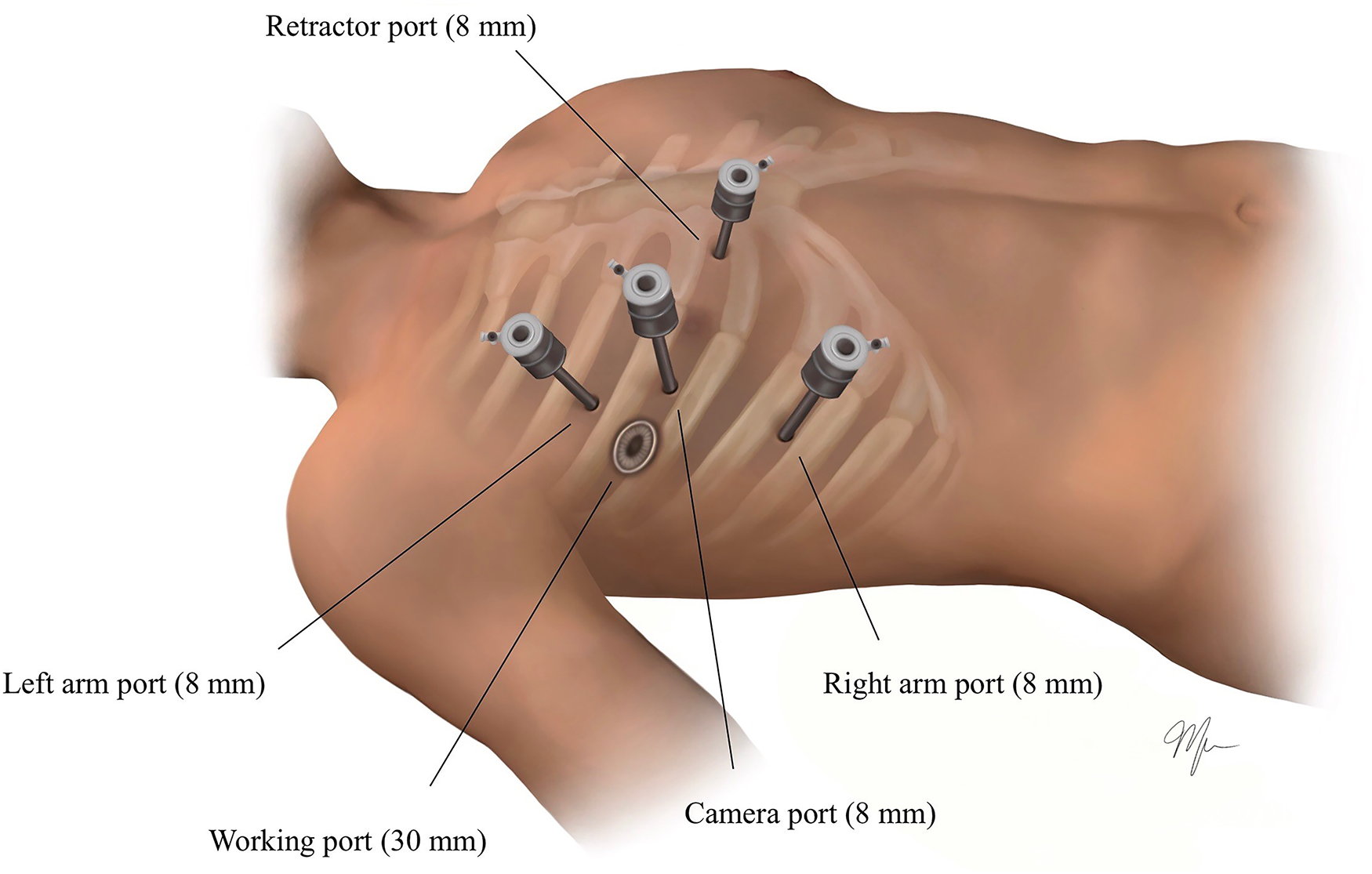
Port placement. An 8-mm camera port in the right fourth ICS along the anterior axillary line. An 8-mm retractor port medial to the camera port in the fourth ICS. Two 8-mm arm ports in the third and sixth ICS at the midclavicular line. The 30-mm working port in the fourth ICS 2 cm lateral to the camera port. ICS, intercostal space.
The right femoral vessels were accessed percutaneously under ultrasound guidance. A right common femoral digital subtraction arteriogram confirmed sheath placement in the common femoral artery (CFA). Heparin was administered. Under fluoroscopy and transesophageal echocardiography (TEE) guidance, a Glidewire (Terumo, Somerset, NJ, USA) was positioned in the superior vena cava (SVC). Using the Seldinger technique, the Glidewire was exchanged for an Amplatzer Super Stiff guidewire (Boston Scientific, Marlborough, MA, USA), and the tract was dilated to accommodate a 24-F femoral venous cannula. The femoral artery was accessed with the same technique and dilated to accommodate a 20-F OptiSite arterial cannula (Edwards Lifesciences, Irvine, CA, USA). The cannulae were appropriately de-aired, secured, and connected to the bypass circuit. The SVC was cannulated by exchanging the right IJ catheter with a 17-F drainage catheter for bicaval drainage. The robot was docked, and the instruments were inserted under direct camera vision.
A right hemidiaphragm retraction suture was placed and exteriorized laterally. The right intercostal nerves (T3 to T9) were cryoablated to minimize postoperative pain. Pericardiotomy was performed and cardiopulmonary bypass (CPB) initiated. Pericardial retraction sutures were placed and exteriorized laterally. The Chitwood aortic cross-clamp was placed. Retrograde del Nido cardioplegia was given through a right IJ cardioplegia cannula. An aortotomy was performed with direct cardioplegia to the left main and right coronary arteries. Cardiac arrest was achieved.
A left atriotomy was created, and the sump drain was placed in the left pulmonary veins (Fig. 2a). The atrial retractor provided further exposure. The left atrial appendage was closed with a double-layer 3-0 V-loc suture (Medtronic, Minneapolis, MN, USA). Static testing of the MV confirmed Barlow's valve with bileaflet prolapse. Two sets of neochords were placed to prevent systolic anterior motion (SAM) and posterior prolapse. rMVr with remodeling annuloplasty was performed using the Medtronic SimuPlus flexible band, size 36, placed with 2 nonresorbable 3-0 V-loc sutures in a running horizontal mattress with each suture starting at the trigones, meeting in the middle of P2, then secured to the band (Fig. 2b). The posterior annulus was secured with an everting pledgeted 2-0 Ethibond mattress suture (Ethicon, Raritan, NJ, USA) secured to the annuloplasty band with a Cor-Knot Device (LSI Solutions, Victor, NY, USA). Static testing revealed a competent valve with posterior coaptation. The vent was placed across the MV into the left ventricle. The left atrium was closed with 2 nonresorbable 3-0 V-loc sutures starting from each end of the atriotomy, then run to the middle and tightened around the vent.
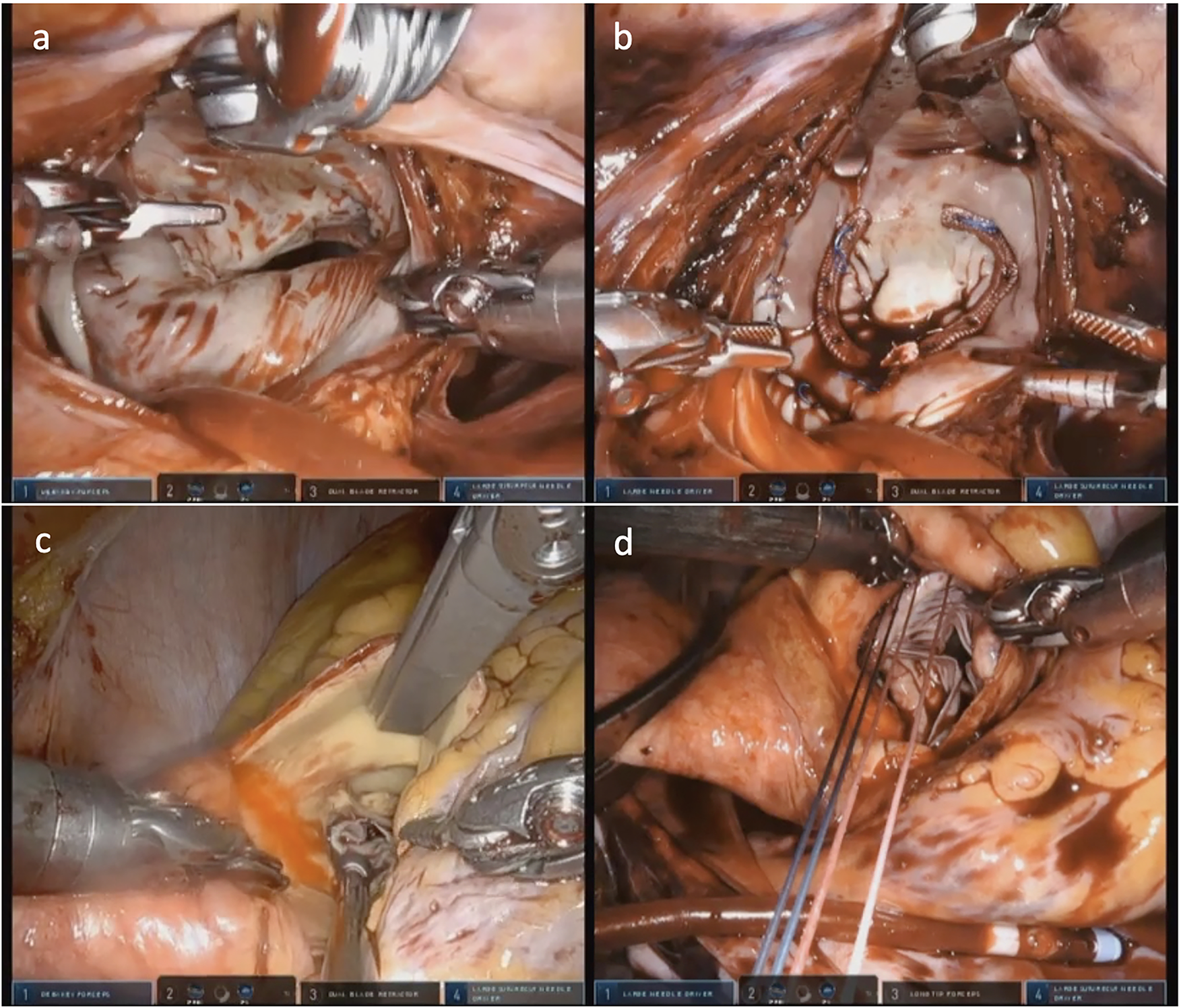
(a) Left atriotomy created with robotic scissors revealed excessive posterior leaflet prolapse. (b) Mitral valve repair with remodeling annuloplasty band placed with V-loc sutures. (c) Spiral aortotomy extended toward the noncoronary sinus showed prolapsed aortic valve leaflets. (d) Aortic valve prosthesis placed through the lateral working port was secured with circumferential sutures and the Cor-Knot device (LSI Solutions, Victor, NY, USA).
The aortotomy was extended toward the noncoronary sinus (Fig. 2c), revealing prolapsed AV leaflets that were excised with robotic scissors. The annulus was sized, and a 25-mm Epic porcine valve (St. Jude Medical, Saint Paul, MN, USA) was placed with circumferential 2-0 pledgeted Ethibond sutures that were secured with the Cor-Knot (Fig. 2d). The aortotomy was closed with two 3-0 V-loc sutures starting from each end and run to the middle. The ends of the 2 sutures were secured with the Cor-Knot. The aortotomy was further reinforced with interrupted 3-0 Prolene pledgeted mattress sutures.
After de-airing maneuvers, the cross-clamp was removed. A ventricular pacing wire and pericardial drain were placed. The left atriotomy and aortotomy suture lines were inspected and found to be hemostatic. The pericardium was loosely approximated with a 3-0 nonresorbable V-loc suture. The port sites were checked for bleeding, the robotic instruments were removed, and both lungs were slowly ventilated. The patient was easily weaned from CPB. The cross-clamp time was 188 min, and the CPB time was 246 min. Intraoperative TEE showed a well-seated AV prosthesis without paravalvular regurgitation (PAR), mitral regurgitation, SAM, or wall motion abnormalities and with normal biventricular function.
After undocking the robot, the patient was decannulated. A Bentson wire was placed across the arterial cannula in the right CFA. Protamine was given. An 8-F Angio-Seal (Terumo) was placed with wire removal, and the 2 ProGlides were tightened, locked, and cut. The venous cannula was removed, and the 2 venous ProGlides were tightened, locked, and cut. Hemostasis was achieved. Completion ultrasound of the right CFA showed good flow. The SVC drainage catheter was removed, and the percutaneous purse string was tightened with a Rumel tourniquet. Right video thoracoscopic re-exploration of the chest ensured good hemostasis. A right pleural drain was placed. Port and groin puncture sites were closed in standard fashion.
The patient was discharged to acute rehab on postoperative day 8. He was recovering well at 1-month follow-up.
Discussion
This was our institution's first rAVR with rMVr. While concomitant robotic mitral and tricuspid valve repair has been performed safely and reproducibly, 5 fewer combined robotic mitral and aortic valve procedures have been documented. The advantages of our lateral approach were previously described. 6 Our technique promoted postoperative pain reduction by avoiding rib spreading in combination with cryoablation nerve block, which is associated with significant reductions in pain scores and lower request for pain medication. 7 The use of V-loc sutures eliminated knot tying to maximize efficiency within the limited working space.
CT has preoperative utility in MICS and robotic procedures as a screening tool for CAD, aortic atherosclerotic plaques, aorto-iliac atherosclerosis, mitral annular calcification, pleural plaques/adhesions, and aberrant anatomy, which may identify patients contraindicated for rAVR with rMVr. CT-obtained annular diameter and area can be used to predict PAR, which is associated with increased morbidity and mortality after transcatheter AVR. 8 Moreover, the 30-mm working port allows the use of conventional prostheses, which have greater durability than transcatheter AVR and MVR valves. This may make rAVR with rMVr appropriate for patients who are ineligible for transcatheter tissue valves.
The lateral approach has immense potential for combined valve procedures. Further technological innovation, investment in personnel training, and large-scale studies comparing traditional and robotic approaches are key to establishing the safety and efficacy of this procedure.
Supplemental Material
Visual abstract - Supplemental material for Totally Endoscopic Robot-Assisted Aortic Valve Replacement and Complex Mitral Valve Repair: The Lateral Approach
Supplemental material, sj-pptx-1-inv-10.1177_15569845221106939 for Totally Endoscopic Robot-Assisted Aortic Valve Replacement and Complex Mitral Valve Repair: The Lateral Approach by Daniella H. Wong, Colin C. Yost, Jake L. Rosen, Meagan Wu and T. Sloane Guy in Innovations: Technology and Techniques in Cardiothoracic and Vascular Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Guy is a consultant for Edwards Lifesciences, Medtronic, and a case observation site and proctor for Intuitive Surgical.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.