
Abstract
Bipolar esophageal exclusion is a “Hail Mary” procedure for control of leak and persistent mediastinal soilage from esophageal injury. Usually, the esophageal remnant scars down without negative consequences. Esophageal mucocele is a rare complication of bipolar esophageal exclusion. This is a case report of an iatrogenic esophageal transection and the subsequent treatment course. A retrospective chart review of the patient’s medical and surgical history was performed. After a robotic hiatal hernia repair at an outside institution, the patient suffered an esophageal leak and was surgically treated with esophageal exclusion, wide drainage of the mediastinum, and decortication of the resulting empyema. She subsequently underwent retrosternal gastric conduit for esophageal reconstruction 4 months later. Three years after this, she developed a rare complication of esophageal exclusion, a symptomatic esophageal mucocele that required resection.
Introduction
Esophageal injury is a challenging, life-threatening condition that requires aggressive surgical intervention early on for a successful outcome. This may require bipolar exclusion with esophagostomy and distal transection. Although this would invariably fail in any other segment of the gastrointestinal tract, the lack of significant excretory function of the esophagus allows for this unusual surgical treatment to be successful in the vast majority of cases. Development of a mucocele—a pathologic dilation of the excluded segment with secretions—is exceedingly rare. Here we present one such case and the treatment thereof.
Case Report
A 70-year-old woman underwent an elective robotic hiatal hernia repair at an outside facility for a large, type III paraesophageal hernia with organoaxial and mesoaxial volvulus. A postoperative esophageal leak required a return to the operating room. Attempted repair was unsuccessful, and she was transferred to our institution with uncontrolled sepsis. After resuscitation, she underwent robotic bipolar esophageal exclusion with feeding gastrostomy. Full esophageal resection was not attempted due to the patient’s critical condition. A week later, she required thoracoscopic debridement and decortication of a right-sided empyema and a tracheostomy. After a prolonged hospital course of 4 weeks, she was discharged to a skilled nursing facility on tube feeds and trach collar.
Four months later, she underwent extra anatomic retrosternal esophageal reconstruction. 1 The cervical esophagostomy was mobilized. The left sternoclavicular joint was resected. After extensive lysis of adhesions with robotic assistance, the gastric conduit was prepared by taking down the gastrostomy and performing a pyloromyotomy. The diaphragm was divided at its insertion on the xiphoid. The substernal tunnel was developed to the thoracic inlet, connecting to the cervicotomy dissection plane. A Penrose drain was pulled into the abdomen, secured to the conduit and the conduit was pulled into the retrosternal location. A feeding jejunostomy was created before undocking the robot. The cervical esophagogastrostomy was then created with an EndoGIA stapler (Medtronic, Dublin, Ireland), and a side-to-side functional end-to-end fashion as has previously been described. 2 Her postoperative course was uncomplicated, and she was discharged home on postoperative day 7.
She returned to the office 3 years later after workup by her primary care physician for dysphagia and chest pain, which revealed a large mediastinal mass diagnosed on cross-sectional imaging as an esophageal mucocele (Fig. 1). The decision was made to proceed with resection. Prior to docking the robot, she required extensive thoracoscopic lysis of adhesions due to her previous empyema. After complete lung mobilization, the mucocele was exposed. It was encircled with a Penrose drain and mobilized circumferentially up to the thoracic inlet superiorly. Distally, the dissection was difficult due to petrification of the retained barium and obliviated tissue planes. The lumen was entered, and white mucus was removed, decompressing the esophagus. The distal esophagus was then transected and removed (Fig. 2). The small remaining patch of distal esophageal mucosa was ablated with cautery. She progressed well postoperatively and was discharged to home 8 days after surgery. Final pathology results were benign and showed multinucleated giant cells, chronic inflammation, fibrosis, and Barium crystals. She was seen in follow-up and is doing well with resolution of her symptoms. Although the source of dysphagia could not be explained based on the anatomic relationship between the conduit and the mucocele, late onset of the problem and resolution after the procedure suggest a causative relationship, perhaps on a neural or reflexogenic basis.
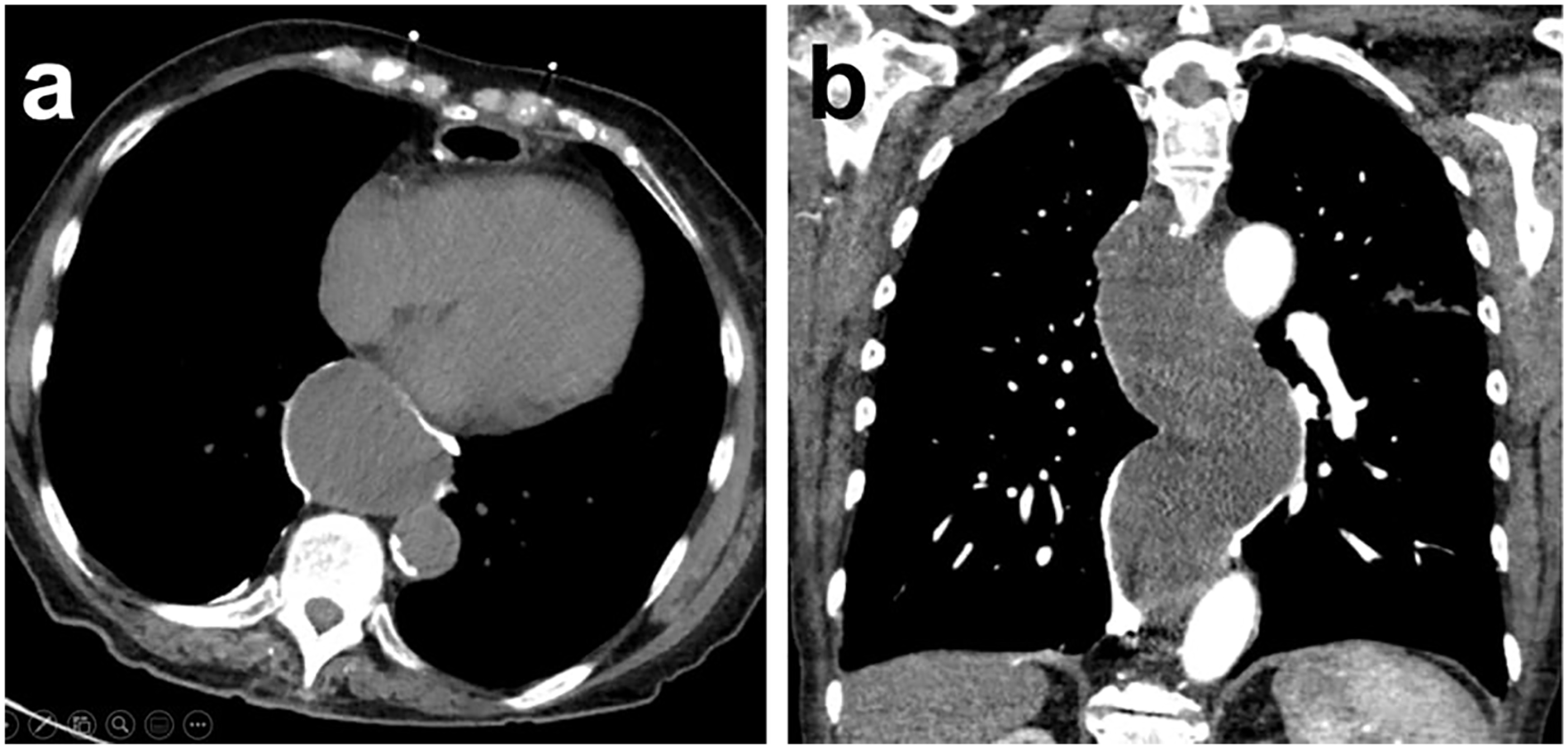
Cross-sectional imaging demonstrating esophageal mucocele. (a) Axial reconstruction, (b) coronal reconstruction.

Gross image of the esophageal specimen.
Discussion
Recent developments in endoscopic and radiologic interventions for the perforated esophagus have brought significant success in the management of this feared condition. As such, esophageal diversion with bipolar exclusion is now a rare procedure, used only as a last resort to control persistent esophageal leak and ongoing mediastinal/thoracic soilage. Usually, these patients are so profoundly unstable due to sepsis that they would not tolerate a more invasive procedure, such as an esophagectomy. This procedure carries significant quality-of-life implications due to cervical esophagostomy and enteral feeding dependance, and those who survive desperately seek a reconstruction. Reconstruction is difficult, demanding an extra-anatomic conduit placement. As such, esophageal exclusion is regarded as a “Hail Mary” procedure, used only in desperate situations.
Most of the time, retained esophageal segments scar down without subsequent complications. The development of an esophageal mucocele is an exceedingly rare complication, with the most recent literature review finding a mere 17 adult cases. 3 It is hypothesized that the glands along the esophagus cease to produce secretions due to the buildup of even minimal pressure and are self-limited. 4 A case of symptomatic mucocele development followed by resolution with expectant management lends credence to this theory. 5 In rare instances of mucocele development, internal drainage 3 and external drainage 6 have been employed, but resection is the most common and sensible procedure to be performed. Most commonly, this is accomplished via thoracotomy, though thoracoscopic management has been reported on 2 occasions.7,8 We believe the development of the mucocele in the present case was due to retained Barrett’s mucosa due to long-standing reflux in the patient with paraesophageal hernia. Although our specimen failed to show any persistent Barrett’s metaplasia on pathology, we are suspicious that the segment that was left in situ and was ablated with electrocautery would have shown a persistent segment of Barrett’s mucosa. Although this patient developed an esophageal mucocele after bipolar exclusion, we believe there is no role for routine monitoring for mucocele development with cross-sectional imaging due to extreme rarity of the condition and a significant lead time.
Application of the robotic technology allowed this case to proceed minimally invasively without conversion at all stages of her care and, specifically, despite overwhelming, carpet-like intrathoracic adhesions from previous empyema. Rapid development and continued refinement of the robotic technology affords continued expansion of the minimally invasive realm in the hands of expert surgeons.
Supplemental Material
Visual abstract – Supplemental material for A Rare Complication of Esophageal Exclusion: Esophageal Mucocele
Supplemental material, sj-pptx-1-inv-10.1177_15569845221124131 for A Rare Complication of Esophageal Exclusion: Esophageal Mucocele by Jonathan A. Nitz, Charles T. Bakhos, Roman V. Petrov and Abbas E. Abbas in Innovations: Technology and Techniques in Cardiothoracic and Vascular Surgery
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.