
Abstract
Objective:
Barbed nonabsorbable sutures have been widely adopted for tissue closure in noncardiac robotic surgery to improve intraoperative efficiency. Here, we examine the profile in robotic mitral valve repair (rMVR), which utilized barbed nonabsorbable sutures. To our knowledge, this is the first report to describe clinical outcomes for rMVR with barbed nonabsorbable sutures.
Methods:
A retrospective review identified 90 patients who underwent rMVR using barbed nonabsorbable sutures at our center between 2019 and 2021. The primary outcome measure was dehiscence, while other relevant outcomes included 30-day readmission and 30-day mortality.
Results:
In addition to fixation of the mitral annuloplasty band, barbed nonabsorbable sutures were employed commonly in concomitant pericardiectomy closure (100.0%, 90 of 90), atriotomy closure (100.0%, 90 of 90), and left atrial appendage closure (if eligible; 98.8%, 83 of 84). One patient who underwent mitral valve annuloplasty using only barbed nonabsorbable suture required reoperation for annuloplasty ring dehiscence. Immediate postoperative ring dehiscence was not observed in any patients after the routine reinforcement of barbed nonabsorbable sutures with everting pledgeted polyester sutures, and no additional patients required reoperation for suture-related complications. Clinical signs of dehiscence were not observed after pericardiectomy, atriotomy, or left atrial appendage closure with barbed nonabsorbable sutures. The 30-day readmission rate was 3.3% (3 of 90), and 30-day mortality was 0% (0 of 90).
Conclusions:
These data suggest the initial feasibility of barbed nonabsorbable sutures in robotic cardiac surgery, specifically within rMVR. Further research is necessary to explore the long-term safety and efficacy profile of such approach.
Central Message
For patients undergoing robotic mitral valve repair by an experienced surgeon, cases in which barbed nonabsorbable sutures were employed were found to have generally low rates of dehiscence, 30-day readmission, and 30-day mortality.
Introduction
Robotic cardiac surgery is a rapidly evolving minimally invasive approach to repairing the heart. Among its many advantages, robotic cardiac surgery has demonstrated shorter length of stay and fewer perioperative and postoperative complications with no significant difference in mortality compared to traditional median sternotomy approaches.1–4 Additionally, the robotic approach has demonstrated comparable operative cost to traditional sternotomy and thoracotomy when total hospitalization cost is considered.5,6 Especially for robotic mitral valve repair (rMVR) and replacement, the robotic approach has become the method of choice for many centers with robotic capabilities. 7
Despite the numerous benefits, an unresolved downfall to robotic cardiac surgery is procedure length, which remains longer than comparable nonrobotic operations.1,4 Robotic platforms often require the console surgeon to scrub in and out of the procedure for various steps, including for port setup and mechanical suturing. Operative time is further increased during the initial phases of a new robotic program given the significant learning curve among team members.8,9 Therefore, ongoing innovation to decrease operative time is an important consideration for robotic cardiac surgery. Abbreviating the lengthy process of mechanical suturing presents a key opportunity to decrease operative time. Accordingly, barbed sutures pose a potential solution to improving suture efficiency.
Barbed sutures were first proposed by Dr. John Alcamo in 1967 in an effort to increase intraoperative efficiency. 10 Since then, they have been made commercially available and are heavily utilized in several noncardiac fields, including orthopedics, obstetrics, gynecology, and plastic surgery.10–14 Among the several barbed options, the polybutester V-loc™ Wound Closure Device (Medtronic, Dublin, Ireland) has been used in robotic cardiac surgery. 15 The nonabsorbable suture consists of a monofilament with barbs along its length to restrict backsliding, similar to the mechanism of an everyday zip tie. This design also eliminates knot tying, a chief benefit for operative efficiency. The suture can be easily deployed and tightened by the robotic arm, preventing the need for mechanical suturing at various steps. For instance, V-loc™ sutures have been suggested to reduce procedural length compared to traditional interrupted sutures when fastening the mitral annuloplasty band. 15
Despite widespread documentation of improved operative efficiency,10,14,16,17 the use of barbed sutures in cardiac surgery is poorly documented. Aside from technique publications, real-world data on the use of barbed sutures in robotic cardiac surgery inside the thoracic cavity are virtually nonexistent.15,18 However, robotic cardiac surgery poses plentiful opportunities for barbed suture implementation. In addition to the previously mentioned fastening of the mitral annuloplasty band during rMVR, our center uses barbed sutures for several operative steps including pericardial and atrial reapproximation and left atrial appendage closure, among others. In this single-center retrospective review of 90 patients, we provide the first known outcome report for patients undergoing rMVR using V-loc™ barbed nonabsorbable sutures.
Methods
Study Design
We conducted a retrospective review of 90 patients who underwent robotic cardiac surgery and received barbed nonabsorbable sutures for rMVR annuloplasty band fixation at our center between July 2019 and December 2021. After identification, relevant patient data were extracted from the Society of Thoracic Surgeons (STS) database according to protocol approved by the Institutional Review Board. Due to the retrospective nature of our study, informed consent for patient information was waived.
Outcome Measures
The primary outcome measure was dehiscence of the annuloplasty band for which barbed sutures were used. Other notable measures included 30-day mortality (particularly mortality due to a suture-related complication), 30-day readmission, intensive care unit (ICU) length of stay, and postoperative complications such as stroke, tamponade, pericardial effusion, and hemothorax. Thirty-day readmission was captured through manual chart review, which identified all hospital admissions within 30 days of the date of discharge after the index procedure. These admissions were then screened for relevance to the cardiac index procedure, and “readmission” was defined as inpatient admission for a reason directly related to postoperative complications (stroke, atrial arrhythmia, peripheral vascular complications). Patients were stratified based on number of concomitant procedures for the purpose of presenting median operative and cardiopulmonary bypass (CPB) times.
Statistical Analysis
Continuous variables were presented as median (interquartile range), while categorical variables were presented as frequencies and proportions (%, n of N). R version 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria) was used for all statistical analysis.
Results
Patients
The median patient age was 65.00 (56.25, 72.00) years, and the median STS predicted risk of mortality score was 0.50% (0.28%, 0.88%). The most common preoperative comorbidities were hypertension (64.4%, 58 of 90), atrial fibrillation (27.8%, 25 of 90), and heart failure (17.8%, 16 of 90). Other preoperative comorbidities included coronary artery disease (17.8%, 16 of 90), prior stroke (6.7%, 6 of 90), and diabetes (6.7%, 6 of 90). Current everyday smokers accounted for 5.6% of the included patients (5 of 90), and 5.6% had history of myocardial infarction. Full patient demographic information is provided in Table 1.
Patient Demographic Information.
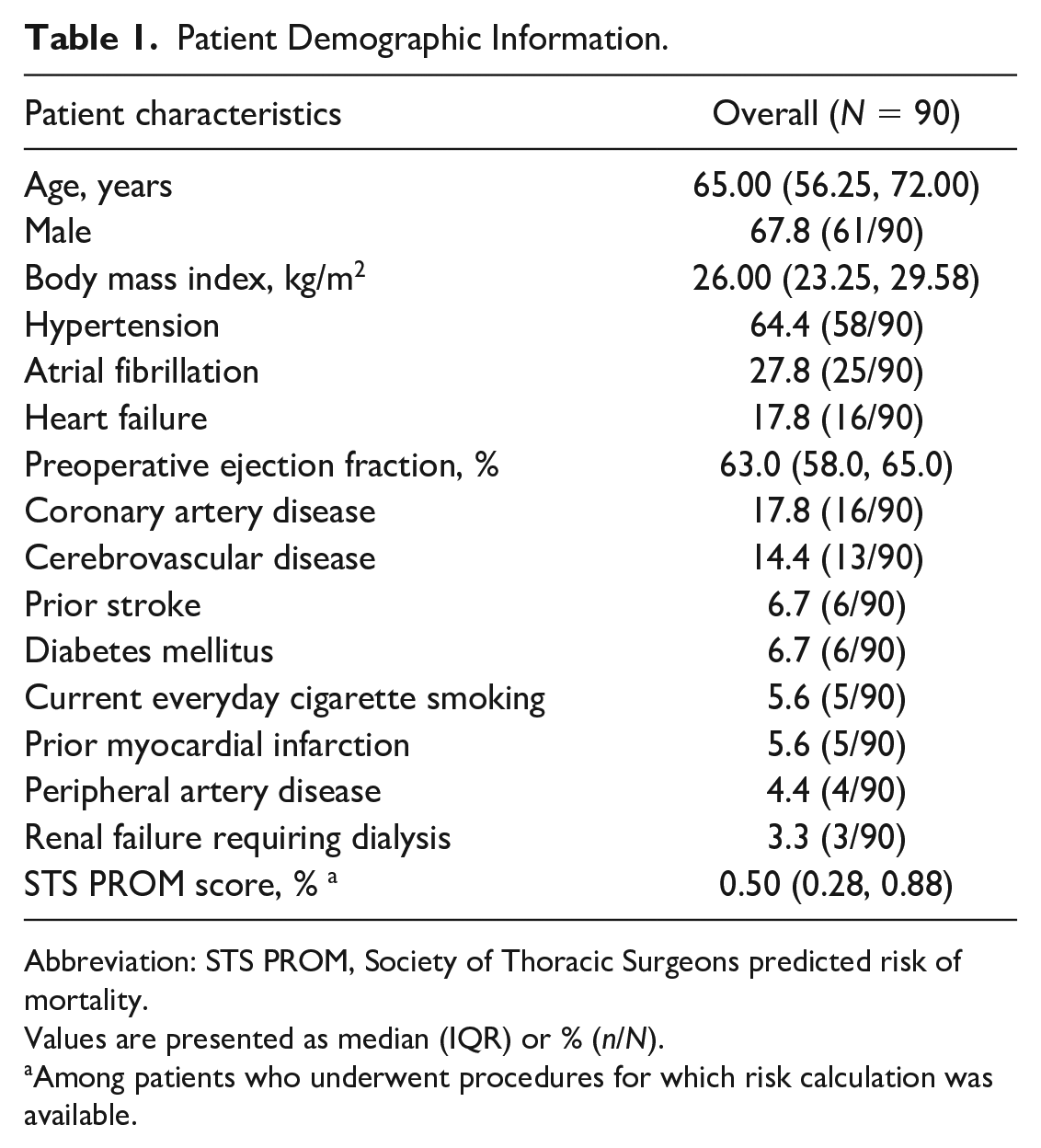
Abbreviation: STS PROM, Society of Thoracic Surgeons predicted risk of mortality.
Values are presented as median (IQR) or % (n/N).
Among patients who underwent procedures for which risk calculation was available.
Procedural Details
Each included patient received rMVR. Patients were included regardless of the number of concomitant procedures. The most common concomitant procedures included left atrial appendage closure (93.3%, 84 of 90), patent foramen ovale closure (30.0%, 27 of 90), and Cox maze IV cryoablation (12.2%, 11 of 90). Of the cases included, 6.7% (6 of 90) were repeat cardiac surgeries. A full list of the procedures performed is provided in Table 2.
Procedural Details and Concomitant Procedures.
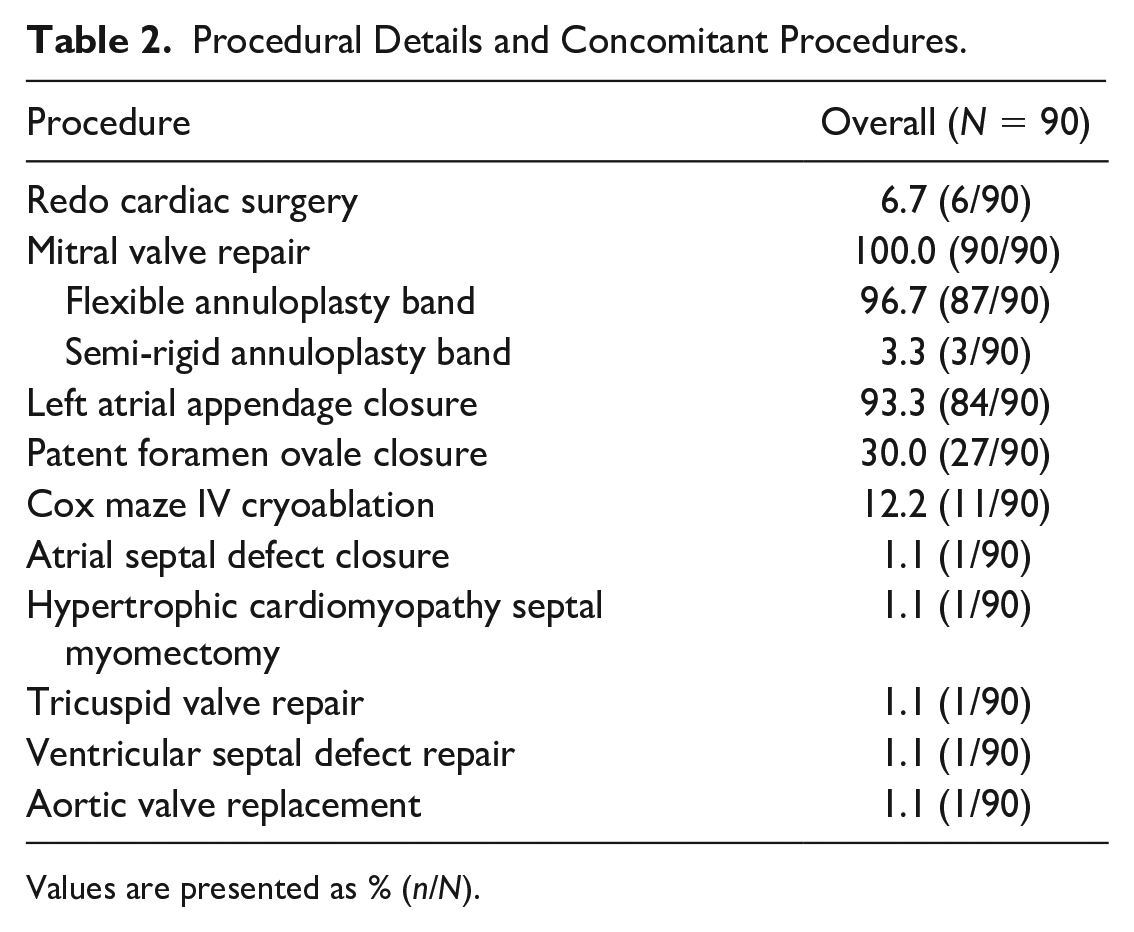
Values are presented as % (n/N).
Uses of Barbed Nonabsorbable Sutures for Concomitant Procedures
Among mitral valve annuloplasties performed with barbed nonabsorbable sutures, 45.6% (41 of 90) were reinforced with an everting pledgeted polyester suture to prevent dehiscence of the primary suture. For patients who underwent concomitant procedures, V-loc™ sutures were used for various steps beyond the inclusion criteria of V-loc™ annuloplasty band fixation. These sutures were used for partial pericardiectomy and atriotomy closure in every patient (90 of 90). V-loc™ sutures were also used for 96.3% of patients (26 of 27) undergoing patent foramen ovale closure and 98.8% of patients (83 of 84) undergoing left atrial appendage closure. A full list of steps employing barbed nonabsorbable sutures is provided in Table 3.
V-loc™ Suture Utilization by Procedure.
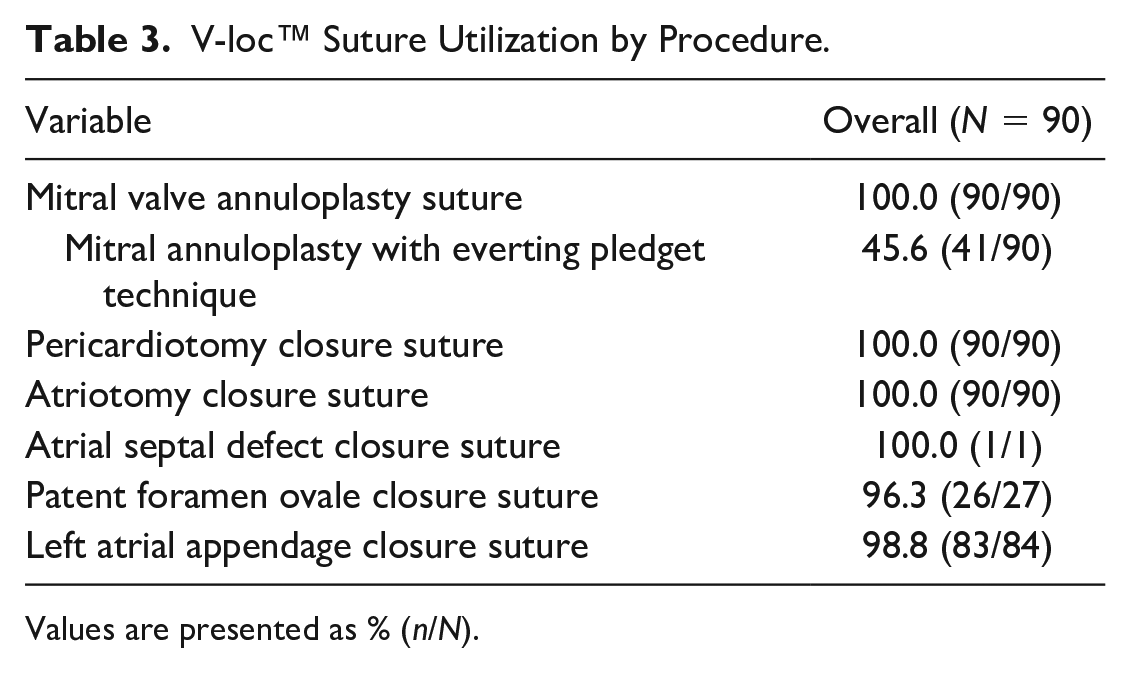
Values are presented as % (n/N).
Outcomes
Median operative time and CPB time generally increased with the number of concomitant procedures performed in addition to MVR (Table 4). The primary exception to this finding was the zero concomitant procedure group, which demonstrated the longest median operative and CPB times. The median operative time and CPB time for patients with 1 concomitant procedure (n = 49) were 260.00 (247.00, 289.00) min and 108.00 (97.00, 123.00) min, respectively. For patients with 2 concomitant procedures (n = 32), the median operative time was 287.00 (267.50, 306.75) min and CPB time was 124.00 (113.00, 139.50) min. The median ICU length of stay was 31.85 (21.67, 51.35) h. Thirty-day readmission rate was 3.3% (3 of 90), and 30-day mortality was 0% (0 of 90). Among those readmitted to the hospital, none were due to suture dehiscence.
Operative and CPB Times Stratified by Number of Concomitant Procedures.
Abbreviation: CPB, cardiopulmonary bypass.
Values are presented as median (IQR).
Complications
One patient who underwent mitral valve annuloplasty using a barbed nonabsorbable suture required reoperation for annuloplasty ring dehiscence. Following this case, the standard V-loc™ suture was reinforced with everting pledged polyester sutures, and no additional ring dehiscence was observed. Similarly, no additional patients required reoperation for suture-related complications. Clinical signs of dehiscence were never observed post-pericardiectomy, atriotomy, or left atrial appendage closure. Postoperative imaging was performed to confirm the absence of dehiscence for soft tissue reapproximation; however, echocardiographic details were not collected through this study.
Discussion
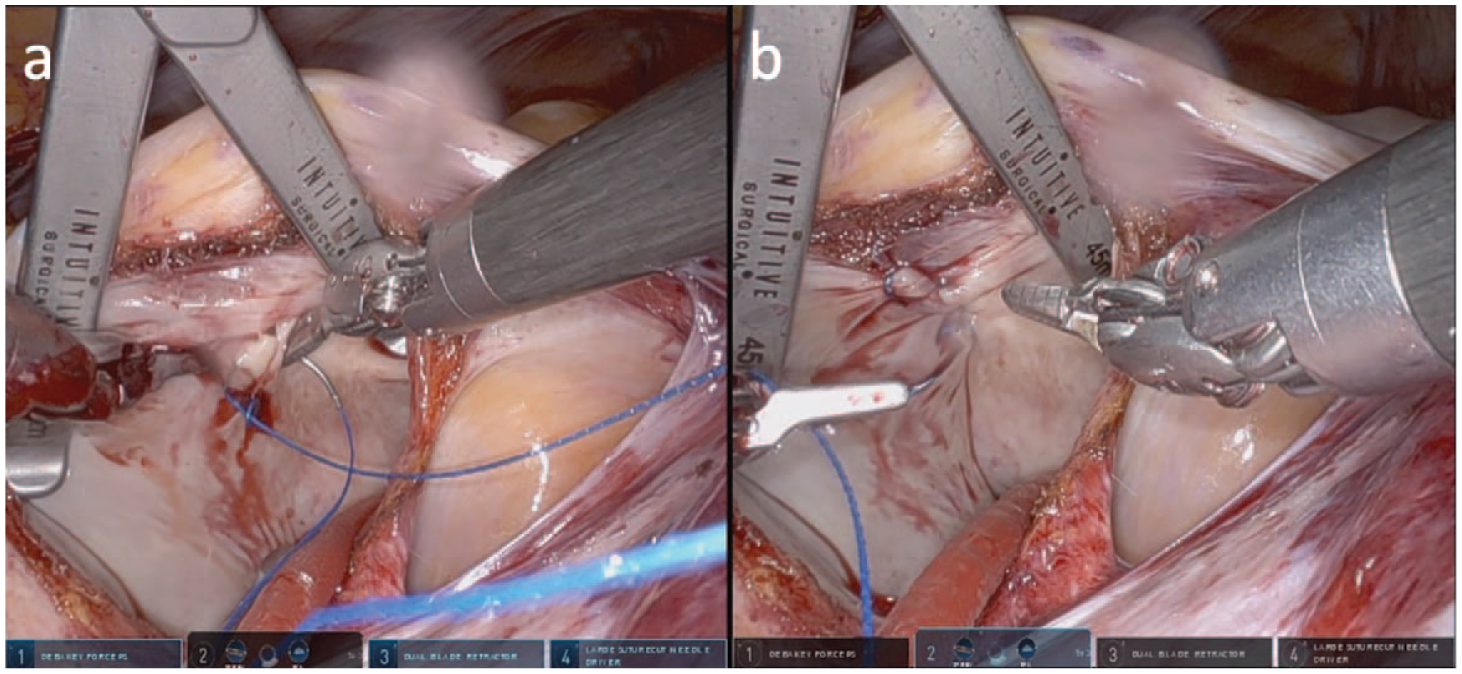
This study details the outcomes of patients who received barbed nonabsorbable sutures for MVR and concomitant procedures during robotic cardiac surgery. In addition to fixation of the mitral annuloplasty band, we employ V-loc™ sutures for a number of procedural steps. These include reapproximation of the pericardium and atrium, left atrial appendage closure, and patent foramen ovale closure. Perhaps most notable of our uses for barbed sutures, though, is in fastening the mitral annuloplasty band to the annulus (Fig. 1). This technique is performed in a running horizontal mattress fashion with each suture starting at the trigones and meeting in the middle of the P2 mitral segment. The suture is then secured to the annuloplasty band. Of the 90 patients in whom a mitral annuloplasty band was secured with V-loc sutures, 1 patient experienced band dehiscence (Table 5). However, following the case in which dehiscence occurred, we began routinely reinforcing V-loc™ annuloplasty band suture with an everting pledgeted 2-0 Ethibond mattress suture (Ethicon, Raritan, NJ, USA) secured to the annuloplasty ring with a Cor-Knot device (LSI Solutions, Victor, NY, USA; Fig. 2). After implementing this modification, we observed no cases of clinical band dehiscence or suture-related complications in the 41 patients who received the reinforcement.
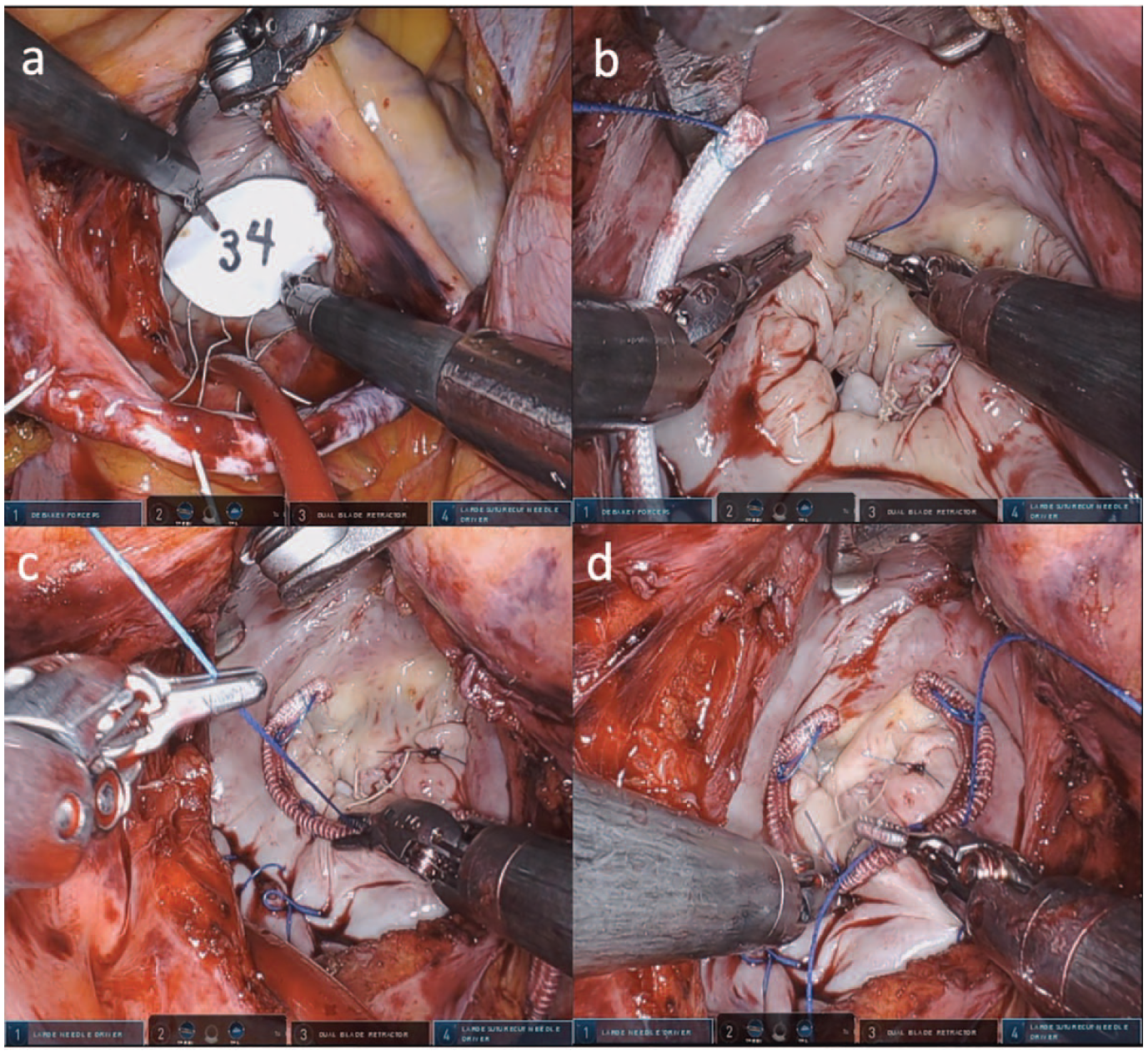
V-loc™ sutures for mitral valve annuloplasty band. (a) The mitral annulus is sized with a paper sizer. (b) Two nonabsorbable 3-0 V-loc™ sutures are then used to fasten the flexible annuloplasty band in running horizontal mattress fashion. (c) The sutures are started at the trigones and meet in the middle of P2. (d) The finished product.
Postoperative Outcomes.
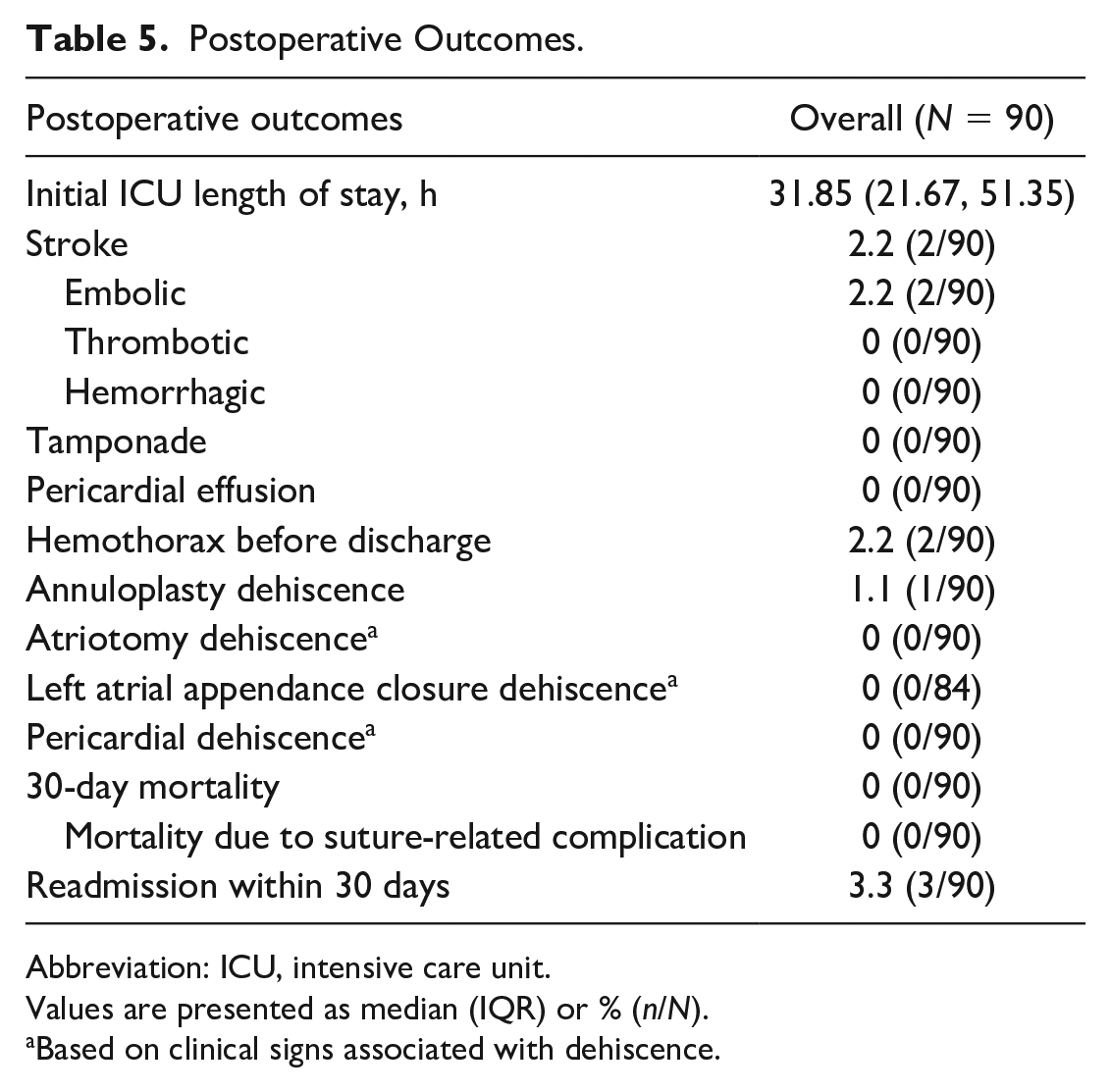
Abbreviation: ICU, intensive care unit.
Values are presented as median (IQR) or % (n/N).
Based on clinical signs associated with dehiscence.
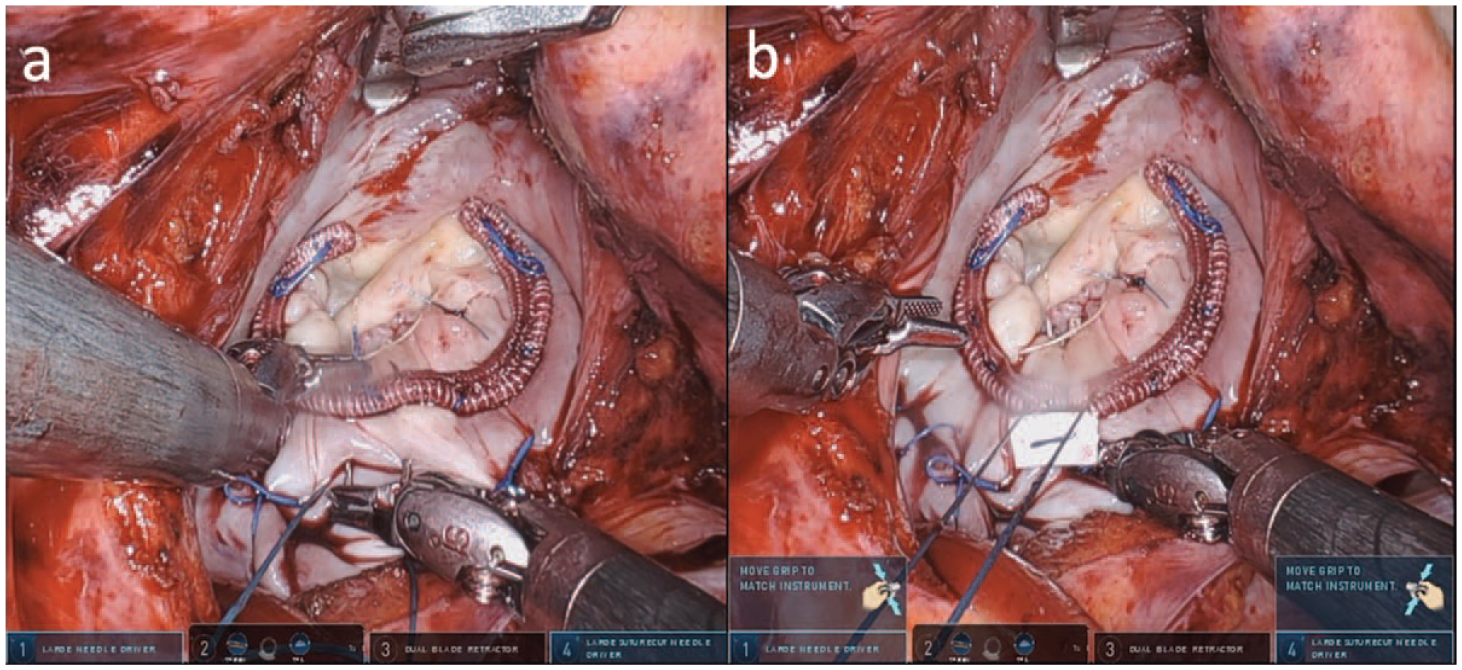
(a) The posterior annulus is reinforced with (b) an everting pledgeted 2-0 Ethibond mattress suture to prevent dehiscence.
In their 2015 technique paper, Watanabe and Ishikawa outlined the method for using barbed sutures during ring fastening in robotic mitral annuloplasty. 15 They noted that the use of V-loc™ nonabsorbable sutures for robotic cardiac surgery reduced aortic cross-clamp time and therefore total cardiac arrest time. 15 These findings are noteworthy given that mortality and complications such as prolonged ICU stay and stroke have been shown to be associated with longer aortic cross-clamp and CPB periods. 19 Reducing procedural time is also valuable given that increased operative time compared to open surgery is a primary critique of the robotic approach. Other alternatives to mechanical suturing have been reported in an effort to increase operative efficiency. Nitinol U-clips have been demonstrated to reduce CPB and band-fastening time by eliminating the need for knot tying during annuloplasty band fixation. 20 Moreover, Gillinov and colleagues reported the use of the Cor-Knot device with 2 continuous sutures and found a reduction in suture deployment time but not overall CPB time. 21 Finally, Lawrie and colleagues reported the use of a running propylene suture for robotic mitral annuloplasty band fixation. 22
While not demonstrated extensively in the literature within cardiac surgery, V-loc™ has been shown to be associated with increased operative efficiency.10,14 Because robotic cardiac surgery has been associated with increased procedural length, iterations with the utilization of V-loc™ has made robotic cardiac surgery more seamless at our institution.1,4 As noted above, Watanabe and Ishikawa demonstrated decreased cross-clamp times by over 12 min with the use of V-loc™ versus monofilament 2-0 sutures. 15 Distinctly, we believe that V-loc™ allows for a tighter suture line between throws with the suture’s unidirectional barbed model. Thus, the continuous nature of V-loc™ avoids knot tying and enables greater versatility for the bedside assistant.
That said, we are aware that V-loc™ has limitations. If a ring is misplaced with V-loc™, the process to remove and resize the ring would be difficult. Fortunately, we presize all valves to help mitigate this risk. Like any other suture, there is risk of suture dehiscence. When compared against interrupted 2-0 nonpledgeted sutures (what we would otherwise use in rMVR), there is a theoretical increased risk of complete ring dehiscence with V-loc™. Thus, nonpledgeted sutures with traditional tying may pose a specific advantage in this aspect. While studied in vitro with no apparent increased risk of dehiscence in a high-pressure system, this does require further exploration. 23
Prior studies have demonstrated low intraoperative mortality rates with rMVR, such as a 2015 multicenter review from Paul et al. that determined the intraoperative mortality rate of rMVR to be 1.3%. 24 In our population, the use of V-loc™ sutures for rMVR resulted in a reported 30-day mortality rate of 0% (0 of 90). Moreover, our patients demonstrated low rates of stroke (2.2%, 2 of 90), pericardial effusion (0%, 0 of 90), and tamponade (0%, 0 of 90) following robotic cardiac surgery. These findings support the short-term operative viability that the use of barbed nonabsorbable sutures can possibly provide.
For experienced surgeons, V-loc™ sutures can be easily deployed by the robotic platform. V-loc™ sutures incorporate characteristic barbs protruding from the suture monofilament to prevent backsliding of the filament. A unidirectional motion, which ensures secure embedment in the tissue and prevents slack accumulation without knot tying, can be applied to the fibrous annuloplasty band when performing MVR. Given this versatility, V-loc™ sutures can be utilized for a variety of steps involving tissue and/or synthetic materials. As such, in additional to MVR, atriotomy closure, and pericardiectomy closure (Fig. 3), we also routinely employ V-loc™ sutures for left atrial appendage closure (Fig. 4), patent foramen ovale closure (Fig. 5), and atrial septal defect closures.
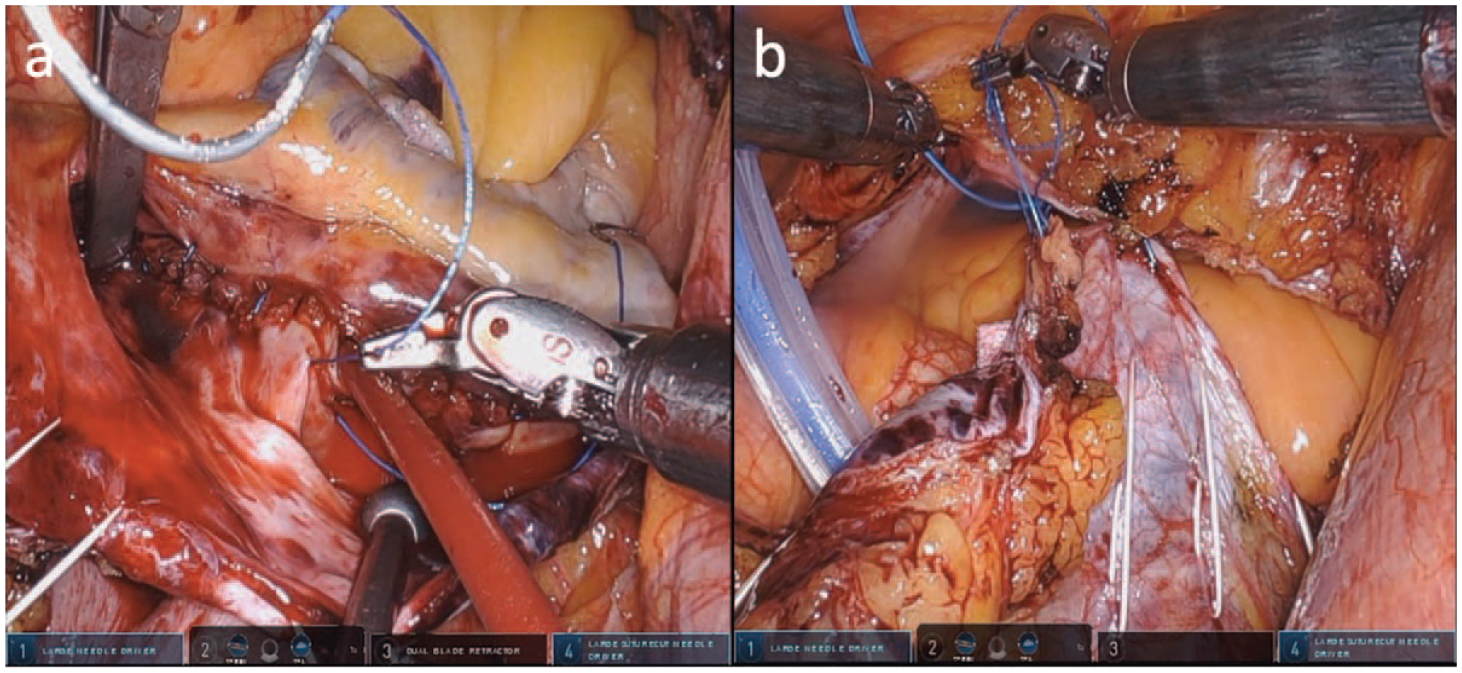
V-loc™ sutures for (a) atriotomy and (b) pericardiectomy closure.
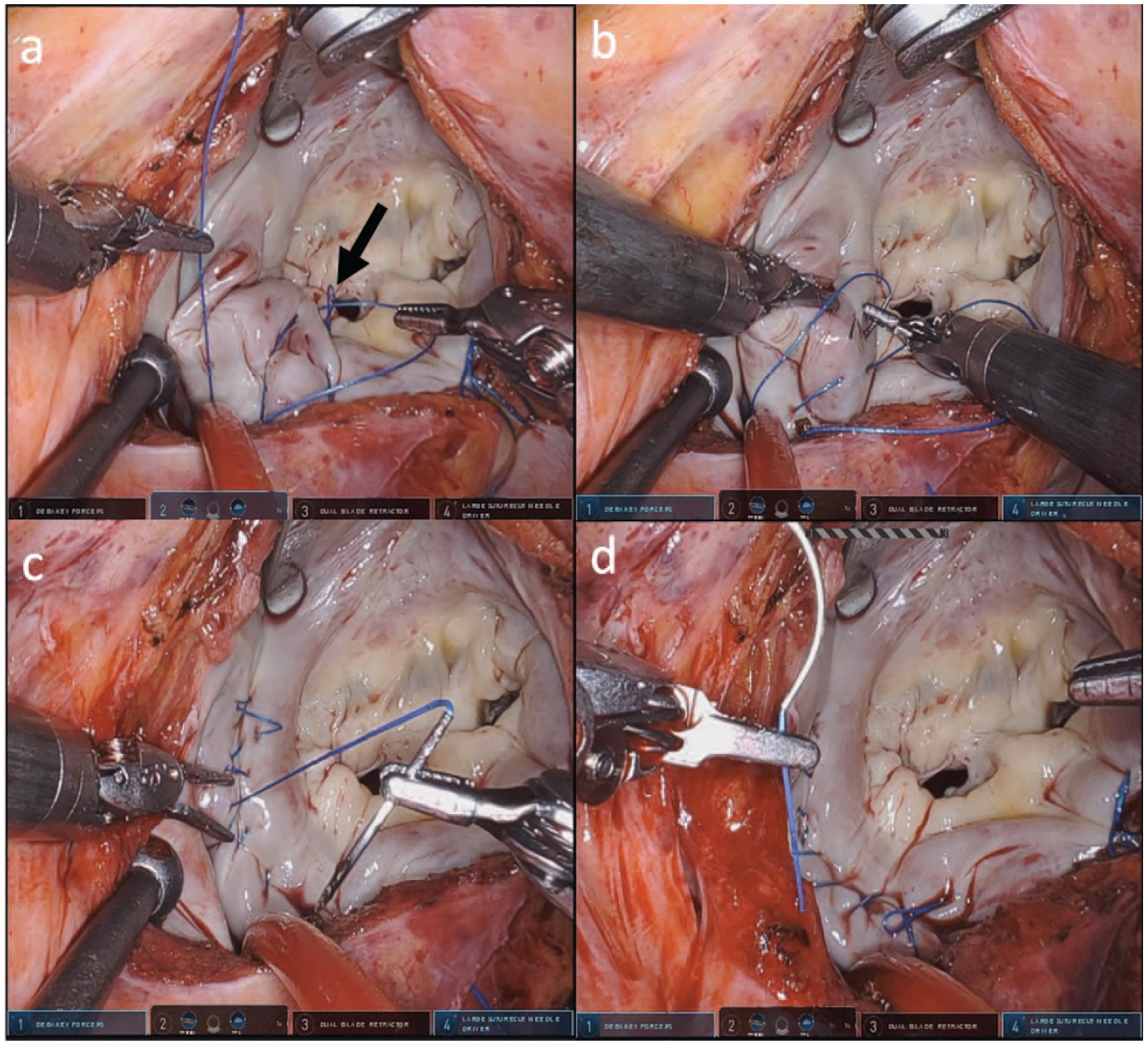
V-loc™ sutures for left atrial appendage closure. (a) The loop design (black arrow) of the V-loc™ suture eliminates the need for knot tying. (b) (c) The left atrial appendage is closed in double-layer fashion. (d) The finished product.
V-loc™ sutures for patent foramen ovale closure. (a) The patent foramen ovale is closed in double-layer fashion. (b) The finished product.
Limitations
Among the limitations to this study, the most pressing relates to the nature of its retrospective review design. Without a comparator group, we cannot compare operative efficiency and patient outcomes between V-loc™ sutures and traditional approaches to reapproximation and annuloplasty band fastening. Rather, we seek to demonstrate the safety in a diverse array of applications for barbed sutures in robotic cardiac surgery. While our clinical protocol is such that each patient receives an echocardiogram at multiple time points, we do not have clinical echocardiographic data in this study. Much of the data were not present in our collection. Consequently, we cannot judge dehiscence through imaging and the reliance on clinical symptoms may be inadequate. This needs to be further explored when reviewing longer-term data.
All cases were completed by the same experienced surgeon, which obscures the learning curve some institutions may encounter when first implementing barbed sutures. However, any learning curve with barbed sutures should be evaluated with consideration of the previously demonstrated learning curve associated with other commercially available knot-tying devices.25,26 Moreover, regarding nonmitral applications (left atrial appendage, atriotomy, and pericardiectomy closure) of the V-loc™ sutures, we did not perform postoperative imaging due to its costly and invasive nature. The atrial suture line, which in every patient was performed at Waterson’s groove, was never reinforced with extra hemostatic sutures; the V-loc suture was used in isolation, and there were no clinical signs of dehiscence in any patient as demonstrated through direct surgical inspection and the lack of need for reoperation. Finally, our data are limited to short-term outcomes, and long-term outcome data would help provide better evidence for the efficacy and safety of barbed sutures. Although the study is observational in nature, we hope to further follow outcomes in patients undergoing cardiac surgery with barbed sutures to further assess safety and efficacy of such approach.
Conclusions
This study demonstrates V-loc™ sutures as a viable option for annuloplasty band fixation and soft tissue reapproximation in robotic cardiac surgery. The field would benefit from more extensive prospective investigation into the long-term outcomes and safety profile for patients who undergo rMVR with barbed V-loc™ sutures with the intention to increase operative efficiency.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Guy is a consultant for Edwards Lifesciences, Medtronic, and a case observation site and proctor for Intuitive Surgical.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.