Gender-Based Disparities for Outcomes in Esophagectomy
Emily L. Larson1, Jessica M. Ruck2, Alice L. Zhou1, Stephen C. Yang2, Richard J. Battafarano2, Stephen R. Broderick2, Errol L. Bush2, Jinny S. Ha2. 1Johns Hopkins School of Medicine, Baltimore, MD, USA, 2Johns Hopkins Hospital, Baltimore, MD, USA.
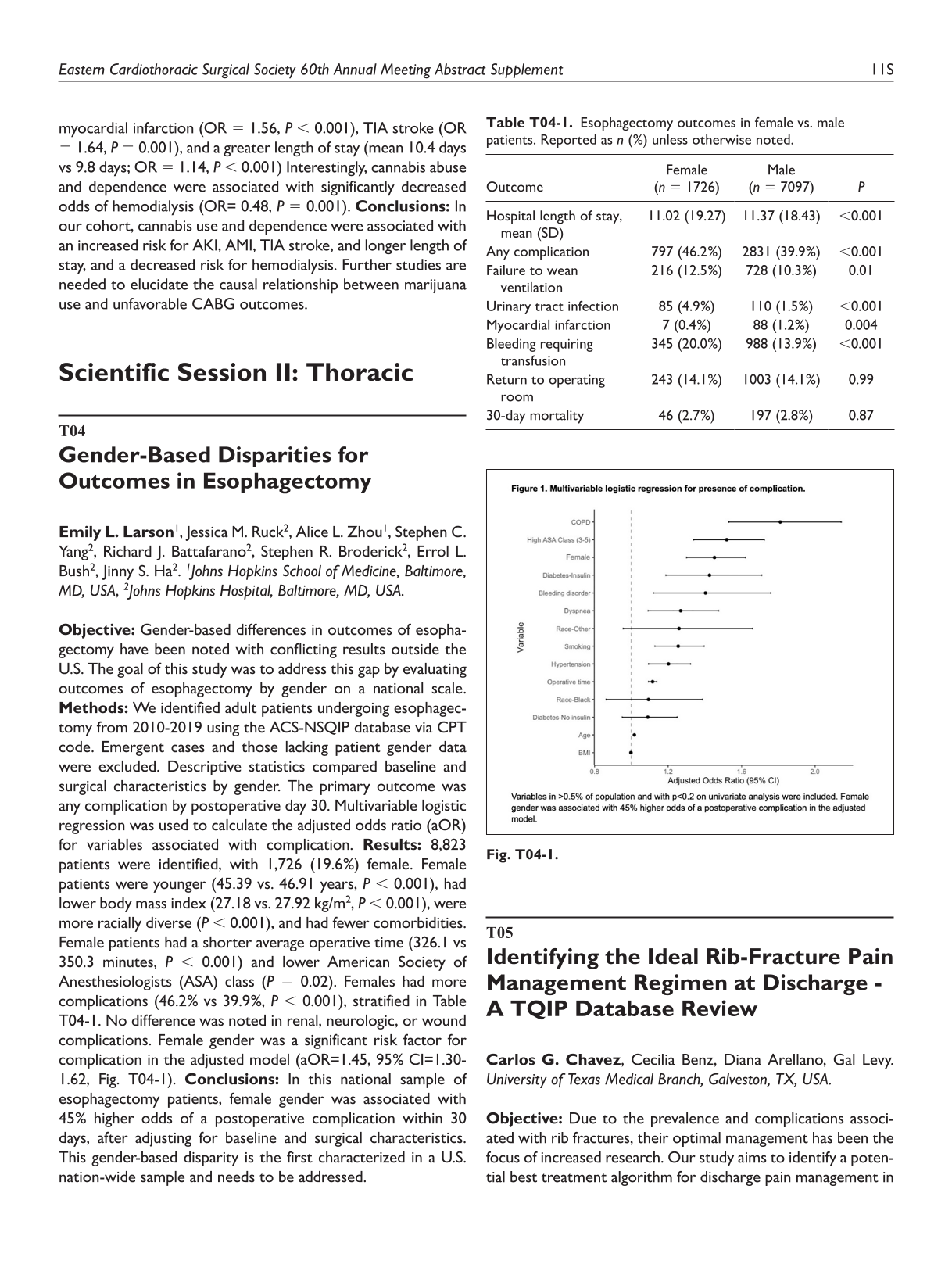
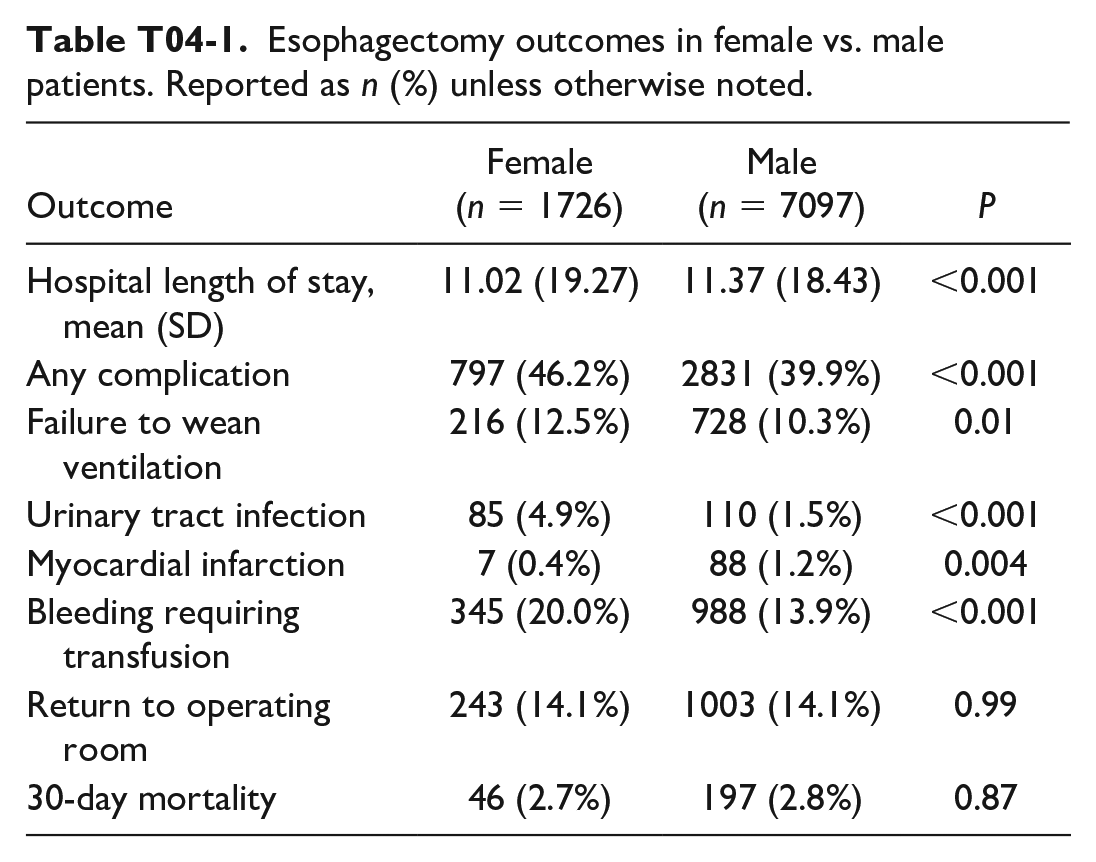
Objective: Gender-based differences in outcomes of esophagectomy have been noted with conflicting results outside the U.S. The goal of this study was to address this gap by evaluating outcomes of esophagectomy by gender on a national scale. Methods: We identified adult patients undergoing esophagectomy from 2010-2019 using the ACS-NSQIP database via CPT code. Emergent cases and those lacking patient gender data were excluded. Descriptive statistics compared baseline and surgical characteristics by gender. The primary outcome was any complication by postoperative day 30. Multivariable logistic regression was used to calculate the adjusted odds ratio (aOR) for variables associated with complication. Results: 8,823 patients were identified, with 1,726 (19.6%) female. Female patients were younger (45.39 vs. 46.91 years, P < 0.001), had lower body mass index (27.18 vs. 27.92 kg/m2, P < 0.001), were more racially diverse (P < 0.001), and had fewer comorbidities. Female patients had a shorter average operative time (326.1 vs 350.3 minutes, P < 0.001) and lower American Society of Anesthesiologists (ASA) class (P = 0.02). Females had more complications (46.2% vs 39.9%, P < 0.001), stratified in Table T04-1. No difference was noted in renal, neurologic, or wound complications. Female gender was a significant risk factor for complication in the adjusted model (aOR=1.45, 95% CI=1.30-1.62, Fig. T04-1). Conclusions: In this national sample of esophagectomy patients, female gender was associated with 45% higher odds of a postoperative complication within 30 days, after adjusting for baseline and surgical characteristics. This gender-based disparity is the first characterized in a U.S. nation-wide sample and needs to be addressed.
Esophagectomy outcomes in female vs. male patients. Reported as n (%) unless otherwise noted.
Outcome
Female (n = 1726)
Male (n = 7097)
P
Hospital length of stay, mean (SD)
11.02 (19.27)
11.37 (18.43)
<0.001
Any complication
797 (46.2%)
2831 (39.9%)
<0.001
Failure to wean ventilation
216 (12.5%)
728 (10.3%)
0.01
Urinary tract infection
85 (4.9%)
110 (1.5%)
<0.001
Myocardial infarction
7 (0.4%)
88 (1.2%)
0.004
Bleeding requiring transfusion
345 (20.0%)
988 (13.9%)
<0.001
Return to operating room
243 (14.1%)
1003 (14.1%)
0.99
30-day mortality
46 (2.7%)
197 (2.8%)
0.87
T05
Identifying the Ideal Rib-Fracture Pain Management Regimen at Discharge - A TQIP Database Review
Carlos G. Chavez, Cecilia Benz, Diana Arellano, Gal Levy. University of Texas Medical Branch, Galveston, TX, USA.
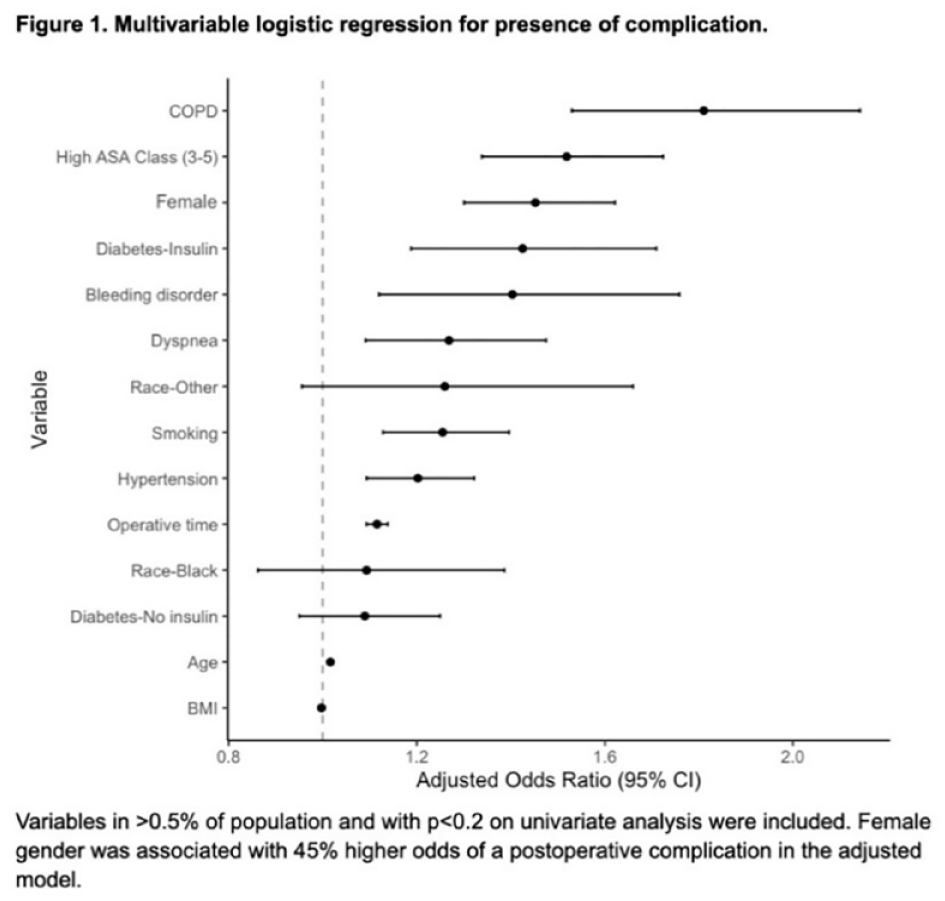
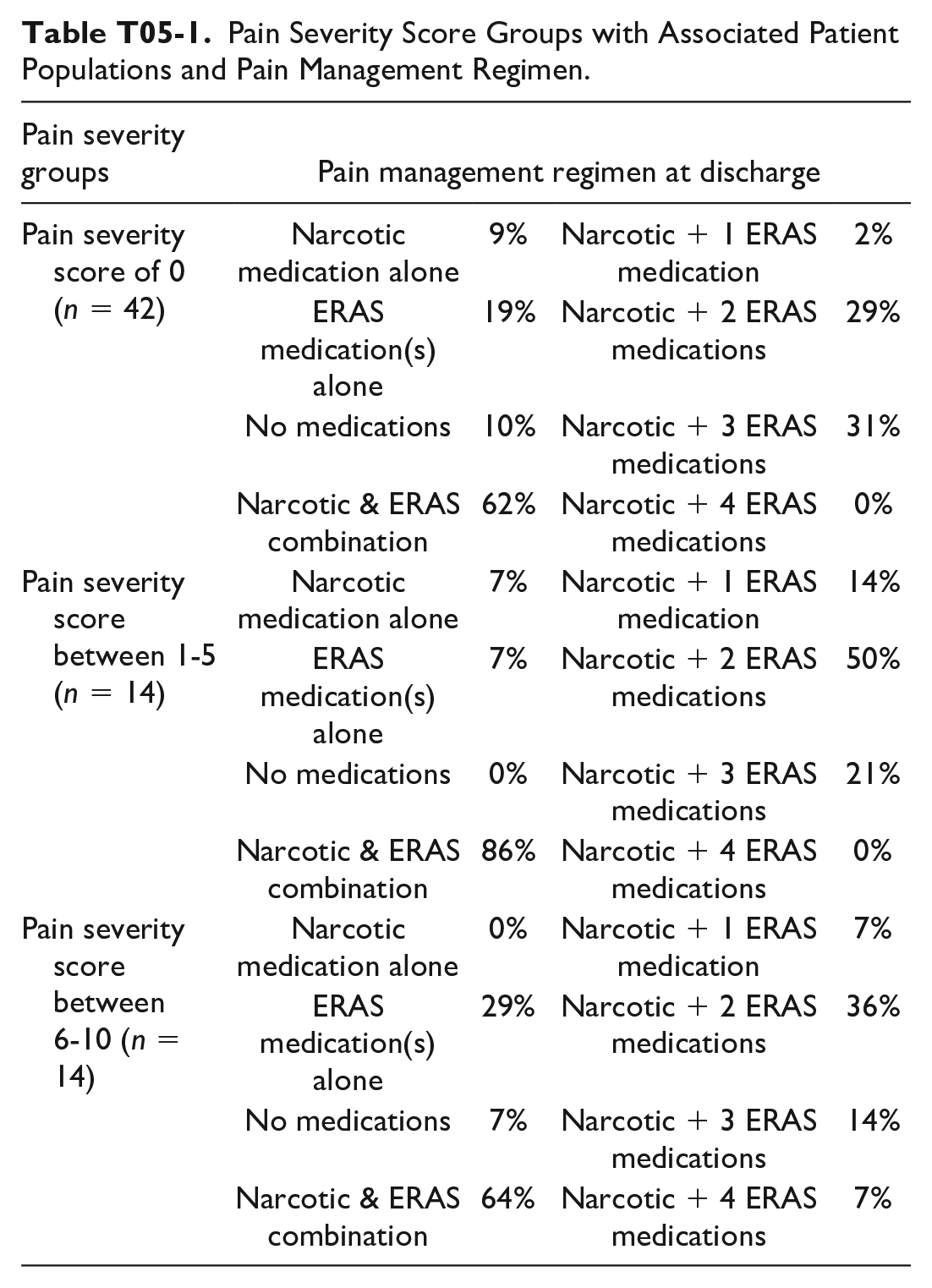
Objective: Due to the prevalence and complications associated with rib fractures, their optimal management has been the focus of increased research. Our study aims to identify a potential best treatment algorithm for discharge pain management in isolated rib fracture patients. Methods: A retrospective chart review was conducted using the Trauma Quality Improvement Program (TQIP) database. Discharge medication regimen as well as follow-up visit setting, reason, and pain score were documented. Patients were stratified by pain score, visit reasoning, and pain management mechanism defined as a narcotic agent and/or Enhanced Recovery After Surgery (ERAS) medications; consisting of acetaminophen, NSAIDs, muscle relaxers, and/or nerve pain agents. Descriptive statistics were used to quantify the percentage of combinations per follow-up score. Results: The majority of patients with a pain score of 0 were on a narcotic with 3 ERAS medications with no complaints on follow-up.1 The majority of patients with a 1-5 pain score were on a narcotic with 2 ERAS medications with fracture-associated complaints.1 The majority of patients with a 6-10 pain score were on a narcotic with 2 ERAS medications.1 This group had the most patients seen in the ED with fracture-associated complaints and the most treated with ERAS-only medications. Conclusions: Our observations suggest that neither narcotic nor ERAS medications alone are sufficient pain control methods. The ideal combination seems to be a narcotic agent alongside 3 ERAS medications. This has helped identify a potential best treatment algorithm for the minimization of pain and complication rates in isolated rib fracture patients.
Pain Severity Score Groups with Associated Patient Populations and Pain Management Regimen.
Pain severity groups
Pain management regimen at discharge
Pain severity score of 0 (n = 42)
Narcotic medication alone
9%
Narcotic + 1 ERAS medication
2%
ERAS medication(s) alone
19%
Narcotic + 2 ERAS medications
29%
No medications
10%
Narcotic + 3 ERAS medications
31%
Narcotic & ERAS combination
62%
Narcotic + 4 ERAS medications
0%
Pain severity score between 1-5 (n = 14)
Narcotic medication alone
7%
Narcotic + 1 ERAS medication
14%
ERAS medication(s) alone
7%
Narcotic + 2 ERAS medications
50%
No medications
0%
Narcotic + 3 ERAS medications
21%
Narcotic & ERAS combination
86%
Narcotic + 4 ERAS medications
0%
Pain severity score between 6-10 (n = 14)
Narcotic medication alone
0%
Narcotic + 1 ERAS medication
7%
ERAS medication(s) alone
29%
Narcotic + 2 ERAS medications
36%
No medications
7%
Narcotic + 3 ERAS medications
14%
Narcotic & ERAS combination
64%
Narcotic + 4 ERAS medications
7%
T06
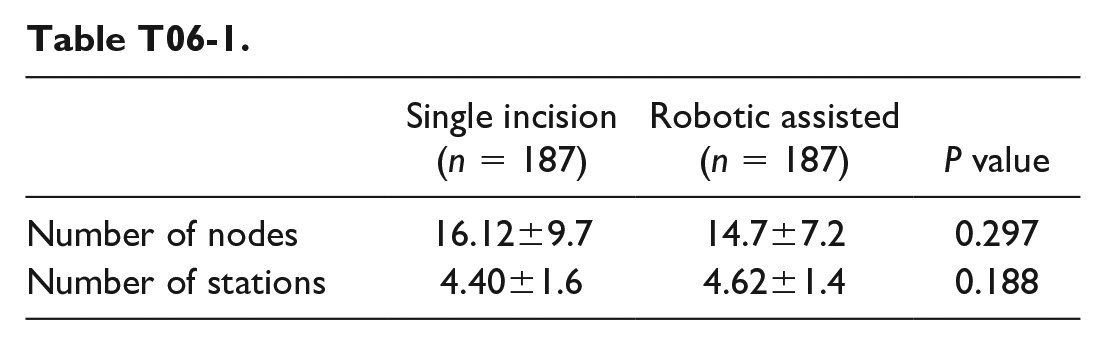
Mediastinal Lymph Node Dissection During Minimally Invasive Pulmonary Resections: Is Uniportal VATS Good Enough?
Joshua S. Newman1, Stevan S. Pupovac1, Kyle W. Riggs1, Miguel Alexis1, Sridhar Uttara2, Julissa Jurado1, Kevin Hyman1, Paul C. Lee1, David Zeltsman1. 1Northwell Health, New Hyde Park, NY, USA, 2Northwell Health, Manhasset, NY, USA.
Objective: Single-incision VATS offers a most minimally invasive approach to pulmonary resection; however, it is questioned if this approach offers as adequate of a lymph node dissection as alternative modalities including robotic VATS approaches. We demonstrate that single incision VATS allows oncologic resections and staging non-inferior to robotic assisted approaches. Methods: We performed a retrospective review comparing robotic-assisted and single-incision VATS lobectomy over 27-months. Inclusion criteria were age 18-90 years at operation and anatomic lobectomy by either robotic assisted or single-incision VATS approaches. Exclusion criteria were incomplete demographic data, benign diagnosis on frozen pathology, and intraoperative conversion to an alternative modality (eg: thoracotomy). Our cohort was propensity matched. The study was approved by the Northwell Health Internal Review Board. (IRB: 21-0738). Results: Five hundred and twenty-six (n = 526) patients met inclusion but not exclusion criteria with a resultant 187 matched pairs. There was no statistically significant difference in average number of lymph nodes sampled between the robotic and single-incision cohorts. (14.7 vs 16.1; P = 0.30) Furthermore, the number of lymph node stations sampled was not different between the robotic and single-incision cohorts. (4.62 vs 4.40, P = 0.19; Table T06-I). Length of stay was not statistically significantly different between the robotic and single incision cohorts (P = 0.06). Conclusions: VATS is readily utilized for oncologic pulmonary resection. Although concern exists over the ability to perform an adequate lymph node dissection via a most minimally invasive single-incision approach, we suggest this modality offers non-inferior lymph node sampling and staging when compared with a robotic assisted approach.