
Abstract
Objective:
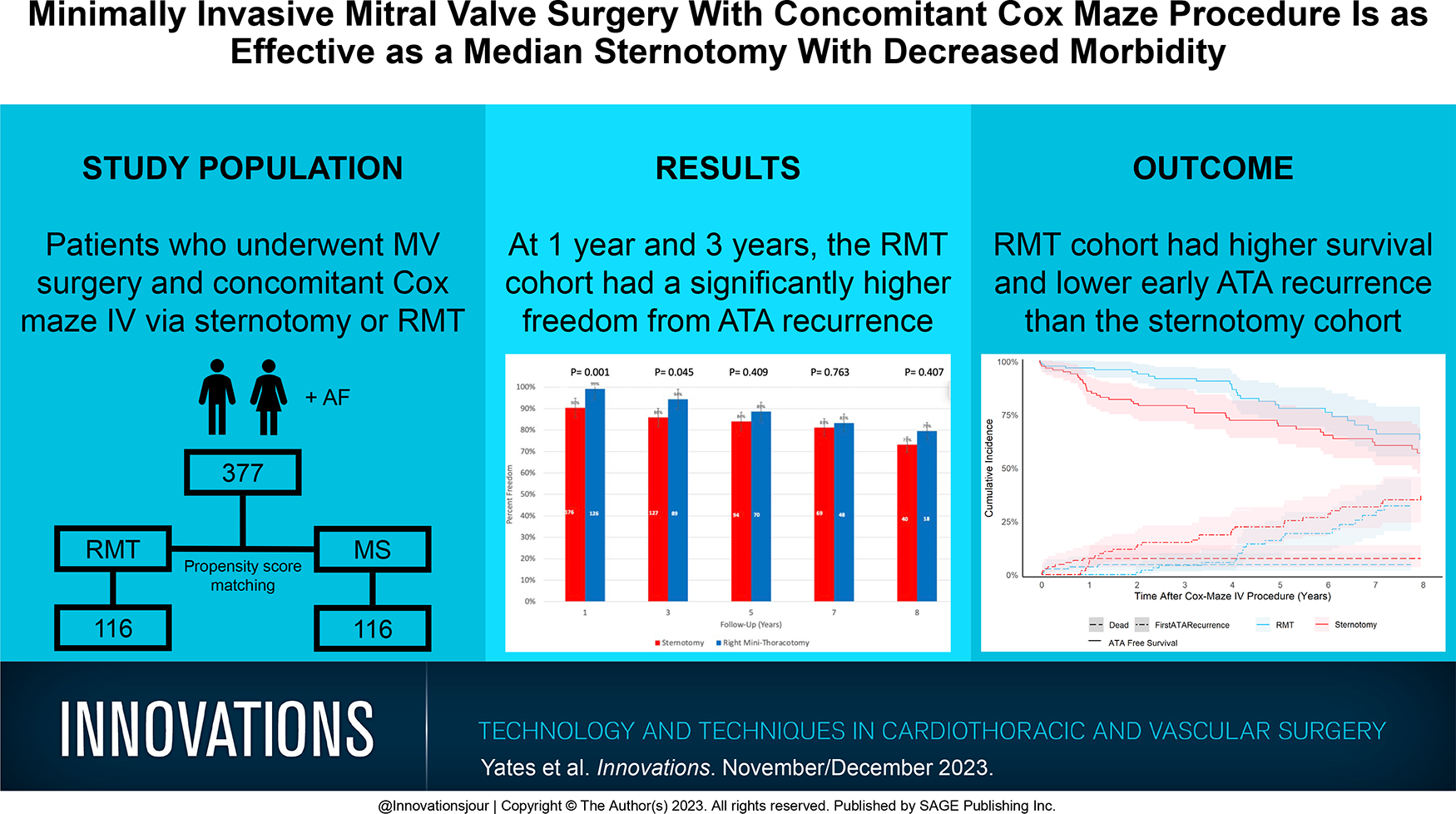
A right minithoracotomy (RMT) is a minimally invasive surgical approach that has been increasingly performed for the concomitant Cox maze IV procedure (CMP) and mitral valve surgery (MVS). Little is known regarding whether long-term rhythm and survival outcomes are affected by the RMT as compared with the traditional median sternotomy (MS) approach.
Methods:
Between April 2004 and April 2021, 377 patients underwent the concomitant CMP and MVS, of whom 38% had RMT. Propensity score matching yielded 116 pairs. Freedom from atrial tachyarrhythmias (ATA) was assessed with prolonged monitoring annually for 8 years. Survival, rhythm, and perioperative outcomes were compared.
Results:
The unmatched RMT cohort had a greater freedom from ATA recurrence at 1 year (99% vs 90%, P = 0.001) and 3 years (94% vs 86%, P = 0.045). The matched RMT cohort had longer cardiopulmonary bypass (median: 215 [199 to 253] vs 170 [136 to 198] min, P < 0.001) and aortic cross-clamp (110 [98 to 124] vs 86 [71 to 102] min, P < 0.001) times but shorter intensive care time (48 [24 to 95] vs 71 [26 to 144] h, P = 0.001) and length of stay (8 [6 to 11] vs 10 [7 to 14] h, P < 0.001). More pacemakers (18% vs 4%, P < 0.001) and postoperative transfusions (57% vs 41%, P = 0.014) occurred in the MS cohort. The 30-day mortality (P = 0.651) and 8-year survival (P = 0.072) was not significantly different between the cohorts.
Conclusions:
Early 1-year and 3-year freedom from ATA recurrence was better in the RMT cohort compared with the MS cohort. Despite longer operative times, the RMT cohort had shorter lengths of stay, fewer postoperative transfusions, and fewer pacemakers placed.
Keywords
Central Message
The early 1-year and 3-year freedom from ATA recurrence was better in the RMT cohort compared with the MS cohort. Despite longer operative times, the RMT cohort had shorter lengths of stay, fewer postoperative transfusions, and fewer pacemakers placed. Long-term freedom from ATA and survival was not significantly different between surgical approaches.
Introduction
Atrial fibrillation (AF) is the most common sustained arrhythmia and is associated with an increased risk for stroke, hemodynamic instability, and death. 1 The Cox maze procedure (CMP) is the gold standard for surgical treatment of AF because it has had excellent long-term rhythm and survival outcomes as well as a reduced risk for stroke.2 –4 Of patients with mitral valve (MV) disease requiring MV surgery, 30% to 40% have AF. The MV patients who undergo concomitant cardiac ablation for AF at the time of surgery comprise most of those treated with concomitant surgical ablation.5,6
Minimally invasive surgery, either via right minithoracotomy (RMT) or thoracoscopically, is increasingly used as an alternative to the traditional median sternotomy (MS) in patients undergoing MV surgery with or without concomitant CMP.5,7–10 Potential benefits of an RMT are a smaller incision allowing for optimal visualization of the MV with less tissue dissection and bleeding, the cosmetic benefit of a smaller scar, less postoperative pain, and reduced length of stay in the hospital and intensive care unit (ICU) compared with an MS approach.11 –14
The long-term outcomes after MV surgery, via RMT versus MS approach, have been well described in recent meta-analyses, which found similar MV repair outcomes without significant differences in all-cause mortality, stroke rate, or reoperation rate between the surgical approaches.10,15 However, there are few data that compare the long-term rhythm outcomes, based on surgical approach, for patients undergoing concomitant surgical ablation and MV surgery.16,17 Knowing the long-term outcomes after an RMT approach is critical because the RMT approach requires modification of both the ablation and surgical strategies. 18 The goal of our study was to examine both the long-term rhythm and survival outcomes, based on RMT versus MS surgical approach, in 116 propensity-matched pairs, all of whom underwent concomitant CMP-IV and MV surgery.
Methods
Patients
This is a single-center, retrospective, cohort study that was approved by the Washington University School of Medicine in St. Louis Institutional Review Board (No. 201105322, approval date February 16, 2022). Informed consent and permission for release of information were obtained from all patients. The rhythm data were prospectively collected, and perioperative variables were defined by the Society of Thoracic Surgeons Adult Cardiac Surgery Database definitions. Acute kidney injury (AKI) was defined by the KDIGO guidelines as a ≥1.5-fold increase in serum creatinine from baseline within 7 days. 19 Missing data were ascertained through chart review, contact with patients, and referring physicians. Patients who were alive at 30 days and had missing long-term rhythm data at every annual follow-up time point were excluded from the long-term rhythm analysis. Patients who were alive at 30 days and had few missing rhythm data at specific time points were included in the long-term analysis, and only the missing data of those specific years were excluded.
Between April 2004 and April 2021, 975 patients with AF underwent MV surgery. There were 377 patients (age ≥18) who underwent concomitant MV surgery and CMP-IV ablation with left atrial appendage (LAA) excision or exclusion with or without concomitant tricuspid valve (TV) surgery and/or atrial septal defect closure (Table 1).
Operations.
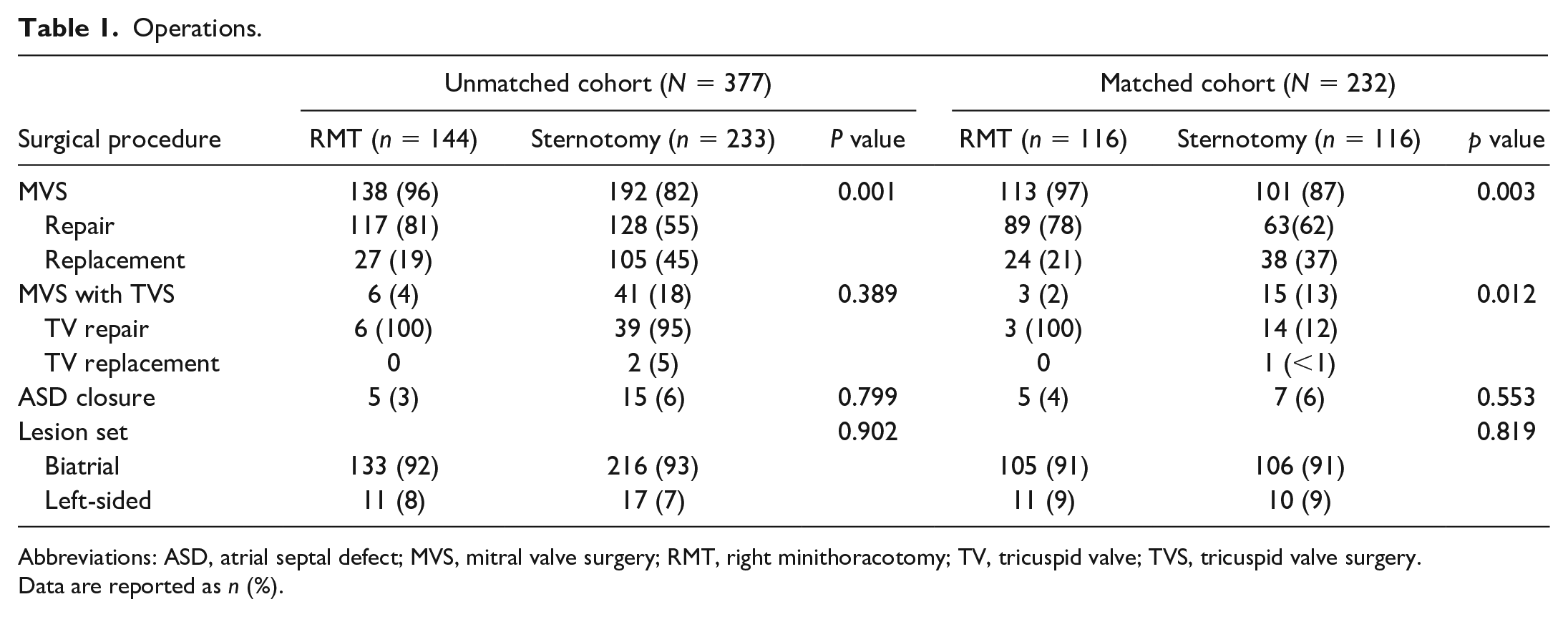
Abbreviations: ASD, atrial septal defect; MVS, mitral valve surgery; RMT, right minithoracotomy; TV, tricuspid valve; TVS, tricuspid valve surgery.
Data are reported as n (%).
The selection criteria for a patient to undergo an RMT was dependent on surgeon preference and patient anatomy. Generally, patients were candidates for the RMT if their preoperative computed tomography angiogram revealed adequate size of the iliac and femoral vessels, minimal atherosclerotic disease of the thoracic and abdominal aorta, and appropriate chest wall anatomy, particularly the anterior-posterior diameter of ≥10 cm.
The selection criteria for left-sided CMP were paroxysmal AF with a duration ≤1 year without right atrial enlargement, TV disease, or pulmonary hypertension. LAA management varied by patient with closure achieved by amputation with epicardial oversewing, epicardial placement of an AtriClip (AtriCure Inc, Mason, OH, USA), or oversewing the endocardium. Patients were excluded from the study if they underwent any other concomitant cardiac surgeries or had active endocarditis, cardiac tumors, emergent case, or incomplete left posterior wall ablation such as pulmonary vein (PV) isolations (n = 598). Contraindications to performing an RMT included previous thoracotomy, atherosclerotic disease preventing a single femoral arterial cannulation and retrograde perfusion, and/or left ventricular ejection fraction (LVEF) ≤20%.
The AF type of each patient was defined by the current 2017 Heart Rhythm Society (HRS) guidelines. 20 Long-standing persistent AF (LSPAF) was defined as continuous AF for >1 year, persistent AF was defined as lasting beyond 7 days, and paroxysmal AF was defined as terminating spontaneously or with intervention within 7 days. 20 The operative details of the CMP-IV lesion set using radiofrequency (RF) and/or cryoablation via MS or RMT have been described previously by our group.17,18,21
The CMP-IV lesion set in both surgical approaches were identical, but the energy sources used to make the lesions were different. In the RMT, bipolar RF clamps were used to isolate the right PVs, with exit block testing confirmed, and cryoablation was used to encircle the left PVs ensuring overlap with the superior PV and inferior PV connecting lesions created by RF ablation. In the MS, bipolar RF clamps were used to isolate both the right and left PVs, with exit block testing confirmed bilaterally. The second difference was the right-sided ablation set. In the RMT, the right-sided ablation set was performed via 3 purse strings. In the MS, the right-sided lesion set was performed via 1 atriotomy and 1 purse string. Finally, femoral cannulation was used for the RMT and central bicaval cannulation for the MS patients.
Rhythm Monitoring
Freedom from atrial tachyarrhythmias (ATAs) was assessed with electrocardiogram and prolonged monitoring using a Holter monitor, pacemaker (PPM) interrogation, or implantable loop recorder for up to 8 years. 20 Failure was defined based on current HRS guidelines, as any episode of ATAs lasting greater than 30 seconds outside of the 3-month blanking period. 20 To better describe long-term rhythm outcomes, our group and others have reported rhythm outcomes at each annual follow-up evaluation.22,23
Anticoagulation and antiarrhythmic drugs (AADs) were initiated in all patients in the postoperative period, and cardioversion before discharge was performed in patients with ATAs unresponsive to AADs, unless contraindicated. 24 Dual-chamber PPM were implanted in patients with symptomatic bradycardia who failed to recover from persistent bradycardia, complete heart block, or junctional rhythms after 5 to 7 days.
At follow-up, AADs were discontinued after 2 to 3 months if the patient remained in normal sinus rhythm (NSR), and anticoagulation was discontinued after 3 to 6 months if a patient was both in NSR and had no LA stasis or thrombus documented by echocardiography, irrespective of the patient’s CHA2DS2-VASc score. 25
Statistics
Continuous variables were expressed as mean ± standard deviation (SD) or as median with interquartile range, and a Student’s t test was used for comparisons. Categorical variables were expressed as frequencies and percentages, and a chi-square test was used for comparisons. A P value <0.05 was considered statistically significant.
Propensity score matching (PSM) was conducted with RMT patients matched 1:1 to MS patients. The propensity score was calculated via logistic regression including comorbid variables (Table 2) and calculating the likelihood of a patient undergoing MS; caliper width was 0.05 (0.24 times the SD of the logits of the propensity score), and matching was optimized for closeness. From the original RMT cohort of 144, 28 participants were excluded for lack of an appropriate match, with a final propensity-matched cohort of 232 participants. Covariate balance before and after PSM was evaluated using the distribution of propensity scores and P value between cohorts (Table 2). Statistical analyses were performed using SAS Studio 3.8 on SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
Baseline Demographics.
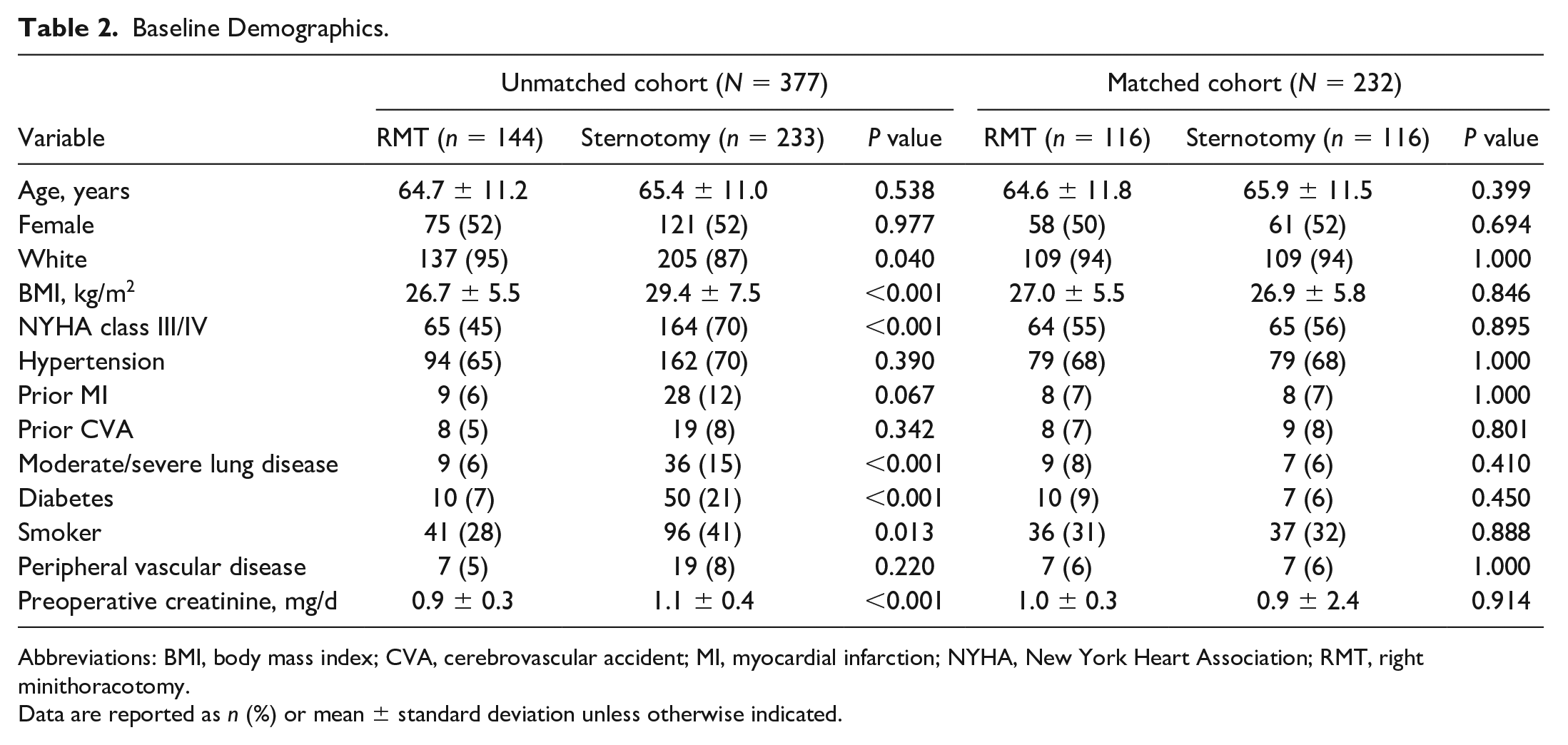
Abbreviations: BMI, body mass index; CVA, cerebrovascular accident; MI, myocardial infarction; NYHA, New York Heart Association; RMT, right minithoracotomy.
Data are reported as n (%) or mean ± standard deviation unless otherwise indicated.
Composite endpoint survival was reported as a Kaplan–Meier estimate. The Fine–Gray test for competing risk analysis was used to compare the incidence of first ATA recurrence, with death during the follow-up period serving as the competing risk. Univariable and multivariable Fine–Gray regression was used to identify predictors of first ATA recurrence in 21 perioperative variables. Univariates that with P values ≤0.05 were chosen for the multivariable analysis. Fine–Gray test and Fine–Gray regression were performed using R4.2.2 and the tidycmprsk package (R Foundation for Statistical Computing, Vienna, Austria).
Results
Demographics
The average age in the unmatched cohort (N = 377) was 65 ± 11 years. Most patients were White (91%, 342 of 377) and female (52%, 196 of 377). Of the patients, 92% (349 of 377) underwent a bilateral CMP-IV and 8% (28 of 377) had a left-sided CMP. Nonparoxysmal AF was reported for 59% of patients (222 of 377), of whom 42% (156 of 377) had LSPAF and 17% (66 of 377) had persistent AF. The other 42% of patients (155 of 377) had paroxysmal AF. After PSM, 116 matched pairs had no significant differences in baseline covariates (Table 2).
AF and Hemodynamics
In the matched cohort, there was no statistical difference in the proportion of patients with nonparoxysmal AF (P = 0.230), duration of AF (P = 0.151), preoperative PPM (P = 0.473), or prior catheter ablation (P = 0.370) between the RMT and MS cohorts (Table 3). Patients who had an RMT had a higher LVEF (58.7% ± 10.0% vs 55.8% ± 11.3%, P < 0.032) and smaller LA diameter (4.9 ± 1.1 cm vs 5.4 ± 1.1 cm, P < 0.001) compared with the MS cohort (Table 3). The MS cohort had significantly more patients who underwent concomitant TV surgery (P = 0.012; Table 1). The most common valve etiology for MV surgery was degenerative disease, followed by rheumatic disease (Supplemental Table 1).
AF and Hemodynamic Characteristics.
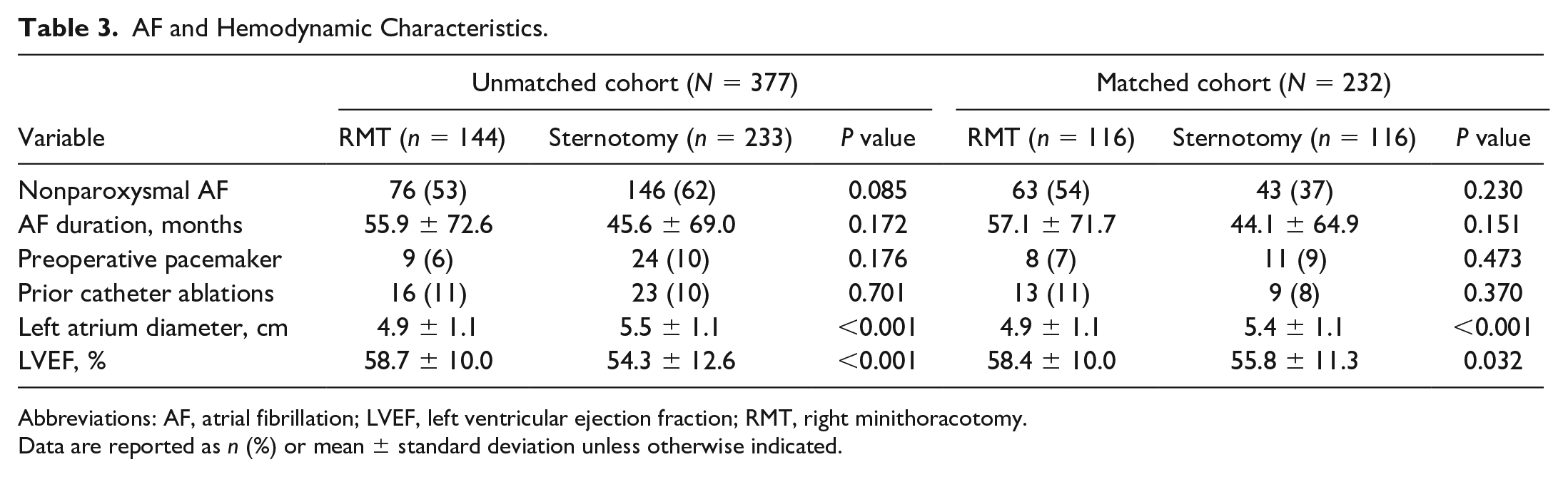
Abbreviations: AF, atrial fibrillation; LVEF, left ventricular ejection fraction; RMT, right minithoracotomy.
Data are reported as n (%) or mean ± standard deviation unless otherwise indicated.
Perioperative Outcomes
For the matched cohort, there were no significant differences between the RMT and MS cohorts in 30-day mortality (p = 0.651), cerebrovascular accident (p = 0.316), intra-aortic balloon pump (p = 0.734), intraoperative blood transfusions (p = 0.078), reoperation for rebleeding (p = 0.175), pneumonia (p = 0.122), AKI (p = 0.534), or renal failure requiring dialysis (p = 0.732; Table 4).
Perioperative Outcomes.
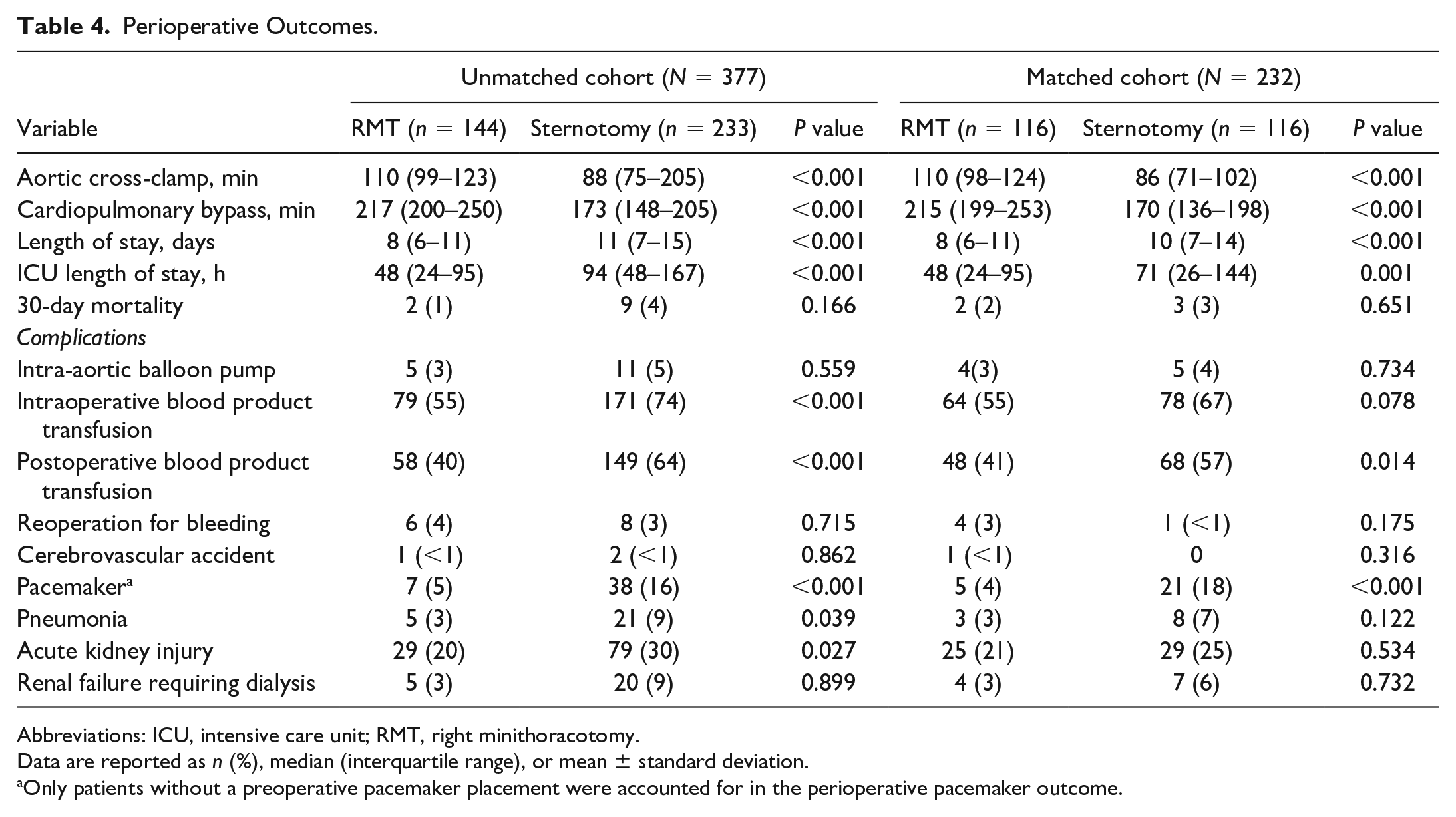
Abbreviations: ICU, intensive care unit; RMT, right minithoracotomy.
Data are reported as n (%), median (interquartile range), or mean ± standard deviation.
Only patients without a preoperative pacemaker placement were accounted for in the perioperative pacemaker outcome.
The RMT matched cohort had longer cardiopulmonary bypass time (p < 0.001) and aortic cross-clamp time (p < 0.001). Despite the increased operative times, the RMT cohort had a shorter length of stay (p < 0.001) and shorter ICU length of stay (p = 0.001). The MS cohorts had more postoperative transfusions (68 [57%] vs 48 [41%], p < 0.014) and PPM placed (21 [18%] vs 5 [4%], p < 0.001) compared with the RMT cohort (Table 4). The overall PPM placement rate was 11% (26 of 232), and the most common etiology for PPM in the MS cohort was sick sinus syndrome (71%, 15 of 21), followed by complete heart block (29%, 6 of 21). For the RMT cohort, 60% of the PPM (3 of 5) were placed for complete heart block and 40% (2 of 5) were placed due to sick sinus syndrome.
Rhythm Outcomes and Follow-Up
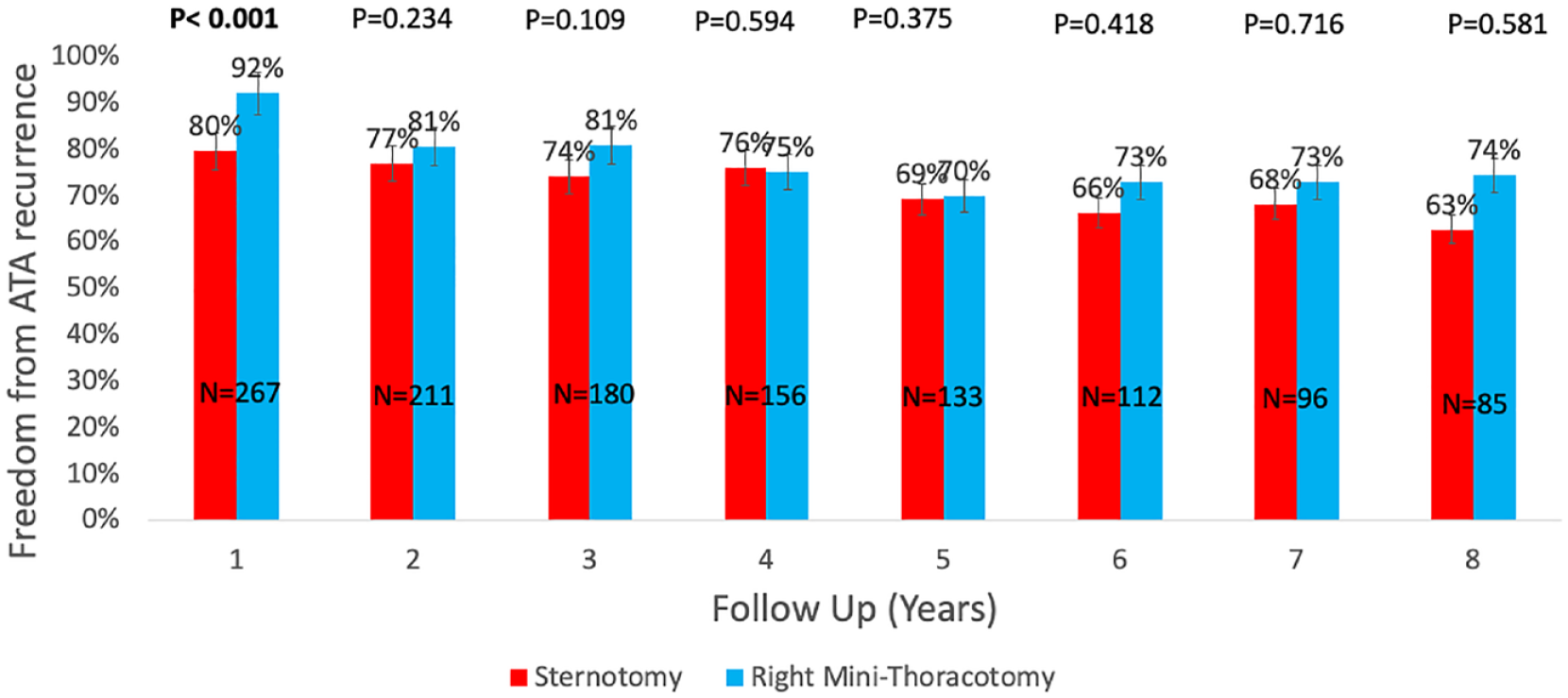
Patients who had an RMT had significantly greater overall freedom from ATA recurrence at 1 year (99% [125 of 126] vs 90% [159 of 176], p = 0.001; Fig. 1) and at 1 year off AADs (92% [116 of 126] vs 80% [140 of 176], p < 0.001; Fig. 2). In addition, those who had an RMT had greater overall freedom from ATA recurrence at 3 years (94% [84 of 89] vs 86% [109 of 127], p = 0.045; Fig. 1). All other years had no significant difference in the overall freedom from ATAs on or off AADs based on surgical approach (Fig. 1, Fig. 2).

Overall freedom from ATA recurrence. At 1 year and 3 years, the right minithoracotomy cohort (blue) had a significantly higher freedom from ATA recurrence compared with the sternotomy cohort (red). ATA, atrial tachyarrhythmia.
Freedom from ATA recurrence off antiarrhythmic drugs. At 1 year, the right minithoracotomy cohort (blue) had a significantly higher freedom from ATA recurrence compared with the sternotomy cohort (red). ATA, atrial tachyarrhythmia.
The mean follow-up time was 5.6 ± 4.4 years. Of the patients, 8% patients (30 of 377) were lost to follow-up (10 RMT and 20 MS patients) with missing data at every annual follow-up time, and they were excluded from the long-term rhythm analysis. For all included patients, there were no rhythm data points missing for years 3, 6, and 7. However, at years 1, 2, 4, 5, and 8, there were 37, 35, 33, 32, and 30 rhythm data points missing, and therefore, those specific times for those specific patients were excluded from the long-term rhythm outcome analysis.
For the overall cohort (N = 377), prolonged monitoring was completed at 1, 5, and 8 years for 70% (212 of 302), 60% (97 of 164), and 47% (50 of 106) of patients, respectively (Supplemental Table 2). At 1, 5, and 8 years based on surgical approach, the RMT cohort had 83% (104 of 126), 67% (47 of 70), and 62% (24 of 39) of patients who received prolonged monitoring, while the MS cohort had 62% (108 of 176), 53% (50 of 94), and 39% (26 of 67) of patients who received prolonged monitoring (Supplemental Table 3). The number of patients who underwent prolonged monitoring at each time point and the type of prolonged monitoring used is described in detail in Supplemental Table 2 and Supplemental Table 3. Our success rate defined as freedom from ATA recurrence, for patients with prolonged monitoring versus without prolonged monitoring, was 97% versus 87% at 1 year (p = 0.003) and 87% versus 85% (p = 0.782) at 5 years. There were 59 ATA recurrences, including 16% in the RMT cohort (24 of 144) and 15% in the MS cohort (35 of 233, p = 0.884). Of all ATA recurrences, 85% were AF (50 of 59) and 15% were atrial flutter (9 of 59).
Survival and Predictors of ATA Recurrence
At 8 years, there was no composite endpoint survival difference found between the approaches (Gray test, p = 0.072; Fig. 3). Furthermore, over the 8 years, there was no difference between cumulative incidence of ATA recurrence found between the approaches (Gray test, p = 0.400; Fig. 4). On multivariable analysis, age (subhazard ratio [SHR] = 1.06, 95% confidence interval [CI]: 1.03 to 1.09, p < 0.001), LA diameter (SHR = 1.40, 95% CI: 1.14 to 1.71, p = 0.001), and AF duration in years (SHR = 1.05, 95% CI: 1.01 to 1.10, p < 0.018) were all independent predictors of ATA recurrence (Table 5).
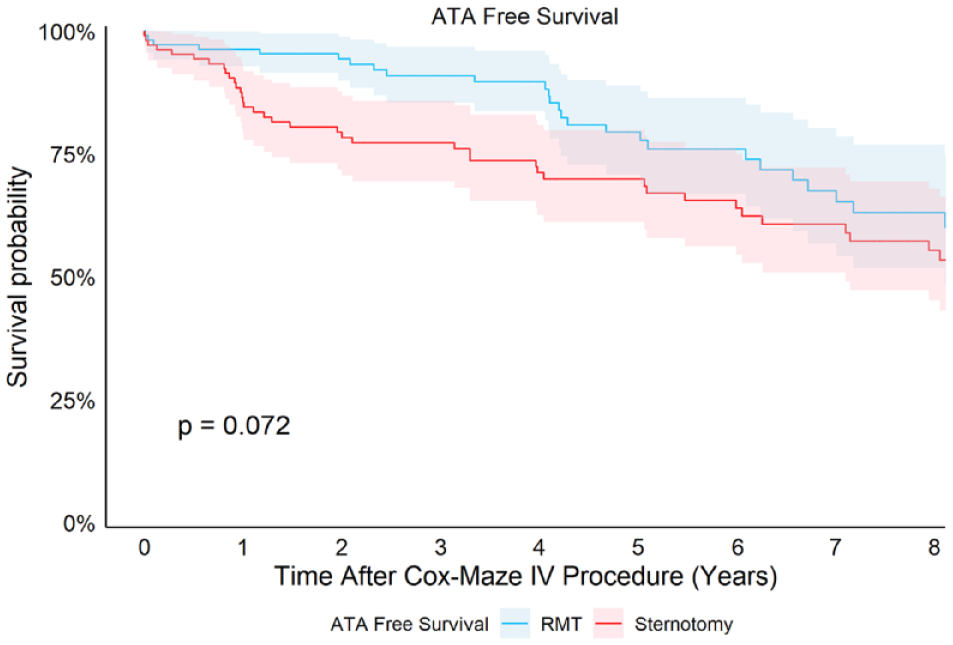
ATA recurrence-free survival. Composite endpoint survival (freedom from ATA recurrence and death) reported as a Kaplan–Meier estimate (Fine–Gray test, P = 0.072). ATA, atrial tachyarrhythmia; RMT, right minithoracotomy.
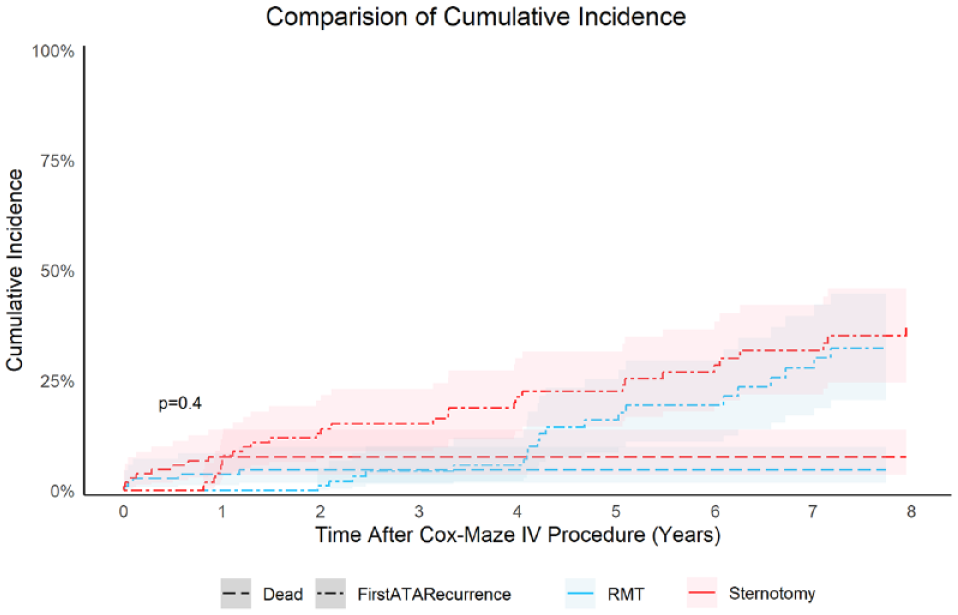
Cumulative incidence function curves showing the competing risk of first ATA recurrence in the RMT (blue) and sternotomy (red) cohorts (Fine–Gray test, P = 0.400). ATA, atrial tachyarrhythmia; RMT, right minithoracotomy.
Univariable and Multivariable Predictors of ATA Recurrence.
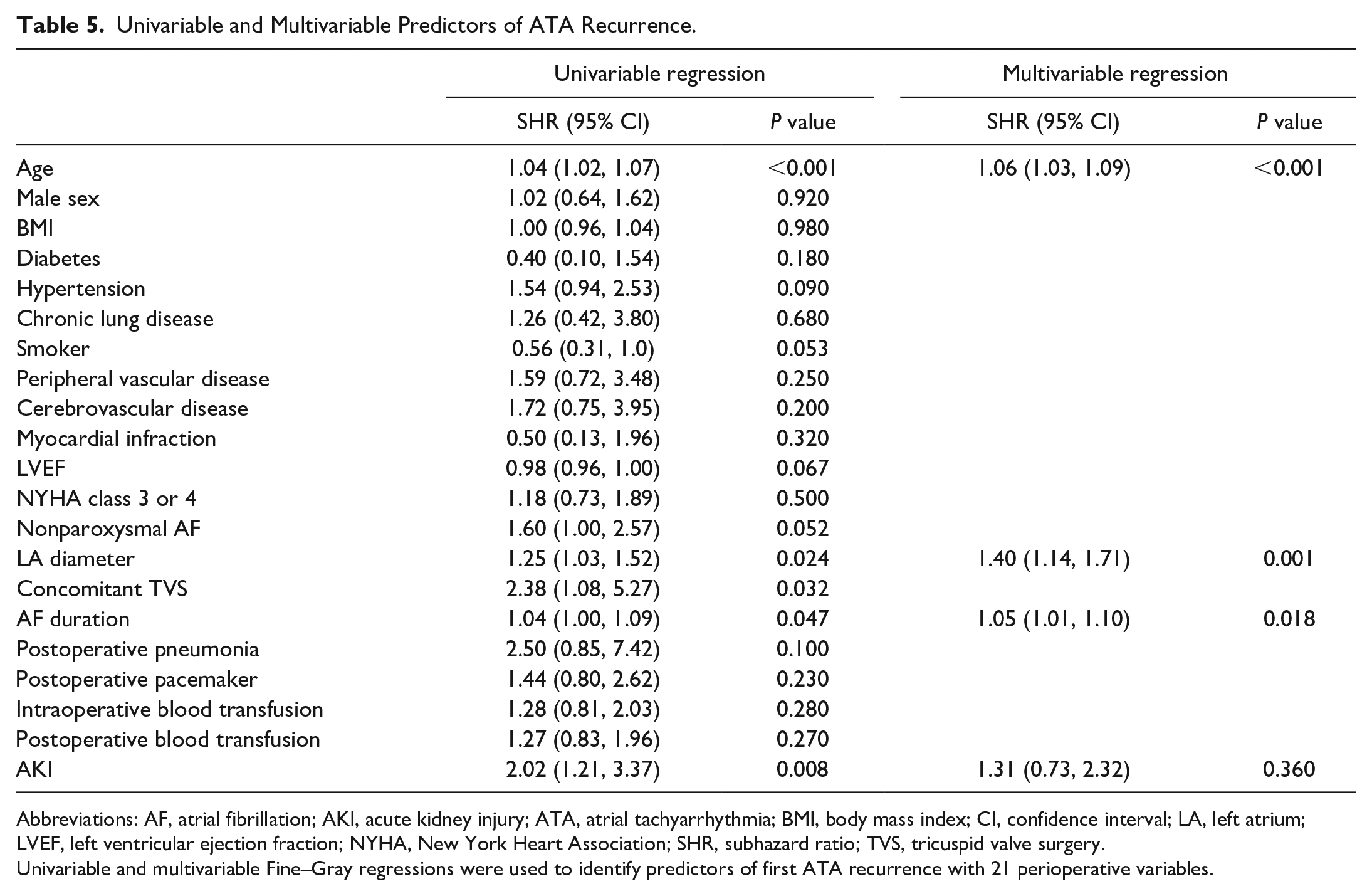
Abbreviations: AF, atrial fibrillation; AKI, acute kidney injury; ATA, atrial tachyarrhythmia; BMI, body mass index; CI, confidence interval; LA, left atrium; LVEF, left ventricular ejection fraction; NYHA, New York Heart Association; SHR, subhazard ratio; TVS, tricuspid valve surgery.
Univariable and multivariable Fine–Gray regressions were used to identify predictors of first ATA recurrence with 21 perioperative variables.
Discussion
Patients who had an RMT had a higher early overall freedom from ATA recurrence at 1 and 3 years compared with the MS cohort (Fig. 1, Fig. 2). The late freedom from ATA recurrence on or off AADs was not significantly different between surgical approaches. These early rhythm findings differ from what has been reported in the literature with fewer patients. In a study by Jiang et al., 69 RMT and 83 MS patients who underwent MV surgery and concomitant CMP had no difference in NSR reported at 2 years (82% RMT vs 89% MS). 16 Similarly, in another study, RMT and MS patients who underwent concomitant CMP and MV surgery had no significant difference in the freedom from ATA recurrence at any time up to 2 years. 17 Both studies had limited follow-up and unmatched cohorts.
There are several explanations for the better early rhythm outcomes in the RMT cohort. Age, LA diameter size, and AF duration were found to be predictors for ATA recurrence. Of these factors, patients in the RMT cohort had a smaller LA diameter, which may have contributed to greater early freedom from ATA recurrence compared with patients in the MS cohort. However, there were no differences in any other AF or hemodynamic characteristics that would have influenced differences in ATA recurrence. Another study comparing the 2 surgical approaches also found LA diameter to be a predictor of ATA recurrence. 17 Second, patients who were selected for the RMT had a lower risk profile, as shown in Table 1. Third, the RMT approach became more commonly performed over the past 2 decades. From 2004 to 2014, 32% of concomitant MV surgery and ablation cases (58 of 179) were performed via RMT, compared with 43% of cases (86 of 198) performed from 2014 to 2021. Finally, our most experienced surgeon performed most of the RMT cases. While all these variables may have influenced our outcome data, we initially performed this analysis to ensure that we could obtain similar results with the RMT approach along with lower morbidity. There were no differences in 30-day mortality, composite endpoint survival, or cumulative incidence of first ATA recurrence. Our data strongly support the fact that the minimally invasive approach did not compromise procedural efficacy and had significantly lower morbidity. Despite longer operative times, the RMT cohort had decreased morbidity with shorter ICU and hospital length of stay. These findings were consistent with the 2 studies mentioned above.16,17 Furthermore, the RMT cohort had less postoperative blood transfusions, a finding consistent with the Jiang et al. study. 16 An interesting finding in our study was the difference in permanent PPM rate between the surgical approaches (18% MS vs 4% RMT). Although the overall PPM rate of 11% is comparable to previously reported rates in the literature for concomitant MV surgery and CMP-IV,2,12,16,17,26,27 the PPM difference between these 2 surgical approaches has not been reported.
In our study, the most common overall reason for PPM was sick sinus syndrome, which was highest in the MS cohort. The normal aging process has been described as the underlying cause for a dysfunctional sinus atrial node that is unmasked after the surgical ablation of AF. 28 Others studies have reported predisposing risk factors for PPM such as longer duration of AF, nonparoxysmal AF, New York Heart Association class III/IV heart failure, and concomitant TV surgery.2,28,29 The MS cohort had larger LA diameters and more concomitant TV surgery (Table 1, Table 3). The differences in surgical and ablation techniques of the RMT and MS approaches could be an additional reason to explain the perioperative PPM rates and further studies are needed. In the RMT approach, less manipulation of the right atrium occurs with femoral instead of bicaval venous cannulation, lateral endoscopic assistance instead of an open approach, and with purse-string access instead of an atriotomy for ablation.
There are a few limitations. PSM was done in an attempt to balance baseline demographics. However, we cannot exclude the possibility that there was selection bias for lower-risk patients to undergo the RMT. Second, as in any large institution, surgeon experience in performing the CMP-IV varied. Although 10 surgeons performed all concomitant ablation and MV surgeries, 96% of the operations (361 of 377) were performed by the most experienced CMP surgeons (5 of 10 surgeons). Of these 5 experienced CMP surgeons, 3 performed both RMT and MS approaches, and thus surgeon experience was less likely to influence our results. However, most of the RMT cases (98%, 141 of 144) were performed by our most experienced surgeon, and this may have had an influence on our results. Third, this is a single-institution retrospective cohort study, and due to the study design, it lacked randomization of patients into the RMT versus MS cohorts. Fourth, patients reported rhythm outcomes as a combination of prolonged monitoring and electrocardiogram monitoring, with most of the office visits consisting of prolonged monitoring at both early and late follow-up. Despite this, early rhythm outcomes were different, and this study is one of the most comprehensive follow-ups ever reported for concomitant AF ablation in patients with MV disease.
Conclusions
Both the RMT and MS approach had excellent long-term rhythm outcomes, with more than 80% of patients having freedom from ATA recurrences at 7 years. Both approaches had similar late rhythm and ATA recurrence outcomes. However, the RMT cohort had a higher early 1-year and 3-year freedom from ATA recurrences despite longer operative times. Furthermore, the RMT approach was associated with less morbidity and thus should be strongly considered in selected patients at centers with expertise in minimally invasive techniques.
Supplemental Material
sj-pdf-1-inv-10.1177_15569845231209974 – Supplemental material for Minimally Invasive Mitral Valve Surgery With Concomitant Cox Maze Procedure Is as Effective as a Median Sternotomy With Decreased Morbidity
Supplemental material, sj-pdf-1-inv-10.1177_15569845231209974 for Minimally Invasive Mitral Valve Surgery With Concomitant Cox Maze Procedure Is as Effective as a Median Sternotomy With Decreased Morbidity by Tari-Ann Yates, Martha McGilvray, Connor Vinyard, Laurie Sinn, Nicholas Razo, June He, Harold G. Roberts, Matthew R. Schill, Christian Zemlin and Ralph J. Damiano in Innovations
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ralph J. Damiano, Jr, MD, is a consultant for Medtronic and Edwards Lifesciences and a speaker for AtriCure Inc.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Ralph J. Damiano, Jr, MD, has received funding for this study through Barnes Jewish Hospital Foundation and NIH R01 HL032257.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.