
Abstract
Objective:
Extracorporeal circulation (ECC) is generally based on standards established in the last decade. In recent years, a concept of perfusion management during ECC, goal-directed perfusion (GDP), has emerged to create optimal conditions for oxygen delivery and extraction, initiated by Rannuci et al. The aim of the present work was to determine whether the ECC procedure can truly be optimized with the current state of knowledge and understanding of human physiology.
Methods:
Discussed articles from 2017 to 2022 were selected from the MEDLINE (PubMed) database using the keywords “cardiopulmonary bypass” AND “cardiac surgery” AND “oxygen delivery” with the conditions of “clinical trial” OR “randomized controlled trial.”
Results:
The concept of GDP is an attempt to reproduce the physiological conditions of tissue respiration during ECC. Published articles, also due to their retrospective nature, are based on standards and recommendations that do not fully fit the field of physiological circulation. There are still insufficient tools to assess the relationship between volemia, perfusion pressure, and pump performance. Limitations include indications for vasoactive drugs. Methodology has rarely taken into account the period of starting and stopping the heart-lung machine, the most pronounced periods of circulatory destabilization with reduced oxygen delivery.
Conclusions:
Problems associated with ECC such as acute kidney injury, liver failure, vasoplegic syndrome, and others must await its resolution. The use of advanced monitoring technology and data engineering may allow the development of baseline hemodynamic models, which may make the ECC procedure more physiologic and thus improve the safety of the procedure.
Keywords
Central Message
The use of advanced monitoring technology and data engineering may allow the development of baseline hemodynamic models, which may make the extracorporeal circulation procedure more physiologic and thus improve the safety of the procedure.
Introduction
The widely accepted extracorporeal circulation (ECC) procedure is based on specific guidelines and standards for perfusion management established by the American Society of Extracorporeal Technology (AmSECT). Perfusion management according to the last published edition of the 2013 recommendations remains unchanged despite updates in 2015 and 2017, with all attention focused on pump design and its adjustable parameter, pump flow.1,2 During the ECC period, the patient remains under the care of cardiac surgeons and anesthetists, who have common, but sometimes conflicting, therapeutic goals. The main point of contention is the level of blood pressure. For cardiac surgeons, blood pressure that is too high complicates the procedure by increasing bleeding in the surgical field or making it difficult to perform invasive vascular access. However, for anesthetists, the overriding goal is to maintain a sufficiently high tissue perfusion. In contrast, perfusion pressure, the stabilization of which is the primary goal of therapy in the treatment of intensive care unit (ICU) patients, becomes a secondary, poorly-defined parameter during ECC.3–5 Unlike the ICU, where cardiovascular therapy is based on extensive diagnostic capabilities, hemodynamic monitoring during EEC is very limited. Therefore, it is very difficult to determine the relationship between adequate pump output, systemic vascular resistance, and blood pressure. As a result, the pump flow rate is often not adapted to the actual hemodynamic conditions, and vasoconstrictors are overused to increase blood pressure.1,2,6,7
In recent years, a concept of perfusion management during ECC, goal-directed perfusion (GDP), has emerged to create optimal conditions for oxygen delivery (DO2) and extraction, initiated by Rannuci et al. 8 Based on his observations of renal function and DO2 during ECC, the model of adequate tissue perfusion and optimal DO2 during ECC is proposed. There are many doubts as to whether the new GDP methodology is based on a solid foundation for understanding and restoring human physiology in the newly created hemodynamic system, the patient-heart-lung machine model. The aim of the present work was to determine whether the ECC procedure can be truly optimized with the current state of knowledge and understanding of human physiology. The key question is whether modern methods of patient monitoring during ECC and data science methodology can be used to create more physiological hemodynamic algorithms adapted to the physiology of each individual patient.
Methods
Articles were selected from the MEDLINE (PubMed) database at the time of the search using the keywords “cardiopulmonary bypass” AND “cardiac surgery” AND “oxygen delivery” with the conditions of “clinical trial” OR “randomized controlled trial” (Table 1). All articles published between 2017 and 2022 were considered for inclusion. Only articles published in English were included. A brief overview of ECC, clinical issues, and changes introduced by GDP is provided.1,2,9
Publications Found in the PubMed Database Using Keywords “Cardiopulmonary Bypass” AND “Cardiac Surgery” AND “Oxygen Delivery.”
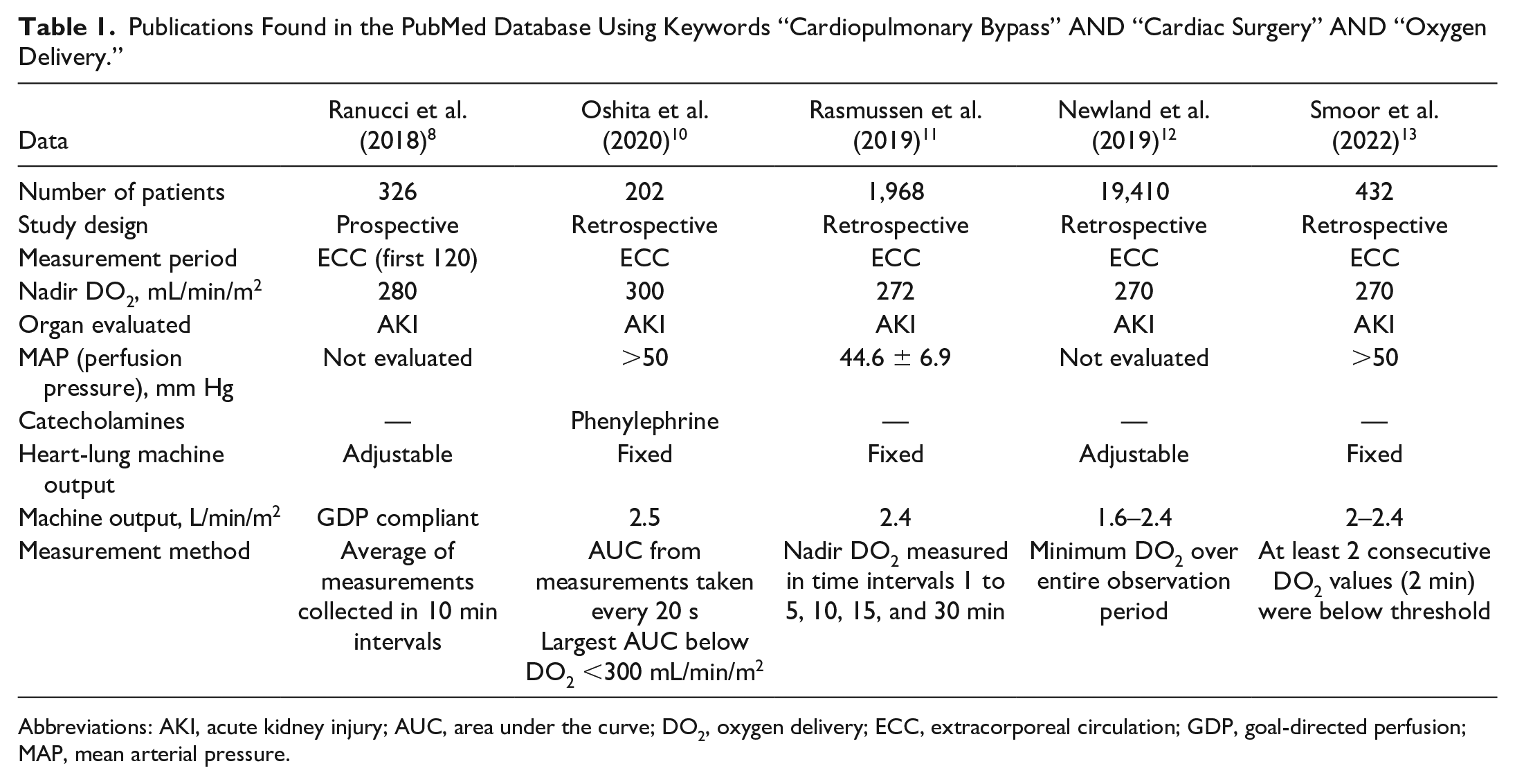
Abbreviations: AKI, acute kidney injury; AUC, area under the curve; DO2, oxygen delivery; ECC, extracorporeal circulation; GDP, goal-directed perfusion; MAP, mean arterial pressure.
ECC Protocols
Current ECC protocols are mainly based on guidelines from the 1990s, and their latest update has not changed the basic concepts.1,2,9 It is still recommended to calculate the pump flow from body surface area (BSA) for all patients, regardless of age or sex. The latest European recommendations also support the concept of determining heart-lung machine performance based on BSA but allow the pump flow, previously kept constant at 2.4 to 2.5 L/min/m2, to be adjusted to ensure adequate organ perfusion and optimize DO2 and extraction.1,2,9 However, recommendations still do not define the appropriate values for optimal perfusion pressure or DO2. Other methods of assessing ECC are the results of biochemical and diagnostic tests with assessment of lactate levels and cerebral oximetry.1,2,9,14 The definition of adequate perfusion pressure during ECC remains undefined. This appears to be difficult to determine as the minimum perfusion pressure varies from organ to organ as well as from person to person and depends on the underlying disease.4,5,14
What Is GDP?
GDP is an ECC concept in which the target for tissue perfusion is defined as a minimum DO2 threshold to ensure proper tissue respiration and maintain organ function during the perioperative period. This concept is based on modern in-line monitoring methods that continuously collect data on oxygen transport in the body and also facilitate the estimation of the difference in gas content between the ECC venous system and the arterial system.
Results
There are methodological and computational limitations in determining normal tissue perfusion and DO2.
Perfusion Pressure
Studies evaluating oxygen transport in the ECC neglect the issue of perfusion pressure. The problem arises from the lack of strict standards and a universally accepted minimum mean arterial pressure (MAP) of 50 mm Hg.1,2,9 It would seem that if we know the pump flow rate and the arterial blood gas results, we have all the necessary data to calculate DO2 and extraction. However, the driving force for the blood to overcome the systemic vascular resistance that is the determinant of adequate tissue respiration is the perfusion pressure.3–6 In addition, because of the lack of knowledge about the relationship between pump flow, blood rheological properties, and systemic vascular resistance, catecholamine therapy is often used during ECC to achieve the desired blood pressure. The risk of microcirculatory occlusion and even counterproductive effects such as worsening of DO2 is associated with the overuse of vasoconstrictors.3–6 Although there are no well-defined standards for the appropriate minimum perfusion pressure for ECC, it is increasingly recognized that a level of 50 mm Hg is still too low to maintain renal function. 5 Therefore, the accepted perfusion pressure is more likely to correspond to the experience of normal renal perfusion and should be greater than 65 mm Hg.5,15,12 It is inexplicable that the articles describing tissue DO2 omit perfusion pressure from their basic assumptions (Table 1).8,10–14 The microcirculation is not taken into account; only the correct DO2 and extraction rate are determined. In the case of hypotension or excessive use of vasoconstrictors, the microcirculation may remain occluded, giving an apparently normal oxygen extraction. In this case, neither the pump flow rate nor the venous blood saturation (oxygen extraction rate) can fully describe the adequacy of tissue perfusion.4,16
According to the equation, DO2 in GDP depends on the oxygen content of the blood—the hemoglobin level—and also on the pump flow rate. An increase in blood volume and viscosity, as well as an increase in blood flow, leads directly to an increase in perfusion pressure. However, MAP is either not considered at all in the clinical observations performed, or it is considered in advance to be of no importance for proper oxygen transport and delivery (Table 1).8,10–14
Cardiac Surgery Procedure
Advances in cardiac surgery require the perfusionist to reduce or even temporarily stop blood flow to the heart-lung machine. As a result of such surgical manipulations, the inevitable pharmacologic effects cause temporary destabilization and pressure drops. The beginning and end of ECC appear to be the most critical for hemodynamics and oxygen transport. These momentary drops in blood flow may cause organ dysfunction in the mechanism of hypoperfusion, regardless of the concept of perfusion pursued. The widely reported results of various studies usually do not cover the entire period of connection to the heart-lung machine but only the ECC period during aortic cross-clamping (Table 1).
Figure 1 shows the measurements taken at 10 s intervals to determine DO2 in relation to hemoglobin level and cardiac index during 270 ECC procedures. 7 Each point on the graph is described by 3 parameters: DO2, hemoglobin level, and pump flow. These inseparable parameters occupy the entire graph, even in the areas of nonphysiological low DO2, because there are expected decreases in all ECC procedures, as previously mentioned. 7 These decreases are mainly due to the reduction in pump flow, as other factors such as hemoglobin level, saturation, and oxygen content are usually kept constant during ECC.
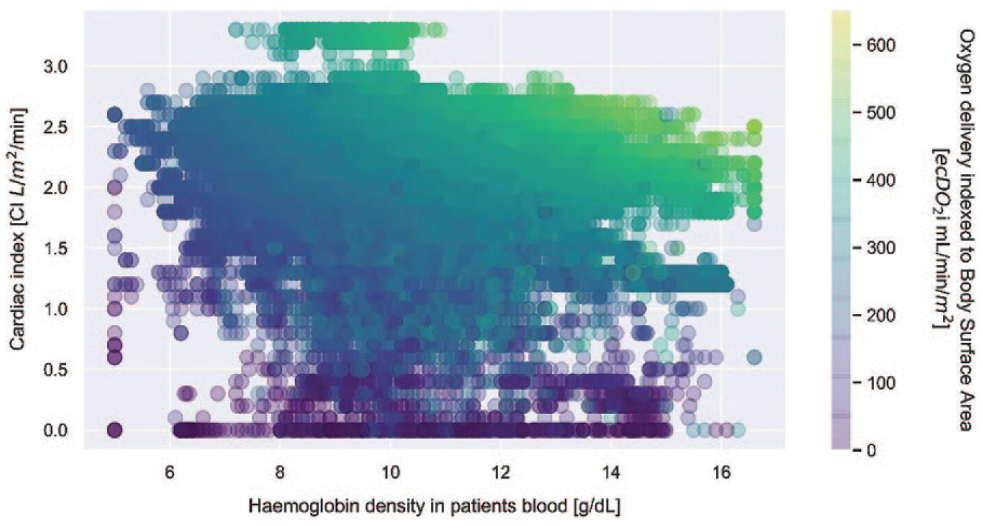
A full set of the cardiac index data during extracorporeal circulation, in the function of hemoglobin density and tissue oxygen delivery for patients with mixed venous oxygen saturation above 68% and mean arterial pressure above 60 mm Hg. Oxygen delivery has been illustrated with color, where the darker shades correspond with lower values. Image reprinted with no modifications from Lukaszewski et al., “The use of data science to analyse physiology of oxygen delivery in the extracorporeal circulation,” BMC Cardiovasc Disord, 2019, under the terms of the CC BY 4.0 license. 7
Calculation Limitations
The calculation method based on averaging the ECC periods of oxygen transport to the tissues is a serious limitation of the sensitivity of the tests and the assessment of GDP efficiency. As a result, data analysis is limited and can lead to errors. Even a very short period of hypoperfusion, which is not taken into account by averaging, can lead to organ dysfunction (Fig. 2). It should be noted that visceral perfusion is characterized by a certain inherent organ resistance to transient disturbances in blood flow. Restoration of blood flow then allows visceral function to be restored, with possible periods of transient dysfunction. On the other hand, the brain is extremely sensitive to hypoperfusion, which can be a much greater problem during the ECC procedure. For this reason, the averaging method may not be a suitable tool for calculating and evaluating DO2. 17
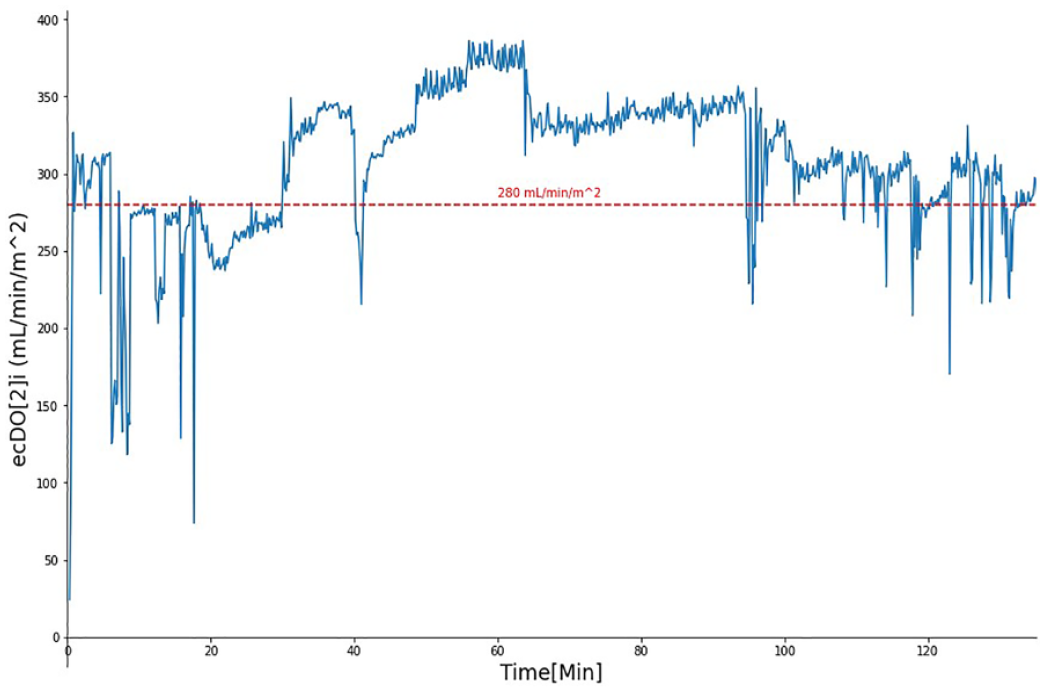
Example of DO2 measurements collected at 10 s intervals. On the y axis is DO2, on the x axis is elapsed time, and the red line in the graph is the recognized lowest DO2 level for renal dysfunction. DO2 measurements collected by in-line noninvasive real-time monitoring System M (Spectrum Medical, Gloucester, UK) during extracorporeal circulation procedure. DO2, oxygen delivery.
Discussion
This article has attempted to show that the physiology of ECC is misunderstood. There is no other circulation and its physiology, whether the driving force is the heart or a mechanical device. Scientific observational papers report information randomly and show superficial correlations, as in the case of the cited publications (Table 1). The main problem in estimating which parameter is more important comes from the physiological relationships between them. For example, increasing pump output increases perfusion pressure; increasing hemoglobin level increases blood viscosity, systemic resistance, and perfusion pressure. There is no way to determine whether the physiological state is being maintained by adequate DO2 or by adequate blood viscosity and blood flow, which translates into systemic pressure.
From the formula for DO2, it is easy to deduce that we could calculate a recognized minimum level of DO2 of 280 mL/min/m2:
280 mL/min/m2 = 2.4 L/min/m2 (average cardiac output) × 1.3 × (average hemoglobin level during ECC – 90 g/L)
Such averaged parameters during ECC give a statistically correct perfusion pressure also during ECC. Therefore, statistics on very large groups of patients will report this value of DO2 as the most physiological. Similarly, in the Magruder et al. publication, this most optimal and near-average physiological state will provide the statistical effect. 18 But to return to the large study under physiological conditions, the basis for proper cellular respiration is proper perfusion; in the case of the kidney, the perfusion pressure should be above 65 mm Hg. 5
The assumptions of the GDP concept are logical and based on the physiological basis of tissue respiration and oxygen transport. However, failure to include the correct perfusion pressure in the calculations reduces the specificity of the observations presented (Table 1). Low perfusion pressure occludes the microcirculation, and the use of vasoconstrictors in the presence of inadequate blood volume and cardiac output may further increase tissue damage.3,5,19–21 Table 1 lists publications assessing oxygen transport and its impact on postoperative kidney function. The methodological limitations described above were repeated in all publications that were found. The authors present the perfusion pressure value as an average over the whole observation, not as an instantaneous value. In addition, the exact period of DO2 measurements is not specified (whether it concerns the entire ECC procedure or only the aortic cross-clamp period) and the use of vasoconstrictive drugs is not taken into account. Finally, the authors analyze the arithmetic mean of measurements taken at different time intervals.8,10 –13
The concept of GDP is an attempt to reproduce the physiological conditions of tissue respiration during ECC. However, to apply this concept in practice, it is necessary to know the correct hemodynamic relationships in the patient-heart-lung machine model. This is a very difficult task when we compare ECC therapy with the possibility of hemodynamic diagnosis and treatment of ICU patients in hemodynamic shock. We still do not have sufficient tools to assess the correlation between volemia, cardiac output, and systemic vascular resistance. 3 Therefore, the goal of cardiovascular therapy in hemodynamic shock according to the Surviving Sepsis Campaign guidelines is to maintain MAP (i.e., perfusion pressure) with fluid therapy, improved cardiac output, and the use of catecholamines.3,5,7,22,23 However, ultimately the validity of the applied cardiovascular therapy is confirmed by the basic clinical indicators of normal organ function, such as renal excretory function and correct arterial blood gas results, including lactate levels.
The data presented in Table 1 use statistical averaging to define circulatory parameters in ECC based on DO2. However, it is not the average result that is important for patient management but rather the optimization of treatment, which is more like a Gaussian curve. A more flexible approach to machine performance is needed; even in human physiology, the range of normal cardiac output is twice as wide, blood viscosity and hemoglobin levels need to be taken into account, higher perfusion pressure is required, and vasoconstrictors need to be used much more carefully.
The introduction of modern monitoring methods and the ability to analyze a huge medical database using data science tools has revealed new limitations of current therapeutic standards (Fig. 1, Fig. 2). The monitoring of hemodynamics and oxygen transport during ECC is an excellent example of technical excellence introduced into medical practice. In contrast to the intensive care patient, the performance of ECC with the use of extensive in-line monitoring allows a more precise determination of hemodynamic dependencies. 22 In the case of patients connected to the heart-lung machine, thanks to structural data (oxygen supply and extraction, CO2 production, cardiac output, perfusion pressure) and nonstructural data (age, sex, body mass index, additional diseases), taking into account the use of modern data analysis possibilities with large databases, including data science, it is possible to create basic hemodynamic models on the basis of which it will be possible to perform the ECC procedure in a more physiological way. 6 We believe that the goal of GDP should be to create such optimal hemodynamic conditions in which it will be possible to maintain correct perfusion through the microcirculation by adjusting the optimal projection to the volemia and the pressors used.6,7,24–27 Currently, the generally accepted pump flow rate is 2.4 L/min/m2, irrespective of the patient’s sex, age, anthropometric characteristics, and disease burden. The lack of consideration of perfusion pressure, indicators of systemic vascular resistance, and indications for the use of catecholamines seems to be an extreme medical archetype in the GDP concept. With data science, an analysis of the relationship between machine output, perfusion pressure achieved, hemoglobin and blood viscosity levels, and microperfusion assessment, performed on a sufficiently large group of matched patients, can generate physiological patterns. Based on these patterns, the creation of hemodynamic models of ECC could be performed in a more physiological manner by adapting the appropriate machine output to cardiovascular physiology and reducing the often-abused toxic use of vasoconstrictor doses.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.