
Abstract

Introduction
Median sternotomies must be safely and steadily fixed from the operating room to guarantee the adequate recovery of patients. Sternal fixation using wires is the most commonly used technique because it is inexpensive, quick, and relatively safe. However, wires can break or loosen in high-risk patients or can break osteoporotic bones more easily than other systems, facilitating wound dehiscence. 1
This series of cases presents the first worldwide use of a rigid fixation system made of biocompatible carbon fiber. This system is intended to provide similar safety and performance outcomes to other rigid fixation systems, with an easier application and a midpoint cost increase with respect to wires.
Case Series
This case series includes 30 consecutive patients who were undergoing elective cardiothoracic surgery at a tertiary hospital between March and July 2022. All patients granted written consent before undergoing surgery.
Patients in the series had to be older than 18 years and undergoing elective cardiothoracic surgery requiring median sternotomy. The mean age of the patients was 69.1 ± 10.2 years, 63.3% were men, and 86.7% had at least 1 risk factor associated with poor recovery after sternotomy (obesity, diabetes, osteoporosis, chronic obstructive pulmonary disease [COPD], kidney failure, use of steroids, cardiopulmonary bypass exceeding 2 h, or bilateral internal mammary artery interventions).
All patients in this series underwent sternotomy closure using the carbon-fiber rigid fixation system (STERN FIX Sternal Stabilization System; NEOS Surgery S.L., Barcelona, Spain) following the manufacturer’s instructions for use (Supplemental Video 1). This system consists of 2 components: male and a female parts that telescopically match each other by a ratchet mechanism that allows their movement in the closing direction and, at the same time, impedes their backward movement. Both components have a curved arm that embraces the sternum laterally and does not perforate the intercostal fascia; therefore, there is no possibility of bleeding into the retrosternal space (Fig. 1). The implant is made of biocompatible carbon-fiber reinforced polyether-ether-ketone (CFR-PEEK) and is safe for magnetic resonance imaging. There are 5 sizes of this device available to accommodate different sternal bone thicknesses between 9.5 and 17 mm. In case of emergency or elective redo sternotomy, the device can be easily cut laterally using a standard wire cutter.
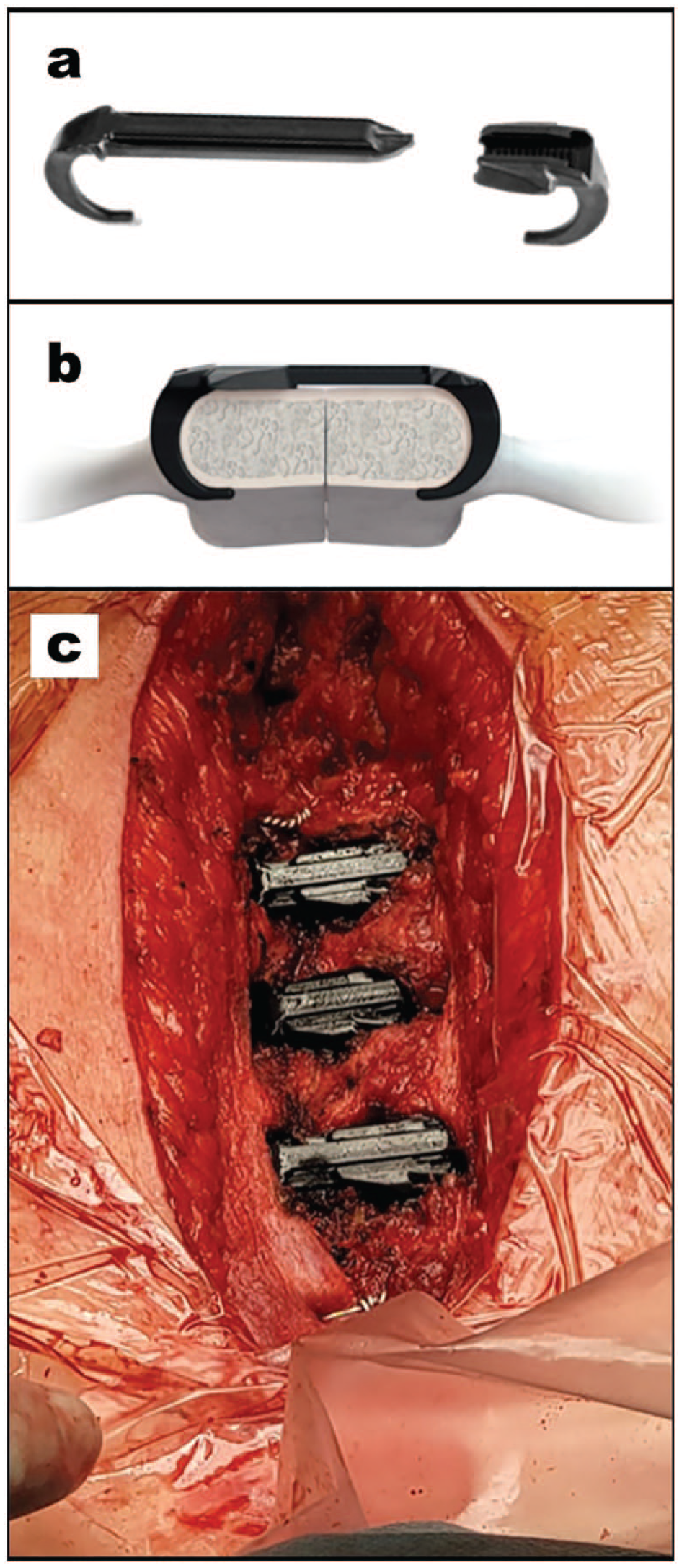
(a) Parts of the carbon-fiber rigid fixation device. (b) Depiction of the devices placed on the sternum. (c) Intraoperative picture of the implanted devices.
All surgical interventions were performed by the same surgeon. In most cases, the investigational devices were implanted in intercostal spaces 2, 3, and 4, except in 2 cases, in which only 2 devices were implanted in the second and third spaces. In all cases, complementary stabilization of the sternum was performed using stainless steel wires to provide a minimum of 5 fixation points. The sternal closure was achieved in a mean of 15.9 ± 3.8 min (from the beginning of measurement of the intercostal spaces to the closure of the last intercostal space). The surgeon considered the use of the device to be easy or very easy in most cases (79.3%). According to the surgeon’s subjective assessment, the bleeding caused by the investigational device was less than the closure with wires in 48.3% of cases and similar in 44.8%. The surgeon was satisfied or very satisfied with the sternotomy closure result in most cases (96.6%).
Twenty-nine patients were discharged uneventfully, and 1 patient had excessive bleeding during the first 24 h postoperatively that required re-exploration; the bleeding was not related to the devices implanted. The device was removed following the manufacturer’s instructions by cutting it with a wire cutter. Device removal was reported as easy, and this patient was then closed with wires. Three patients died before the 6-month visit, and 2 were lost to follow-up. Twenty-four implanted patients completed the 6 months of follow-up.
Sternal stability was clinically assessed using the Sternal Instability Scale (SIS). 2 The assessment was performed by a trained nurse by palpating along the sternum to notice any separation or motion. A score of 0 meant no motion, 1 meant minimal motion (such as clicking), 2 meant moderate increase in motion, and 3 meant marked increase in motion. Sternal instability was reported in the case of a score of 2 or higher. All patients had an SIS score of 0 at discharge. One patient of 28 (3.6%) had an SIS score of 1 and the rest had a score of 0 at 1 month of follow-up. All patients had SIS scores of 0 at 6 months of follow-up.
After 6 months of follow-up, there were no serious adverse events (SAE) related to the device and no cases of dehiscence nor deep wound infections in any of the 30 patients implanted. There was 1 case of superficial wound infection (3.3%) that was unrelated to the study product. The patient suffered from obesity, diabetes, and COPD. The case was resolved without sequelae with 1 week of antibiotic treatment.
Chest pain levels, upper limb functionality, and quality of life of the patients worsened significantly after surgery and returned to presurgical levels at 6-month follow-up (Supplemental Fig. 1).
Upon chest inspection at 1 month after surgery, the patients had no bulging in the sternotomy area caused by the wires or the investigational device.
Twenty-five patients had a computed tomography (CT) scan performed 6 months after the surgery. The CT scan images showed no artifact caused by the investigational device. The sternal healing measured with Stacy’s scale (Supplemental Fig. 2) 3 had a mean score of 3.5 ± 1.0 (Fig. 2, Supplemental Video 2). There were no cases of device migration.
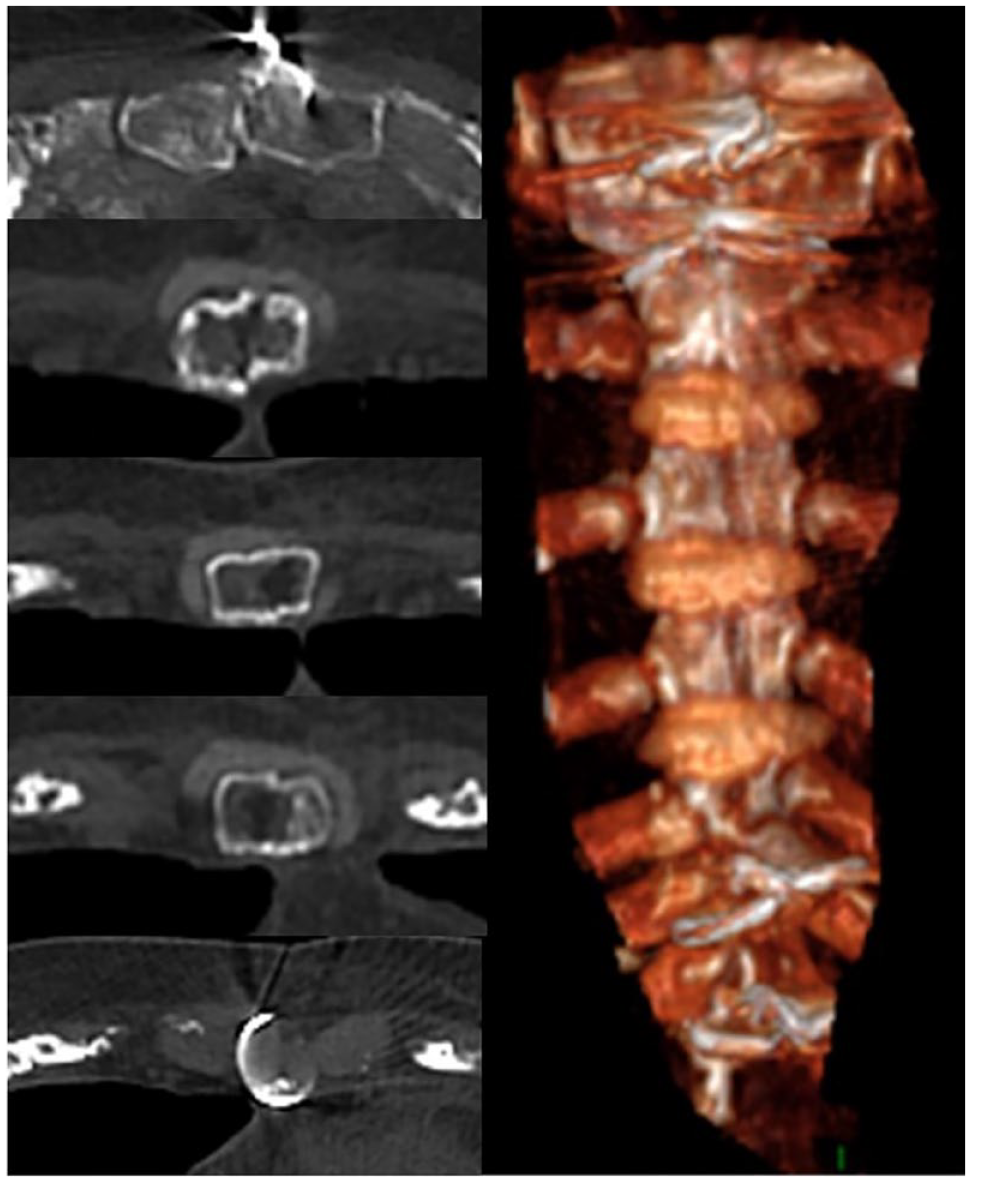
Computed tomography scan slices used to assess sternal healing (left) and 3-dimensional reconstruction of the sternum (right).
Discussion
This is the first-in-human use of this novel carbon-fiber rigid fixation system. All patients included in this study underwent cardiothoracic surgery with access via median sternotomy. The study’s primary endpoint was to assess whether the device could stably close a sternotomy. This primary endpoint was achieved 1 month after surgery with only 1 patient (3.6%) with a score of 1. Previous studies assessing sternal instability after sternotomy using SIS found that up to 70.8% of patients had an SIS score of 1, 1 month after closure with wires. 4
The sternal healing 6 months after surgery was also assessed by means of the analysis of the CT scan. The mean sternal healing score obtained was 3.5 ± 1.0, which is slightly better than the scores found in the literature for wires (3.3 ± 1.1). 5 Previous studies found that sternotomies usually have delayed bone healing, as they showed that a sternotomy may not demonstrate complete healing in CT evaluations up to 2 years after the procedure, despite clinical evidence of union. 6
Shortly after the surgery, the observed pain was within the usual levels for these kinds of patients, 7 in most cases with mild levels of pain at rest and when walking and moderate levels of pain when forcing a cough.
The safety assessment of this device was one of the main secondary outcomes of this first-in-human study. During the trial, there were no perioperative complications caused by the investigational device or study procedures, and during the 6 months of follow-up there were no AE or SAE related to the device or device deficiencies. As for sternotomy complications, there were no cases of dehiscence or deep wound infections, and there was a single case of superficial wound infection that was not serious and not related to the device; this patient had diabetes, which is a known risk factor for slow wound healing and infection. The incidence of sternotomy complications was equal or even lower than incidences reported in the literature, 8 thus confirming that the investigational device is a safe method to close median sternotomies, including high-risk patients.
In summary, the results of this clinical investigation demonstrate that the use of a CFR-PEEK rigid fixation system stabilizes safely and effectively the closure of median sternotomies. Achieving sternal stability with a system that does not perforate the intercostal fascia and therefore minimizes mediastinal bleeding may reduce the incidence of postoperative complications. A randomized controlled trial that compares the safety and performance of this device against the current standard of care (wire cerclage) will increase the evidence obtained in this series of cases.
Supplemental Material
sj-pdf-1-inv-10.1177_15569845241252393 – Supplemental material for Novel Carbon-Fiber Rigid Fixation for Sternal Closure
Supplemental material, sj-pdf-1-inv-10.1177_15569845241252393 for Novel Carbon-Fiber Rigid Fixation for Sternal Closure by Alessandro Affronti, Blanca Domenech-Ximenos, Núria Pichel, Alba Ricarte, Laia Hernández, Brayan Rubio, Belén Cevallos, Marcelo Sanchez and Manuel Castellà in Innovations
Supplemental Material
sj-pdf-2-inv-10.1177_15569845241252393 – Supplemental material for Novel Carbon-Fiber Rigid Fixation for Sternal Closure
Supplemental material, sj-pdf-2-inv-10.1177_15569845241252393 for Novel Carbon-Fiber Rigid Fixation for Sternal Closure by Alessandro Affronti, Blanca Domenech-Ximenos, Núria Pichel, Alba Ricarte, Laia Hernández, Brayan Rubio, Belén Cevallos, Marcelo Sanchez and Manuel Castellà in Innovations
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Study funded by NEOS Surgery S.L.
Ethics Statement
Clinical Trial Registry Number NCT04593732 (clinicaltrials.gov). Official title of “Clinical Investigation to Evaluate the STERN FIX Device as a Sternal Fixation System in Medium Sternotomy.” The study was reviewed and approved by the Clinical Research Ethics Committee of Hospital Clínic de Barcelona on July 15, 2020, under the code HCB/2020/0773. All patients included in this study signed an informed consent form prior to any study-specific procedure. Patients agreed that the data obtained in this study could be used in scientific publications and that no identifiable data would be shared. This study complies with the Regulation (EU) 2016/679 of the European Parliament and of the Council of April 27, 2016, on the protection of natural persons with regard to the processing of personal data and on the free movement of such data.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.