
Abstract

Introduction
Coronary artery bypass grafting (CABG) is one of the most performed operations worldwide. However, CABG is often as invasive today as it was 50 years ago. Less invasive CABG, or minimally invasive CABG (MICS CABG), can take many forms. Regardless of which iteration is undertaken, less invasive CABG represents one of the most technically challenging operations that a cardiac surgeon can perform today. Indeed, through a small incision, reconstructive microsurgery must be performed flawlessly, with different exposures for the harvesting of each conduit, the sourcing of inflows, and the grafting of every myocardial territory. If MICS CABG were to fail, consequences can be ominous—since alternatives such as percutaneous intervention and conventional CABG have long demonstrated their reliability, despite their shortcomings. It is germane for our patients and for the field that centers of excellence in coronary artery surgery dedicate resources and expertise to developing safe, high-quality, reproducible, and durable forms of less invasive CABG. This article, in the format of “10 Commandments of Less Invasive CABG,” proposes a stepwise path for the safe uptake of MICS CABG, toward increasing its adoption in one or several of its forms.
1. Become a Master at OPCAB First
Nonsternotomy CABG, whether single vessel or multivessel, is a technically difficult operation.1,2 There are several steps that require intricate exposure and which only prior mastery of sternotomy off-pump coronary artery bypass (OPCAB) can help overcome. For instance, the exposure of a deep intramyocardial left anterior descending artery (LAD), or precise coronary suturing on the beating heart at a distance through a limited field of view, are techniques that OPCAB best prepares for. It is recommended that teams wanting to engage in nonsternotomy CABG first be experts at OPCAB, not only in selected patients but also in all-comers with left ventricular dysfunction, obesity, acute coronary syndrome, and diffuse coronary artery disease. Only this way can cardiac anesthesia, nursing, and perfusion progressively align toward developing together a “routine OPCAB culture” that will be invaluable to the subsequent successful uptake of less invasive CABG. 3
2. Engage Your Team
Less invasive CABG is a team effort. First, the hospital administration should understand that this novel operation will at first represent a niche modality, which can readily grow into a large program, given that more than 50% of adult cardiac surgeries performed around the world are CABG. It is recommended at first that a single cohesive team be put together to develop MICS CABG. In this regard, involvement from cardiac anesthesiologists, nurses, intensivists, and advanced practice practitioners is key. The cardiac anesthesiologist provides a unique set of skills to keep the patient’s ventilation, perfusion, and cardiac volume balanced and optimized (Table 1), on which the surgeon has comparatively little intraoperative recourse, especially through a small thoracotomy incision. Nursing engagement is critical to ensure smooth procedural delivery and seamless processes around the operation. The cardiac intensive care team is important for rapid transfer to the ward and thoughtful progression toward early discharge. Advanced practice providers such as specialized nurse practitioners have a central role in ensuring patient evaluation and optimization prior to MICS CABG as well as their ultra-rapid discharge, safe outcome, and thorough follow-up after surgery.4,5
Key MICS CABG–Enabling Features From the Cardiac Anesthesiologist.
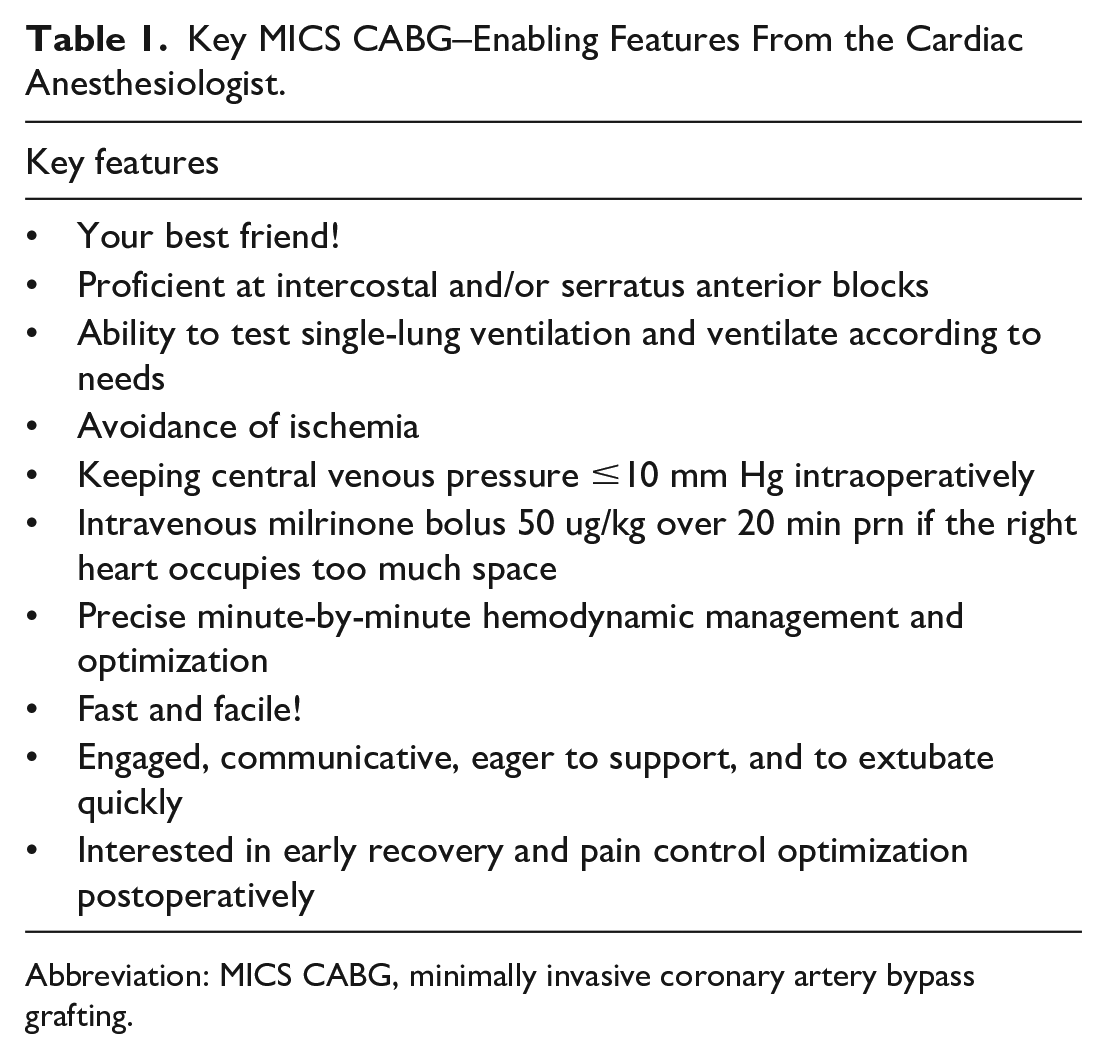
Abbreviation: MICS CABG, minimally invasive coronary artery bypass grafting.
3. Get Training in Less Invasive CABG
It is relatively easy to get training for MICS CABG. Peer-to-peer opportunities are available on each major continent. Companies that produce surgical MICS CABG instruments are generally favorable to help train and support sites that will hopefully turn into successful programs. 6 According to the author of this article, the key prerequisite for a peer-to-peer MICS CABG training request is that commandments 1 and 2 above are met. Per commandment 2, it is germane that the whole team be engaged and supportive, from the hospital administrators to the cardiac anesthesia team, aiming to support MICS CABG patients, their surgeon, and their growing program.
4. Select the Right Patients Particularly at Beginning of Experience
Table 2 summarizes key factors in choosing easier patients for MICS CABG, particularly early on as teams embark on their program. When experience has been gained, higher-risk patients can be offered MICS CABG. Nevertheless, a surgeon should resist the temptation to offer MICS CABG because a patient might not survive sternotomy CABG; to the contrary, the goal of a less invasive CABG operation is faster recovery in patients who can benefit from it, rather than enhancement of operative survivability. Unique situations (i.e., amputations, permanent tracheostomy, porcelain aorta, etc.) warrant case-by-case consideration.7,8
Criteria for Nonsternotomy MICS CABG.
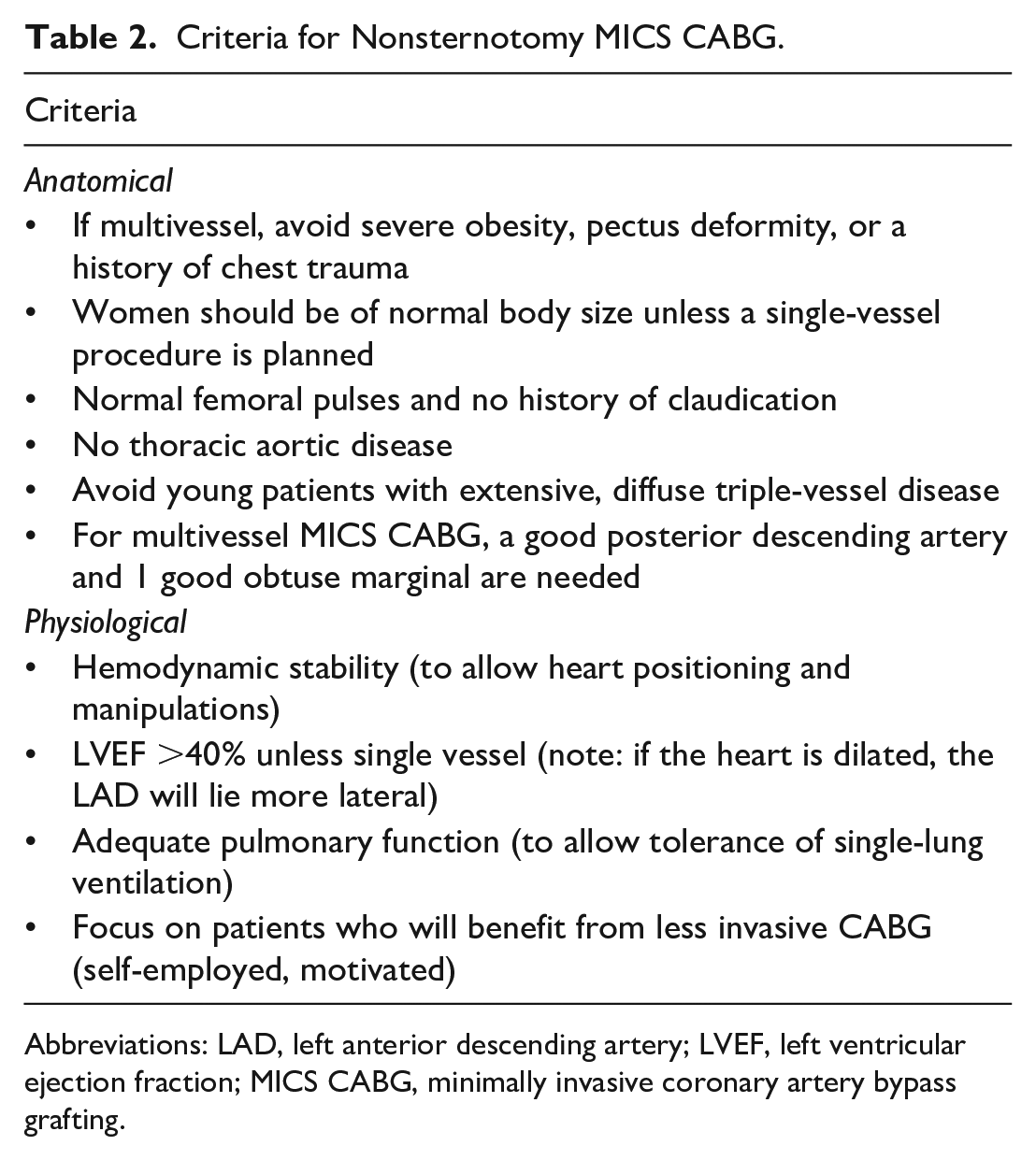
Abbreviations: LAD, left anterior descending artery; LVEF, left ventricular ejection fraction; MICS CABG, minimally invasive coronary artery bypass grafting.
5. Pay Close Attention to Positioning the Patient and Incising the Right Way
It is germane that the surgeon personally positions the patient for MICS CABG. Generally, a right decubitus of about 15° to 25° is preferred. The left arm can rest on the side (necessary for robotic approaches) or be gently brought over the head and supported (Fig. 1). The latter position slightly opens the rib cage; however, care should be taken to consider possible bone anomalies that, for instance, might stenose a neural foramen. 9
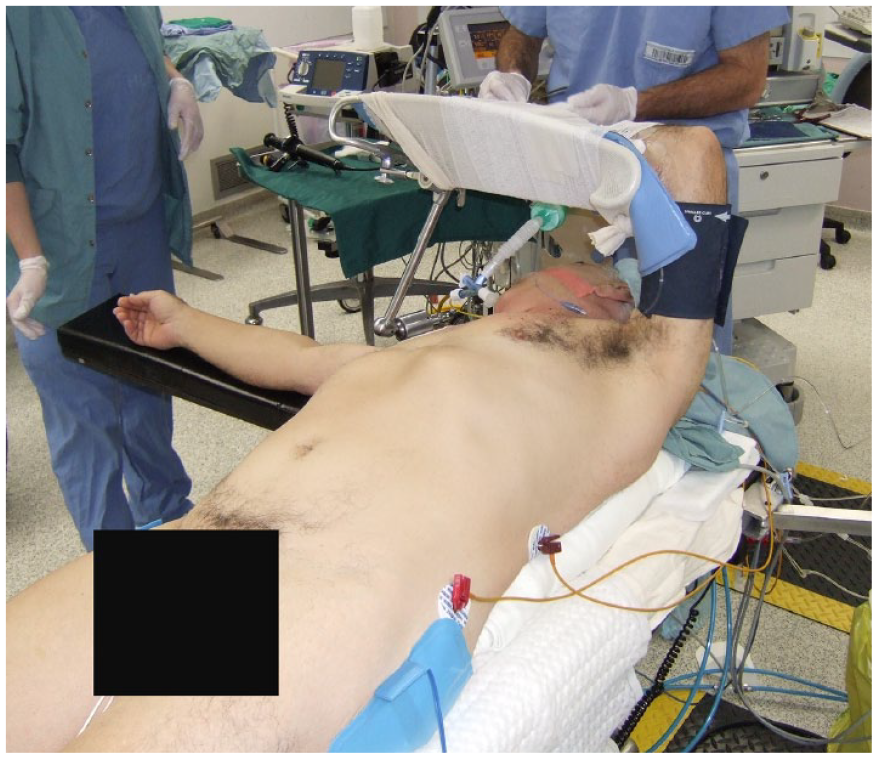
Positioning for MICS CABG. A right decubitus of about 15° to 25° is preferred. The left arm can rest on the patient’s side (necessary for robotic approaches) or be gently brought over the head and supported, as depicted. MICS CABG, minimally invasive coronary artery bypass grafting.
Regarding the incision, the fifth intercostal space is usually best for multivessel nonsternotomy CABG, but the fourth space may be preferred if only a left internal thoracic artery (LITA) to LAD or grafts to anterior vessels are considered, particularly if the grafting of those anterior vessels takes place proximally or midsegment. In the vast majority of multivessel MICS CABG, the correct incision site can be selected by imagining a triangle between the sternal angle and the xiphoid process and choosing the corresponding site in the left midaxillary line (Fig. 2). Once that intercostal space is entered, for multivessel MICS CABG it should correspond to 1 space cephalad to where the apex of the heart can be palpated. This site usually provides the best exposure to all conduits and multiterritory coronary vessels including the ascending aorta (if needed), the LAD, the lateral wall, and the diaphragmatic surface of the heart (to graft the inferior wall). If it is felt that moving up or down 1 space would make the operation easier, the surgeon should not hesitate to do so, as this can easily be accomplished within the same limited skin and pectoralis muscle incision which, in our experience, does not adversely affect the patient’s recovery.
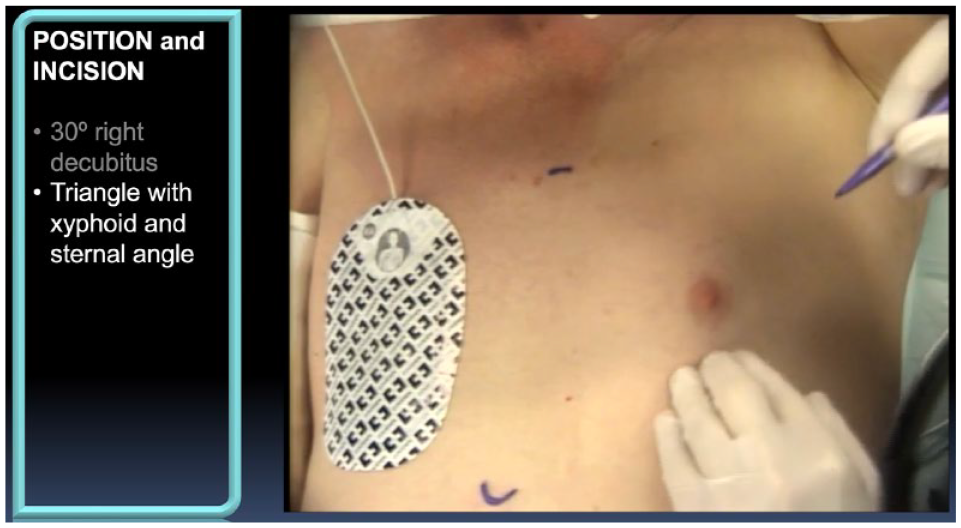
Performing the MICS CABG Incision. The incision site is chosen by imagining a triangle between the sternal angle and the xiphoid process and choosing the corresponding site at the left midaxillary line. MICS CABG, minimally invasive coronary artery bypass grafting.
6. Harvest High-Quality, Preferably Multiarterial Conduits
Minimally invasive coronary surgery should maximize the use of arterial grafts. The key premise of MICS CABG is to provide the benefits of internal thoracic or radial artery grafts without the detrimental aspects of sternotomy, broad surgical invasion, and, in some cases, cardiopulmonary bypass (CPB). Radial artery harvest, particularly if performed endoscopically, makes sense (Fig. 3) and is typically performed prior to positioning for MICS CABG. The LITA can easily be taken down either by a conventional small left thoracotomy or by a robotic approach. With regard to the right ITA (RITA), it can be harvested through the small left thoracotomy as well, but if a robot is not available, one has to select a patient with a relatively low or normal body mass index. Robotic RITA harvest works well in overweight patients, but it is not easy and carries a significant learning curve, especially with regard to harvesting the entire conduit all the way from the subclavian vein proximally to the bifurcation distally (Fig. 4). Nevertheless, once mastered, robotic bilateral ITA harvest represents a powerful tool that allows for both ITAs to reach the left heart circulation without sternotomy (even in overweight patients), without T or Y grafts, without proximal anastomoses, without CPB, and without any aortic manipulation.

Patient who underwent multiarterial MICS CABG ×3 at 1 month postoperatively. An endoscopic radial approach provided excellent cosmesis and enabled multiarterial grafting. MICS CABG, minimally invasive coronary artery bypass grafting.
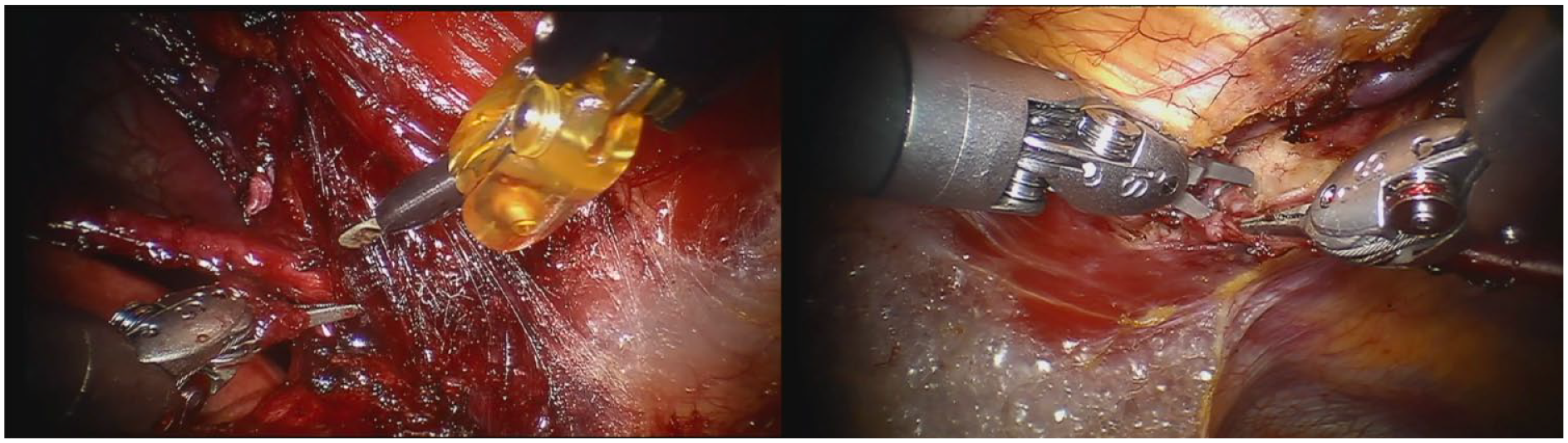
Robotic RITA harvest. The RITA is harvested cephalad past the ligated right medial internal thoracic vein (left panel) all the way down to the bifurcation (right panel). RITA, right internal thoracic artery.
7. Source Inflows in Several Possible Ways
While anaortic CABG carries appeal, extremely low levels of complications can also be achieved by meticulously sourcing conduits such as the radial artery and the saphenous vein from the ascending aorta. In our published experience of 566 patients, 1 stroke occurred, several days after extubation and with full recovery prior to hospital discharge. 10 Important safety criteria for inflow sourcing from the ascending aorta are to (1) exclude patients with proximal aortic disease and to not hesitate to use aortic scanning, (2) clamp the ascending aorta with a systolic blood pressure below 90 mm Hg, (3) clamp the aorta over a length of at least 3 cm, and (4) release to evacuate air and blood prior to tying the suture. With these key principles, cerebrovascular complications of proximal aortic sourcing can be kept to near nonexistent levels (Fig. 5). 11
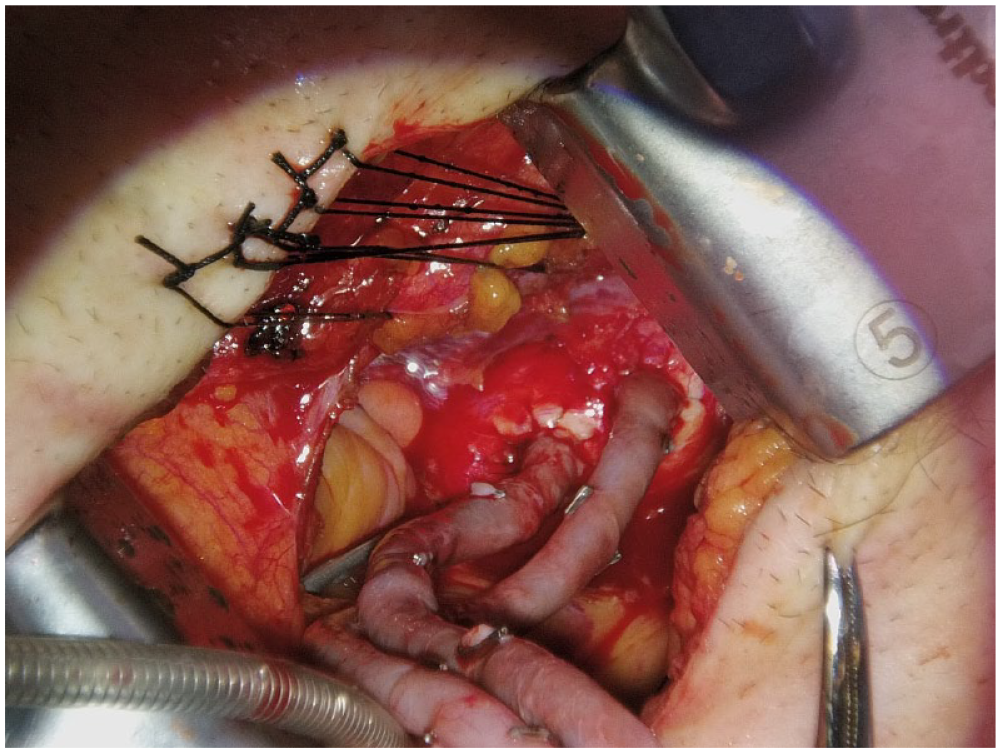
Sourcing proximal anastomoses from the ascending aorta. In elderly patients, the availability, excellent exposure, and simplicity of sourcing minimally invasively harvested saphenous vein directly from the ascending aorta represents an attractive option. By following key principles (see text), the risk of stroke can, in our experience, be decreased to virtually zero. Note how the pericardium is kept mostly closed to help mobilize the mediastinum inferiorly and leftward.
Alternatively, T, Y, or I grafts can also be performed. For instance, a limited length of the RITA can be used as an I-graft source to connect a radial artery, via a separate small right thoracotomy, prior to bringing it back in and advancing the I-graft into the left chest.
8. Skillfully Position and Expose Each Distal Without Hesitating to Use CPB Support
Distal anastomoses during MICS CABG can be difficult to perform. Our preference is to usually finish the grafting sequence with the LITA-LAD, as it can get in the way if performed first, therefore risking injury. Typically, the inferior wall is grafted first. An armless cardiac positioner is positioned approximately 3 cm distal and in the axis of the target vessel (Fig. 6). For the posterior descending artery, the cardiac positioner is pulled toward the patient’s left shoulder. For circumflex branches, the cardiac positioner is pulled toward the right hip. Just prior and during distal target exposure, deflating the right lung for about 30 s helps create space for exposure. Once the target has been brought and secured into view, the right lung is restarted and an epicardial stabilizer is positioned to allow for a motionless distal field. If exposure remains difficult, femoro-femoral or axillary-femoral CPB can be safely performed, allowing for decompression of the heart, hemodynamic stability, and for both lungs to be turned off during the distal anastomoses, thereby providing additional space to work within the closed chest. 2
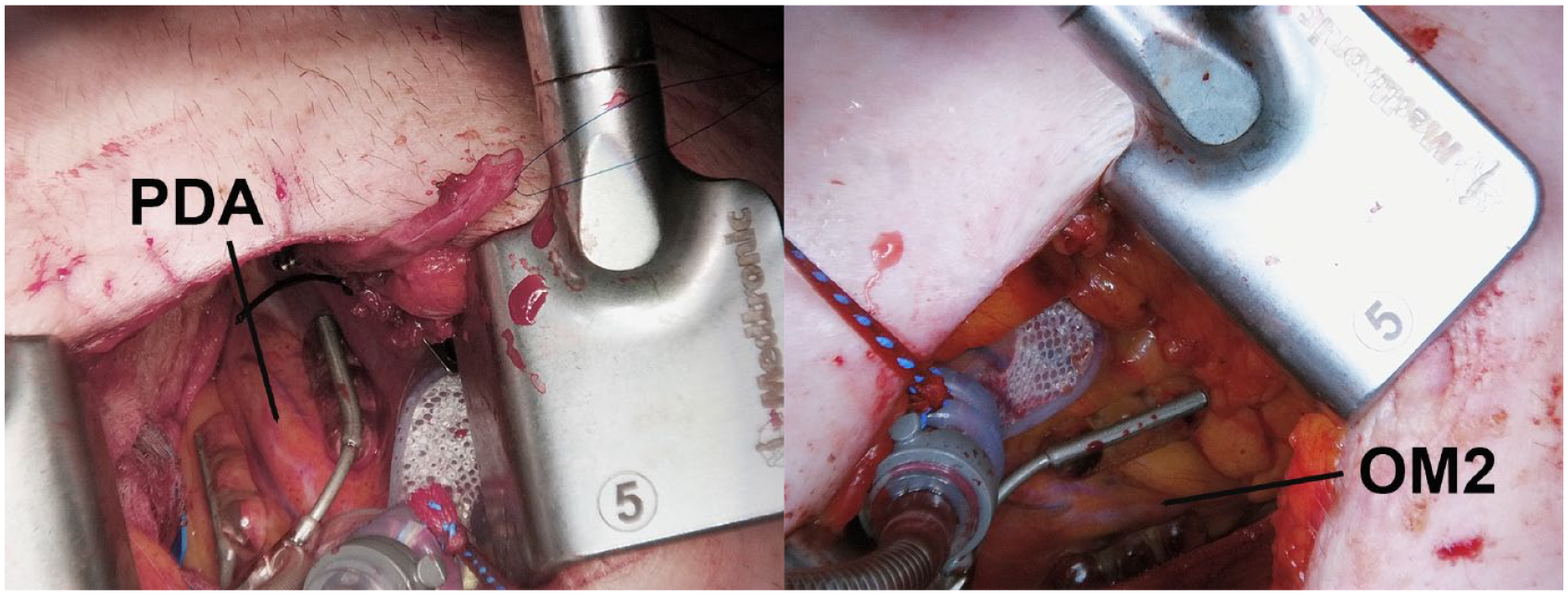
Armless cardiac positioner positioned approximately 3 cm distal and in the axis of the target vessel. For the PDA, the cardiac positioner is pulled toward the patient’s left shoulder (left panel). For the OM2 of the circumflex, the cardiac positioner is pulled toward the right hip (right panel). OM2, second marginal branch; PDA, posterior descending artery.
The left posterolateral pericardium should be incised open, behind the phrenic nerve and anterior to the left pulmonary veins, over a distance of at least 2 cm at any point during the procedure (usually while grafting the lateral wall). 12 To achieve this through a small thoracotomy, deflating the right lung for about 20 to 30 s is again tremendously helpful. Although still unproven in the MICS context, we have found that this extra step helps with early discharge by decreasing the likelihood of atrial fibrillation and pericardial effusion.
9. Have a Hybrid Backup
A hybrid backup strategy is an attractive approach for teams wishing to initiate multivessel MICS CABG. As their program takes off, selecting patients in whom non-LAD targets could also be addressed either with percutaneous coronary intervention or with medical therapy alone makes sense while also fostering a growing collaboration between the referring interventional cardiologists and the MICS CABG surgeon and team.
10. Objectively Check Every Graft
Given the technical implications of MICS CABG, it is imperative to check every graft with transit time flow measurements (TTFM). Although each precision stitch can usually be seen during MICS CABG, suturing occurs at a much greater distance than via a sternotomy, as the surgeon essentially works within a long, narrow tunnel. If not extremely meticulous, a higher risk of graft twisting, kinking, or even leaving behind small coronary artery flaps from incomplete or inadvertently torn bites may occur. Every graft should be checked with TTFM and redone if a discrepancy exists between the expected flow characteristics and the measured flows. For a comprehensive review of TTFM, please see reference. 13
Conclusions
CABG is the operation most commonly performed by adult cardiac surgeons. The 10 commandments outlined in this article represent a stepwise approach to the safe, efficacious, and successful uptake of less invasive CABG, aiming to provide teams with the availability of multiarterial grafting via a nonsternotomy approach. It is important that centers of excellence in coronary artery surgery dedicate resources and expertise to high-quality, safe, reproducible, and durable forms of lesser invasive CABG.
Footnotes
Declaration of Conflicting Interests
The author declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Ruel discloses support for the Minimally Invasive versus STernotomy (MIST) randomized controlled trial and as a MICS CABG proctor (both from Medtronic, Inc.).
Funding
The author received no financial support for the research, authorship, and/or publication of this article.