
Abstract

With the progress, proliferation, and guideline-supported indication of procedures to exclude the left atrial appendage (LAA), 1 the importance of defining what the LAA is both in terms of anatomy and clinical outcome has become all that much more important. With this, the transesophageal echocardiography (TEE) assessment of the LAA has become more regimented than simple exclusion of thrombus. However, this rigor remains lacking when it comes to epicardial surgical LAA ligation (S-LAAO). Indeed, this is not lost on guideline authors, with specific mention of the fact that “many studies do not report assessment of occlusion success” and “this inconsistency has likely contributed to the variability in outcome.” 1 The presence of this statement in society-endorsed guidelines should be a call to arms for the surgical community to demand a more regimented, rigorous assessment of the LAA after S-LAAO.
Arising from this variable approach to assessing S-LAAO success is confusion regarding the defined anatomic goal. This is perhaps due to the lack of randomized controlled trials looking at thromboembolism outcomes in patients on standard oral anticoagulation (OAC) without having had S-LAAO versus those having had ligation but not maintained on anticoagulation (i.e., OAC vs S-LAAO). If there were such a study, there would likely be wider recognition of S-LAAO among the cardiologist community, and that recognition would yield dissemination of what the ligation goal ought to be. In essence, what we need is a clinically derived, procedural (rather than overt anatomic) definition of the superior limits of the LAA to define the success of S-LAAO, which is a working, procedural definition of the LAA ostium, linked to outcomes. This data-derived definition does indeed exist, and we will use that here to work through the “10 Commandments” for systematic TEE assessment of S-LAAO.
1. Know Thy Appendage
The appendage is not form without function, raising the question of what is lost through LAAO? In terms of anatomy, the LAA derives from the primordial left atrium (LA). It is varied in size, number of lobes, geometry, degree of trabeculation, and relation to the LA. 2 The number of lobes is associated with thrombus risk, and most LAAs are bilobed. 3 The ostium of the LAA (which will be discussed below) leads into the neck, which then leads into the body. In a healthy heart, the LAA is an active structure: it is more distensible than the main body of the LA, actively contractile, and through these properties provides a means of augmenting preload, servicing as a decompression chamber during times of elevated left atrial pressures and a signaling pathway through its stretch receptors and release of atrial natriuretic peptide. 2 Unfortunately, with cardiovascular disease—most notably atrial fibrillation and congestive heart failure—many of these beneficial functions of the LAA are mitigated, and the LAA can become a vessel of stasis and thus a source of thromboembolism. 3
2. Define the Goals: What Is Success?
In line with this increased thromboembolic risk, on a background of OAC, the LAAOS III trial demonstrated lower rates of thromboembolism in patients with atrial fibrillation who underwent S-LAAO during cardiac surgery. 4 This then raises the question of what defines a successful exclusion of the LAA? In the first LAAOS study, the definition of successful LAA exclusion was having no residual flow from the LAA and a residual LAA neck of less than 1.0 cm, as determined by TEE. 5 This further raises the question of 1.0 cm from what? In that same study, the authors define the starting point of measurement as the junction of the anterior atrial wall and the appendage, essentially the atrioventricular (AV) groove/sulcus, which we would define on TEE by the anatomic position of the left circumflex coronary artery (LCx).6–8 Taken in sum, a successful surgical exclusion, with outcome data to support, would be a residual stump of less than 1.0 cm (defined as the distance between the AV groove/LCx and the line of S-LAAO) without evidence of residual LAA–systemic communication. Based on the same primary data, this definition is now also accepted within the 2023 atrial fibrillation guidelines with a level of evidence A. 1
What is left undefined in this is how are we extending this measurement from the AV groove/LCx to the lateral aspect of the LAA? Anatomically we often use the tip of the lateral ridge (formed by the ligament of Marshall, commonly referred to as the “Coumadin ridge”) as the lateral aspect of the LAA ostium. However, varied anatomies make this problematic, as often the tip of the ridge sits superior and thus truly in the main body of the LA. A more reasonable measurement would be to extend the “line” from the level of the LCx to the free wall of the LAA, which will typically intersect the mid-lateral ridge in a roughly perpendicular fashion, not at its tip. Again, varied anatomies may lead this hypothetical line to not incorporate lobes and trabeculations that can add to thromboembolic risk. So, perhaps a reasonable “procedural” definition of the LAA ostium would be the line that demarcates the distance between the inferior margin of the LCx and lateral wall of the LA, typically intersecting the lateral ridge in perpendicular fashion and adjusted superiorly to exclude all lobes and trabeculations. Any distance between this line and the line of S-LAAO would be the residual stump, and, based on the LAAOS I and IIII studies,4,5 this stump should be <1.0 cm (Fig. 1). It would be incorrect to extend this measurement to the tip of the lateral ridge that extends into the main body of the LA and thus overestimates the size of the residual stump (Fig. 2, Fig. 3).
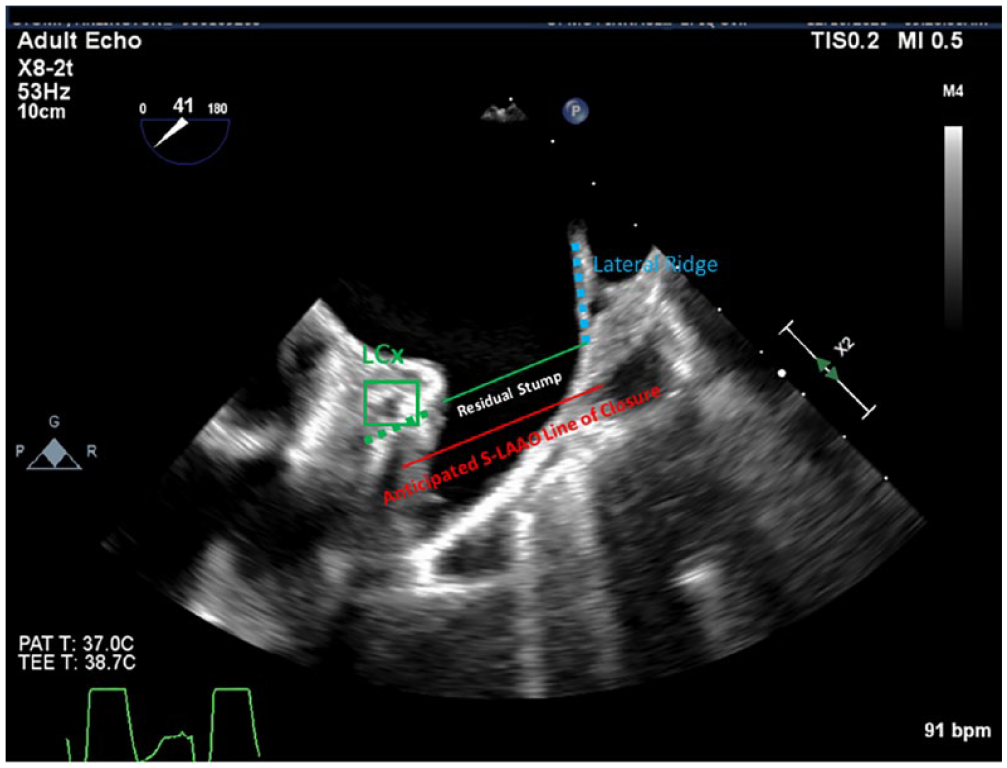
Anticipated line of closure and expected residual stump. The LAA ostium is defined here by the inferior margin of the LCx (green box and green dashed line), extended laterally to intersect the lateral ridge (blue dashed line). The resultant solid green line demonstrates the workable, procedural definition of the LAA ostium. The space inferior to this, up to the point of S-LAAO, would define the residual stump. LAA, left atrial appendage; LCx, left circumflex coronary artery; S-LAAO, surgical LAA occlusion.
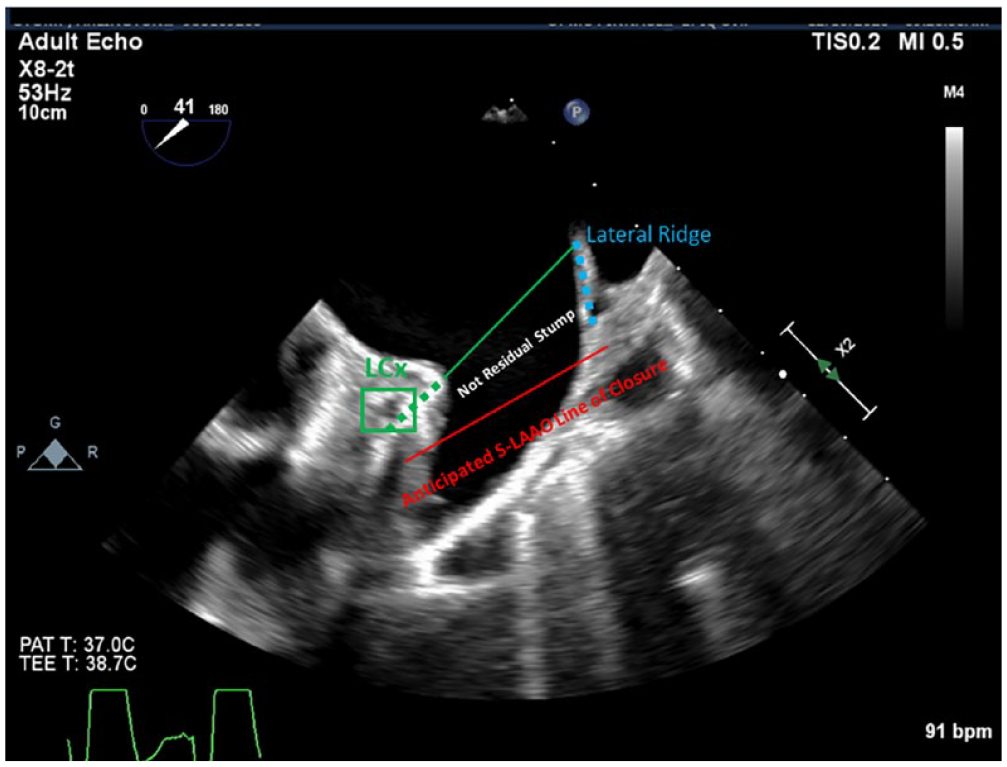
Anticipated line of closure with demonstration of overestimation of residual stump. Here, the ostial line (solid green line) is extended to the tip of the lateral ridge rather than in line with the atrioventricular groove. When measured in this fashion, the residual stump measures inappropriately larger as it carries into the main body of the left atrium. LCx, left circumflex coronary artery; S-LAAO, surgical left atrial appendage occlusion.
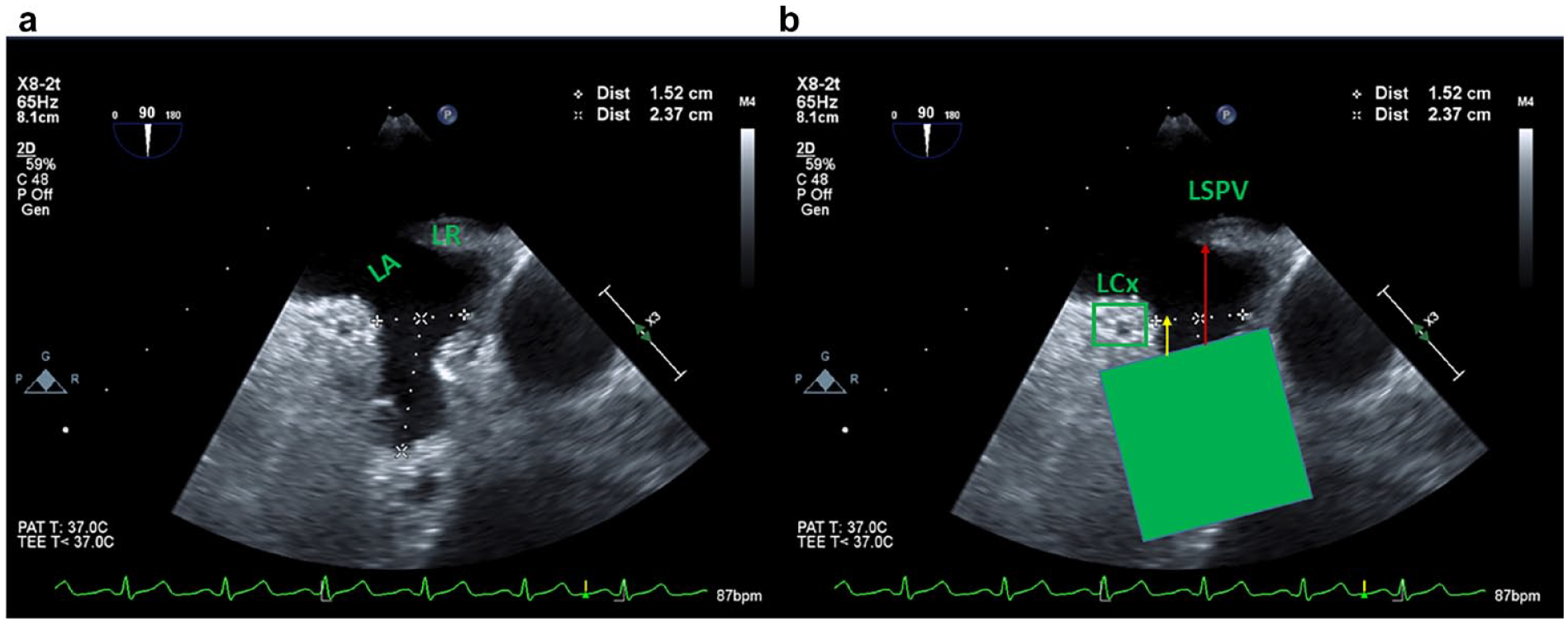
(a) Anatomic variation of the LR, showing it turning into the main body of the LA. (b) Green box shows anticipated surgical LAA occlusion closure line. The yellow arrow demonstrates the correct procedural definition of residual stump, in line with the AV groove that is defined by the inferior margin of the LCx. The red arrow demonstrates the measurement that would result from using the tip of the lateral ridge, inappropriately larger by incorporating the main body of the LA. LA, left atrium; LAA, left atrial appendage; LCx, left circumflex coronary artery; LR, lateral ridge; LSPV, left superior pulmonary vein.
3. Know the Procedure
As of this article, the most recent 2019 ACC/AHA/ASE training guidelines make specific mention of minimum procedural exposures for an interventional/structural heart imager, which inherently requires knowledge of the specific procedures. 9 In line with that, almost all structural heart procedures now require the imager(s) to attend device training AND for the structuralist/surgeon to know the imaging protocols. The logic behind this is very sound. Knowing the device, its manipulation, and how they translate on TEE, the potential complications and outcomes, and the verbiage all allow for more cohesive, outcomes driven communication, a greater collaborative effort, with better outcomes and shorter procedure times. S-LAAO should be thought of as in the family of structural heart procedures and follow the same training requirement.
4. Image in Multiple Angles
Imaging a 3-dimensional (3D) structure via a 2-dimensional (2D) modality (primarily) means that any single view is, by definition, only part of the picture. The LAA extends lateral and posterior from the main body of the LA, which can make imaging challenging. Further, with age and chamber enlargement, imaging angles and structure relationships may not be what we expect. We can compensate for this by ensuring that the LAA is imaged in multiple angles, 6 and those angles should include shallow views (0° to 60°), middle angles (70° to 90°), and steep angles (120° to 140°) that allow for visualization of any posterior lobes.
It is important to identify neighboring structures to serve as landmarks to define the ostium, with a focus on the LCx and the lateral ridge. These structures can be identified by sweeping from shallow to middle angle views—typically between 30° and 90°—often with anteroflexion to ensure the ostium is opened in view. 6
5. Optimize Your Image
With time constraints, we can sometimes gloss over the small maneuvers that allow for image optimization that actually will likely save time by removing ambiguity. Being a lateral and posterior directed structure, the LAA is often viewed at the edge of our screen on TEE imaging and thus the edge of our probe’s imaging sector. A simple countering of the probe to center the LAA in view is a high-yield, no-time maneuver to sharpen our image. Further, adjusting our sector widths, depth of imaging, focus level, and small adjustments of gain and compression settings can yield much better-defined imaging of the LAA. Finally, when simple rotations are insufficient to center our LAA in view, not forgetting to use both knobs to adjust the anteroposterior and right-left flexions of the probe can yield high dividends.
6. Use 3D Imaging
TEE 3D imaging is an important adjunct to 2D imaging,3,8,10 in both preclosure and postclosure assessment. The 3D imaging does provide for lower temporal and spatial resolution; however, there is overall better tissue characterization and the technology continues to rapidly improve. Further, 3D imaging is a more natural way for us to interpret a structure, provides for lower interoperator variability, provides for a single-view assessment, has been shown to be more precise in measurement, and, due to better tissue characterization, can help remove ambiguity that may present on 2D imaging.3,11
Imaging before S-LAAO can help anticipate the line of closure and potential for creation of a cul-de-sac that could be misinterpreted as a residual stump (Fig. 3). Postclosure TEE 3D imaging can better evaluate the entirety of the LA free wall, relation to neighboring structures, and prior location of the ostium. Due to a persistent cul-de-sac inferior to the lateral ridge, there may be concern for a significant stump on 2D imaging, and 3D imaging can hopefully better confirm exclusion and verification of successful LAA exclusion (Fig. 4).
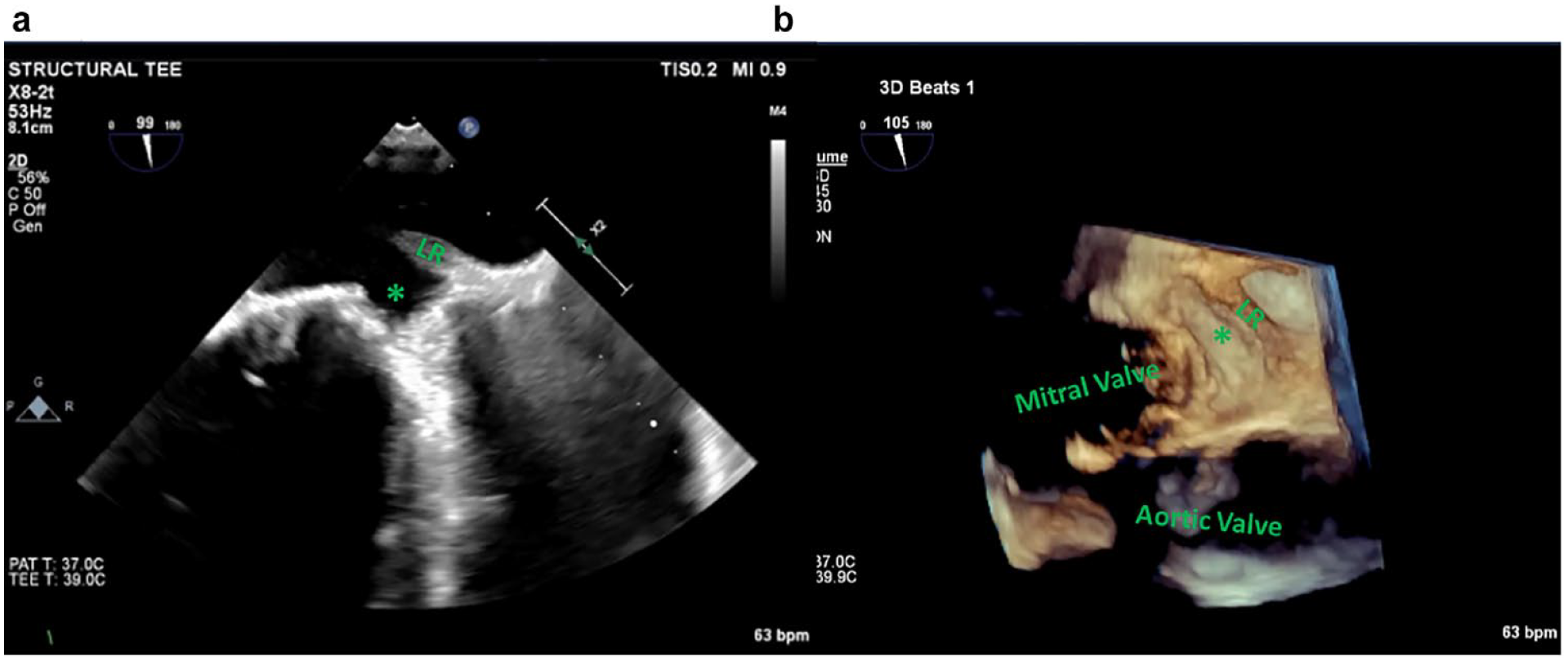
(a) The 2-dimensional image after S-LAAO. The LR is seen, and the space inferior (asterisk) could be interpreted by some as residual stump. (b) The 3-dimensional image of the same shows this inferior space to be a gully within the main body of the left atrium, created by the combination of S-LAAO and mitral valve repair. LR, lateral ridge; S-LAAO, surgical left atrial appendage occlusion.
Finally, although there can be anxiety about the time crunch in the operating room and wanting to provide an answer quickly, with the advances in technology, the time needed for 3D image acquisition is marginally different, if at all, than the multiple 2D images that a single 3D image can replace (Fig. 5).
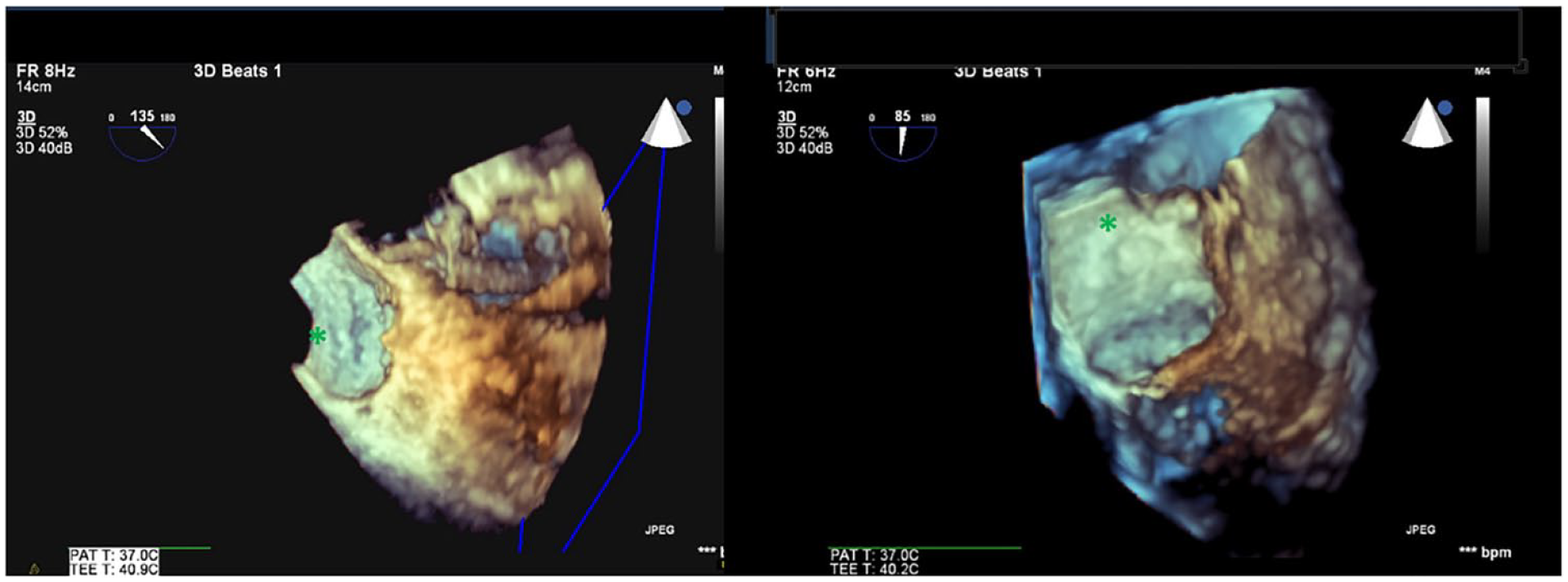
Examples of postdevice 3-dimensional image. The indentation of the epicardial clip device (asterisk) can be made out in both images. In a single view, it is clear there is no residual patency of the LAA. Color Doppler could be added to these images to demonstrate the lack of communication with the now excluded LAA. LAA, left atrial appendage.
7. Follow a Protocol
The 2023 atrial fibrillation guidelines make a Class IA recommendation for atrial fibrillation patients undergoing cardiac surgery to have an S-LAAO. 1 They also give a Class IA recommendation for TEE assessment to verify the success of S-LAAO. By following a standard protocol for image acquisition and assessment, we can fulfill the spirit of these guidelines by verifying LAA exclusion within the definitions already laid out. Protocolized imaging lessens general tendencies and bad habits, decreases interoperator variability, improves team communication, and sets procedural expectations. As it pertains to specifics of a protocol, we would propose:
a. Baseline imaging of the LAA in at least 3 views to include a shallow, middle, and steep angle view. Assess size, shape, lobes, and any thrombus burden.
b. Baseline imaging of neighboring structures that may be affected by S-LAAO. i. Mitral valve form and function, to include with and without color Doppler. ii. Left superior pulmonary vein flow patterns, including noncolor, color, and pulse wave Doppler. iii. A baseline 3D image acquisition, modified from a surgeon’s view of the mitral valve to have the LAA ostium in the foreground (Fig. 6). iv. LCx flow and associated wall motion. LCx flow can typically be best seen at a mid to steep angle view (70° to 100°), with the Nyquist scale turned down into the 30s cm/s, and a slight counterclock probe rotation and anteroflexion. Pulse wave Doppler can be attempted but is not always feasible due to translational motion (Fig. 7).
c. Repeat the above imaging after epicardial device application but before release and then 1 final time after device release. In addition to repeating the above images, assess for any residual communication with color Doppler assessment, at multiple angles from shallow to steep, with the Nyquist scale turned down into the 30s cm/s. Measure the narrowest neck (vena contracta) of this flow (Fig. 8).
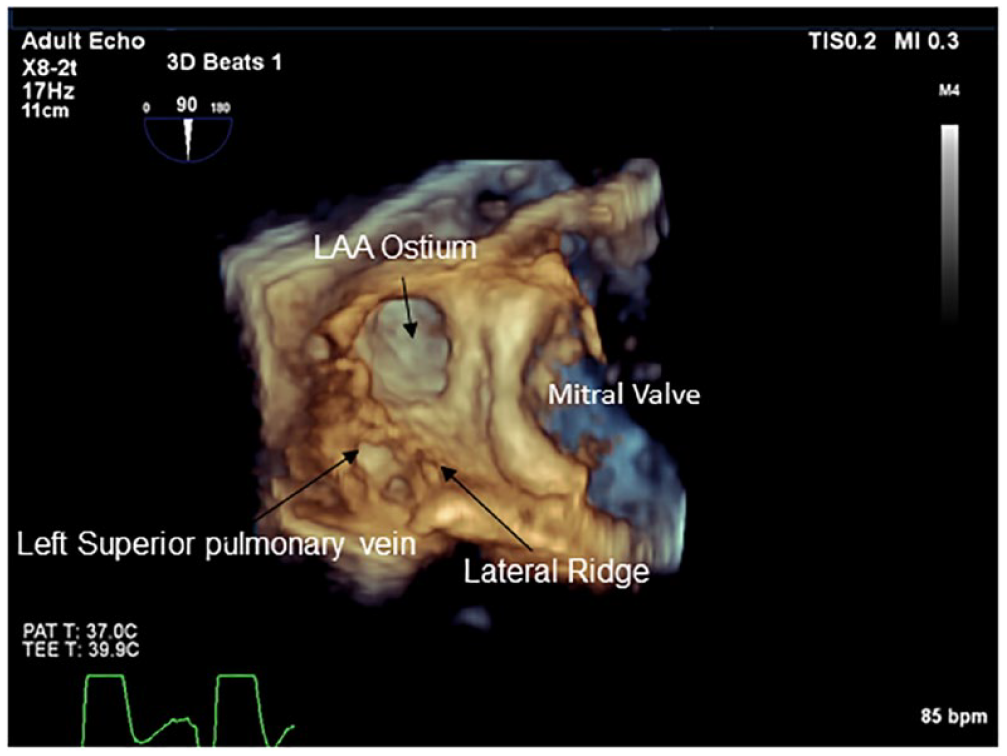
Modified surgeon’s view with the LAA ostium in the foreground. LAA, left atrial appendage.
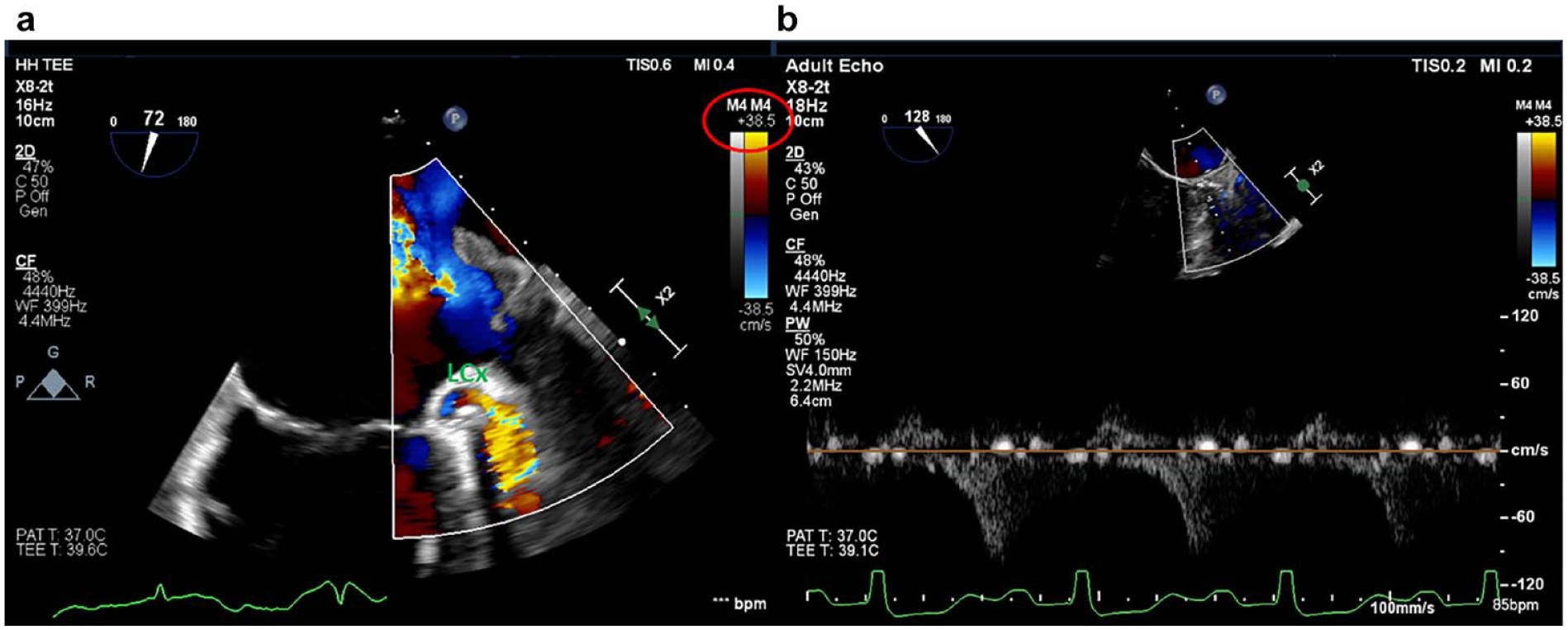
(a) Flow demonstrated in the LCx. Nyquist scale (red circle) is turned down into the 30s cm/s. (b) Pulse wave Doppler showing diastolic flow in the LCx. LCx, left circumflex coronary artery.
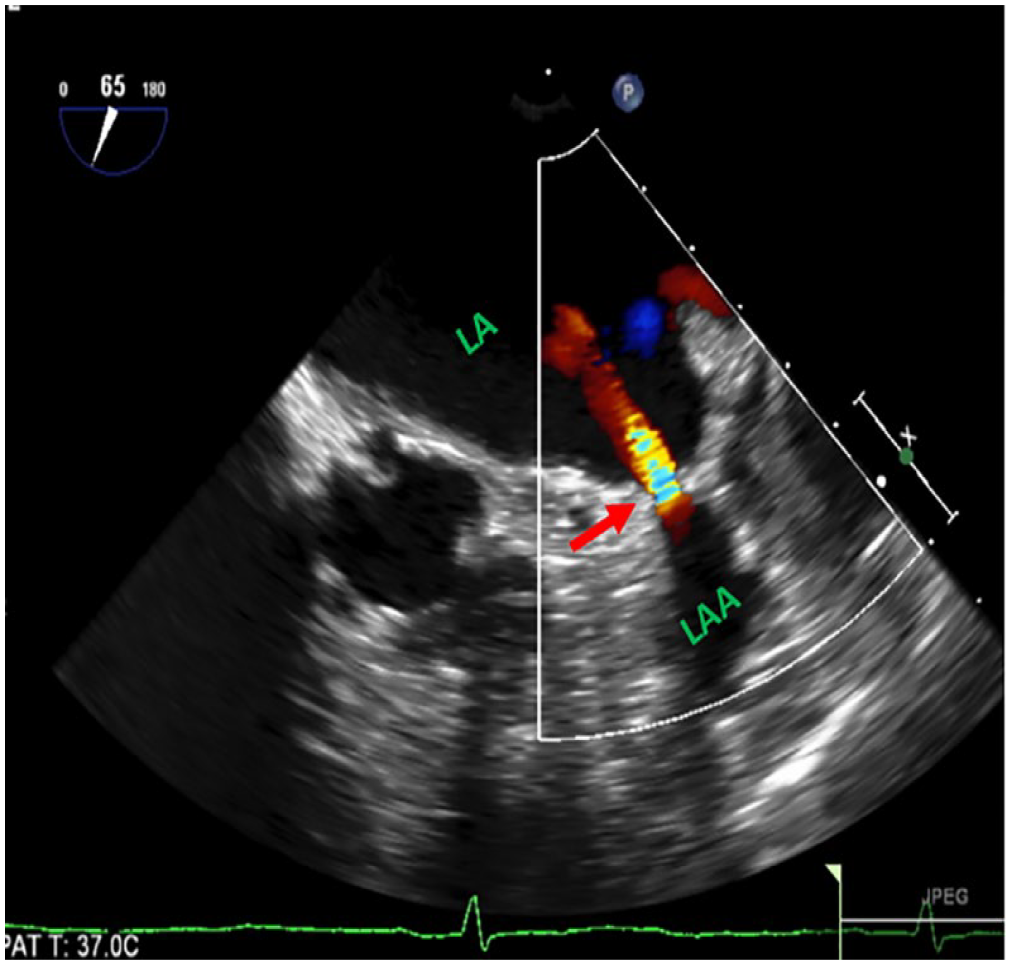
Demonstration of a patent LAA, with color Doppler showing residual communication (arrow) of the LAA with the LA. LA, left atrium; LAA, left atrial appendage.
8. Save Your Images
In the cadence of the operating room, it can often be that images are being obtained but not archived. A lack of archived images makes it all but impossible to objectively assess success after the fact. Although trite to state, the patient’s care is primarily not in the hands of the imager or surgeon but started prior to and continues after surgery with their cardiologist. Without images to review, the cardiologist is left literally in the dark, and these images carry great value when it comes to shared decision making with the patient. Finally, when there is a question raised as to a clinical event with S-LAAO, or later imaging reveals recurrent communication with the LAA, the imager and surgeon are left open to increased liability without the intraoperative images to support a successful LAAO.
9. Communicate
The heart team approach is now a well-established part of cardiovascular care. From a procedural perspective, the team approach should foster open communication at all points of a procedure. For the imager, that means understanding when to speak up, when to hold back, and when to ask for what is needed to optimize the image and thus verification of success (such as more volume for patients on cardiopulmonary bypass, breath hold, etc.). From a surgeon’s perspective, it means being comfortable with asking for a specific image and providing the time for image acquisition. As to the specific time points of the procedure:
a. Before incision: note for the surgeon any anticipated pitfalls (e.g., a large posterior lobe, issues regarding LCx flow or wall motion, mitral valve function or dysfunction, and left superior pulmonary vein flows).
b. After exclusion: be specific and call it out, such as “position looks good, all lobes are excluded, LCx flow and wall motion is intact, OK for device release.”
c. After release: verify and call out that findings remain stable.
10. Practice
Individual and institutional experience matters when it comes to outcomes.12,13 As such, practicing on an individual basis, as a team, and making sure the institution has enough volume to safely offer the procedure is of utmost importance. That is, whether there should be a minimum to target a 95% success rate and what that minimum is may need to be considered. Workflow considerations and the potential impact on productivity to achieve and maintain such targets necessitate institutional support.
Conclusions
On the background of OAC, S-LAAO exclusion of the LAA has shown benefit in reducing thromboembolism risk and is now a Class I, Level of Evidence A recommendation. These guidelines also lay out assessing the success of S-LAAO using intraoperative TEE with the goal of verifying no residual communication and a stump of <1 cm. Here we provide a procedural definition of the LAA ostium off of which this stump measurement is made, along with a protocolized approach to archived assessment before and after epicardial LAA occluder device application. Following a systematic approach to this assessment will ensure the greatest chance of success with minimization of ambiguity.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Consultant for AtriCure, Inc.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.