
Abstract
Objective:
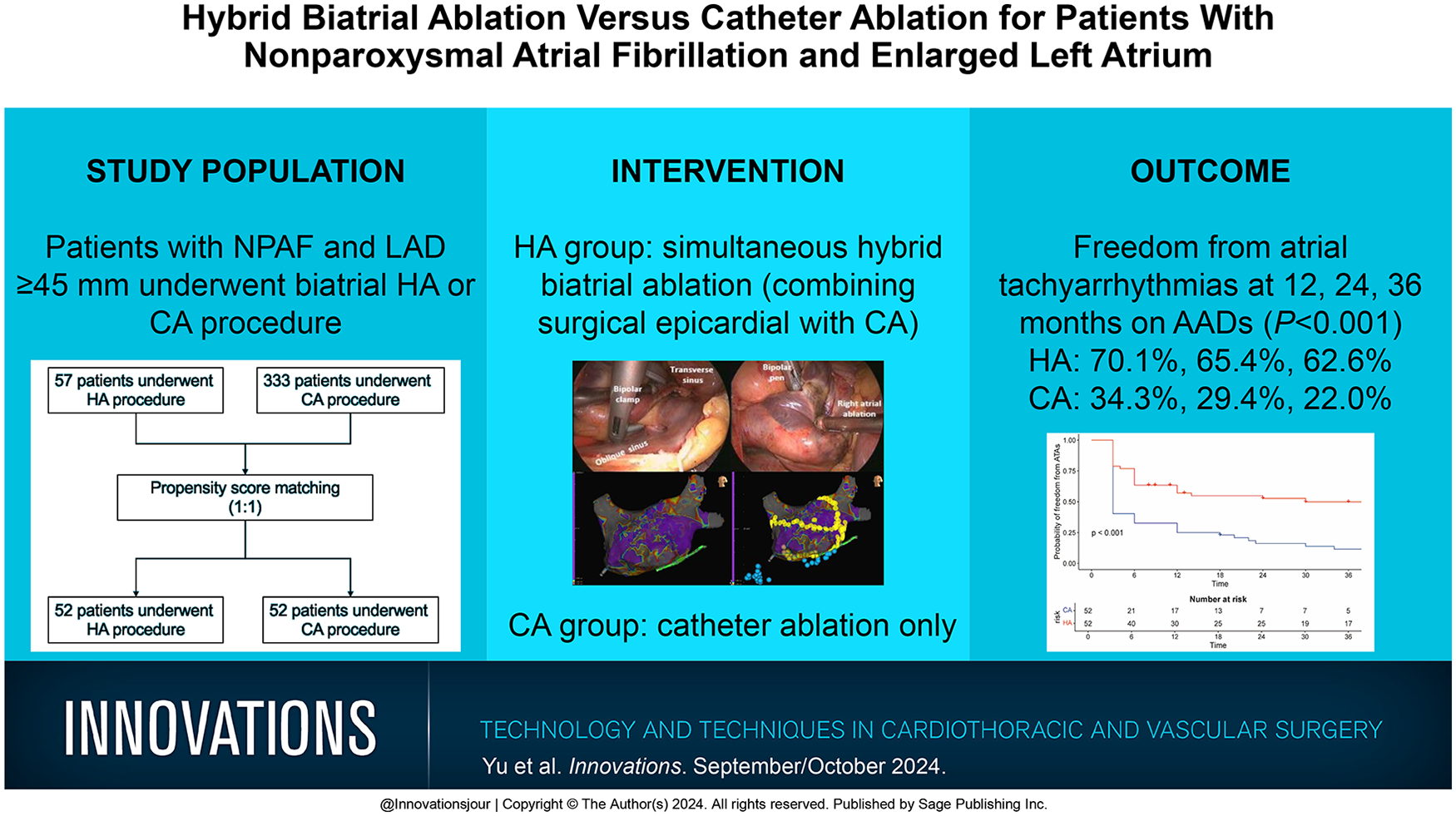
There is no consensus on the optimal ablation strategy for nonparoxysmal atrial fibrillation (NPAF) with enlarged left atrium. We aimed to explore whether hybrid ablation (HA) of combined thoracoscopic surgical ablation with catheter ablation (CA) was superior to CA alone in these patients.
Methods:
Patients with NPAF and left atrial diameter (LAD) ≥45 mm who underwent hybrid biatrial ablation or CA procedure from June 2014 to July 2021 were included in this study. Propensity score matching was applied to select patients in each group. The primary endpoint was freedom from atrial tachyarrhythmias after procedures.
Results:
After propensity score matching, 52 patients with enlarged left atrium (median LAD = 51 mm) were enrolled in each group. The median follow-up was 36 months. The probability of freedom from atrial tachyarrhythmias at 12, 24, and 36 months on antiarrhythmic drugs (AADs) was 70.1%, 65.4%, and 62.6% in the HA group and 34.3%, 29.4%, and 22.0% in the CA group, respectively (P < 0.001); off AADs was 57.1%, 52.7%, and 50.0% in the HA group and 25.0%, 16.2%, and 11.5% in the CA group (P < 0.001); on AADs after redo CA was 76.2%, 73.7%, and 73.7% in the HA group and 43.6%, 43.6%, and 38.2% in the CA group, respectively (P < 0.001); off AADs after redo CA was 62.5%, 60.1%, and 60.1% in the HA group and 30.4%, 25.1%, and 20.9% in the CA group, respectively (P < 0.001).
Conclusions:
For patients with NPAF and enlarged left atrium, hybrid biatrial ablation was superior to CA in sinus rhythm maintenance even if redo CA was performed.
Keywords
Central Message
For patients with nonparoxysmal atrial fibrillation and enlarged left atrium, hybrid ablation was superior to catheter ablation alone in terms of freedom from atrial tachyarrhythmias on or off antiarrhythmic drugs, even if redo catheter ablation was performed.
Introduction
The treatment of nonparoxysmal atrial fibrillation (NPAF) has puzzled interventional electrophysiologists in recent years. Several ablation strategies were undertaken to improve the efficacy of treatment for patients with NPAF, such as pulmonary vein isolation (PVI) plus linear ablation, PVI plus complex fractionated atrial electrogram ablation, rotor ablation, the stepwise approach, and repeated catheter ablation (CA), which did not achieve ideal results.1–3 The success rate of single CA is less than 40% within a year and 50% to 60% following multiple transcatheter reinterventions. 4
In clinical practice, we often encounter patients with NPAF and enlarged left atrium, the mechanism of which is considered more complex.5,6 Most of these patients are first seen by arrhythmia physicians, and a CA procedure is the first treatment they learn about. However, the efficacy of a single CA procedure might be more unsatisfactory, and multiple CA procedures are often needed for these patients. 4 Hybrid ablation (HA), which combines surgical epicardial with catheter endocardial ablation, seems to serve as a more promising procedure for NPAF. Previous studies with a small sample size to explore the efficacy of HA for patients with NPAF have shown promising results.7,8 However, it is unclear whether the newly proposed HA technique is superior to CA or repeated CA in the treatment of patients with NPAF and enlarged left atrium. Therefore, the aim of this study was to explore the optimal first-line ablation strategy for patients with NPAF and enlarged left atrium.
Methods
Patient Population
From June 2014 to July 2021, 72 patients underwent HA procedures, and 3,238 patients underwent CA procedures by our treatment team in Fuwai Hospital. In this cohort, 57 patients with NPAF and left atrial diameter (LAD) ≥45 mm without previous failed CA underwent HA procedures, and 333 patients with NPAF and LAD ≥45 mm without previous failed CA underwent CA procedures (Fig. 1). This study was approved by the Institutional Review Board of Fuwai Hospital (date of review, October 24, 2019; approval 2017-880).
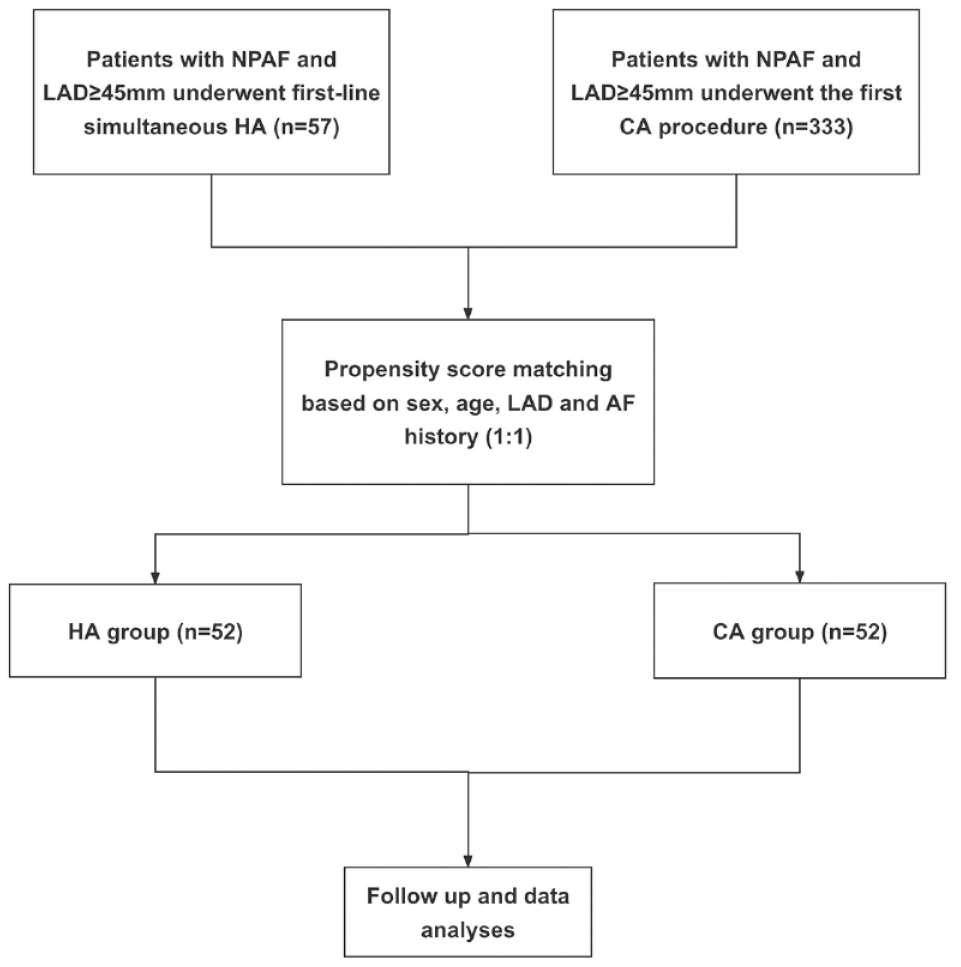
Study flow diagram depicting the participant enrollment. AF, atrial fibrillation; CA, catheter ablation; HA, hybrid ablation; LAD, left atrial diameter; NPAF, nonparoxysmal atrial fibrillation.
Hybrid Biatrial Ablation Procedure
The procedure included epicardial ablation followed by endocardial ablation on the beating heart in the hybrid operating room under general endotracheal anesthesia. The detailed procedure had been introduced in our previous study, as described briefly.9,10
Epicardial biatrial ablation
Access to the pericardial space was achieved through a bilateral transthoracic approach. Two working ports were positioned in the posterior-axillary fourth intercostal space and the midclavicular second intercostal space. A camera port was positioned in the anterior-axillary third intercostal space. The right-side ports were positioned more anteriorly. Generally, left-side ablation was performed first. The left atrial appendage (LAA) was excised by linear stapler (EZ 60; Ethicon Endosurgery, Cincinnati, OH, USA). The ligament of Marshall was divided by ultrasonic scalpel. The bipolar radiofrequency clamp (Isolator Synergy Access; AtriCure, Mason, OH, USA) was used to create left pulmonary vein (PV) isolation, left-sided roof and inferior lines, and left trigone line. The transpolar radiofrequency pen (Isolator Transpolar, AtriCure) was used to complement the left trigone line. We routinely applied bipolar clamps to make the left-sided roof and inferior lines by putting the upper jaw into the transverse sinus and the lower jaw into the oblique sinus simultaneously, and an additional bipolar pen was needed to complement the box lesion when the left atrium was enlarged (Supplemental Fig. 1). The linear lesion connecting the left superior PV to the LAA, and the linear lesion connecting the left inferior PV to the great cardiac vein was ablated with the transpolar radiofrequency pen. On the right side, the lesion set included right PV isolation, ganglion plex ablation at the Waterston groove fat pad, right-sided roof and floor lines, superior vena cava (SVC) to inferior vena cave (IVC) line, right atrial appendage line (the apex to the base at the level of the root of the aorta), and the line connecting the tip of the right atrial appendage to the SVC-IVC line. The bipolar clamp was usually applied to ablate at least 6 times per lesion, and lesions created by transpolar pens were ablated for 80 s at 1 place. See a video of epicardial biatrial ablation in our previous study. 9
Endocardial ablation
Endocardial electrophysiological mapping and CA were performed immediately after thoracoscopic epicardial ablation. Two multipolar catheters were inserted into the coronary sinus (IBI; Abbott, Chicago, IL, USA), and right ventricle (Daig, Abbott). After transseptal puncture, electroanatomic and voltage mapping with the EnSite NavX mapping system (Abbott) was completed. The surgical lesion was confirmed, and the residual conduction gaps were ablated or endocardial ablation in line with the surgical lesion was performed to improve transmurality. Then the ablation of coronary sinus, tricuspid isthmus, and mitral isthmus was delivered. Durable PV isolation and conduction block over each lesion were all confirmed. See a schematic drawing of HA lesion sets in our previous study. 9 If AF continued, direct-current cardioversion would be applied.
CA Procedure
The CA procedure has been described in detail by a previous study. 11 Lasso NAV SAS or Pentaray catheter was used to construct the 3-dimensional surface of the left atrium and PVs with guidance of the CARTO 3 or EnSite NavX system. Radiofrequency ablation was used in all patients with ThermoCool SmartTouch catheter (Biosense Webster, Diamond Bar, CA, USA) or TactiCath cathter (Abbott). PVI was completed in all patients at first. If AF persisted, in general, the following steps were applied: (1) further stepwise linear ablation in anterior wall, roof, mitral isthmus (including the linear lesions connecting left inferior PV and right inferior PV to posterior mitral valve annulus), and coronary sinus ablation, cavotricuspid isthmus would be conducted; (2) if AF continued, intravenous ibutilide (maximum of 1 mg) was administered, followed by elimination of atrial tachycardia under activation and voltage mapping if atrial tachycardia occurred; (3) if AF still continued, direct-current cardioversion would be applied. If sinus rhythm (SR) was restored after any of the steps above, the contact force monitoring (10 to 20 g) would be used to confirm the durable transmural lesions with intensive pacing (10 mA, pulse width 2 ms).
Redo CA
Redo CA was recommended if atrial tachyarrhythmia occurred after 3 months postoperatively in both the HA and CA groups. In the event of redo CA, the lesions made in the initial thoracoscopic surgical ablation or CA were checked for conduction gaps and re-ablated as needed. The ablation procedures targeted mainly re-isolation of PVs where conduction recovery was detected as well as substrate modification that included the anterior wall, roof, mitral isthmus, coronary sinus, cavotricuspid isthmus, and SVC orifice. If atrial flutter was demonstrated after the initial procedure, activation mapping and voltage mapping were performed to identify culprit gaps or linear lesion with conduction recovery and ablation was followed. If AF or atrial flutter persisted, intravenous ibutilide was administered or cardioversion was carried out to restore SR.
Postoperative Drug Treatment
In the HA group, class III antiarrhythmic drugs (AADs) with preference to sotalol would be routinely applied after ablation until 3 months. Anticoagulants were used as soon as bleeding risk was acceptable. It was advised to continue AADs if atrial tachyarrhythmia occurred after 3 months postoperatively, and continuation of oral anticoagulants or antiplatelet drugs relied on the risk of stroke according to the CHA2DS2-VASc score or LAA stump. In the CA group, AADs and oral anticoagulants were routinely applied after ablation until 3 months. Continuation of oral anticoagulants and AADs were advised if atrial tachyarrhythmia occurred.
Data Collection and Follow-Up Visits
The procedural parameters for HA and CA were obtained from the operation records. Patients were followed at 3, 6, and 12 months and annually thereafter and underwent 24-h Holter monitoring. Any arrhythmia symptoms or suspicious atrial tachyarrhythmia recurrence following ablation were deemed deserving 12-lead electrocardiogram. A questionnaire about permanent pacemaker implantation, ischemic stroke, death, and hospitalization for heart failure was completed via telephone.
Endpoint
The primary efficacy endpoint was defined as freedom from any atrial tachyarrhythmias in the absence of AADs, which was defined as no evidence of AF, atrial flutter, or other atrial tachyarrhythmias with a duration longer than 30 s as documented by 24-hour Holter monitoring. 12 The first 3 months after the ablation procedures was considered as a blanking period. Time to atrial tachyarrhythmias in the absence of AADs was defined as the time from the end of the blanking period to the first recurrence of atrial tachyarrhythmias without AADs, and time to atrial tachyarrhythmias with AADs was defined as the time from the end of the blanking period to the first recurrence of atrial tachyarrhythmias after the start of AADs. After the blanking period, patients in both groups who suffered from atrial tachyarrhythmia recurrence might undergo redo CA procedure, and the probability of freedom from atrial tachyarrhythmias after redo CA was also evaluated. Event-free survival of permanent pacemaker implantation, ischemic stroke, death, and hospitalization for heart failure were also reported.
Statistical Analysis
Clinical characteristics were described as frequency (percentage) for categorical variables and median (interquartile range [IQR]) for continuous variables. The Mann–Whitney U test was used in comparison of intergroup differences for continuous variables, while Fisher’s exact test was used for categorical variables. Propensity score matching (1:1) was used on the basis of gender, age, AF history, and LAD to reduce selection bias. The Kaplan–Meier analysis and log-rank test were used to evaluate the time from the first ablation to atrial tachyarrhythmia recurrence, time from redo CA procedure to atrial tachyarrhythmia recurrence, and time to ischemic stroke and hospitalization for heart failure. Univariable and multivariable Cox proportional hazards models were applied to uncover the independent factors related to the primary endpoint. Variables with P < 0.15 in univariable analyses or variables associated with outcomes (sex, age, AF history, and LAD) were selected into the multivariable model. Only a two-sided P value <0.05 was considered to be significant. Analysis was performed using R version 4.1.1 software (R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient Characteristics
After propensity score matching, 52 patients in each group were available for these analyses. There was no significant difference in baseline characteristics between the 2 groups. Overall, the median LAD was 51.0 (50.0 to 54.0) mm and 51.0 (47.0 to 54.0) mm in the HA and CA groups, respectively. Table 1 summarizes the baseline characteristics of patients.
Baseline Characteristics.
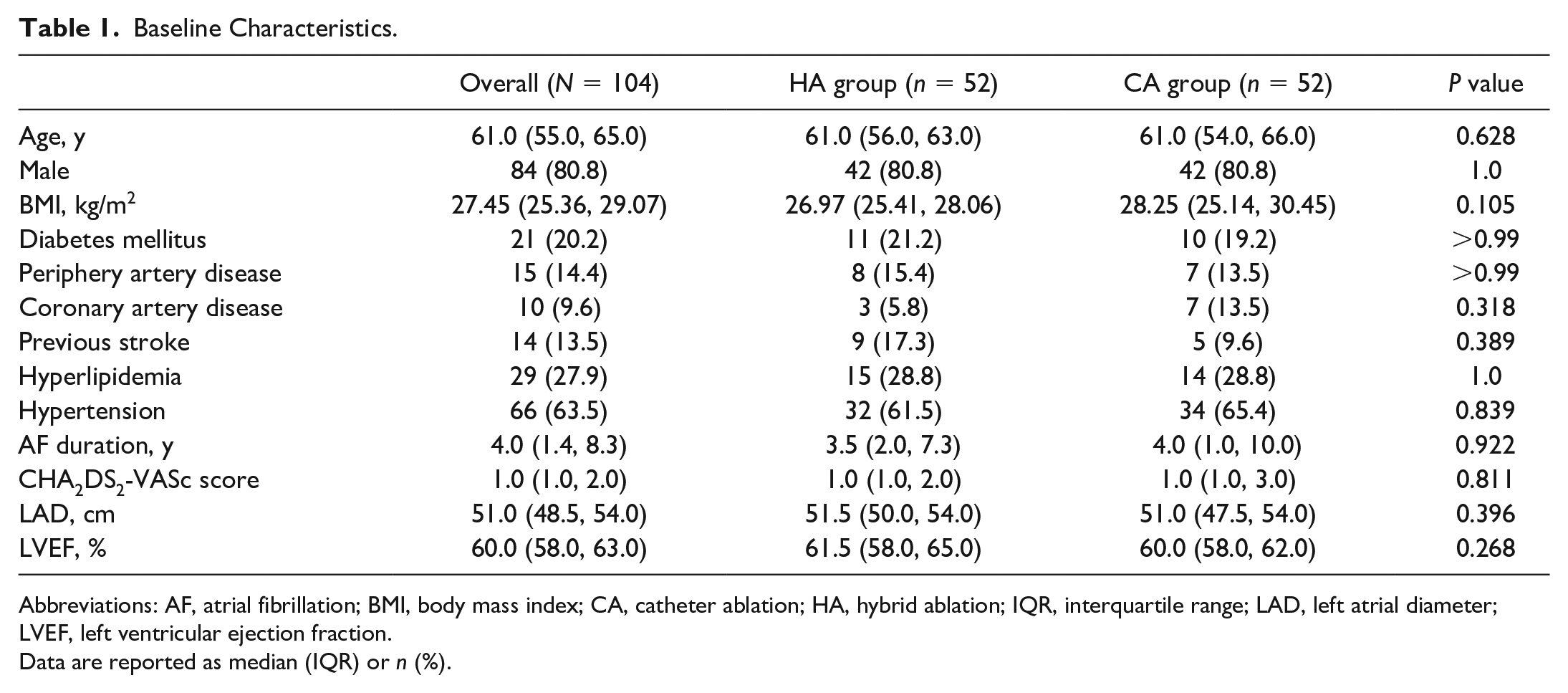
Abbreviations: AF, atrial fibrillation; BMI, body mass index; CA, catheter ablation; HA, hybrid ablation; IQR, interquartile range; LAD, left atrial diameter; LVEF, left ventricular ejection fraction.
Data are reported as median (IQR) or n (%).
Procedural Characteristics
In the CA group, the detailed procedural parameters are presented in Table 2, and voltage mapping and CA lesion set are presented in Figure 2. All patients underwent PVI and left atrial roof line.
Initial Procedural Parameters in the Catheter Ablation Group.
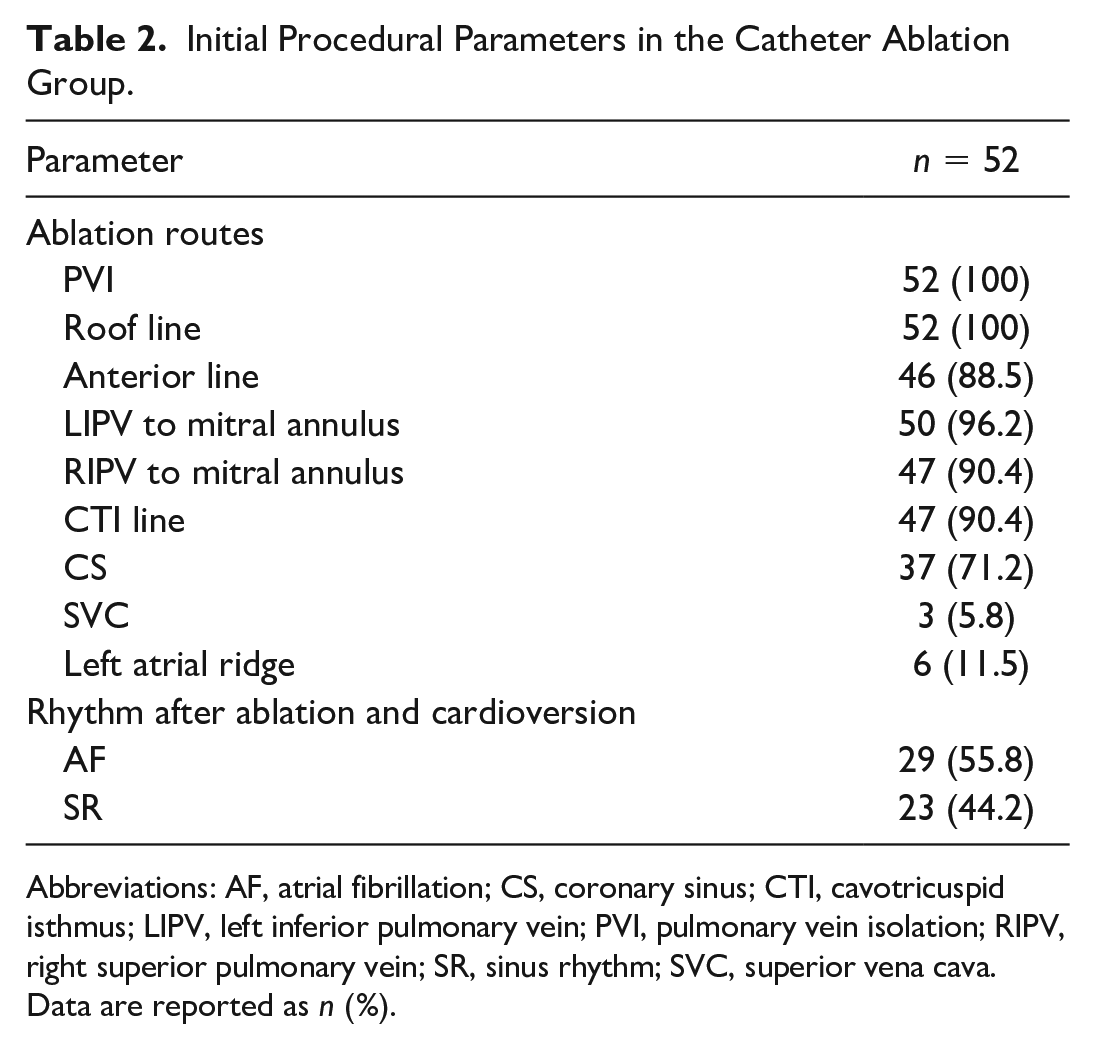
Abbreviations: AF, atrial fibrillation; CS, coronary sinus; CTI, cavotricuspid isthmus; LIPV, left inferior pulmonary vein; PVI, pulmonary vein isolation; RIPV, right superior pulmonary vein; SR, sinus rhythm; SVC, superior vena cava.
Data are reported as n (%).
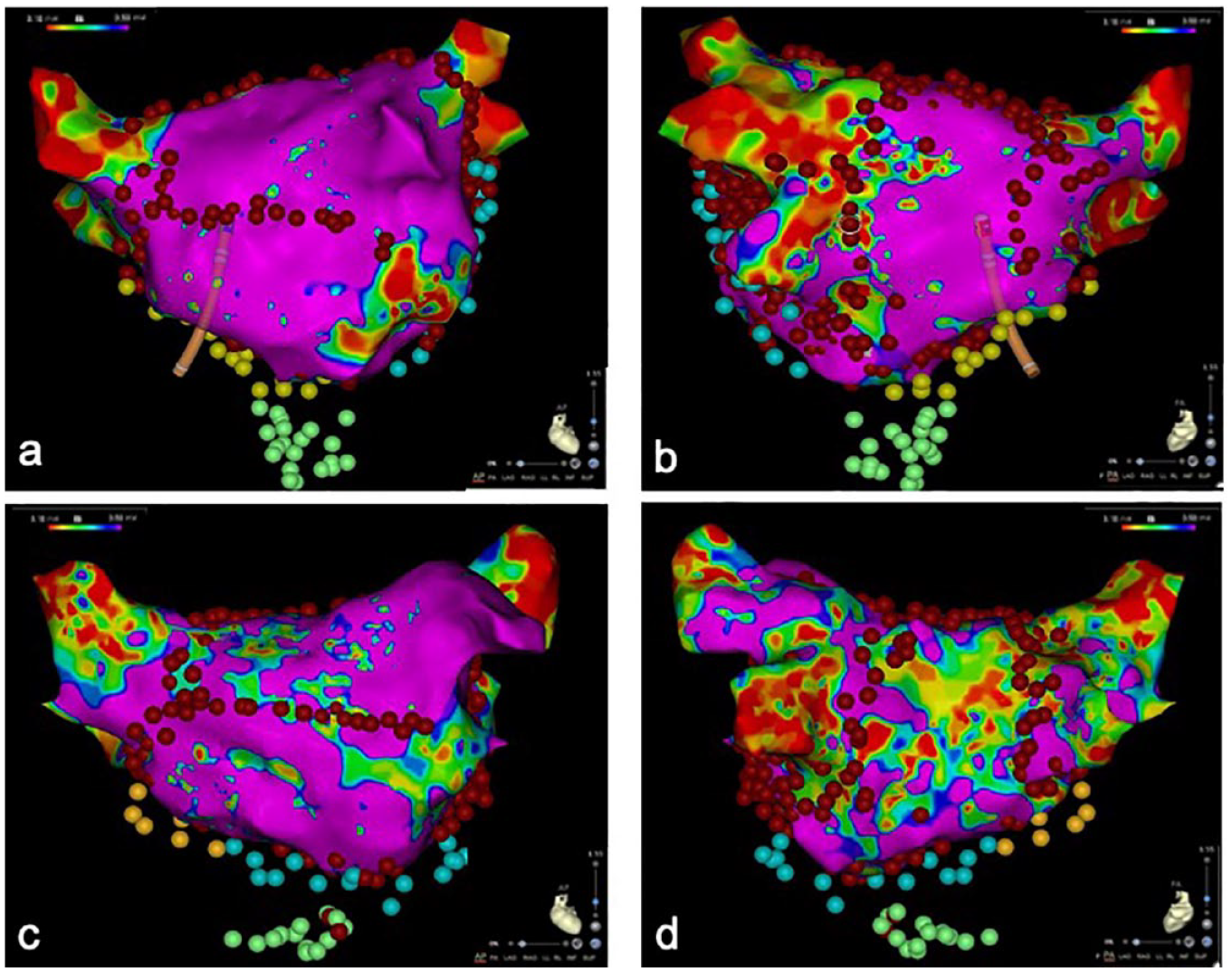
Endocardial 3-dimensional voltage mapping and catheter ablation lesion set in the catheter ablation group. (a) (b) First catheter ablation procedure. Left atrial mapping (anteroposterior view and posteroanterior view) showed the ablation lesion set including pulmonary vein isolation, the roof line, anterior line, mitral isthmus line, coronary sinus line, and cavotricuspid isthmus line. (c) (d) Second catheter ablation procedure. (c) Left atrial mapping (anteroposterior view) showed gaps in the anterior line of the first catheter ablation procedure. (d) Left atrial mapping (posteroanterior view) showed extensive low-voltage areas in the left atrial posterior wall. Endocardial voltage mapping displayed atrial models containing colored areas (low voltage) and rosy areas (normal voltage). The catheter ablation was marked with blue, red, green, and yellow dots.
In the HA group, 3 patients (5.8%) were in SR when thoracoscopic epicardial ablation was performed at the right atrium, and 1 patient (1.9%) was in SR when thoracoscopic epicardial ablation was performed at the inferior line of left atrium. After initial thoracoscopic epicardial ablation, endocardial electrophysiological mapping was performed. Left and right PV entrance-exit blocks were confirmed in 49 patients (94.2%) and in 51 patients (98.1%), respectively. The percentage of areas of persisting normal potentials of the left atrial roof line and left atrial inferior line were 7.0% and 5.7%, respectively. The linear lesion connecting the left inferior PV to the great cardiac vein had the highest percentage of areas with persisting normal potentials (16.7%; Fig. 3).
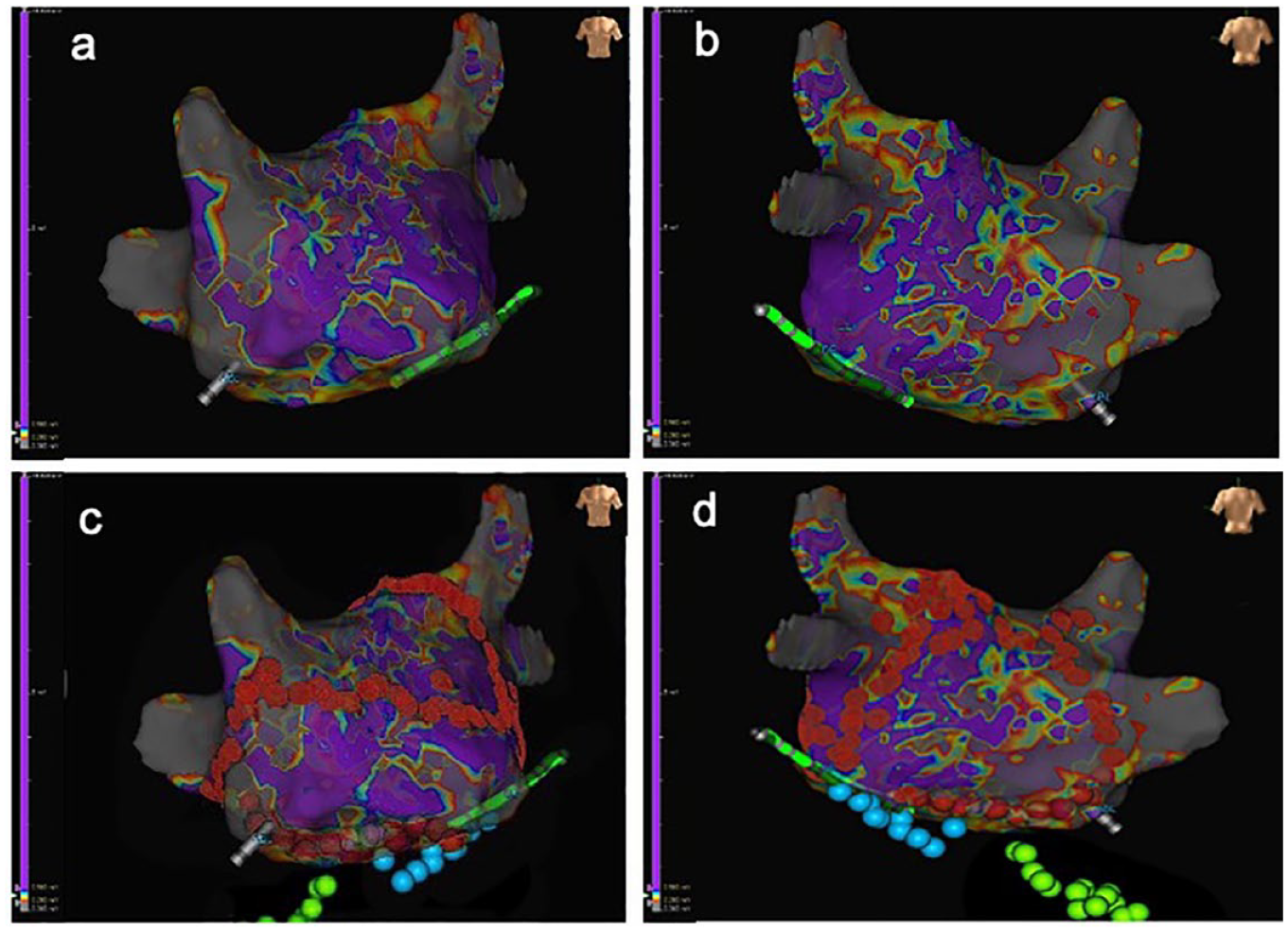
Endocardial 3-dimensional voltage mapping and catheter ablation after initial thoracoscopic epicardial ablation. (a) (b) Left atrial mapping (anteroposterior view and posteroanterior view) showing gray areas located in bilateral pulmonary veins, implying bilateral pulmonary vein isolation completed by thoracoscopic epicardial ablation. (c) (d) Based on the electrophysiological mapping in (a) and (b), reinforced endocardial catheter ablation (yellow spots) was performed at the roof line, anterior line, and bilateral pulmonary veins. The cavotricuspid isthmus line and mitral isthmus line were also created (blue spots). Endocardial voltage mapping displayed atrial models containing gray areas (no voltage), colored areas (low voltage), and purple areas (normal voltage). The catheter ablation was marked with blue, green, and red dots.
Procedural Complications
There was no significant difference in procedural complications between the 2 groups in our study including 3 patients (5.8%) in the HA group and 2 patients (3.8%) in the CA group (P > 0.999; Supplemental Table 1). Two patients (3.8%) in the HA group experienced pleural effusion with delayed withdrawal of drainage tubes. One patient (1.9%) in the HA group suffered from encapsulated hemothorax requiring thoracotomy. One patient (1.9%) in the CA group experienced pericardial effusion, and 1 patient (1.9%) underwent permanent pacemaker implantation in the hospital after the CA procedure.
Follow-Up Results
Heart rhythm
All patients were followed up for at least 6 months (36 [24 to 60] months), 99 patients (95.2%) completed the 1-year follow-up, 79 patients (76.0%) completed the 2-year follow-up, and 63 patients (60.6%) completed the 3-year follow-up. A total of 74 patients (71.2%) experienced atrial tachyarrhythmia recurrence after the 3-month blanking period. Freedom from atrial tachyarrhythmias off AADs was 57.1%, 52.7%, and 50.0% in the HA group and 25.0%, 16.2%, and 11.5% in the CA group at 12, 24, and 36 months, respectively (P < 0.001; Fig. 4a). Freedom from atrial tachyarrhythmias on AADs was 70.1%, 65.4%, and 62.6% in the HA group and 34.3%, 29.4%, and 22.0% in the CA group at 12, 24, and 36 months, respectively (P < 0.001; Fig. 4b).
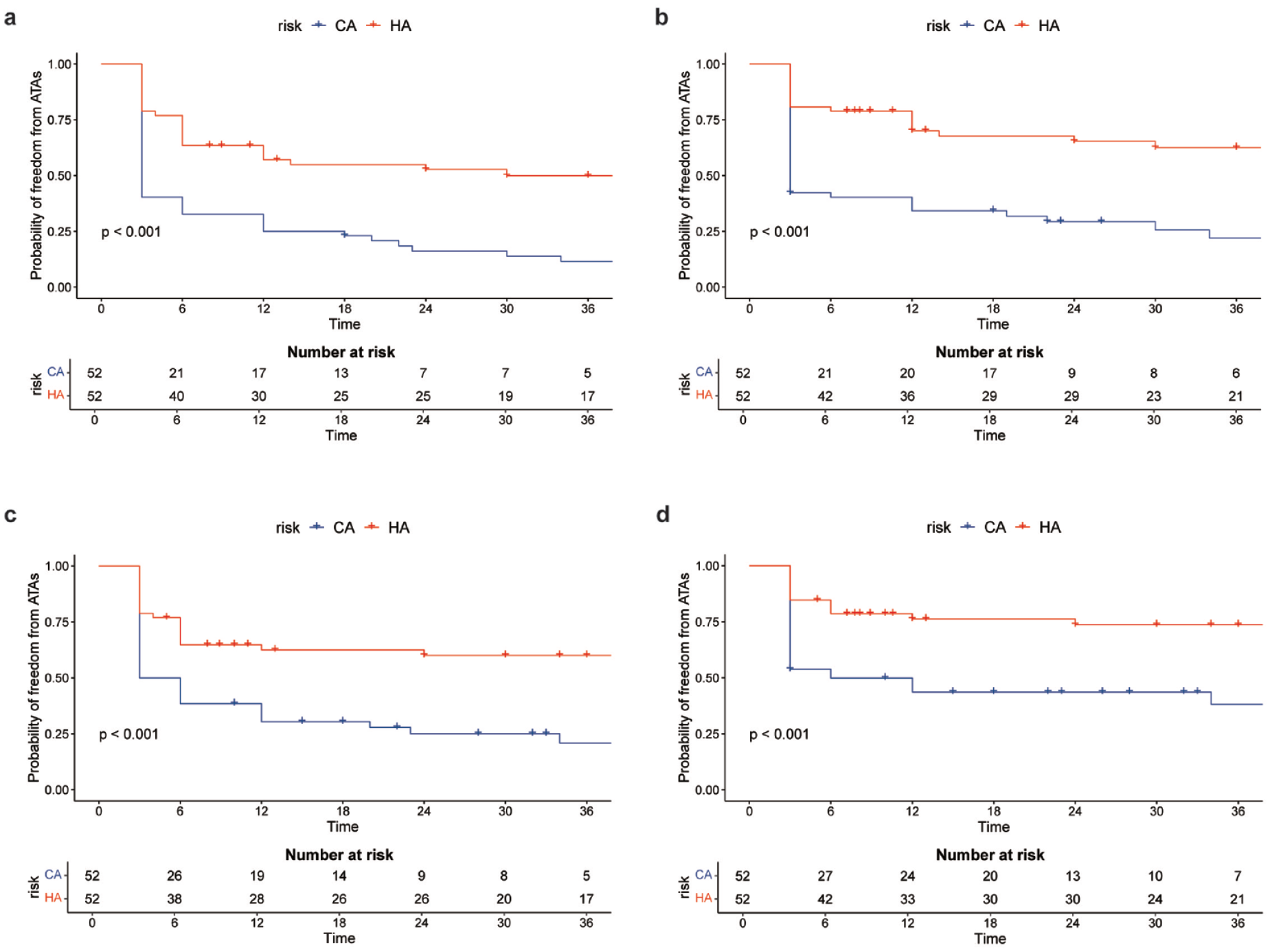
Kaplan–Meier curve showing the percentage of patients free from ATA recurrence (a) without AADs, (b) with AADs, (c) without AADs after redo CA, and (d) with AADs after redo CA. AADs, antiarrhythmic drugs; ATA, atrial tachyarrhythmia; CA, catheter ablation; HA, hybrid ablation.
Heart rhythm after redo CA
During follow-up, 7 patients (13.5%) in the HA group and 29 patients (55.8%) in the CA group underwent redo CA. Six patients (6 of 7) in the HA group and 4 patients (4 of 29) in the CA group were in SR after redo CA. Freedom from atrial tachyarrhythmias off AADs after redo CA was 62.5%, 60.1%, and 60.1% in the HA group and 30.4%, 25.1%, and 20.9% in the CA group at 12, 24, and 36 months, respectively (P < 0.001; Fig. 4c). Freedom from atrial tachyarrhythmias with AADs after redo CA was 76.2%, 73.7%, and 73.7% in the HA group and 43.6%, 43.6%, and 38.2% in the CA group at 12, 24, and 36 months, respectively (P < 0.001; Fig. 4d).
Adverse events
A total of 15 patients (28.8%) and 32 patients (61.5%) in the HA and CA groups were taking anticoagulants at last follow-up. Six patients (11.5%) in the CA group experienced ischemic stroke or transient ischemic attack (TIA) confirmed by cranial computed tomography or magnetic resonance image, whereas there were none in the HA group (P = 0.073; Supplemental Fig. 2a). More patients were hospitalized for heart failure in the CA group, although there was no significant difference (P = 0.17; Supplemental Fig. 2b). One patient died in the HA group at 54 months after the operation for unknown reason. Two patients (3.8%) in each group underwent permanent pacemaker implantation.
Predictors of atrial tachyarrhythmias recurrence
The univariable Cox regression analysis demonstrated that HA was significantly associated with a lower risk of atrial tachyarrhythmia recurrence off AADs after the blanking period (hazard ratio [HR] = 0.32, 95% CI: 0.20 to 0.53, P < 0.001). After adjustment for AF duration history, sex, age, and LAD, multivariable Cox regression analysis suggested that HA procedure was an independent risk factor for reduced risk of atrial tachyarrhythmia recurrence (HR = 0.30, 95% CI: 0.18 to 0.49, P < 0.001); LAD was an independent risk factor for increased risk of atrial tachyarrhythmia recurrence (HR = 1.05, 95% CI: 1.001 to 1.10, P = 0.046; Fig. 5).
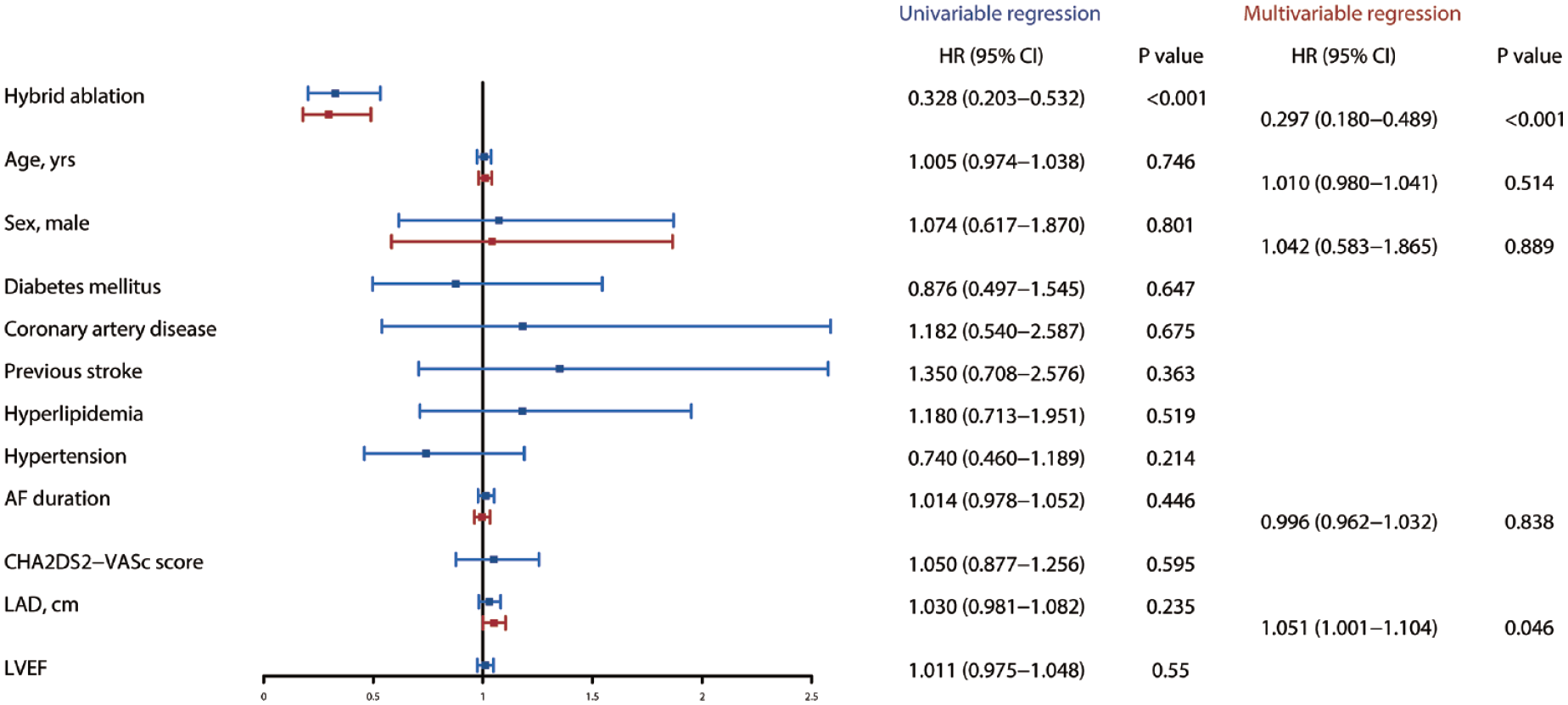
Forest plot of univariable and multivariable Cox regression analyses for recurrence of atrial tachyarrhythmias without AADs. Blue indicates univariable analyses and red indicates multivariable analyses. AADs, antiarrhythmic drugs; AF, atrial fibrillation; CI, confidence interval; HR, hazard ratio; LAD, left atrial diameter; LVEF, left ventricular ejection fraction.
Discussion
To our knowledge, this was the first article to compare the efficacy between HA and CA in patients with NPAF and enlarged left atrium. In this study, we found that for patients with NPAF and enlarged left atrium, HA was superior to catheter endocardial ablation even if redo CA was performed in terms of freedom from atrial tachyarrhythmias on or off AADs. The encouraging results with long-term follow-up of more than 36 months suggested that the HA procedure might be the first-line treatment for patients with NPAF and an enlarged left atrium.
Previous studies have demonstrated that fibrillation waves frequently cross over from the endocardial to the epicardial layers.13,14 In patients with NPAF, the frequency of epicardial breakthroughs was 4 times higher than during acute AF. 14 Even repeated endocardial ablation might not intervene in the epicardial arrhythmia substrates and triggers. Endocardial scar tissue produced by the previous endocardial ablation would hinder radiofrequency energy from transferring to deep tissue in the repeated endocardial ablation. 15 In patients with recurrent AF, atrial flutter, or atrial tachycardia, who are symptomatic and not well controlled medically, we recommend repeat CA. In our practice, we have found that postoperative recurrence of atrial flutter is more mitral isthmus dependent and also left atrial roof line gap dependent. In our study, 7 patients (13.5%) in the HA group and 29 patients (55.8%) in the CA group underwent redo CA during follow-up. However, only 4 patients (4 of 29) in the CA group had SR restored after redo CA. The reason for the results might be that repeated endocardial CA did not completely interrupt the reentry.
Thoracoscopic epicardial ablation is a rapidly emerging treatment of AF that can target the epicardial arrhythmia substrates and triggers. Moreover, continuous linear transmural lesion could be completed by bipolar radiofrequency clamp. We found that left and right PV entrance–exit blocks were confirmed in 94.2% and 98.1% patients, respectively. However, epicardial surgical ablation is unable to create efficacious isthmus lesions by transpolar radiofrequency pen and lacks the opportunity for sophisticated high-density 3-dimensional mapping. 16 In our study, there were residual endocardial potentials in most linear lesions created by transpolar pen. During simultaneous HA, subsequent endocardial mapping and ablation can target the gaps or endocardial residual potentials to improve the transmurality and contribute to the efficacy. 17
Most patients with NPAF are currently first seen by interventionists, and the CA procedure is the first treatment they learn about. Previous studies demonstrated that in patients with NPAF after failed initial CA, thoracoscopic surgical ablation is superior to CA for maintenance of SR. 18 However, due to the lack of electrophysiological mapping systems during the surgical ablation procedure, surgeons cannot be aware of electrophysiological conditions at the lesion set of the initial CA. But during the HA procedure, the advantages of electrophysiological mapping of CA could be well demonstrated. After surgical epicardial ablation, the endocardial strategy allows detailed mapping of atrial tachycardias, the atrial substrate and lesion set, and precise endocardial ablation is followed. 17
Patients in the HA group in our study underwent simultaneous HA procedures. Simultaneous HA and staged HA have their own advantages and disadvantages. As for simultaneous HA, the immediate electrophysiological mapping after surgical ablation might show “false atrial wall transmurality” due to tissue edema and inflammation. However, simultaneous HA is convenient for patients, avoids readmission after discharge, avoids repeated examinations, and reduces costs. Moreover, complications encountered during CA can be treated with surgical intervention in a timely manner. As for staged HA, although electrophysiological mapping can more objectively reflect the atrial wall transmurality of tissue damage after surgical ablation, patients need to be discharged and readmitted to the hospital, which increases the cost; in the process of waiting for the CA after the surgical procedure, patients may experience rapid atrial flutter with more obvious symptoms.19,20 According to previous studies, there was no significant difference in efficacy and safety between simultaneous HA and staged HA.19,20 Further randomized clinical trials are expected to elucidate this issue.
A previous meta-analysis showed that the rate of severe complications after an HA procedure was 5%. 19 In our study, 3 patients (5.8%) in the HA group suffered from perioperative complications, which was similar to previous studies. 19 There were no major complications, such as death, cerebrovascular accident, or atrial esophageal fistula, in our study. The satisfactory safety might be attributed to the extensive experience of the surgeons and electrophysiologists in our center. Therefore, our study emphasizes the importance of experience and the value of collaboration between cardiac surgeons and electrophysiologists. In this study, 4 patients were hospitalized for heart failure and 4 patients underwent permanent pacemaker implantation. Readmission for heart failure might be related to concomitant cardiomyopathy (secondary to prolonged history of AF) or suboptimal medical optimization following the procedure, and permanent pacemaker implantation might be related to nodal dysfunction that was preexisting and unveiled after treatment of AF. In the long-term follow-up results, we concluded that more patients in the CA group experienced stroke/TIA than in the HA group, but there was no statistical difference. In the HA group, we routinely excised the LAA by linear stapler when performing the surgical ablation procedure, which might explain the lack of stroke/TIA in the HA group. The higher success rate of ablation in the HA group also might be another contributing factor. However, the sample size of this study was small, and future studies are needed to validate this question.
Limitations
Our study had several limitations. First, the robustness of our results was restricted by its retrospective nature and limited sample size of patients. However, there are few studies on patients with NPAF and enlarged left atrium. Second, nonsymptomatic paroxysmal AF recurrence might be overlooked at each follow-up period. Repeated monitoring could partially reduce this bias. Third, potential bias might still exist, although propensity score matching was applied. The success rates of CA and repeated CA in our study were relatively low compared with previous studies, 4 which might be associated with the enlarged left atrium sizes of patients (median LAD = 51 mm). Further prospective, randomized controlled trials are needed to verify that the HA procedure has better atrial tachyarrhythmia–free survival compared with CA in patients with NPAF and enlarged left atrium. Fourth, because of the insufficient samples and follow-up duration, we did not find a statistical difference in the probability of freedom from ischemic stroke or TIA between the 2 groups.
Conclusions
In patients with NPAF and an enlarged left atrium, hybrid biatrial ablation combining epicardial and endocardial ablation might provide better freedom from atrial tachyarrhythmia recurrence than a CA procedure, even if it is a repeated CA procedure. Randomized controlled trials are warranted to validate our results.
Supplemental Material
sj-pdf-1-inv-10.1177_15569845241275161 – Supplemental material for Hybrid Biatrial Ablation Versus Catheter Ablation for Patients With Nonparoxysmal Atrial Fibrillation and Enlarged Left Atrium
Supplemental material, sj-pdf-1-inv-10.1177_15569845241275161 for Hybrid Biatrial Ablation Versus Catheter Ablation for Patients With Nonparoxysmal Atrial Fibrillation and Enlarged Left Atrium by Chunyu Yu, Haojie Li, Zhiwei Zeng, Lihui Zheng, Lingmin Wu, Ligang Ding, Yan Yao and Zhe Zheng in Innovations
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences (CIFMS, 2021-I2M-1-063) and the State Sponsored Postdoctoral Researcher Programme (GZC20230304). The funder had no role in study design, data collection, data analysis, data interpretation, or writing of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.