A Hepatocellular Carcinoma Intheheart With No Other Primary. Can Be? Case Report And Review of Literature
Tamer M. Abdalghafoor, Dina alwaheidi, Mohamad El-Kahlout, Mohd Lateef Wani, Abdulwahid Al Mulla. Hamad Medical Corporation, Doha, Qatar.
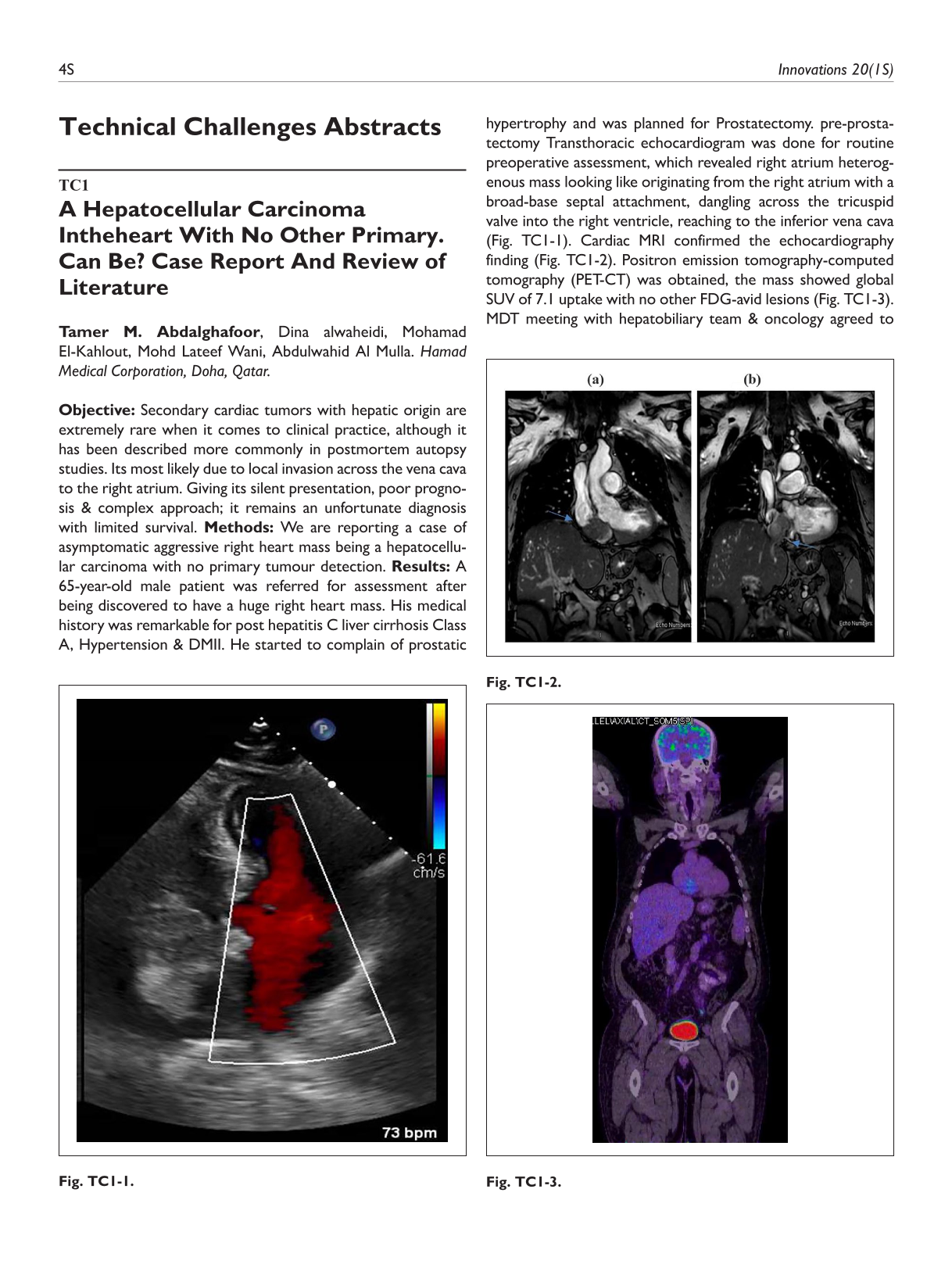
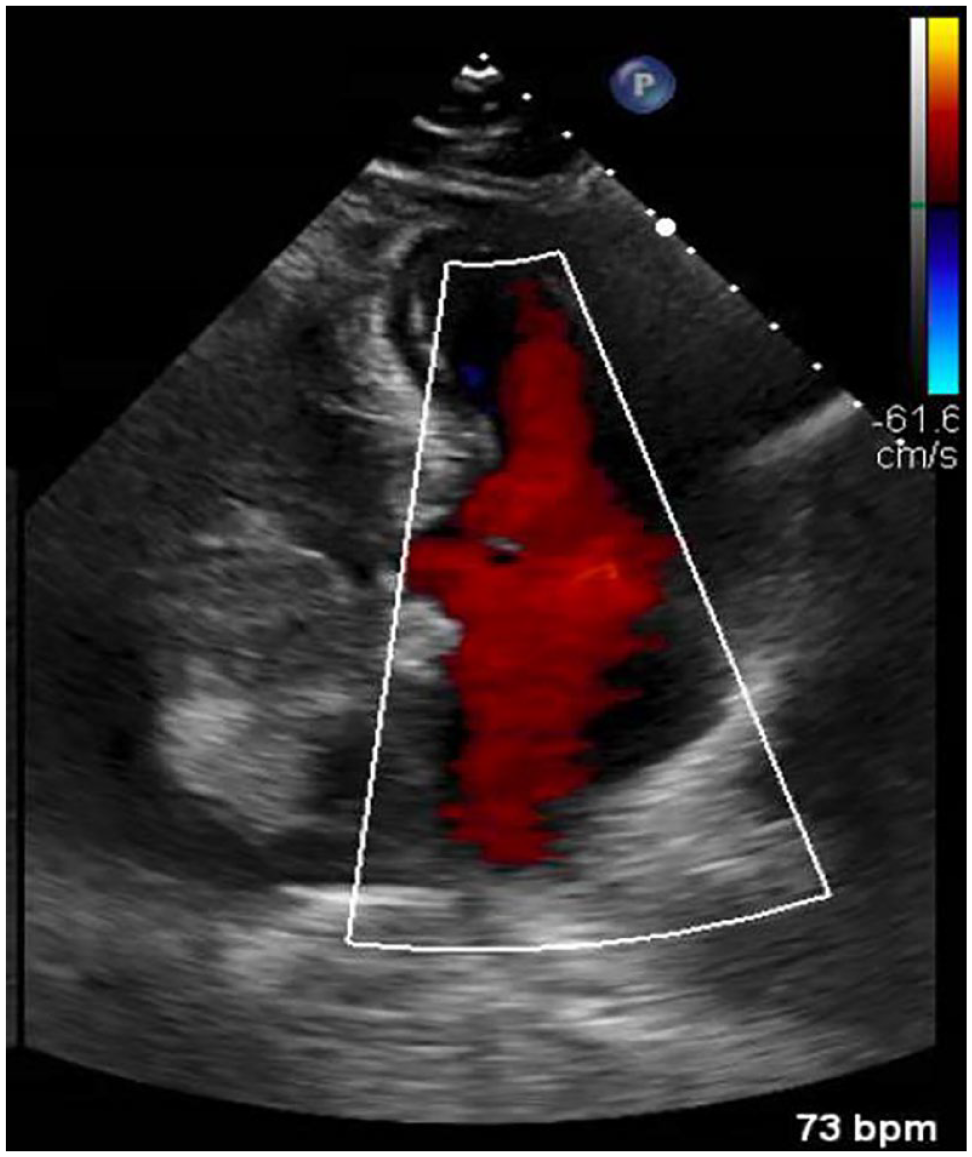
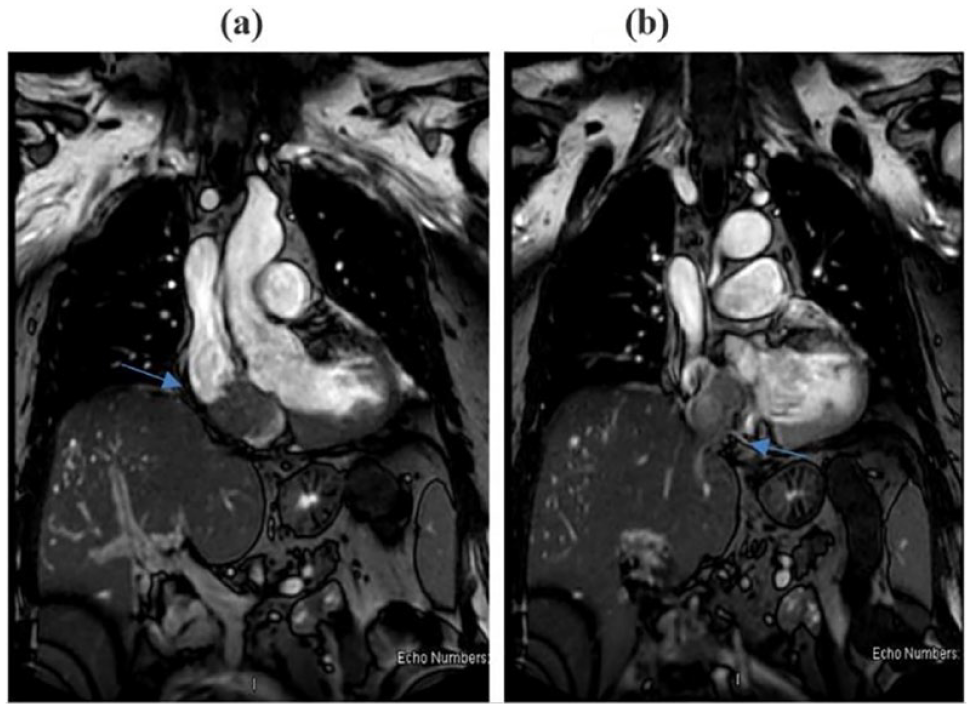
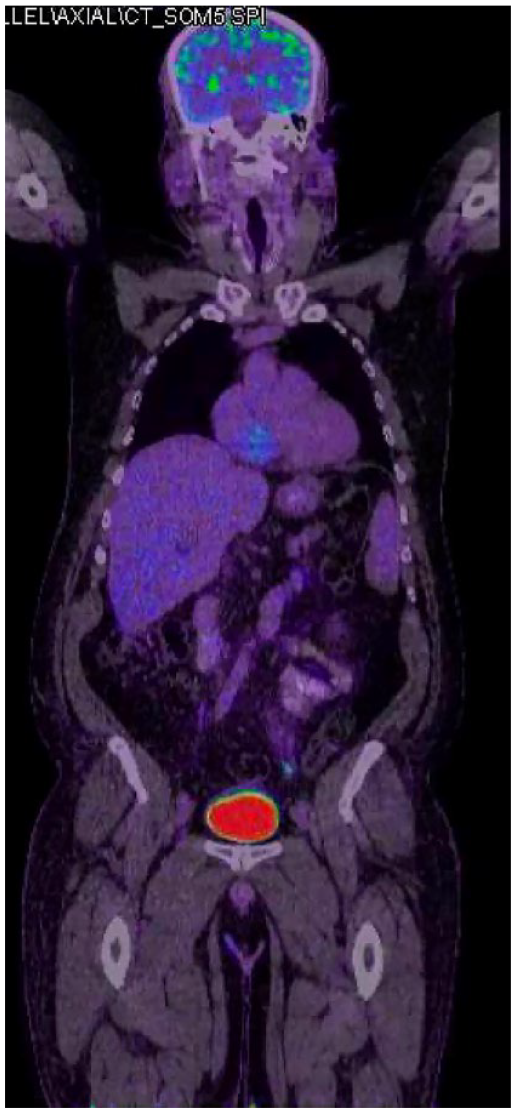
Objective: Secondary cardiac tumors with hepatic origin are extremely rare when it comes to clinical practice, although it has been described more commonly in postmortem autopsy studies. Its most likely due to local invasion across the vena cava to the right atrium. Giving its silent presentation, poor prognosis & complex approach; it remains an unfortunate diagnosis with limited survival. Methods: We are reporting a case of asymptomatic aggressive right heart mass being a hepatocellular carcinoma with no primary tumour detection. Results: A 65-year-old male patient was referred for assessment after being discovered to have a huge right heart mass. His medical history was remarkable for post hepatitis C liver cirrhosis Class A, Hypertension & DMII. He started to complain of prostatic hypertrophy and was planned for Prostatectomy. pre-prostatectomy Transthoracic echocardiogram was done for routine preoperative assessment, which revealed right atrium heterogenous mass looking like originating from the right atrium with a broad-base septal attachment, dangling across the tricuspid valve into the right ventricle, reaching to the inferior vena cava (Fig. TC1-1). Cardiac MRI confirmed the echocardiography finding (Fig. TC1-2). Positron emission tomography-computed tomography (PET-CT) was obtained, the mass showed global SUV of 7.1 uptake with no other FDG-avid lesions (Fig. TC1-3). MDT meeting with hepatobiliary team & oncology agreed to proceed for excisional biopsy of the mass for definitive diagnosis & treatment.Unfortunately, complete excision was impossible but debulking of the mass was done as much as possible & sent for histopathology examination. The patient post-operative course was unremarkable & he was discharged on the 5thHis pathology showed a hepatocellular carcinoma. Referring to oncology team decision was to start systemic chemotherapy. He received his first cycle & currently he is on follow up. Conclusions: Secondary tumors to the heart might be more common than expected and occult HCC lesion could cause diagnostic dilemma.
TC2
Uniportal Endoscopic Resection of a LV Lipoma
Moritz C. Wyler von Ballmoos1, Qasim Al Abri2. 1University Hospital Zurich & University of Zurich, Zurich, Switzerland, 2Houston Methodist DeBakey Heart & Vascular Center, Houston, TX, USA.
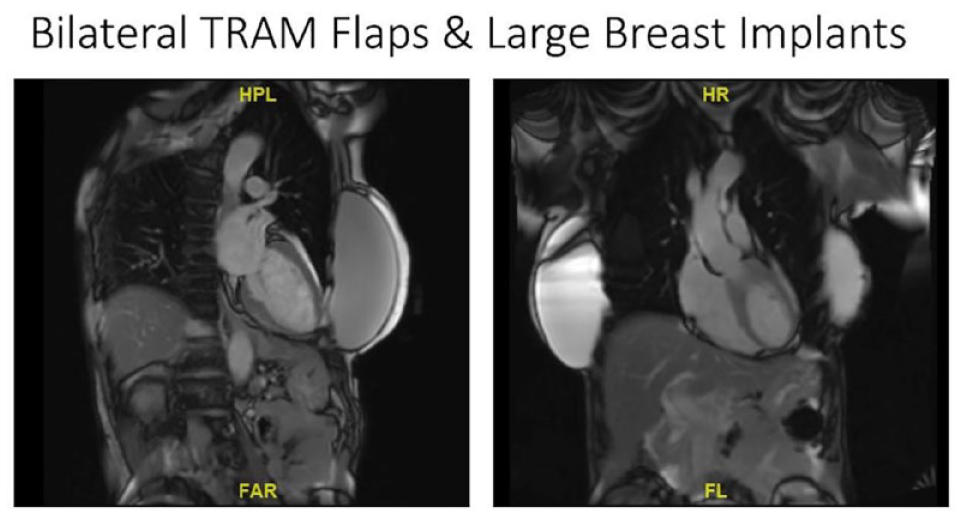
Objective: A 55-year-old patient had an incidental finding of a leftventricular mass on a screening CT scan that was performed with IV contrast. Inthe year prior, she underwent radical mastectomy bilaterally for breast cancer,and a complex reconstruction with bilateral TRAM flaps and large volumesilicone implants (Fig. TC2-1). Further workup of the LV mass by TEE and CMRconfirmed a mobile, lobulated lipoma of approximately 1.5cm x 1cm in the leftventricle underneath the mitral valve. Given the size and mobility of the lipoma,the concern for possible thromboembolic events, resection was offered to thepatient who wanted to proceed with resection. Methods: A standard sternotomy would have been the simplestapproach to resect the tumor. However, the patient expressed a strong desire fora less invasive, sternal-sparing approach. Given the bilateral TRAM flaps andlarge breast implant occupying most of the anterolateral chest wall, there waslimited space available to plan the access. 3-dimensional reconstructions of thecardiac CT scan were used to determine an access site away from the implantsand the right internal thoracic artery with the intent to proceed with a endoscopicresection of the LV lipoma. Percutaneous femoral arterial and venouscannulation was used for cardiopulmonary bypass. Using the endoscope, theaorta was opened after clamping the aorta and arresting the heart with del Nidocardioplegia. The endoscope was inserted into the LV and the lipoma wasidentified and completely resected. The aortotomy was then closed in a standardfashion, the heart deaired and the patient was weaned from CPB. The femoralarterial cannulation was closed with a MANTA device. Results: The patient was discharged home on postoperative day 2. Finalpathology confirmed a lipoma. Conclusions: This presentation & video details CCTA planning for the mostsuitable approach and incision mapping given anatomic constraints as well asthe exact steps of performing an endoscopic cardiac surgery procedure througha single incision.
CT imaging demonstrating extent of large breast implants limitingaccess to the thorax anteriorly and laterally.
TC3
Mini Thoracotomy for ASD Closure in a Patient With Large Breast Implants
Lisardo Garcia. Baptist Health South Florida/Florida International University, Miami, FL, USA.
Objective: Mini thoracotomy has become a safe and less invasive technique to perform cardiac surgery. In patients with breast implants this approach may be challenging. Literature in this area is scarce. Herein we present a female with large breast implants who required surgical repair of an atrial septal defect. Methods: A 53-year-old woman presented to the emergency room complaining of a several week history of shortness of breath and mild chest pain. She had had bilateral breast augmentation with silicon implants six years before her admission. Cardiology work-up revealed a large secundum atrial septal defect with left to right shunting (Qp/Qs 2.2) and enlarged right sided chambers. Patient was not a good candidate for percutaneous approach, and she was referred for surgical closure. On physical exam the breast was soft with no evidence of capsular contracture. The case was discussed with plastic surgery for advice. Results: Right mini thoracotomy was performed through her previous inframammary incision. The breast implant capsule was carefully opened widely, the silicone implant was removed and placed in a basin with betadine solution. The fifth intercostal space was opened; Cardiopulmonary bypass was instituted femorally and the aorta was cross clamped. A single dose of custodiol cardioplegia was given. The large secundum ASD was closed with a 3 x 4 cm pericardial patch. The patient was weaned off cardiopulmonary bypass. The intercostal space was reapproximated with a figure 8 heavy suture; the posterior aspect of the implant’s capsule was closed with a running suture to prevent implant migration. The breast implant was then placed back, and the remaining capsule closed with a continuous suture. Subcutaneous tissue and skin were closed in standard fashion. The patient was discharged home on POD 3 and was seen for follow up three weeks later with no issues. Conclusions: Minimally invasive cardiac surgery can be performed safely in patients with large breast implants. Several factors such as implant age and capsule assessment need to be considered before surgery. Careful handling of the implant and closure of the posterior aspect of the capsule are of paramount importance to prevent complications.
TC4
Percutaneous Trans Catheter Mitral Valve-in-valve Implantation in Surgical Bio-Prosthetic Valve Fracture for Optimising Hemodynamics
Attaullah Khan Niazi1, Mohammed Sharif Nassery2. 1Shalamar Hospital Lahore, Lahore, Pakistan, 2Punjab institute of Cardiokogy, Lahore, Pakistan.
Objective: Transcatheter valve-in-valve implantation is an attractive option for treating surgicalprosthetic valve dysfunction. High residual gradient remains a concern, especially for surgical valves with a small true internal dimensionLimited data exists for bio-prosthetic valve fracture in the mitral position. Present case highlights surgical bioprosthetic valve fracture done to allow full expansion of the transcatheter valve and optimize hemodynamics. Methods: Presenting complaints: breathlessness on exertion on walking 1 fight of stairs or greater since 2017. Past medical details: - Diabetic and hypertensive , 2008,2013 NSTEMI PCI mid LAD - 2017: worsening of dyspnoea , Moderate mitral regurgitation with mild left ventricular systolic dysfunction., Progressive CAD, CABG (SVG to LAD, OM ) with MVR ( Bioprosthetic valve SJM EPIC 25; Tammerfors)2017 Investigation NT Pro BNP- >3000 pg/ml Mean PA pressure- 40mmHg (Cath) ECHO - prosthetic valve dysfunction , Bioprosthetic valve thickened & restricted in Transmitral mean gdt-11mmHg, mitral regurgitation CT parameter Procedure - Transcatheter mitral valve in valve implantation. Transfemoral access. General anesthesia, TEE guidance. Results: 6 months followup Significant improvement of his symptoms. Mean mitral gradient- 4mmHg. No valve thrombosis. Conclusions: This case highlights successful fracture of a surgical bio-prosthetic valve to improve hemodynamics during trans catheter mitral valve- in-valve implantation.
TC5
Recurrent Mitral Regurgitation After Previous Alfieri Stitch, A Case of Transcatheter Mitral Edge-to-Edge Repair
Attaullah Khan Niazi1, Mohammed Sharif2. 1Shalamar Hospital Lahore, Lahore, Pakistan, 2Punjab institute of Cardiology, Lahore, Pakistan.
Objective: 72 year old male, wheelchair bound due to NYHA Class III symptoms with clinical signs of heart failure Past Medical History: AorticrootreplacementwithbioprostheticAVR (2015) and Alfieri repair to mitral valve , Residual moderate-severe mitral regurgitation post-operatively. Permanent atrial fibrillation. Amiodarone induced thyroid dysfunction. Transoesophageal echocardiogram. Severe mitral regurgitation secondary to P2/P3 prolapse. Mild left ventricular impairment in the context of severe mitral regurgitation (ejection fraction 50%). Well seated bioprosthetic aortic valve with normal function (MV mean gradient < 2mmHg Suitable anatomy for Mitral TEER). Methods: Procedural details. Day-case procedure. General anaesthetic/ Transoesophageal echo- guided. Device:PascalACE(EdwardsLifesciences). Access: 11F right femoral vein, pre-closed with 2 x Proglides. Transseptal puncture positioned mid- posteroseptumImplantpositionedmedialtoAlfieristitch(over dominant jet). Results: Final Result. Stable device position. Mild residual MR. Mitral valve mean gradient unchanged (<3mmHg). Conclusions: This case highlights the differences between the Alfieri procedure vs transcatheter edge-to-edge repair (TEER) i. Ability to check the final result in TEER before the end of the procedure under haemodynamically ‘normal’ conditions ii. Can try multiple positions of device and optimise leaflet grasp to get the best possible result. Demonstrates the maneuverability of the Pascal device in challenging anatomy.
TC6
Challenging Hybrid Repair of Non-A-Non-B Aortic Dissection in Patient With Right Sided Angulated Aortic Arch
Yama Shoaib Haqzad, Mohamed Shoeib, Mohamed Sherif, Massimo Cappoccia, Ahmed Nassef, Sapna Puppala, David Shaw, Paul Walker, Pankaj Kaul, Walid ElMahdy. Leeds Teaching Hospitals NHS Trust, Leeds, United Kingdom.
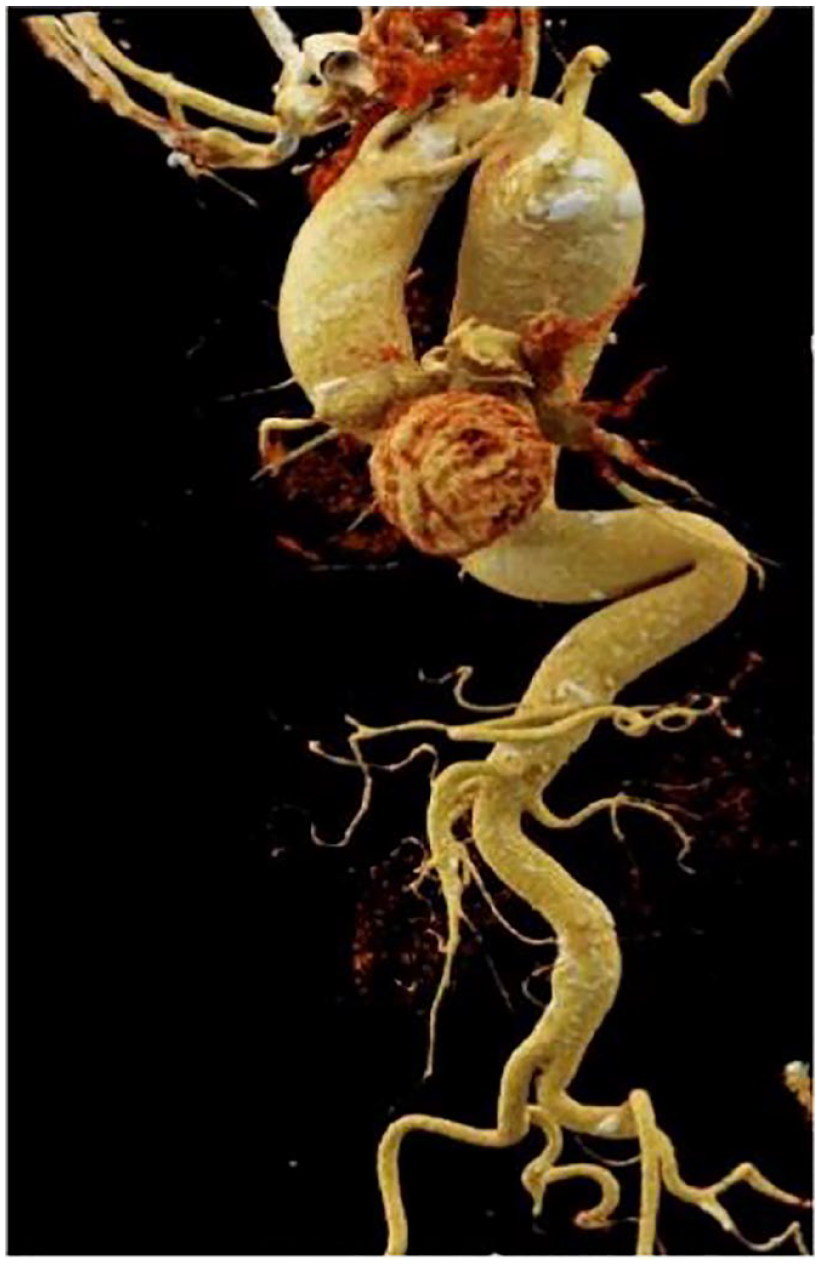
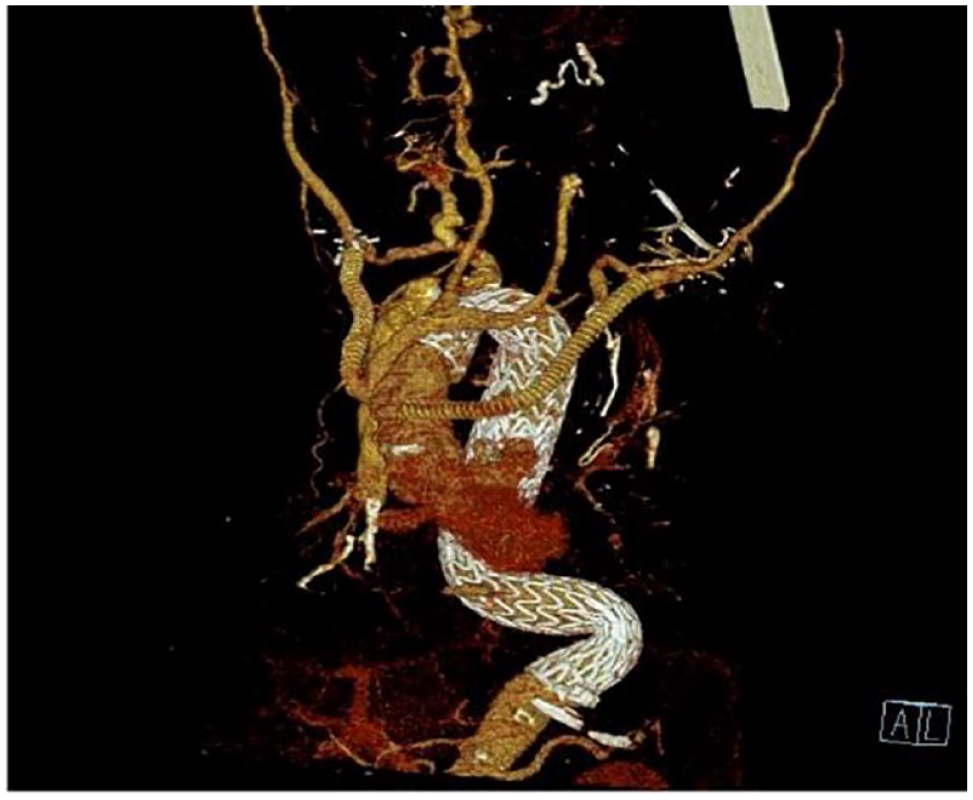
Objective: Patients with right sided aortic arch have a predisposition to develop aortic dissection (AD). The term non-A-non-B aortic dissection was recently updated in the ESVS/EACTS consensus, defined as type B dissection with involvement of the aortic arch. Evidence regarding optimal management is limited. This is a challenging case that was managed successfully using hybrid technique with the involvement of the aortovascular multidisciplinary team(MDT). Methods: 70-year-old lady, with history of hypertension and right sided, angulated (gothic) aortic arch with descending thoracic aortic aneurysm(under surveillance),presented acutely with non-A-non-B aortic dissection, measuring 64mm. The tear just distal to left subclavian origin extending to diaphragmatic hiatus, with retrograde extension to aortic arch and dilated ascending aorta. Anomalous origins of supra aortic vessels, significant angulation and calcification of the aortic arch at the origin of subclavian arteries.Aortovascular MDT concluded non feasibility of endovascular options due to significant aortic angulation, absence of suitable landing zone with high risk of retrograde aortic dissection. Moreover, Frozen Elephant Trunk(FET) was not deemed an option due to risk of failure of expansion of FET stent (weak radial force)in gothic angled arch. Hybrid repair was agreed to be the best option. Results: Joint procedure in Hybrid theatre involving cardiac surgeons, vascular surgeons and vascular interventional radiologists. She underwent ascending aorta replacement, aortic arch debranching with extra-anatomical bypass of both subclavian arteries, and “branch first” technique for both carotid arteries + direct antegrade aortic arch/descending aortic TEVAR(GORE TAG Conformable Stent)connected to aortic graft as a hybrid elephant trunk. The patient had uneventful endovascular coiling of proximal left subclavian artery and TEVAR extension of the descending aorta same admission. Patient survived without bleeding, stroke, paraplegia or malperfusion. Transient vocal cord palsy recovered before her discharge. Conclusions: None A none B AD involving right sided aorta is an extremely rare condition , with limited evidence for optimal management.Aortvascular MDTs with the involvement of cardiac/vascular surgeons, vascular interventionist and anaesthetists allow complex rare aortic cases to be assessed with consideration of relative risks and benefits of various approaches. Hybrid approach for complex aortic pathologies can thus offer safe management strategies, especially in cases like this with challenging anatomy.
TC7
Valve-in-Ring, Possible, But Needs Planning
Gry Dahle, MD PhD1, Per Snorre Lingaas, MD1, Kjell Arne Rein, MD PhD2. 1Rikshospitalet, OUS, Oslo, Norway, 2Rikshospitalet, OUS, OSLO, Norway.
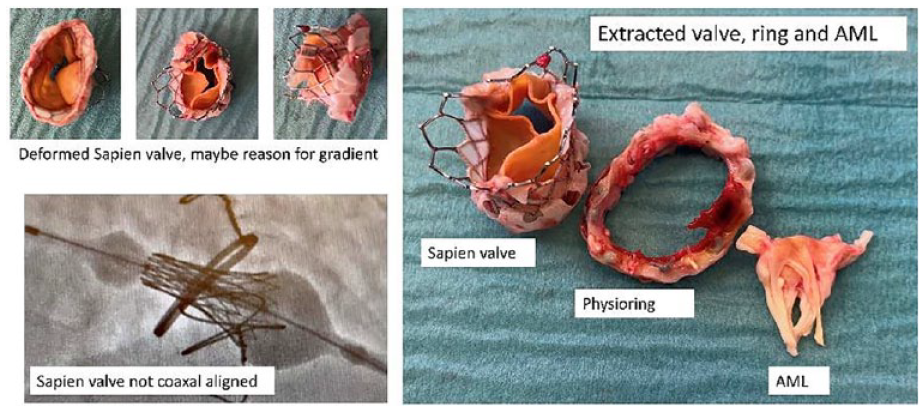
Objective: Valve-in-ring may be an option for patients with failed mitral valve repairs. However, to have a successful procedure some critical features have to be considered. We present a patient who underwent a valve-in-ring procedure for failed repair, but ended up with open redo surgery. Methods: A male, 77 years with atrial fibrillation and hypertension was referred with residual mitral valve regurgitation nine years after previous mitral valve repair with neochorda and Physioring size 32 (Edwards Lifesciences, CA) and coronary artery bypass grafting with initially good result. Evaluation for valve in ring was done by CT reconstruction and echo assessment. He was found anatomically suitable for valve in ring. The procedure was performed in general anesthesia, echo and fluoro guidance and transfemoral, transseptal approach, Edwards Sapien S3 ultra (Edwards Lifesciences, CA) size 29 was choosen. Results: Unfortunately, the valve was not co-axially deployed and there was a substantial paravalvular leak. The antegrade gradient was 9 mmHg and LVOT obstruction occurred. The patient was observed for 3 months. He developed hemolysis requiring weekly blood transfusions, AV block in need of pacemaker, ASD due to transseptal puncture as well as heart- and renal failure. The decision was made for open redo surgery. The Physioring and the Sapien valve was removed, resection of the AML (anterior mitral leaflet) was performed, a Magna Ease mitral valve (Edwards Lifesciences, CA) implanted and the ASD closed. The patient was extubated 9.5 h postoperatively, inotrop support discontinued after 24h. At 3 mo follow up, renal function and hemolysis parameters were normalized. He was in NYHA class II, had no further need of blood transfusion and the mitral valve was well functioning. Conclusions: Surgical mitral valve repairs may fail, and for selected patients, valve-in-ring may be performed. Pre-procedural planning is important and procedural accuracy is essential. Transfemoral transseptal approach is the less invasive, but transapical approach may sometimes be considered for better coaxial alignment to avoid these observed complications.