Efficacy of Single Anesthesia Bronchoscopy and Resection Utilizing the Shape Sensing Robotic Navigational Platform
Bhupaul Ramsuchit, Nicholas MacDonald, Matthew Johnston, Juan Escalon, Luis Herrera. Orlando Health, Orlando, FL, USA.
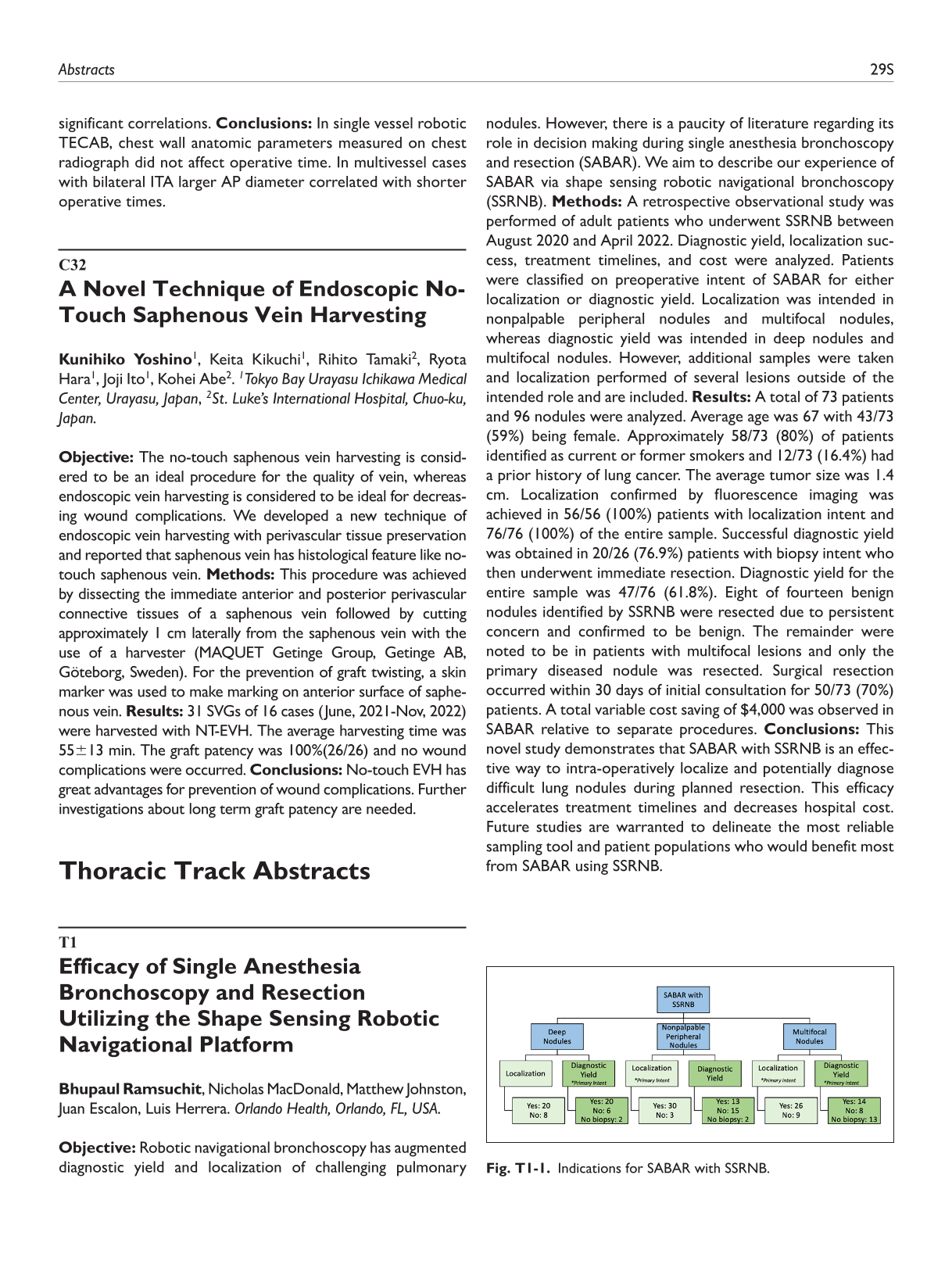
Objective: Robotic navigational bronchoscopy has augmented diagnostic yield and localization of challenging pulmonary nodules. However, there is a paucity of literature regarding its role in decision making during single anesthesia bronchoscopy and resection (SABAR). We aim to describe our experience of SABAR via shape sensing robotic navigational bronchoscopy (SSRNB). Methods: A retrospective observational study was performed of adult patients who underwent SSRNB between August 2020 and April 2022. Diagnostic yield, localization success, treatment timelines, and cost were analyzed. Patients were classified on preoperative intent of SABAR for either localization or diagnostic yield. Localization was intended in nonpalpable peripheral nodules and multifocal nodules, whereas diagnostic yield was intended in deep nodules and multifocal nodules. However, additional samples were taken and localization performed of several lesions outside of the intended role and are included. Results: A total of 73 patients and 96 nodules were analyzed. Average age was 67 with 43/73 (59%) being female. Approximately 58/73 (80%) of patients identified as current or former smokers and 12/73 (16.4%) had a prior history of lung cancer. The average tumor size was 1.4 cm. Localization confirmed by fluorescence imaging was achieved in 56/56 (100%) patients with localization intent and 76/76 (100%) of the entire sample. Successful diagnostic yield was obtained in 20/26 (76.9%) patients with biopsy intent who then underwent immediate resection. Diagnostic yield for the entire sample was 47/76 (61.8%). Eight of fourteen benign nodules identified by SSRNB were resected due to persistent concern and confirmed to be benign. The remainder were noted to be in patients with multifocal lesions and only the primary diseased nodule was resected. Surgical resection occurred within 30 days of initial consultation for 50/73 (70%) patients. A total variable cost saving of $4,000 was observed in SABAR relative to separate procedures. Conclusions: This novel study demonstrates that SABAR with SSRNB is an effective way to intra-operatively localize and potentially diagnose difficult lung nodules during planned resection. This efficacy accelerates treatment timelines and decreases hospital cost. Future studies are warranted to delineate the most reliable sampling tool and patient populations who would benefit most from SABAR using SSRNB.
Indications for SABAR with SSRNB.
T2
Robotic-Assisted Bronchoscopy for Identification of Lung Nodules in Minimally-Invasive Thoracic Surgery
James Shahoud, Benny Weksler, Sohini Ghosh, Aarthi Ganesh, Hiran Fernando. Allegheny General Hospital, Pittsburgh, PA, USA.
Objective: Small pulmonary nodules can be difficult to identify during a minimally invasive surgical (MIS) resection. Previous investigators have reported using bronchoscopy with electromagnetic navigation to help identify lesions. Robotic-assisted bronchoscopy has recently been introduced into clinical practice and has shown utility in identifying small lesions. We report our early experience using robotic-assisted bronchoscopy (with the ION system) with dye marking to aid in minimally invasive thoracic surgery. Methods: Patients with peripheral pulmonary nodules underwent robotic-assisted bronchoscopy before a planned minimally invasive resection, using either robot-assisted or video-assisted thoracic surgery approach. Indocyanine green or methylene blue was injected directly into the targeted lesion. Surgical resection was then performed. Primary success was defined as successful dye localization and sub-lobar resection of the target nodule. Secondary success was defined as successful identification of the lesion without the need for lobectomy or thoracotomy. Results: Thirty patients with a single targeted nodule underwent robot-assisted bronchoscopy followed by MIS resection. Median lesion size was 9 mm (4-25 mm) and the median distance from the pleura was 5 mm (1-32 mm). Primary success rate was 83.3% (25/30). In three cases the dye was not visualized and in two cases there was free extravasation of dye. Secondary success rate was 100%. Pathology revealed non-small cell lung cancer (n = 13, 43.3%), metastatic disease (n = 11, 36.7%), and benign disease (n = 6, 20%). There were no complications related to the use of robotic-assisted bronchoscopy. Conclusions: Robotic-assisted bronchoscopy with dye marking is safe and effective for guiding minimally invasive resection of small peripheral pulmonary nodules.
T3
Contemporary Incidence of Synchronous Multiple Primary Lung Cancers in the Era of Lung Cancer Screening
Nika Samadzadeh Tabrizi, Ben Gallant, Erin Harris, Brian N. Arnold, Thomas Fabian. Albany Medical College, Albany, NY, USA.
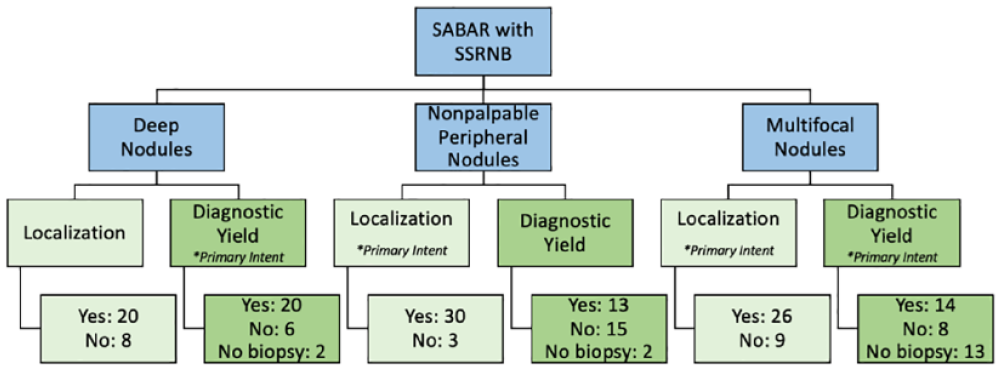
Objective: Not only does the reported incidence of synchronous multiple primary lung cancer (SMPLC) vary widely in the literature, 0.2 - 8%, but so does the reported 5-year survival, 10 - 76%. This discrepancy is partially attributed to inconsistent identification of SMPLCs which has hindered our understanding of these patients. Utilizing strict inclusion criteria, we sought to identify the contemporary incidence and survival of patients with SMPLC. Methods: From January 2018 to September 2019, 227 consecutive patients who underwent lung cancer resection at a single academic institution were retrospectively reviewed. Using the modified Martini criteria, patients with SMPLC were included. Three patients were excluded from survival analysis due to failure to undergo R0 resection for all tumors. Results: During the 21-month period, 297 lung cancers were resected with curative intent. 47 (21%) patients had 113 tumors that were pathologically confirmed SMPLC. Overall and cancer-specific survival (Fig. T3-1) was 42/44 (96%) and 42/43 (98%), 42/44 (96%) and 42/43 (98%), 38/43 (88%) and 38/41 (93%) at 1-, 2-, and 3-years respectively. In those with two SMPLC, tumors were ipsilateral in 20 (43%) and bilateral in 14 (30%). 13 (28%) had multiple tumors which was associated with a significantly lower overall (P = 0.043) and cancer-specific (P = 0.002) survival. Tumor histology was different in 38 (81%) patients. Most tumors were composed of only adenocarcinomas in 28 (60%) or adenocarcinoma(s) mixed with another histologic type in 12 (25%). Adenocarcinomas had a significantly lower overall survival (P = 0.005), but cancer-specific survival was not significantly different (P = 0.08). Demographics and pathologic staging also did not significantly impact survival. Conclusions: The incidence of SMPLC is much higher than historical data would predict. Our 3-year overall survival is also considerably higher than what has been reported, 88% and 63% respectively. This study is highly exclusive and likely reflects the true outcomes for patients with SMPLC. Survivorship in these patients suggests that SMPLCs behave like primary lung cancers - which can be treated with sublobar resection - not metastatic disease. Awareness of SMPLC by thoracic surgeons is critical in accurately staging, managing, and optimizing outcomes in this patient population.
Kaplan-Meier survival curve depicting overall and cancer-specific survival (N = 44). Shaded areas indicate 95% confidence intervals.
T4
Comparison of Robotic-Assisted Versus Video-Assisted Thoracoscopic Segmentectomy: A Single Institution Propensity Matched Study
Kojo Agyabeng-Dadzie1, Inderpal S. Sarkaria1, Ernest Chan1, Ian Christie1, Summer Mazur1, Kristine Ruppert2, Neil Christie1, Omar Awais1, Ryan Levy1, Nicholas Baker1, Rajeev Dhupar1, Arjun Pennathur1, James D. Luketich1, Matthew Schuchert1. 1University of Pittsburgh Medical Center, Pittsburgh, PA, USA, 2University of Pittsburgh, Pittsburgh, PA, USA.
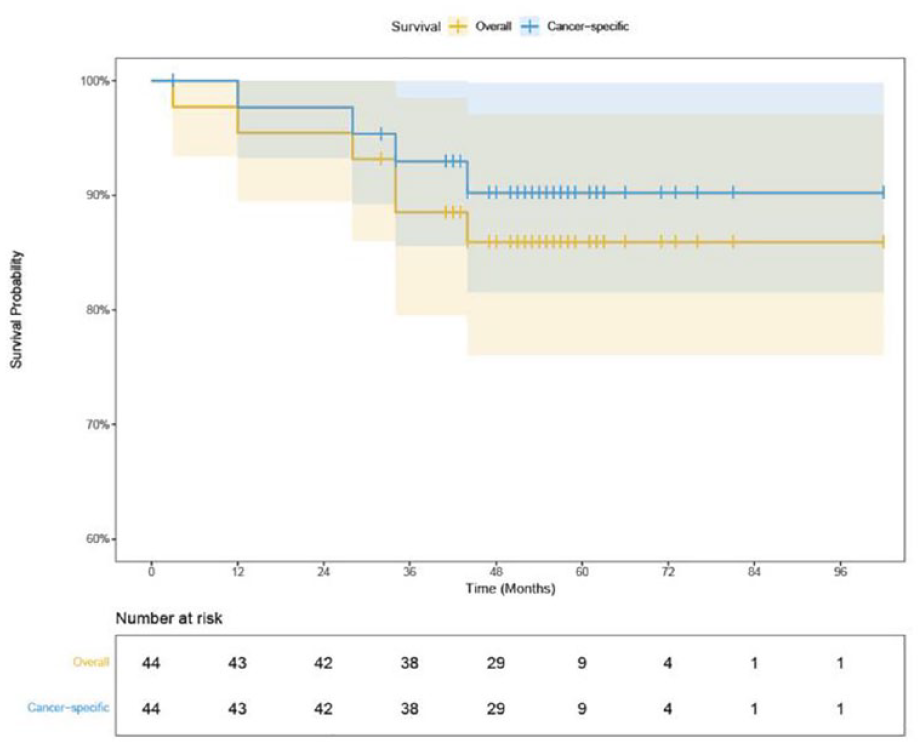
Objective: Previous studies have evaluated the feasibility of robotic-assisted thoracoscopic segmentectomy (RVATS) in comparison to video-assisted thoracoscopic segmentectomy (VATS). We report both short- and long-term outcomes comparing robotic-assisted and video-assisted segmentectomy at a single institution. Methods: This is a retrospective propensity matched cohort study reviewing robotic-assisted and video-assisted segmentectomy for primary non-small cell lung cancer performed from 2013 to 2021 at our institution. 1:2 propensity matching of patient’s age, gender, smoking status, pulmonary function, comorbidities, and clinical stage was performed. Results: There were 108 patients that underwent RVATS and 370 that underwent VATS for primary lung cancer. After propensity matching, we had two well matched cohorts of 102 patients in the RVATS group and 204 in the VATS group. Our data showed no significant difference in 90-day mortality (0 [0%] vs 3 [1.5%]; P = 0.55), 30-day hospital readmission rate (11 [10.8%] vs 14 [6.9%]; P = 0.25), or median number of lymph nodes (13 [IQR, 9-18] vs 12 [IQR, 7-16.5]; P = 0.15), between our RVATS and VATS groups respectively. There was also no significant difference in post-operative morbidity except for pleural effusion (12 [11.8%] vs 8 [3.9%]; P = 0.01) (Table T4-1). RVATS had significantly greater median number of lymph node stations harvested (5 [IQR, 4-6] vs 4 [IQR, 3-5]; P = 0.04), and longer operative time (252.5 mins [IQR, 206-296mins] vs 186.5mins [IQR, 148-263mins]; P < 0.0001). Although both groups achieved R0 resections in all patients, RVATS showed greater negative tumor margin distance compared to VATS (27mm [IQR, 20-40mm] vs 20mm [IQR, 11-30mm]; P < 0.0001). There was a trend towards shorter hospital length of stay for the RVATS group (4 days [IQR, 3-5 days] vs 4 days [IQR, 3-6 days]; P = 0.07). There was no significant difference in disease free survival (mean survival of 2.7 years [RVATS] vs 2.5 years [VATS]; P = 0.40), as well as overall survival (mean survival of 2.5 years [RVATS] vs 2.8 years [VATS]; P = 0.11) between the two groups at 3 years. Conclusions: In our experience, RVATS showed greater number of lymph node stations harvested, greater negative tumor margin distance, and a trend towards shorter hospital length of stay when compared to VATS, without compromising peri-operative and oncological outcomes for segmentectomy performed for non-small cell lung cancer.
T5
Robotic Assisted Right Upper Lobe Anterior Segmentectomy
Andrew R. Brownlee, MD, Justin J. Watson, MD, Shruthi Nammalwar, Amirhossein P. Mahfoozi, MD, Harmik J. Soukiasian. Cedars-Sinai Medical Center, Los angeles, CA, USA.
Objective: Pulmonary segmentectomy is an oncologically appropriate treatment for selected patients with non-small cell lung cancer. Right upper lobe anterior segmentectomy is technically challenging. Methods: In this video, we demonstrate the key surgical techniques to robotic right upper lobe anterior segmentectomy in a 73-year-old patient with a 1.2cm right upper lobe lung nodule. Preoperatively, imaging suggested that an anterior segmentectomy would be technically feasible with an adequate margin. Results: The patient underwent an uncomplicated robotic right upper lobe S3 segmentectomy. Her chest tube was removed on postoperative day 3 and she was discharged. Conclusions: Robotic right upper lobe anterior segmentectomy can be done safely, while observing oncologic principles.
T6
Outside the Cage (OTC) Subcostal RATS Lobectomy, Technical Aspects and Results of the First Series of a Novel Approach
Luciano Bulgarelli Maqueda, Pedro Guimarães Rocha Lima, Feras Abu-Reida, Omniyah Alashgar, Evangelos Koliakos, Maxime Têtu, Gabriel Dayan, Basil Nasir, Pasquale Ferraro, Moishe Liberman. Centre Hospitalier de l'Université de Montréal (CHUM), Montreal, QC, Canada.
Objective: The goal of minimally invasive surgery (MIS) is to reduce trauma to patients and improve their post-operative outcomes. The latest advances in MIS and robotic platforms are spreading worldwide the use of robotic assisted thoracic surgery (RATS) applied to the treatment of lung cancer. Major pulmonary resections were recently reported to be feasible through a single incision RATS with the objective of minimizing the surgical trauma of the traditional multi-portal RATS approach. Withal, both strategies require intercostal incisions potentially provoking immediate and chronic pain derived from intercostal nerves injury, with resulting consequences. Furthermore, major pulmonary resections have been reported feasible through subxiphoid and subcostal incisions with claims of lower postoperative pain compared to intercostal approaches.We used this data as an impetus to develop a non-intercostal outside the thoracic cage (OTC) approach for RATS lobectomy, avoiding intercostal instrumentation which could imply a positive impact in patients’ postoperative recovery. Herein we describe the technical aspects and results of the first reported series of OTC RATS lobectomies. Methods: Retrospective analysis of a series of OTC subcostal RATS lobectomy cases performed at CHUM for lung cancer treatment between August and December 2022. Results: A total of 10 cases were analyzed, the median age of the patients was 63yo [55-84], with a mean IMC of 29 [24-45], an ASA score II-III and a preoperative clinical stage I (≤cT2N0M0). Surgical procedures were uneventful with no conversions of the surgical technique. The mean operative time was 132.6 minutes [98-223], with a 25% decrease between the first and second half of the cases. The median length of stay was 2 days. Two patients with severe COPD experienced prolonged air leak requiring being discharged with Heimlich valves that were removed after in the follow up visits. There were no pain related complications or readmissions and no 30 day mortality was observed in the series. Conclusions: In our series, OTC RATS subcostal lobectomy was feasible and safe. This series served as pilot study for an undergoing phase I clinical trial to prospectively assess the safety of the technique as well as its actual clinical relevance.
T7
Comparing Subxiphoid Versus Intercostal Uniportal Video-Assisted Thoracoscopic Pulmonary Lobectomy - A United Kingdom Centre Experience
Jacie Jiaqi Law1, Karen Chien Lin Soh2, Pranav Kumar Santhosh2, Jeremy Chan3, Giuseppe Aresu4. 1Royal Victoria Hospital, Belfast, United Kingdom, 2University of Cambridge School of Clinical Medicine, Addenbrooke’s Hospital, Cambridge, United Kingdom, 3Bristol Heart Institute, Bristol, United Kingdom, 4Royal Papworth Hospital, Cambridge, United Kingdom.
Objective: Subxiphoid uniportal video-assisted thoracoscopic (SUVAT) lobectomy is a novel approach aimed to enhance recovery by reducing incisional pain after traditional intercostal uniportal video-assisted thoracoscopic (IUVAT) approach.However, evidence on SVAT remains scattered, especially in Europe and Americas. We aim to share our institutional experience with SUVAT lobectomy in the management of primary lung cancer and compare perioperative outcomes with IUVAT lobectomy to assess its safety and feasibility. Methods: Retrospective analysis of prospectively collected data identified 57 patients and 132 patients undergoing SUVAT and IUVAT lobectomy respectively. Data on patient characteristics and perioperative outcomes are presented as mean ± standard deviation. Comparison of continuous and categorical variables between groups was performed with Pearson’s Chi-suqared test, Fisher’s exact test and Wilcoxon rank sum test. Statistical significance was considered at P < 0.05. Results: Patient characteristics such as age (69.84±9.69, P = 0.39), BMI (26.34±4.42, P = 0.07), pulmonary function (FEV1/FVC 62.65±15.24%, P = 0.86 and TLCO 75.19±22.13%, P = 0.68) and ASA grade were similar between two groups. There was no difference in operating times (209±69 minutes vs 199±54 minutes, P = 0.42).Post-operatively, the SUVAT group experienced lower postoperative day 1 drainage volume (96±118ml vs 153±154ml, P < 0.001), shorter duration of chest drain use (3±4.6 days vs 5±4.6, P = 0.043) and reduced hospital length of stay (5±6.4 vs 6±14.3 days, P = 0.04). There was also no difference in R0 resection (P = 0.30), reoperation within 30 days (P = 0.56) and disease recurrence(P = 0.91). Conclusions: Our experience demonstrates that SUVAT lobectomy for primary lung cancer is safe and promising with similar perioperative outcomes and oncological resection results when compared to IUVAT lobectomy.
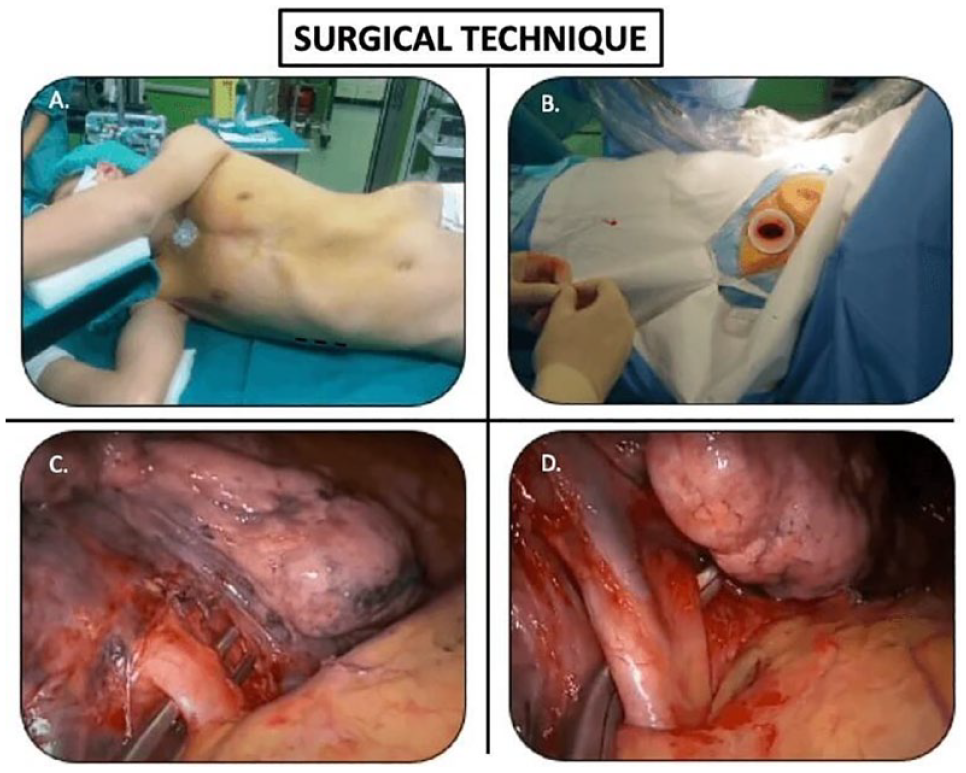
(A) shows the patient positioning and (B) the insertion of a subxiphoid wound retractor in SVAT Lobectomy.(C) demonstrates the dissection of the pulmonary artery and (D) an excellent view of the pulmonary vein.
T8
Locally Advanced: The Role of Robotic Approach
Elisa Sicolo1, Carmelina Cristina Zirafa2, Elena Bagala2, Gaetano Romano1, Federico Davini1, Franca Melfi1. 1Division of Thoracic Surgery, Department of Surgical Medical and Molecular pathology and Critical Area, University Hospital of Pisa, Italy, Pisa, Italy, 2Minimally invasive and robotic thoracic surgery, Robotic Multispecialty Center of Surgery, University Hospital of Pisa, Pisa, Pisa, Italy.
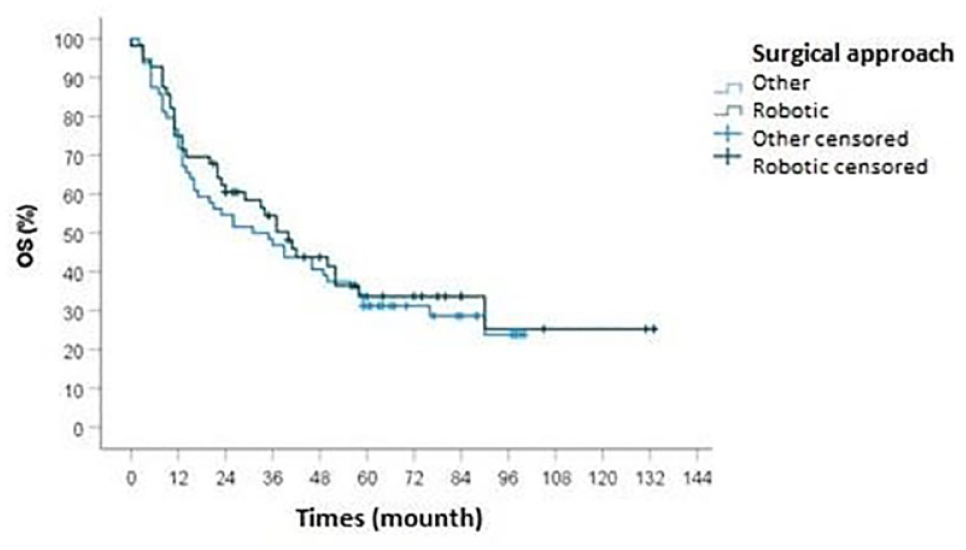
Objective: Locally advanced lung cancer includes a heterogenous group of patients depending on tumor dimension (T3-T4) and lymph node involvement (N1-N2). This study aims to evaluate the safety, feasibility and radicality of the use of robotic surgery to perform anatomic resection in locally advanced Non-Small Cell Lung Cancer (NSCLC). Methods: Data of 61 consecutive patients with locally advanced NSCLC (cIIIA-IIIB) who underwent robotic anatomic resection, from 2010 to 2021, has been analyzed and compared with data of 70 consecutive patients treated by thoracotomy. It was evaluated operative, post-operative and oncologic results. Results: In robotic group, there were 61 patients with a median age of 67.33 years (range 32-80), with a median operative time of 256 minutes (range 120-440) and a median postoperative hospital stay of 7 days (range 2-27). Post-operative complications occurred in 28 patients (45.9%).The open group included of 70 patients with a median age of 69.44 years (range 48-82), with a median operative time of 131 minutes (range 60-235), and a median postoperative hospital stay of 9 days (range 4-48). Post-operative complications were verified in 36 patients (51.4%). Analyzing oncologic outcomes of the robotic group, loco-regional recurrence was observed in 29 patients (47.5%), distant metastases in 37 patients (60.6%); the 5-year OS was 34% (Fig. T8-1). In the open group, loco-regional recurrence was detected in 30 patients (42.8%), distant metastases in 41 patients (58.6%); the 5-year OS was 31% (Fig. T8-1).No statistically significant differences were observed in terms of postoperative complications and oncological results. Conclusions: Our experience confirms that the robotic approach is safe and feasible in terms of postoperative mortality and incidence of complications, when performed by skilled surgeons.The long term oncological outcomes are in line with the most consistent open surgery results, confirming that robotic approach is associated with oncological radicality.
Overall survival.
T9
Robotic Right Middle Sleeve Lobectomy for Endobronchial Carcinoid Tumor
John K. Sadeghi, MD, Charles T. Bakhos, MD, MBA, MS. Temple University Health System, Philadelphia, PA, USA.
Objective: Lung cancer with endobronchial involvement in proximity to the mainstem bronchi historically required pneumonectomies, open sleeve lobectomies, or VATS sleeve lobectomies. In the past, the threshold for pneumonectomy was low for cancer abutted the central airways. The robotic platform provides an easier approach to these lesions and raises the threshold for a pneumonectomy. Here, we share the crucial components to our standardized technique of performing a robotic sleeve lobectomy (RSL) for cancer. Methods: A 45-year-old man with a 15-pack year smoking history presented with complete atelectasis of his right middle lobe. He was taken for a bronchoscopy which showed an obstructing lesion of the RML bronchus. The lesion was biopsied, and laser ablated. Pathology showed a carcinoid tumor. The lesion was PET avid and stations 4R and 7 were negative on EBUS biopsy. He was taken to the operating room for a robotic right middle sleeve lobectomy. In this video we highlight the technique of anastomosing the remaining bronchi with barbed absorbable suture. Post-operatively, the patient did well and was discharged from the hospital after 3 days. He did not have any complications from the procedure and was in good health on follow-up. Final pathology showed negative margins and a positive level 8 lymph node. Results: Key steps of the entire procedure include utilization of 4 robotic arms, completion of the fissures, proximal and distal mobilization of the airway segment of the planned sleeve resection, negative margins on frozen pathology prior to the anastomosis, stay sutures to approximate the ends of the airway, running 2 unidirectional barbed absorbable sutures starting at the cartilaginous side, coverage with a tissue flap, and extubation in the OR. Conclusions: RSL for lung cancer is technically safe and feasible. It presents many advantages over open and VATS sleeves, namely the angulating wrist motion and 3-D magnification paired with running two barbed absorbable sutures. RSL may be the optimal approach to lesions that are near the main bronchi to best preserve patients’ lung functions.
T10
Robotic Left Upper Lobectomy Post Induction Immuno-Chemotherapy
Justin Watson, MD, Andrew Brownlee, MD, Shruthi Nammalwar, MD, Harmik Soukiasian, MD. Cedars Sinai Medical Center, Beverly Hills, CA, USA.
Objective: To demonstrate a robotic left upper lobe lobectomy surgical technique post immunotherapy and chemotherapy induction. Methods: In this video we demonstrate the key technical aspects of a patient undergoing a robotic left upper lobectomy who had preoperative induction immunotherapy and chemotherapy for Stage IIIA lung adenocarcinoma. Results: Findings and operative techniques as narrated in the video. Conclusions: Robotic left upper lobectomy can be safely performed in patients with induction immunotherapy and chemotherapy. Patients appear to have slightly stiffer parenchyma and significantly enlarged lymph nodes encountered during dissection.
T11
Starfish Success: Thoracic Tumour Resection With Novel Use of Starfish Heart Positioner
Lauren Bidois, MBChB, Harsh Singh. Christchurch Hospital, Christchurch, New Zealand.
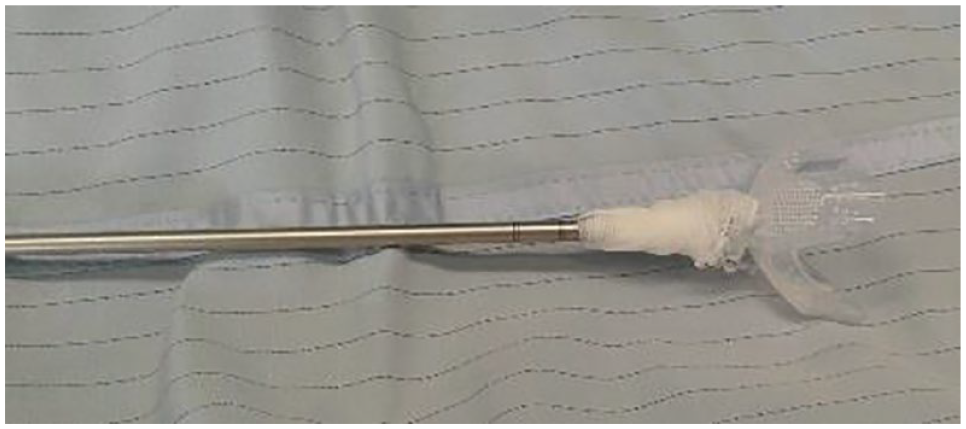
Objective: Adequate visualisation within the hemithorax is a vital component of successful video-assisted thoracoscopic surgery (VATS), allowing for complete tumour resection and to reduce risk of conversion to open thoracotomy. Additionally, the ability to manipulate tissues in order to provide this ample visualisation is paramount. In VATS, this tissue mobility is already hampered by the limited angles afforded by the intercostal spaces, and this in combination with a large tumour (>5cm) can mean standard VATS graspers may not lend themselves to a quick and technically easy operation. We present a successful case of using an improvised suction instrument to improve visualisation and tissue manipulation. Methods: A Starfish Heart Positioner was combined with thoracoscopic suction in a novel manner to retract and excise a 58x44x54mm fibrous pleural tumour in a 49-year-old patient. Results: We had an excellent surgical resection result and a significant reduction in operating time, due to enhanced visualisation and mobility afforded by our instrument. Conclusions: The Starfish Heart Positioner in combination with thoracoscopic suction is a viable grasping and retraction instrument for use in VATS tumour excision, however, further assessment is required before using it on other tissues within the thorax.
Starfish Heart Positioner combined with thoracoscopic suction.
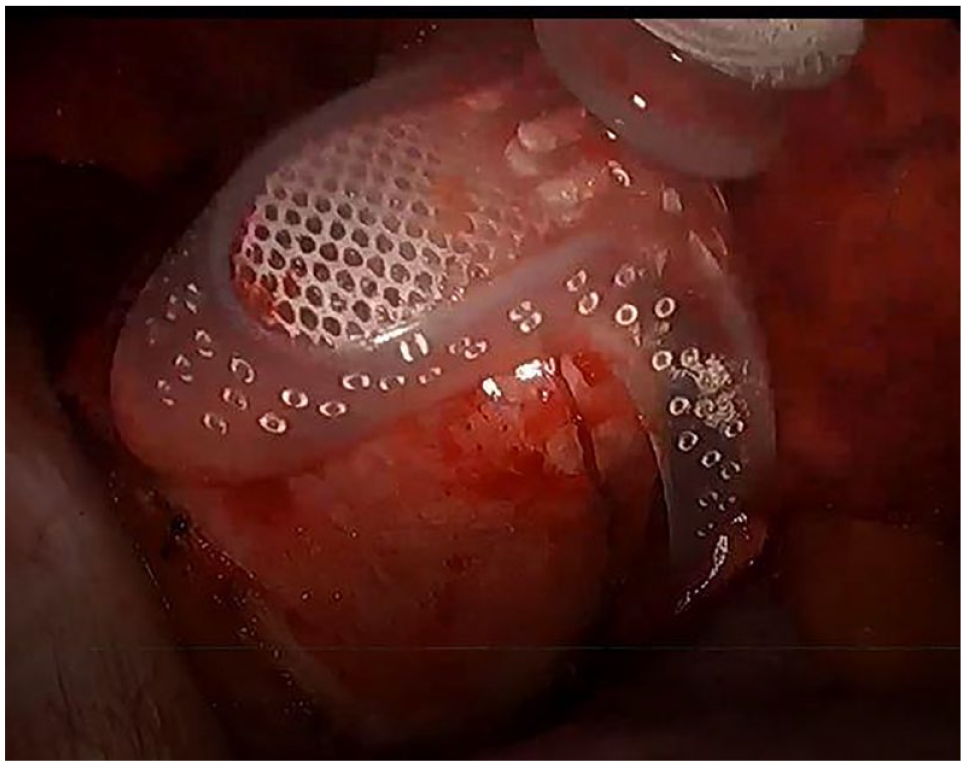
Intra-operative view of improvised starfish suction instrument in use to retract a large thoracic tumour.
T12
Prediction of the Course of Air Leaks After Pulmonary Lobectomy Using Continuous Flow Data
Kwanyong Hyun1, Gongmin Rim1, Sook Whan Sung2, Deog Gon Cho3. 1Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea, Republic of, 2Ewha Womens University Seoul Hospital, Seoul, Korea, Republic of, 3St. Vincent's Hospital, The Catholic University of Korea, Suwon, Korea, Republic of.
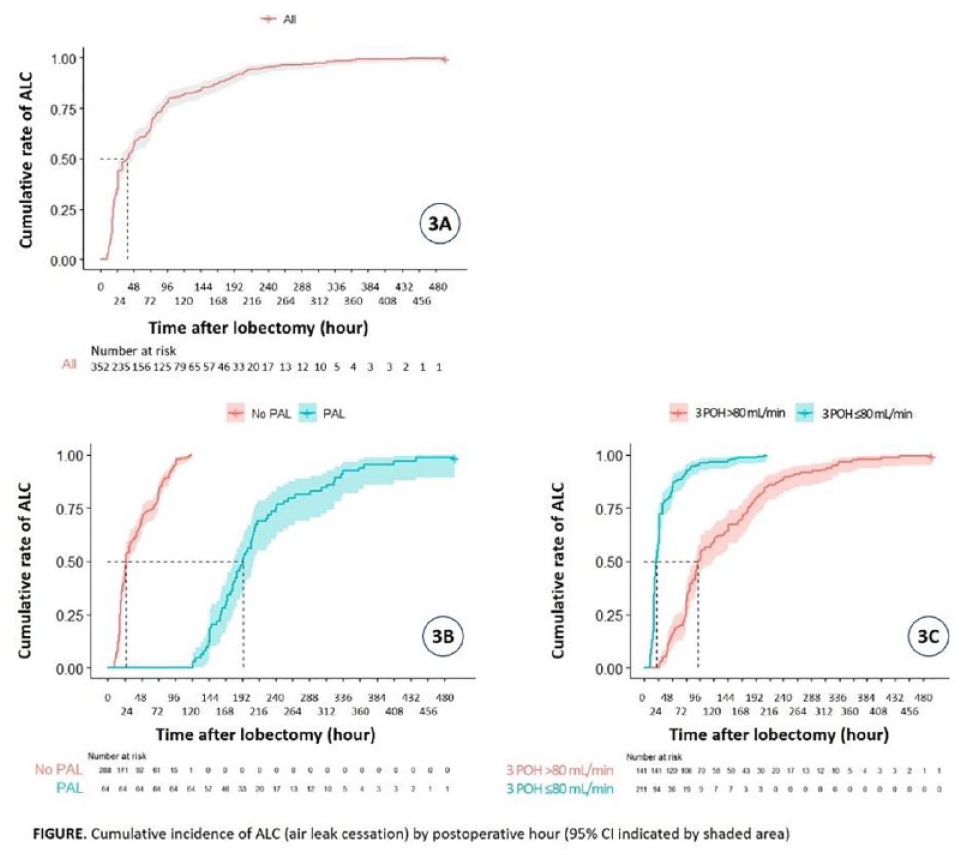
Objective: The assessment for a degree of air leak has been conducted by the subjective analysis of air bubble and this leads to the difficulty for using air leak as an evaluation factor. The aim of this study was to extract predictive factors of prolonged air leak (PAL) and air leak cessation (ALC) including air flow data as objective parameter by digital drainage system. Methods: 352 patients who underwent lung lobectomy and had flow records were reviewed. The flow data were extracted at a designated interval (1, 2, and 3 postoperative hours (POH), then 3 times a day thereafter (06AM, 13PM, 19PM)). ALC was determined to be less than 20 mL/min for the past 12 hours and PAL was defined having ALC after 5 days. Using Kaplan-Meier estimate of time to ALC, cumulative incidence curves were obtained. Cox regression analysis were performed to determine the effect of variables on the rates of ALC. Results: Incidence of PAL was 18.2% (64/352). By ROC curve analysis, a cut-off value was set at 180 mL/min for 3 POH flow and 73.3 mL/min for 1 POD flow, having the sensitivity and specificity of 88.9% and 82.5%, respectively. The rates of ALC were 56.8% at 48 POH and 65.6% at 72 POH by Kaplan-Meier analysis. Multivariate Cox regression analysis revealed 3 POH flow (≤80 mL/min), operation time (≤220 min), and RML lobectomy independently predicted ALC. Conclusions: The air flow measured by digital drainage system will be useful predictors of PAL and ALC, which may provide optimization of hospital course.
Cumulative incidence of ALC (air leak cessation) by postoperative hour (95% CI indicated by shaded area).
T13
Thymectomy: Does the Robotic Approach Improve Outcomes for Non-Thymomatous Myasthenia Gravis Patients?
Zhuoran Yao1, John K. Waters2, Hellen Chiou3, Allante Milsap1, Rachel Hurst4, Michael A. Wait2, Scott I. Reznik2, Michael E. Jessen2, Shaida Khan5, Steven Vernino5, Kemp H. Kernstine2. 1The University of Texas Southwestern Medical School, Dallas, TX, USA, 2Department of Cardiovascular and Thoracic Surgery, The University of Texas Southwestern Medical Center, Dallas, TX, USA, 3Department of Surgery, Rutgers Robert Wood Johnson Medical School, New Brunswick, NJ, USA, 4Department of Emergency Medicine, The Medical College of Wisconsin, Milwaukee, WI, USA, 5Department of Neurology, The University of Texas Southwestern Medical Center, Dallas, TX, USA.
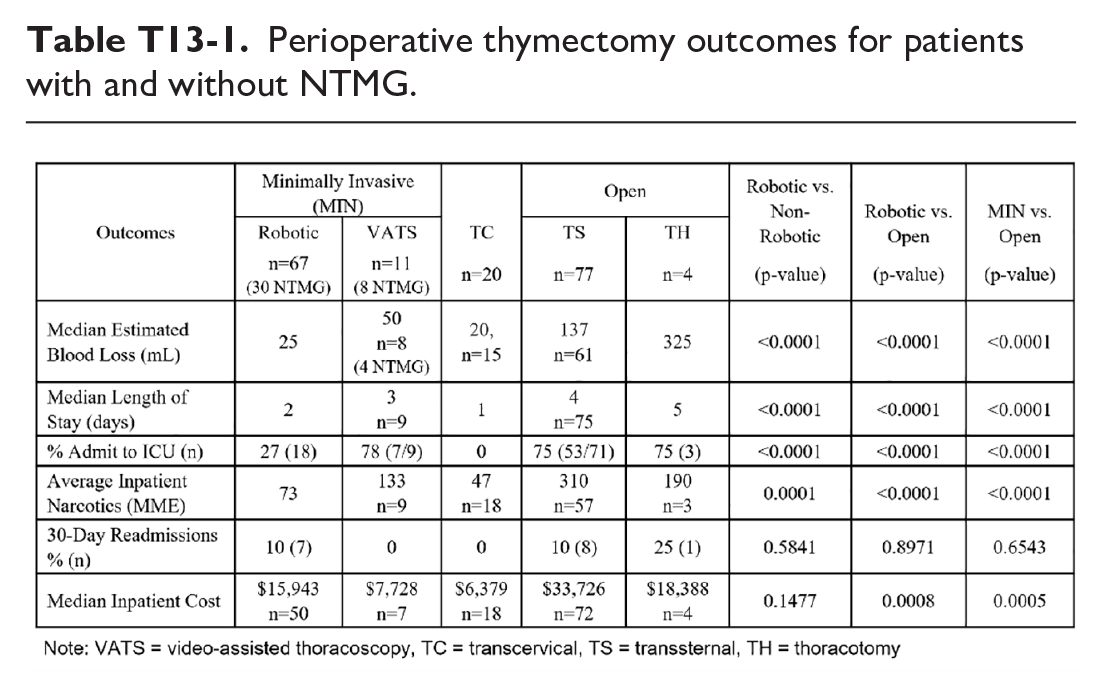
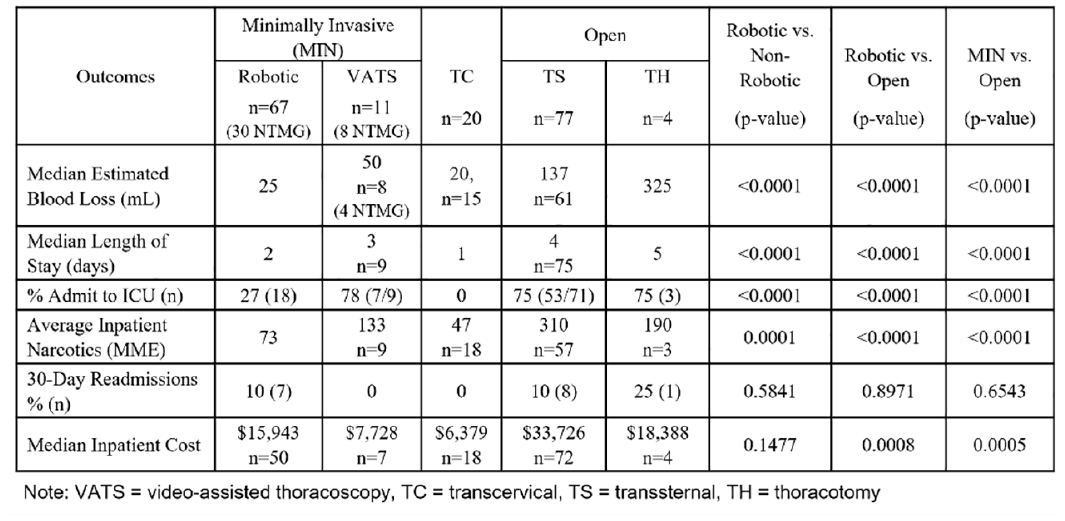
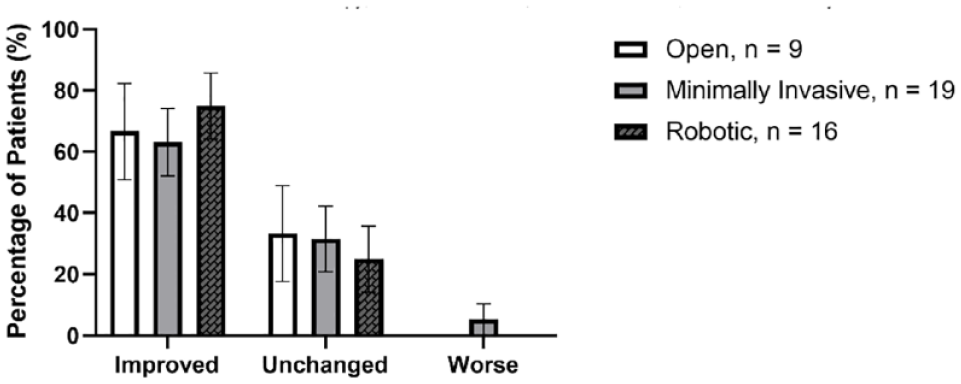
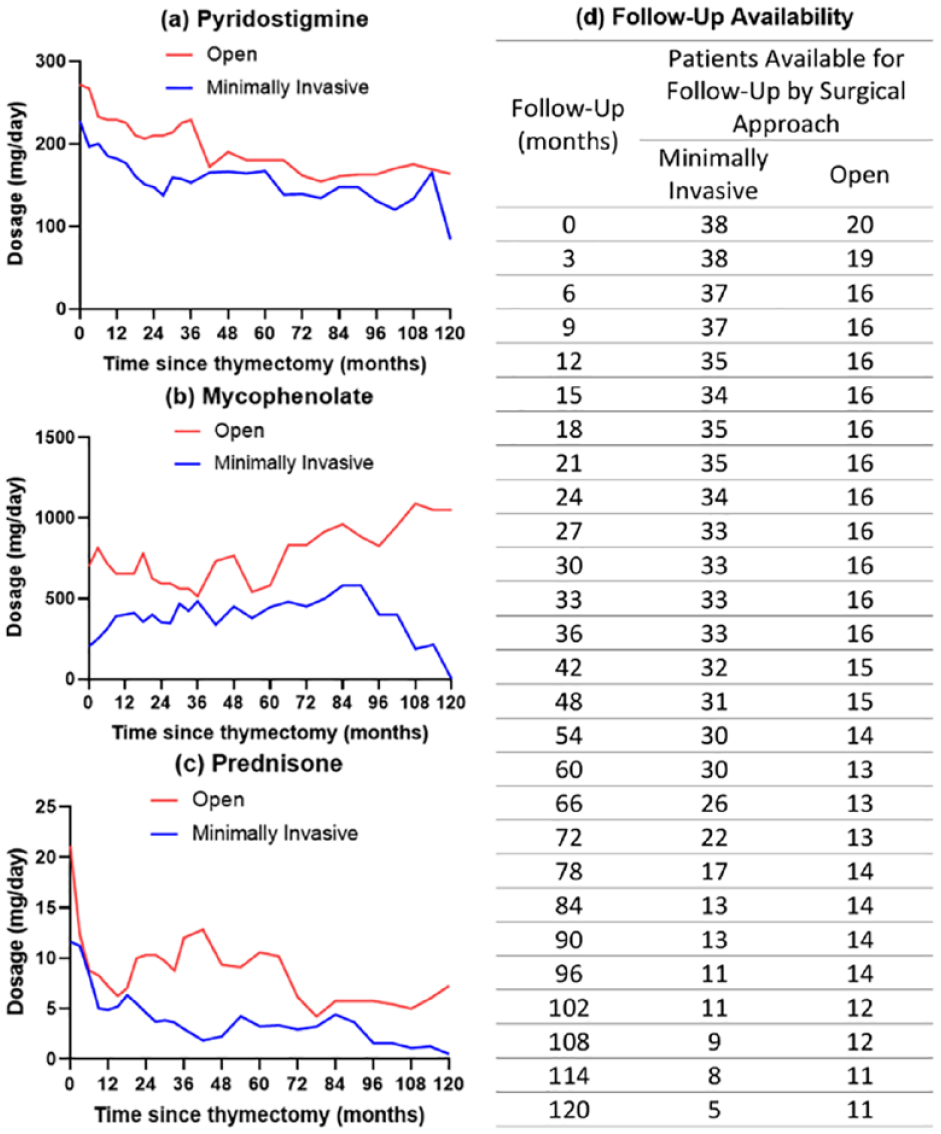
Objective: Thymectomy has significantly altered the course of myasthenia gravis (MG). Few long-term outcomes have been reported for minimally invasive, especially robotic, thymectomy in treating non-thymomatous myasthenia gravis (NTMG). This study aimed to compare the outcomes of robotic (minimally invasive overall) vs. non-minimally invasive thymectomies for NTMG patients. Methods: A retrospective, IRB-approved single-institution review of thymectomies between 1/1/2006 and 6/21/2017 compared the indications, demographics, clinical data, outcomes, and hospital costs for different approaches. Long-term outcomes were assessed and managed by our neurologists. Perioperative outcomes were analyzed for all cases, with long-term outcomes evaluated for NTMG patients. MGFA post-intervention status (MGFA-PIS) was tracked postoperatively to assess long-term symptomatic changes. Pyridostigmine, mycophenolate, and prednisone requirements were followed for up to 10 years. There was no protocol for weaning medications. Chi-squared and Fisher's exact tests were used for categorical variables and two-tailed t and Mann-Whitney U tests for continuous variables with a threshold of P < 0.05. Results: In 179 thymectomies (32% NTMG), the mean patient age was 47 years [14-82]. The patients were 64% female and 47% white. The thymectomies were 43% transsternal, 8% thoracoscopic, 11% transcervical, and 38% robotic. Compared to the 81 patients who underwent open thymectomies, those undergoing robotic thymectomies experienced 83% less blood loss (P < 0.0001), 76% lower inpatient narcotic usage (P < 0.0001), 48% lower ICU admission rates (P < 0.0001), and 50% shorter hospital stay (P < 0.0001), as shown in Table T13-1. Robotic thymectomies cost 53% less than transsternal ones (P = 0.02). Preoperatively, in the 58 NTMG patients, 38% had MG for >24 months and 7% for <6 months. The median follow-up was 78 months [3-120]. Two recipients of robotic thymectomy (7%) and two of transsternal thymectomy (7%) achieved complete remission. There were no significant differences in long-term MG outcomes between minimally invasive (robotic & VATS) and open (transsternal) approaches in terms of changes in MGFA-PIS (Fig. T13-1) and MG medication requirements (Fig. T13-2). Conclusions: For NTMG, robotic thymectomy is associated with reduced perioperative blood loss, duration of stay, ICU admission, inpatient narcotic use, and inpatient costs without compromising long-term benefits when compared to non-minimally invasive approaches. To confirm these findings, a prospective trial is warranted.
Perioperative thymectomy outcomes for patients with and without NTMG.
Changes in MGFA post-intervention status (MGFA-PIS) of NTMG patients at 3-year follow-up.
Mean NTMG pharmacotherapy requirements followed over 10 years.
T14
Outcomes of Robotic Assisted Anterior Mediastinal Resections for Large Primary Thymic Tumors: A Single Institution Experience
Abigail Fong, Inderpal Sarkaria, Nicholas Baker, Neil Christie, Rajeev Dhupar, Ryan M. Levy, Omar Awais, Tadeusz Witek, Alicuben T. Evan, James D. Luketich, Arjun Pennathur, Matthew Schuchert. UPMC, Pittsburgh, PA, USA.
Objective: This study seeks to describe our large series of robotic mediastinal resections and investigate the safety and efficacy of this surgical modality in both small and large primary thymic malignancies. Methods: A retrospective review was performed of robotic assisted anterior mediastinal resections in our institution from 2014-2022. Data was gathered on these patients including demographics and perioperative outcomes. Data was stratified by pathologic diagnosis and a group of primary thymic malignancies was identified and outcomes compared by tumor size. Statistical analysis was performed using chi-squared, fisher exact test and T-tests to compare samples as appropriate. Results: 234 robotic assisted anterior mediastinal resections were performed during the time frame of the study. Of these, 130 (56%) were performed for benign disease, 104 (44%) for malignant disease. The most common malignant diagnoses were thymoma (61, 26%), metastatic disease (14, 6%), lymphoma (9, 3.8%) and thymic squamous cell carcinoma (6, 2.6%). The overall median length of stay was 2 days, and median operative time was 178 minutes. 66 were found to be primary thymic malignancies. Of these, the average tumor size was 5.6cm, median hospital stay was 3 days and median operative time was 186 minutes. When comparing our primary thymic malignancies larger than 4cm (44,67%) vs =<4cm (22, 33%), those >4cm were found to have a longer average operative time (227 vs 172 minutes, P = 0.04), but no difference in average length of stay (6.9 days vs 5.5 days, P = 0.69) or Clavien-Dindo grade III-V complication rate (3 grade III/IV vs 1 grade III/IV and 1 grade V, P = 0.18). In the >4cm primary thymic malignancy group 39 (89%) R0 resections were seen, compared to 22 (100%) R0 resections in the =<4cm group (P = 0.15), showing no significant difference. Of note 16 of the thymic malignancy group ranged in size from 7-14cm with negative margins. Conclusions: Robotic mediastinal resections can be safe and effective, even in large primary thymic malignancies > 7cm, although some concern regarding greater rates of margin positivity in these tumors remains. Further work is necessary to identify factors potentially predicting positive margins in these patients.
T15
Combined Cervicotomy and Robotic-Assisted Surgical Approach for Intrathoracic Thyroid Goiter: A Case Series
Giorgia Piccioni, Alessandra Siciliani, Fabiana Messa, Paolo Mercantini, Erino Angelo Rendina, Mohsen Ibrahim. Sapienza University of Rome - Sant'Andrea Hospital, Rome, Italy.
Objective: Goiter is a benign pathological condition of the thyroid gland, characterized by slow growth rate, occasionally reaching the mediastinum and extending through the thoracic inlet. In most cases, retrosternal goiters originate from the cervical portion of the thyroid. Most frequently, goiters are found in the superior mediastinum. In this case, a complete thyroidectomy could be guaranted through a cervical approach. Extension of the goiter into the anterior mediastinum is less common. In these patients, a single cervical approach could not lead to a radical excission of the mediastinal mass. Transcervical approach to intrathoracic thyroid goiters can be difficult, often necessitating a thoracotomy or sternotomy access. Methods: This series describes the cases of five patients, affected by thyroid goiter extended into the anterior (n = 3) and posterior (n = 2) mediastinium, who underwent combined cervicotomy and robotic-assisted surgery. The masses presented a polylobulated morphology, and extended until the peritracheal area, contracting close contiguous relationships with the surrounding vascular or tracheal tissue structures. In each case, the thoracic and mediastinal portion of the goiter was approached with robot-assisted minimally invasive surgical techniques. Left or right triportal incisions, according to the predominance of the laterality of the mass (respectively at the 5th intercostal space along the anterior axillary line, at the 3rd intercostal space along the mid-axillary line and at the 5th intercostal space along the midclavicular line) were used to gain access to the mediastinum via the homolateral pleural cavity. Total thyroidectomy was then completed using the cervical approach. Results: The procedure was well tollerated, with minimal intraoperative blood loss. The postoperative course was characterized by the absence of complications, without symptoms of dyspnoea or dysphonia. Patients were discharged after a short hospital stay (3-5 days). The pleural and cervical drainage tubes were removed on discharge. Conclusions: Combined Cervicotomy and Robotic assisted technique for surgical excission of intrathoracic thyroid goiter, is a feasible and safe procedure. This surgical approach avoid the use of invasive surgical access such as thoracotomy and sternotomy, with a positive impact on the onset of postoperative complications, reducing postoperative pain and lenght of stay.
T16
Primary Exploration of Tubeless Robot-Assisted Thymectomy for Myasthenia Gravis
Minghui Zhu1, Yujun Lian2, Jinglong Li1, Dazhi Pang1, Rutaiyang Liu1, Yanan Liang1, Zhihai Liu1, Guangqiang Shao1, Jianguo Lu1, Jitian Zhang1. 1Department of Thoracic Surgery, The University of Hong Kong-Shenzhen hospital, Shenzhen, China, 2Department of Anesthesiology, The University of Hong Kong-Shenzhen hospital, Shenzhen, China.
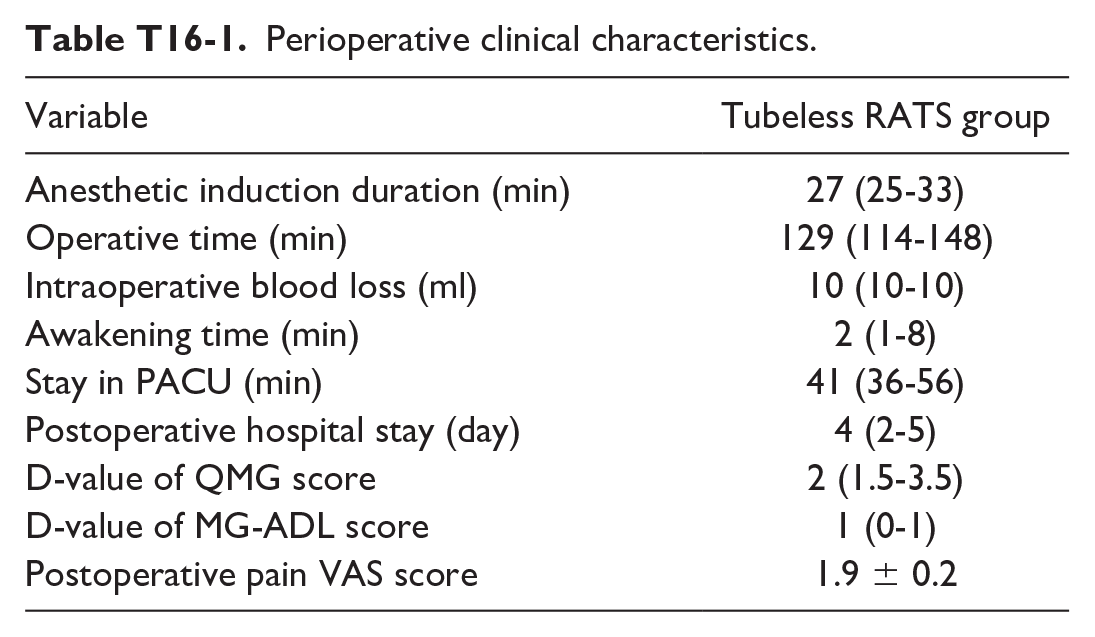
Objective: In order to accelerate recovery of myasthenia gravis (MG) patients, and avoid the adverse effects of muscle relaxants on them, we explored and evaluated a new tubeless (general anesthesia without endotracheal intubation, urinary catheterization and thoracic drainage tube) approach to perform robot-assisted thoracoscopic thymectomy for MG. Methods: The clinical characteristics of 13 patients who were diagnosed as MG and underwent a tubeless RATS thymectomy in our center from February 2022 to September 2022 were collected. All included patients were required these criterias:16-60 years old, American Society of Anesthesiologists (ASA) grade ≤ II, no history of thoracic surgery and no coexisting urinary diseases, etc. Results: All patients (Myasthenia Gravis Foundation of America (MGFA) Classification I:4, II A:1, II B:2, III A:1 and III B:5, median [interquartile range] age: 25[19-40] years old) underwent operation uneventfully without muscle relaxants, tracheal intubation, urinary catheterization and thoracic drain. No significant complications were seen, and none of them converted to a median thoracotomy approach intraoperatively. The anesthesia and operating time were 27[25-33] and 129[114-148] min, respectively. The blood loss was 10[10-10] ml. The awakening time was 2[1-8] min and the Post-anesthesia Care Unit (PACU) stay time was 41[36-56] min. None of patients complained of significant pain and the pain Visual Analog Scale (VAS) scores were 1.9 ± 0.2, 1.8 ± 0.1, and 1.8 ± 0.1 on the operative day, 1st postoperative day and 2nd postoperative day, respectively. The difference value in Quantitative Myasthenia Gravis (QMG) scores between the preoperative and 2nd postoperative day was 2[1.5-3.5], and the one in Myasthenia Gravis-Activities of Daily Living (MG-ADL) scores was 1[0-1]. All patients had no need for chest drainage in general ward and they were discharged on the 2nd-6th day (postoperative hospitalization was 4[2-5] days) respectively after surgery. Conclusions: The tubeless RATS thymectomy for MG is feasible in partial selected patients. Muscle relaxants, tracheal intubation, urinary catheterization and thoracic drain are not crucial in all MG cases.
Perioperative clinical characteristics.
Variable
Tubeless RATS group
Anesthetic induction duration (min)
27 (25-33)
Operative time (min)
129 (114-148)
Intraoperative blood loss (ml)
10 (10-10)
Awakening time (min)
2 (1-8)
Stay in PACU (min)
41 (36-56)
Postoperative hospital stay (day)
4 (2-5)
D-value of QMG score
2 (1.5-3.5)
D-value of MG-ADL score
1 (0-1)
Postoperative pain VAS score
1.9 ± 0.2
T17
Prediction of Smooth Non-Intubated Thoracoscopic Lobectomy Through Pulmonary Function Test Values
Kwanyong Hyun1, Gongmin Rim1, Sook Whan Sung2. 1Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea, Republic of, 2Ewha Womens University Seoul Hospital, Seoul, Korea, Republic of.
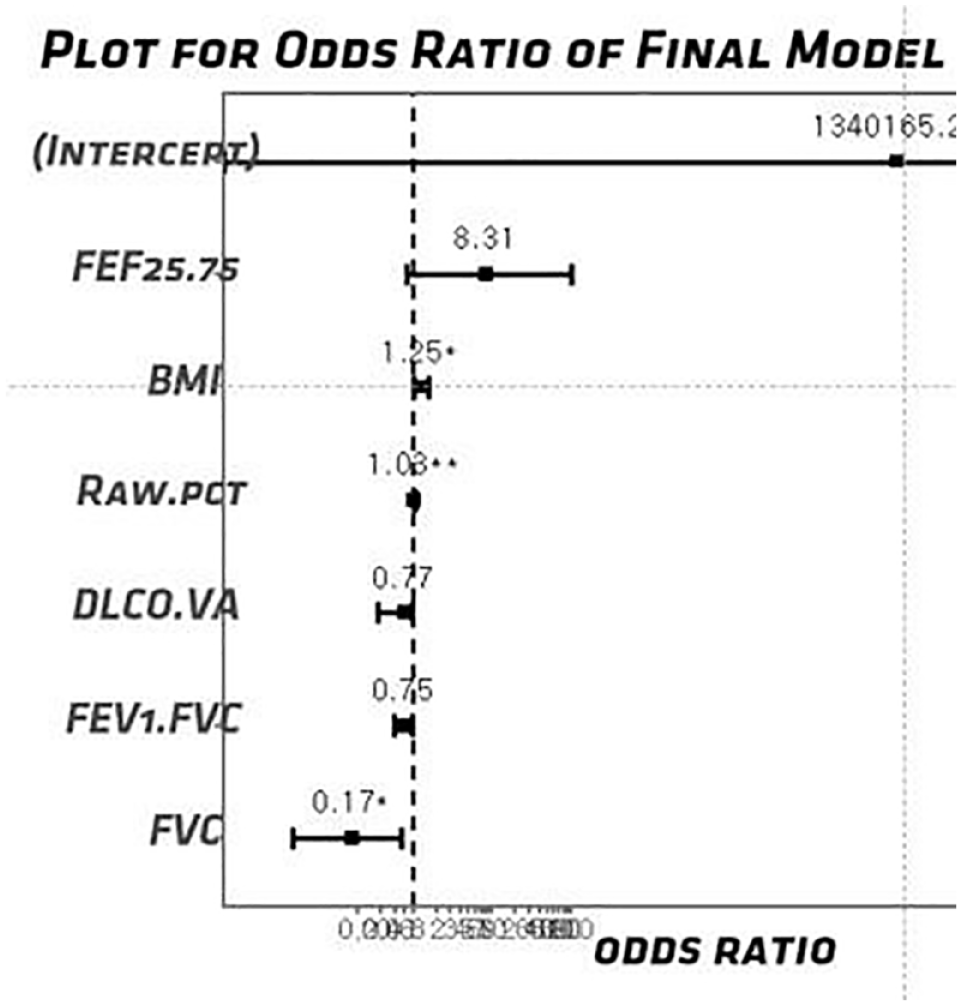
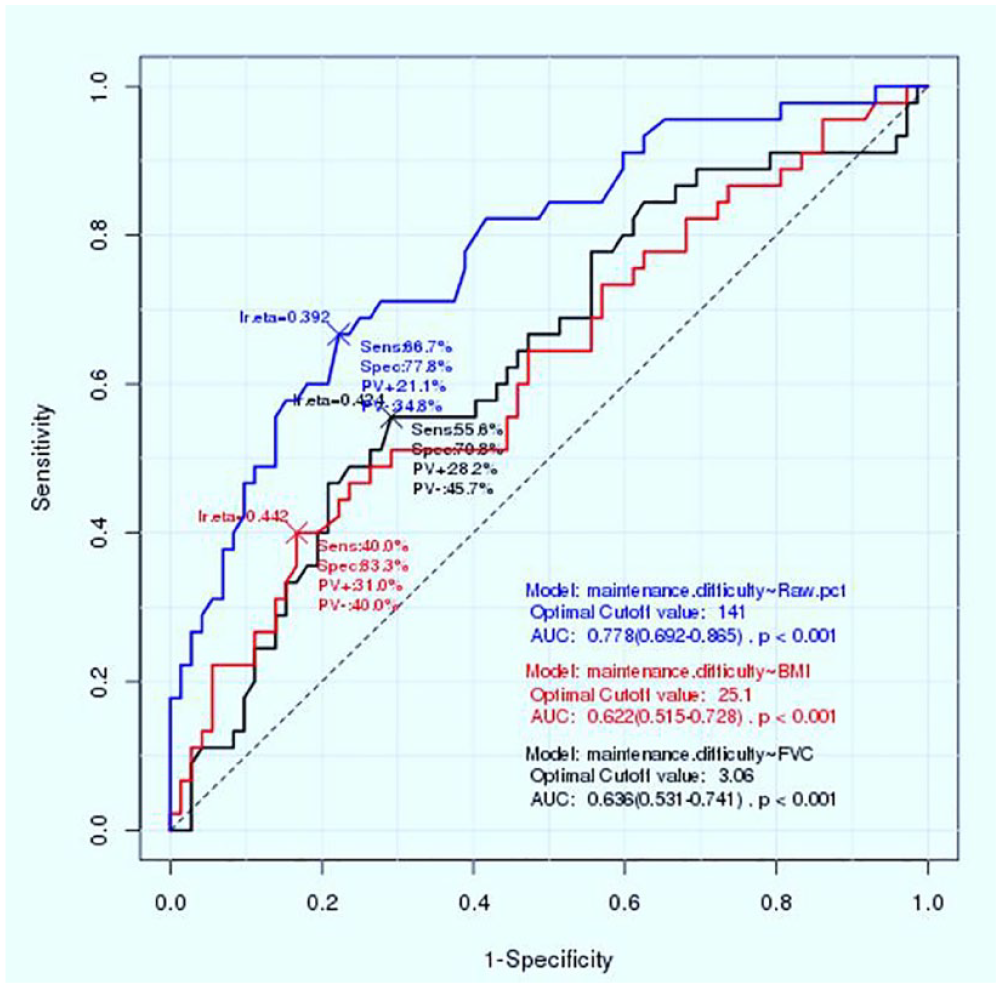
Objective: We investigated the safety of non-intubated thoracoscopic lobectomy and patient factors vulnerable to non-intubated stress. Methods: A total of 126 patients were electively operated with non-intubated thoracoscopic lobectomy from August 2016 to May 2018. 117 patients were analyzed after exclusions (insufficient pulmonary function test data, conversion to tracheal intubation due to pleural adhesions). Pulmonary airflow disturbances were investigated with pulmonary function tests (PFT). Group V (vulnerable to non-intubated stress) included patients with unstable pulmonary gas exchange of a mean SpO2<95% and mean EtCO2>50, and in-danger patients with vigorous (significant) diaphragmatic and mediastinal movement that could hamper subsequent operative procedure. Results: The mean BMI of all patients was 23.6 with a mean operation time and hospital stay of 142 minutes and 6.6 days, respectively. 45 patients (38%) were classified to group V and 72 patients (62%) were classified to group NV (non-vulnerable to non-intubated stress). Group V showed a significant higher mean EtCO2 and a lower mean SpO2 during the one-lung ventilation when compared to group NV (45.3 vs 48.3, P = 0.021; 100 vs. 97.6%, P = 0.000). Four patients (3.4%) required conversion to tracheal intubation and all these patients were from group V. In multivariable analysis using clinical factors, group V is predicted by the presence of high BMI, low FVC and high airway resistance (Raw) (Fig. T17-1). The optimal cutoff value of BMI, FVC and Raw for predicting group V were 25.1, 3.06L, and 141%, respectively by ROC curve analysis (Fig. T17-2). Conclusions: Our results support a policy of non-intubated procedure on thoracoscopic lobectomy in highly selected patients. We believe that more caution should be taken in doing non-intubated one-lung ventilation for patients with low functional reserve and high airway resistance.
Forest Plot for predictors of non-intubated stress.
ROC Curve Analysis for predictors of non-intubated stress.
T18
The Modified Collard-Orringer Anastomosis for Thoracoscopic Robotic-Assisted Ivor Lewis Esophagectomy
Matthew Inra, MD, Subroto Paul, MD. Lenox Hill Hospital, New York, NY, USA.
Objective: The purpose of this video is to show a successful, reproducible technique for intrathoracic esophagogastric anastomosis for minimally invasive robotic-assisted Ivor Lewis esophagectomy. Methods: Intraoperative video is used to show the steps of the anastomosis. Results: The video shows a completed thoracoscopic robotic-assisted intrathoracic esophagogastric anastomosis using the technique that was first described by Collard and colleagues and was later modified by Orringer and colleagues. Conclusions: This anastomotic technique is well described for open transthoracic esophagectomy and is translatable and reproducible for the thoracoscopic robotic-assisted approach.
T19
Robotic-Assisted Ivor Lewis Esophagectomy With Totally Robotic Intrathoracic/Intracorporeal Anastomosis
Matthew D. Stanley, MD, Manu S. Sancheti, MD. Emory University, Atlanta, GA, USA.
Objective: The rapid adoption of robotic-assisted thoracic surgery has led to increased interest in totally robotic-assisted procedures. Previously, robotic-assisted Ivor Lewis esophagectomy required the creation of a mini-thoracotomy and introduction of thoracoscopic instrumentation and staplers. Methods: We present a totally robotic-assisted Ivor Lewis esophagectomy with intrathoracic anastomosis creation and intracorporeal suturing. Results: After positioning in the left lateral decubitus position, five ports are placed (four robotic and one assistant) in standard fashion. After complete mobilization, the esophagus is divided proximally at the level of the azygos vein using a robotic-assisted stapler. Next, the conduit and specimen are delivered into the chest ensuring to maintain the correct orientation. Completion of the conduit is accomplished using a robotic-assisted stapler and the specimen can be removed from the thoracic cavity. The proximal esophageal staple line is removed using robotic-assisted monopolar scissors and can be sent as a proximal margin. After gastrostomy creation, a robotic-assisted stapler is used to create a side-to-side, functional end-to-end gastroesophageal anastomosis. Two corner retraction sutures are placed at the lateral edges of the common anterior opening to facilitate intracorporeal suturing. The nasogastric tube is passed distally, and the anterior common opening is closed in two-layers using barbed suture. The corner retraction sutures are tied, and any gaps can be filled with interrupted sutures. Finally, the integrity of the anastomosis is checked with an air leak test. Conclusions: We demonstrate a safe, efficient and reproducible method for creation of an totally robotic-assisted Ivor Lewis esophagogastric anastomosis.
T20
National Trends in Operative Approach to Esophagectomy: Utilization Rates, Disparities and Overall Survival
Akbarshakh Akhmerov, Andrew R. Brownlee, Justin Watson, Shruthi Nammalwar, Amirhossein Mahfoozi, Harmik Soukiasian. Cedars-Sinai Medical Center, Los angeles, CA, USA.
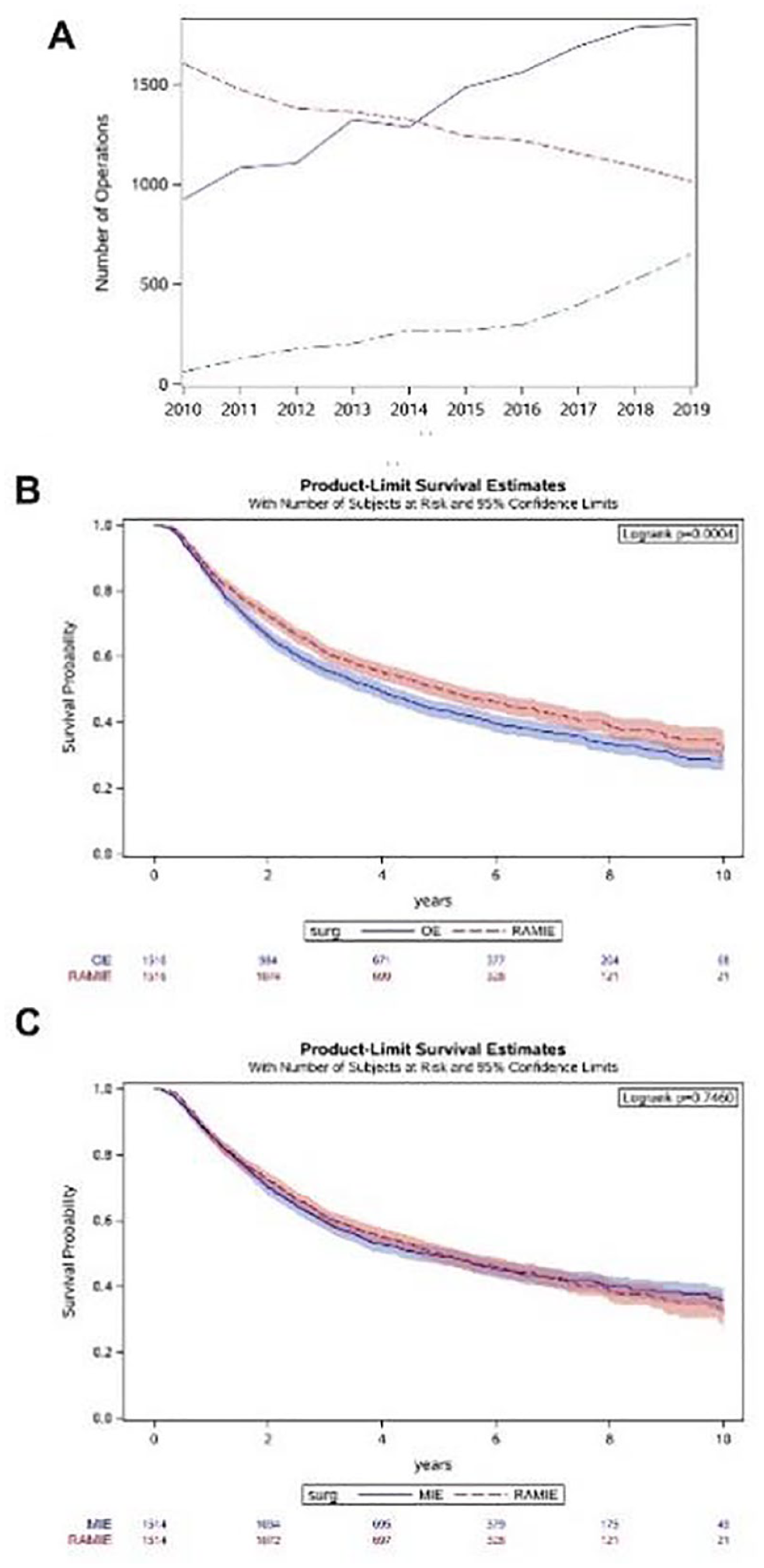
Objective: Although open esophagectomies (OE) have traditionally been favored, minimally invasive approaches are increasingly utilized and associated with improved outcomes. We investigated the adoption rates of robotic-assisted minimally invasive esophagectomy (RAMIE) and minimally invasive esophagectomy (MIE) compared with OE. Factors impacting the surgical approach, perioperative outcomes, and overall survival were analyzed. Methods: The NCDB was queried for patients who underwent OE, MIE, and RAMIE for esophageal cancer from 2010-2020. Adoption rates of RAMIE, MIE and OE were determined for all patients. Patients with primary cervical esophageal cancer, stage 4 disease, unknown staging, or missing 30-day follow-up data were excluded. Propensity matched cohorts were created for each surgical approach and compared. Results: A total of 14,467 patients underwent an esophagectomy for stage I, II, and III disease (OE: n = 8,445; MIE: n = 4,506; RAMIE: n = 1,516). Between 2010 and 2020, OE decreased by 39%, while MIE and RAMIE increased by 88% and 918%, respectively (Fig. T20-1A). At non-academic centers, OE was performed more frequently (42%) than MIE (35%) or RAMIE (36%) (P < 0.001), and uninsured patients were more likely to undergo OE (1.9%) than MIE (1.4%) or RAMIE (0.7%) (P = 0.012). In the propensity matched cohort, the number of sampled lymph nodes was higher in RAMIE, compared with OE (16 [11,23] vs 14 [9, 20]; P < 0.001). The length-of-stay (LOS) was shorter in the RAMIE group compared with OE (9 [7, 13] days vs 10 [8, 15], P < 0.001). Long-term survival was significantly better in the RAMIE group, compared with OE (P < 0.001; Fig. T20-1B), while RAMIE had comparable lymph node harvest (P = 0.212) and overall survival (P = 0.076) with MIE (Fig. T20-1C). Conclusions: This contemporary review of a national cohort demonstrates the rapid adoption of minimally invasive esophagectomy techniques, without compromise in short-term or long-term outcomes. However, the adoption of minimally invasive technology has not been uniform, highlighting the need to expand access to minimally invasive esophageal procedures.
John K. Sadeghi, MD1, Nosayaba Enofe, MD, MPH2, Roman Petrov, MD, PhD, MBA3, Zubair Malik, MD1, Charles T. Bakhos, MD, MBA1. 1Temple University Health System, Philadelphia, PA, USA, 2Fox Chase Cancer Center, Philadelphia, PA, USA, 3The University of Texas Medical Branch, Galveston, TX, USA.
Objective: Complications from transoral incisionless fundoplication (TIF) including TIF herniation and esophageal diverticulum are rarely reported and can be difficult to manage when they occur. We describe our experience with a rarely reported TIF complication using a minimally invasive surgical approach. Methods: A 69-year-old man with pulmonary fibrosis and COPD underwent a left lung transplant. The patient also had GERD and was found to have a 2 cm hiatal hernia by high resolution manometry. He underwent a TIF procedure but developed worsening symptoms and reflux after 6 months. He was then found to have a distal esophageal diverticulum with a 1 cm hiatal hernia, severe reflux on pH impedance, and concern for TIF herniation. We review the key steps to a robotic TIF takedown and esophageal diverticulum repair in this complex patient. Results: Key steps include: Intra-operative esophagogastroduodenoscopy and distal esophageal diverticulum identification. Division of the gastrohepatic ligament and identification of the right crus. Circumferential hernia sac dissection and identification of the left crus. Identification of the polypropylene TIF fasteners with extensive peri-hiatal adhesiolysis from the post-TIF inflammatory process. Identification and protection of the Vagi nerves. Greater curvature mobilization and short gastric transection. TIF hernia reduction and wrap take down. Intrathoracic esophageal mobilization and dissection to ensure at least 3 cm of intra-abdominal esophagus without tension. False esophageal diverticulum with wide neck about 2 - 3 cm long exposure. Muscle imbrication over the diverticulum to avoid introducing a staple line in an immunocompromised patient. Cruroplasty and gastropexy to recreate the angle of HIS. No fundoplication due to the diverticulum in the lumen of the esophagus and concern for mechanical obstruction potentially leading to future worsening of the diverticulum. Conclusions: TIF may not be an adequate option for patients with GERD in the setting of small (up to 2 cm) hiatal hernias. Patient selection is key to avoiding serious complications which can be successfully managed with a robotic-assisted approach. In our practice, we currently reserve TIF to patients with GERD and no documented hernia on the pre-operative work-up.
T22
Robotic-Assited Repair of a Large Bochdelak Hernia
Robert D. Allman, MD, Carlos Anciano, MD, Audrea Oliver, MD, Mark Iannettoni, MD, James Speicher, MD. East Carolina University, Greenville, NC, USA.
Objective: 43 year old female who presented with symptoms of pain in the right upper quadrant, dysphagia, and difficulty sleeping. Patient was found to have a large right-sided Bochdalek hernia on CT scan. Methods: Patient underwent a Robotic-assisted Bochadalek hernia repair with mesh. Results: Patient had a satisfactory postoperative course with discharge home on postoperative day 2. Conclusions: Robotic assisted repair of Bochadalek hernias is a effective method to treating large hernias.
T23
Outcomes Comparison of Robotic-Assisted and Video-Assisted Thoracoscopic Cardiac Sympathetic Denervation
Albert Leng1, Kelsey Melinosky1, Christopher R. Johnson1, Katherine Giuliano1, Eric Etchill1, Harikrishna Tandri2, Malcolm V. Brock3, Jinny Ha3. 1Department of Surgery, Johns Hopkins University School of Medicine, Baltimore, MD, USA, 2Department of Cardiology, Johns Hopkins University School of Medicine, Baltimore, MD, USA, 3Division of Thoracic Surgery, Department of Surgery, Johns Hopkins University School of Medicine, Baltimore, MD, USA.
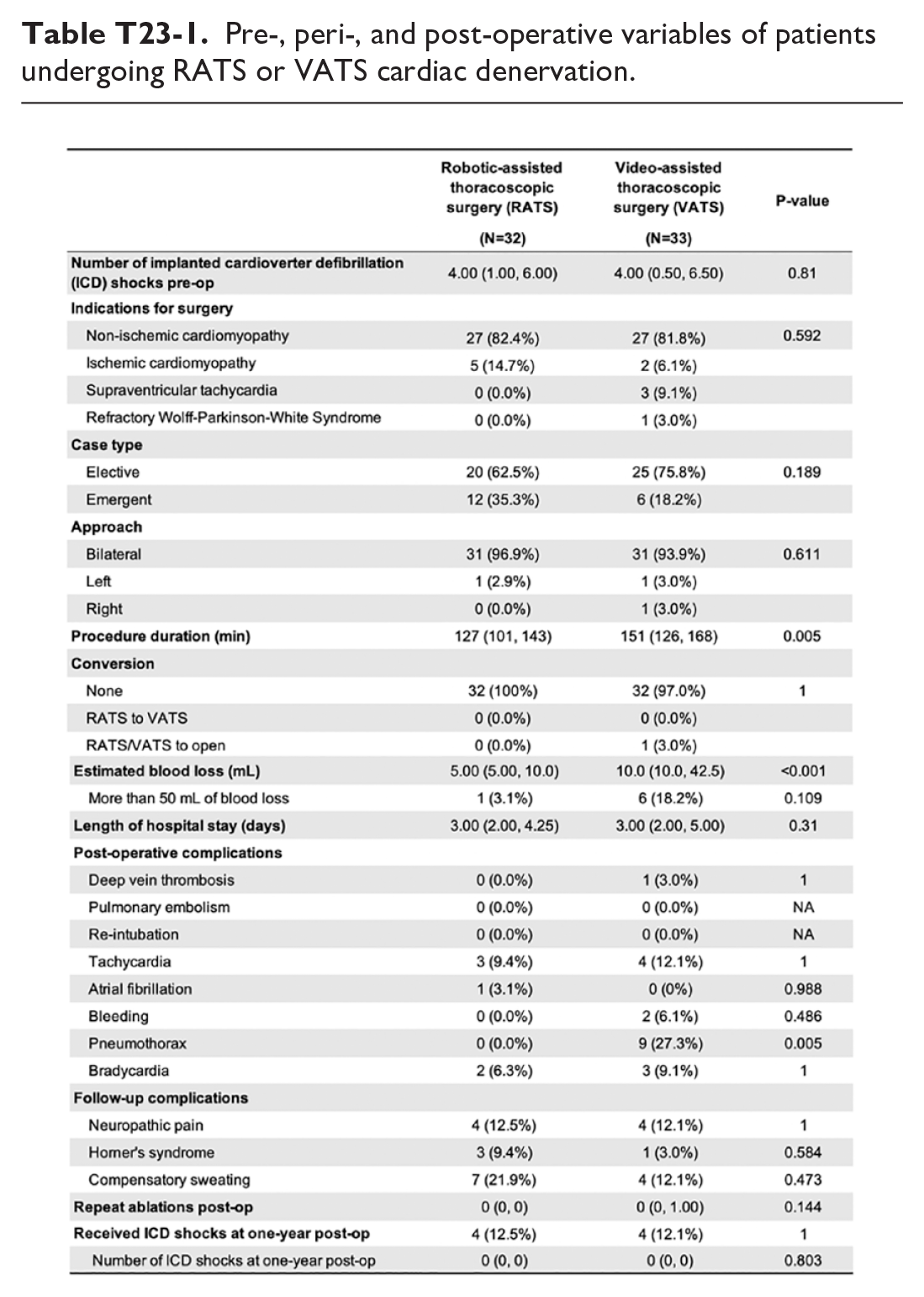
Objective: Cardiac sympathetic denervation (CSD) is a surgical antiadrenergic procedure that can reduce sustained ventricular tachyarrhythmia (VT) and implanted cardioverter defibrillation (ICD) shocks. Video-assisted thoracoscopic surgery (VATS) is currently the standard approach utilized in CSD, however, the practicality for robot-assisted thoracoscopic surgery (RATS) has yet to be investigated. Methods: We conducted a single-center retrospective study of all adult patients (n = 65) who underwent CSD from 2019 to 2021 and collected follow-up data up to at least one-year post-operation. Patients were stratified into two groups: those who underwent RATS denervation and those who underwent VATS denervation. In robotic-assisted CSD, the sympathetic chain was removed from the inferior aspect of the stellate ganglion to the fourth intercostal space. Results: A total of thirty-two patients underwent RATS cardiac denervation and thirty-three underwent VATS cardiac denervation. Compared to the VATS cohort, the RATS cohort had a significantly higher number of male patients (P = 0.003); all other demographic characteristics were not significant. Those undergoing RATS denervation had significantly shorter procedure durations with a median of 127 minutes (P = 0.005) and less estimated blood loss (P < 0.001); but, when adjusting to only account for blood loss of 50 mL and above, the significance disappears (P = 0.109). Patients receiving the VATS approach were significantly complicated by pneumothorax (P = 0.005) when compared to the RATS approach. At one-year post-op, both groups had significant reductions in ICD shocks compared to pre-op, both decreasing from a median of 4 to 0 shocks (P < 0.001). Additionally, at one-year post-op, the percentage of patients with persistent ICD shocks and the median of ICD shocks were similar between groups. No conduction changes occurred as PR and QT intervals were not significantly different between pre- and post-op for both VATS and RATS denervation. Conclusions: The RATS approach to cardiac denervation has similar one year follow-up outcomes in reducing recurrent VT as the VATS approach, however, patients undergoing RATS denervation experienced better peri-operative outcomes. This shows promise for robotic CSD to be an effective therapeutic option for patients with malignant arrhythmias.
Pre-, peri-, and post-operative variables of patients undergoing RATS or VATS cardiac denervation.
T24
Robotic Approach to Catamenial Pneumothoraxwith Diaphragmatic Hernia
Shruthi Nammalwar, Justin Watson, MD, Andrew Brownlee, Harmik Soukiasian, Amirhossein Mahfoozi. Cedars Sinai Medical Center, Beverly Hills, CA, USA.
Objective: A 37 year old female with cyclic pelvic pain managed with oral contraceptives presented with shortness of breath and chest pain and was found to have a catamenial pneumothorax. Methods: Technical steps to robotic repair of catamenial pneumothorax with primary repair diaphragmatic defect, right upper lobe and right lower lobe blebectomy, and chemical pleurodesis. Results: Findings and operative techniques as narrated in the video. Conclusions: Robotic approach to catamenial pneumothorax with diaphragmatic herniation can be safely performed.
T25
Crisis Resource Management in Robotic Thoracic Surgery
Gaetano Romano1, Fabrizia Calabrò2, Carmelina Cristina Zirafa1, Claudia Cariello3, Alda Mazzei3, Selene Tognarelli4, Beatrice Manfredini5, Federico Davini1, Franca Melfi1. 1Minimally Invasive and Robotic Thoracic Surgery, University of Pisa, Pisa, Italy, 2Department of Surgical, Medical, Molecular and Critical Care Pathology, University of Pisa, Pisa, Italy, 3Department of Anesthesia and Critical Care Medicine, University Hospital of Pisa, Pisa, Italy, 4The BioRobotics Institute, Scuola Superiore Sant'Anna, Pisa., Pisa, Italy, 5Division of thoracic surgery, department of medical and surgical sciences, University of Modena and Reggio Emilia, Modena, Italy, Modena, Italy.
Objective: Robotic surgery represents the ultimate evolution of minimally invasive surgery. In high-volume centers it is mandatory to set an adequate training program for robotic surgery which also include the management of intraoperative adverse events. The objective of this video is to illustrate the simulation of the management of arterial bleeding during robotic major lung resection. Methods: A robotic operating room was set up asking all professionals to participate. The figures involved were: console surgeon, assistant surgeon, nurse, assistant nurse, anesthetist, assistant anesthetist. The operating table was set up with a high-fidelity physical model integrated with an animal lung and a balloon filled with colored water to simulate bleeding. Results: As bleeding occurred, the console surgeon kept the “bleeding vessel” closed with the robotic instrument, allowing the assistant and nurse to begin undocking and simulate thoracotomy. Afterwards the first surgeon moved to the operating table for completion of surgery. Conclusions: The project proved to be effective in training the team for the adverse event, especially in the debriefing phase, during which each professional identified their tasks and any errors.
T26
Robotic Incision of Median Arcuate Ligament
Fazil Abbas, Michael Sestito, Guhlam Abbas, MD. West Virginia University School of Medicine, Morgantown, WV, USA.
Objective: Median Arcuate Ligament Syndrome is also known as celiac artery compression syndrome, celiac axis compression syndrome or Dunbar syndrome.10-24% have compression of Celiac Axis but rarely symptomatic. Methods: Fibrous tissue connecting left and right crus and making the anterior surface of aortic hiatus, compressing the celiac axis. The pain may be due to compression of sympathetic chain. Pt are usually young females presenting with post prandial colicky pain, Nausea, Anorexia, Weight loss, Diarrhea. Results: It is a Diagnosis of exclusion. Workup includeDuplex ultrasonography : Peak systolic velocity > 200 cm/sCT Angiography: Fish hook appearance of Celia Axis originDynamic MR Angiography: Compression of Celiac Axis during respiration. Conclusions: Robotic incision of median arcuate ligament for MALS is a novel minimally invasive approach in well selected patients. it leads to faster recovery as compare to open approach.
T27
Robotic Assisted Transhiatal Esophageal Epiphrenic Diverticulectomy Technique Compared to Other Diverticulectomy Techniques
Nidhi Desai, John Waters, Tanya Pothini, Scott Reznik, Steve Ring, Michael Jessen, Sravanya Gavini, Howard Weiner, Kemp Kernstine. UT Southwestern Medical Center, Dallas, TX, USA.
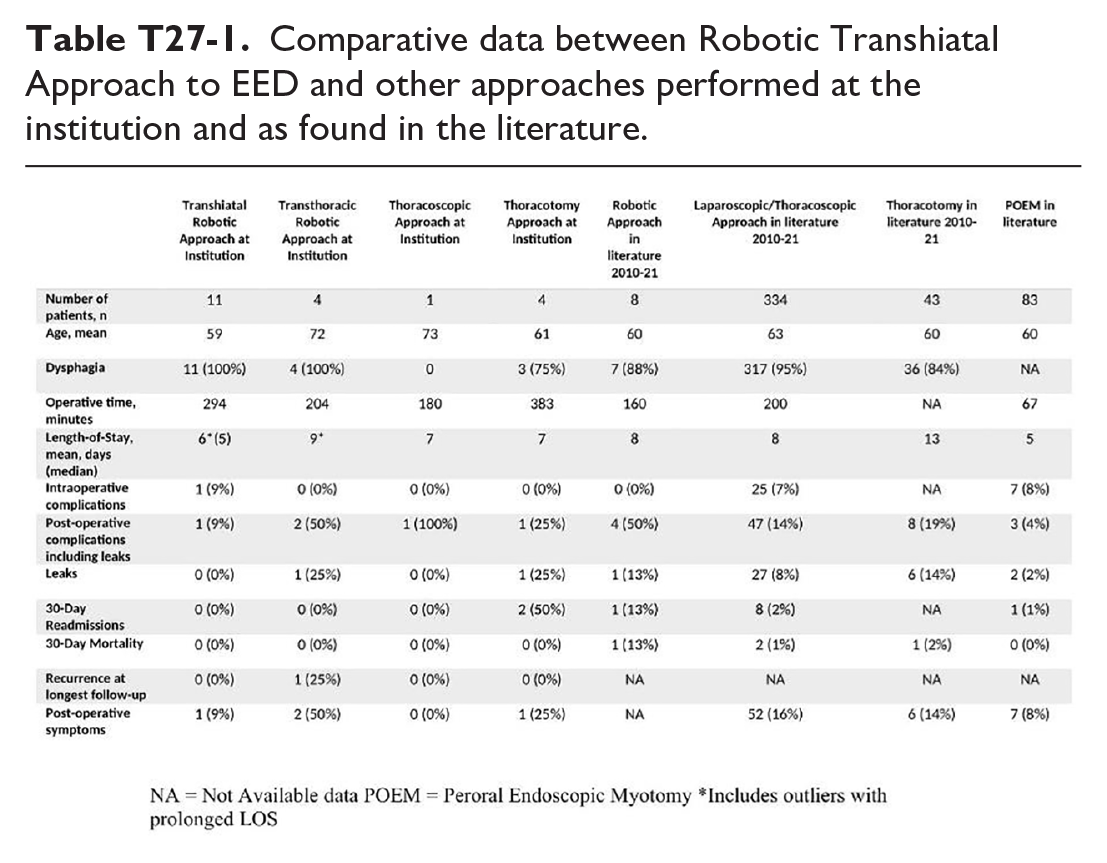
Objective: Historically, epiphrenic esophageal diverticula (EED) have been resected through left thoracotomy. We designed a robotic transhiatal (RTED) technique that minimizes perturbation of the esophageal hiatus, avoids transthoracic access and blind passage of dilators, and resects the diverticulum. We compared short- and long-term outcomes of this technique to other techniques at our institution and the literature. Methods: From 2005 to 2022, we performed a retrospective review of a prospectively managed database of EED patients. The 4-arm robotic approach requires 7 laparoscopic ports for a diverticulectomy and a 180-degree Heller myotomy that is extended 4 cm onto the stomach along with a Dor fundoplication. Demographic, clinical, and perioperative outcomes are delineated. We performed a systematic review of the literature. We compared RTED to other approaches at our institution and in the literature. Results: 15 patients underwent robotic diverticulectomy, 11 RTED and 4 transthoracic. For the RTED patients, average age 59 y (22 to 75 y), 36% males, average BMI of 27. 100% with dysphagia, 9% with weight loss (> 5% of their body weight) and 9% with evidence of chronic aspiration. The mean operative time was 294 minutes and estimated blood loss was 60 ml. Average size of the resected diverticulum by barium esophogram was 4.7 cm (2.3 to 6.6 cm). The median length-of-stay (LOS) was 5 days. There were no clinical leaks. 1 (9%) patient developed intra-operative bilateral pneumothoraces. 1 (9%) patient developed post-operative bilateral pulmonary embolism and right pleural effusion. 1 (9%) patient reported occasional dysphagia which resolved with dilation. Patient who presented with weight loss achieved stabilization. There were no recurrences, no 30-day readmissions, and no mortality. The mean Likert postoperative pain level on days 1, 2, and 3 were 6, 4, and 3, respectively and the 24-hr morphine equivalents were 336, 97, and 41 grams, respectively. The average cost of care was $36,699. Table T27-1 compares the clinical details and outcomes between this group, other techniques at our institution, and the literature. Conclusions: The RTED appears safe and efficient. Compared with alternative techniques at our institution and in the literature, the procedure takes longer to perform, but there is benefit in a shorter LOS and reduced complication rate. It restores normal anatomy while preserving key elements of the normal swallowing function.
Comparative data between Robotic Transhiatal Approach to EED and other approaches performed at the institution and as found in the literature.
T28
Traumatic Diaphragm Hernia Repair
Haley Leesley, MD, Gal Levy, Roman Petrov. UTMB-Galveston, Galveston, TX, USA.
Objective: 54 year old incarcerated male with longstanding traumatic diaphragm hernia repair presented with progressive shortness of breath. This was repaired with an endoscopic anterior component separation, followed by right thoracotomy, reduction of abdominal contents, and placement of mesh. Endoscopic anterior component separation is a relatively quick procedure, with low morbidity and can be used to treat and/or prevent abdominal compartment syndrome in large volume hernias.