
Abstract

One of the most complex and challenging procedures in the field of cardiac surgery has been and remains the replacement of the entire aortic arch. Almost 7 decades have passed since the first reported successful total aortic arch operation by DeBakey and colleagues in 1957. 1 Many surgical and technological advances have made this operation much safer, faster, and more durable.
The “elephant trunk” procedure from Borst and colleagues was published in 1983, and it simplified the second operation (i.e., descending or thoracoabdominal aortic repair). 2 This procedure underwent a technological evolution in 2001, when Karck and colleagues replaced the free-floating elephant trunk with an endovascular stent graft. This procedure was named the “frozen elephant trunk” (FET) by Hans Borst himself. 3 Twenty-four years later, the FET procedure has undergone substantial modifications and improvements. It is now common practice to use prefabricated, off-the-shelf, hybrid prostheses, which come in a variety of sizes and models, such as straight or multibranched grafts.4 –7
In this editorial, we were asked to comment on the “10 Commandments” of the FET. It is a great honor and pleasure for us to do so.
First Commandment: Preoperative Planning
Preoperative planning of the anticipated surgical procedure is crucial. Patients with aortic aneurysm and chronic aortic dissection undergo elective surgery, and there is usually enough time for thorough planning. In contrast, patients with acute aortic type A dissection require an emergent operation, leaving less time for planning. Nonetheless, even in such emergent situations, attention must be paid to medical conditions such as pericardial tamponade or mesenteric malperfusion, as these may affect the surgical plan.
Assessment of the patient and development of a surgical plan are key to ensuring a successful operation. This involves evaluating the medical underlying aortic pathology (aneurysm, chronic dissection, acute dissection), coexisting medical conditions, and review of the imaging studies. For instance, cardiac conditions such as reduced left ventricular ejection fraction or valvular disease will have a direct impact on the operation. Furthermore, coexisting medical conditions such as severe chronic obstructive pulmonary disease or chronic kidney disease will have to be taken into account for the surgical plan or might even render a patient inoperable. All of these conditions will affect the surgical plan.
Second Commandment: Preoperative Imaging
Generally speaking, a cardiac gated computed tomography angiography (CTA) is the most appropriate imaging test for planning aortic surgery. Magnetic resonance imaging (MRI) is an alternative; however, cardiac gated CTA provides higher resolution and is more widely available. In contrast, MRI is more time-consuming but offers dynamic imaging, has no radiation, and is less detrimental to the kidneys. The scan should be electrocardiogram triggered and should depict the supra-aortic vessels down to the bifurcation of the common femoral artery.
We consider an echocardiogram mandatory in aortic arch surgery, as it reveals important information on right and left ventricular function, valvular disease, and so forth. In elective operations, this should be done in the preoperative phase. In emergent settings, a bedside echo might be helpful, and intraoperative transesophageal echocardiography should be considered mandatory in every case. Coronary clearance is mandatory in elective operations. In dedicated centers, coronary clearance by CTA might be sufficient. If CTA shows concerns for obstructive coronary artery disease, invasive coronary angiography should be ordered. Imaging of the intracranial vessels, especially to evaluate the circle of Willis, would be ideal but is not always possible, especially in emergent situations.
Third Commandment: Aortic Pathology
The underlying aortic pathology (i.e., the indication for surgery) has a great impact on the aortic arch operation. It is important to note that complex aortic aneurysm, acute dissection, and chronic dissection are 3 different diseases and should be treated differently.
Originally, the FET was used to treat complex aortic aneurysms involving the aortic arch and proximal descending aorta. Ideally, the FET treats a complex aortic aneurysm in a single-stage operation as long as the disease ends at the “landing zone” of the FET stent. This is a major advantage when compared with the classic elephant trunk operation, which always requires a second operation or intervention. Even if the aortic disease is not limited to the proximal descending aorta at the landing zone, the FET provides an ideal landing zone for future interventions. 8
The FET can be used to treat acute aortic dissection DeBakey type I. Its usage remains controversial, but multiple specialized aortic centers have demonstrated excellent outcome. Moreover, the American Association for Thoracic Surgery published an expert consensus article on aortic dissection with recommendations on the usage of FET in this setting. 9 Class IIa recommendations for the use of FET include (1) a primary entry tear in the aortic arch or proximal descending aorta, (2) peripheral malperfusion, and (3) aortic arch or thoracic aortic aneurysm or rupture. Class IIb recommendations include (1) promoting favorable aortic remodeling and (2) young patients with Marfan syndrome or hereditary thoracic aortic disorder.
Chronic aortic dissection can be another indication for the use of FET. The stent graft portion of the FET will stabilize the true lumen and may seal proximal entry tears. If the entry tear is located more distally, or if there are multiple entries, often future endovascular interventions might be necessary.
Fourth Commandment: Cannulation and Cardiopulmonary Bypass
The setup of cardiopulmonary bypass (CPB) may vary from institution to institution. Retrograde autologous priming can be helpful to avoid hemodilution. Probably the most common arterial access site is the right axillary artery. This artery can be easily exposed by a right infraclavicular cut down. One of the main benefits of it is that it not only allows initiation of CPB but also provides unilateral cerebral perfusion circulatory arrest. Alternatively, central aortic cannulation is another common access site. We highly recommend echocardiography-guided and Seldinger technique placement of the arterial cannula. This helps to confirm cannulation of the true lumen in cases for aortic dissection and helps to avoid accidental placement of the cannula to one of the supra-aortic vessels.
Femoral arterial cannulation is considered inferior nowadays, as there is a risk of retrograde embolization of thrombotic debris, especially in elderly patients. However, it may be helpful in emergent cases with pericardial tamponade, as it allows initiation of CPB and cooling of the patient before opening of the pericardium. Nonetheless, the CTA scan should be carefully reviewed to ensure that the dissection membrane does not affect the common femoral artery.
Alternative access, such as direct open aortic cannulation (Samurai technique) or cannulation of the left ventricle are also possible and can be considered for emergent situations. Venous cannulation is usually done by cannulation of the right atrium. Bicaval cannulation is sometimes required for complex multiprocedural operations involving additional procedures such as mitral or tricuspid repair.
A left ventricular vent that is usually inserted via the right superior pulmonary vein can help decompress the heart and clear the operative field.
Fifth Commandment: Standardization of Surgical Technique and Sequence
Standardization of surgical technique is highly advisable. Having a surgical plan that incorporates every single step of the operation will facilitate the operation. In this section, we will give a step-by-step overview of the entire operation.
In both elective and emergent (acute aortic dissection) settings, we prefer to cross-clamp the aorta and proceed with the proximal repair during the cooling phase. We believe that profound hypothermia is not needed nowadays in most cases, and moderate hypothermia (approximately 25 to 28 °C) with cerebral protection is acceptable. Once the target temperature is reached and proximal aortic repair has been completed, circulatory arrest is initiated. We prefer cerebral protection via antegrade delivery, either unilateral through the right axillary artery or bilateral through selective cannulation of the innominate and left subclavian artery. During arch repair, myocardial perfusion (beating heart arch surgery) is an option to avoid prolonged cardiac ischemia in complex operations. 10 With regard to distal aortic repair (Fig. 1), we prefer to perform the distal anastomosis in zone 2, as this will simplify this surgical step. Further, we commonly anastomose the left subclavian artery with a Dacron graft before initiating the circulatory arrest to minimize the duration of circulatory arrest. After completion of the distal anastomosis (Fig. 2), rewarming is begun, and the main body of the FET prosthesis is anastomosed to the ascending aorta. Then, the left carotid artery and the innominate artery are anastomosed to the side branches of the FET graft. The graft to the left subclavian artery is then anastomosed to the third branch of the FET graft (Fig. 3).
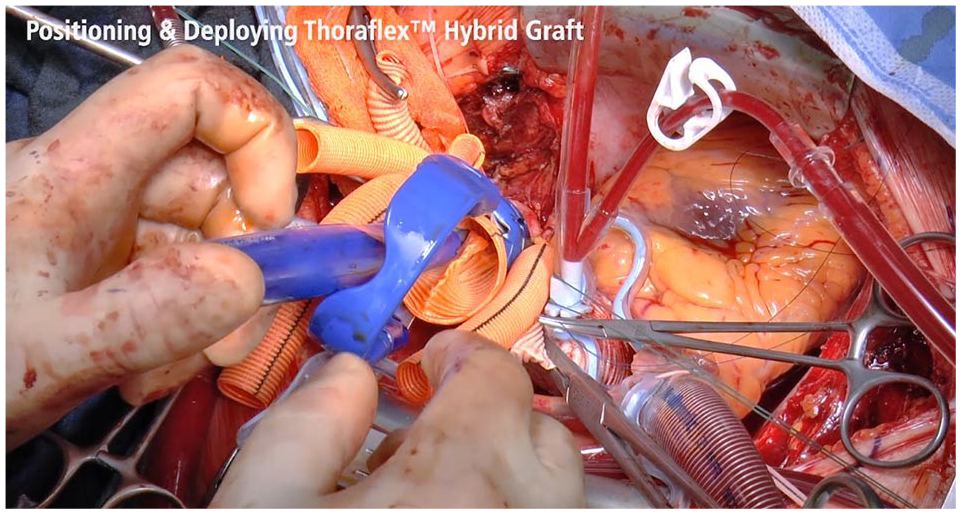
Deployment of 4-branched frozen elephant trunk prosthesis.
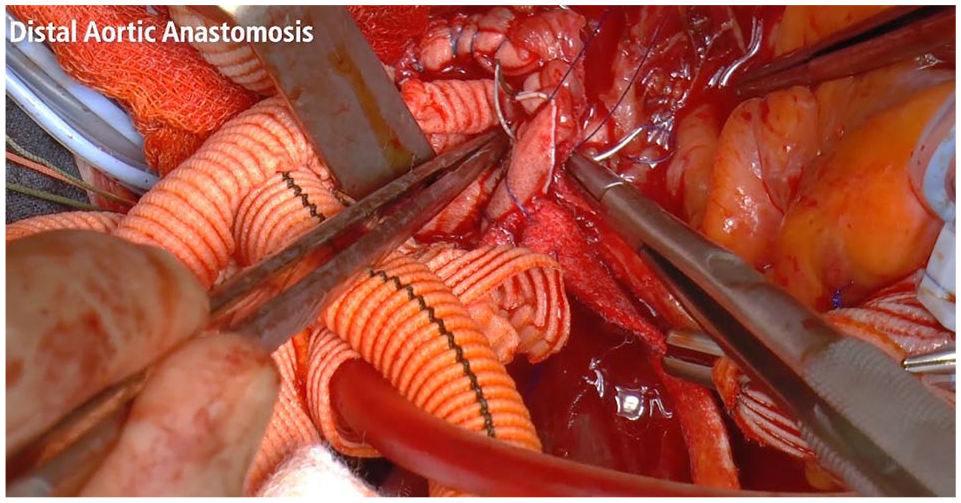
Distal aortic anastomosis between a 4-branched frozen elephant trunk graft and the aortic arch.
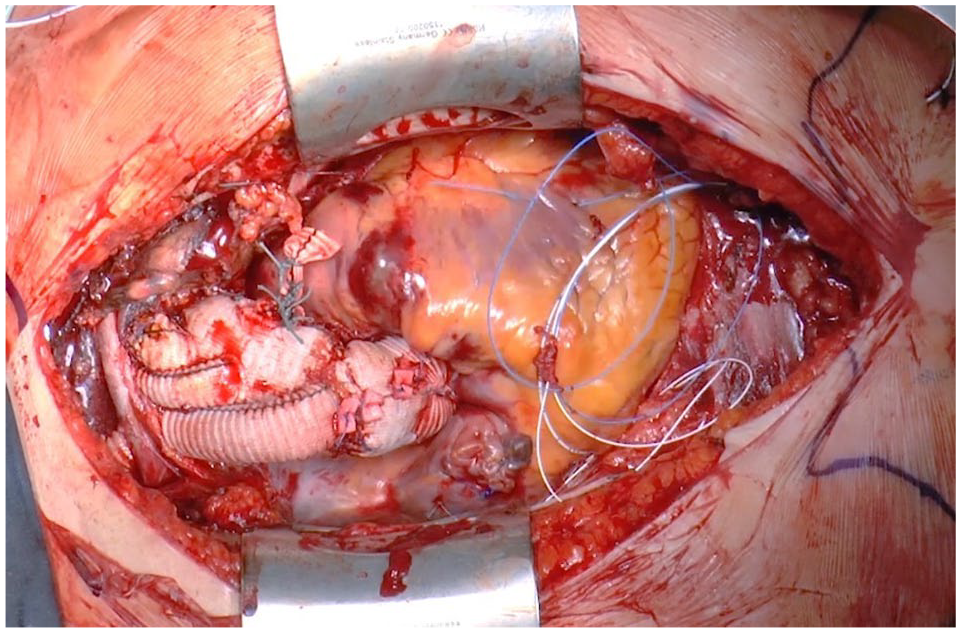
Completed total aortic arch repair using a 4-branched frozen elephant trunk prosthesis.
We believe that 4-branched grafts facilitate the operation and offer the benefit of selective anastomosis of every supra-aortic artery. Once the aortic cross-clamp is removed and CPB discontinued, the fourth branch used for antegrade perfusion is ligated and resected.
Sixth Commandment: Sizing of the FET
The correct sizing of the FET graft is of crucial importance. The sizing has to be tailored to the underlying aortic pathology. In aortic aneurysms, the goal, if possible, is to achieve a single-stage procedure. In turn, the stent graft should be slightly oversized, and the distal landing zone should be beyond the aneurysmal part of the proximal descending aorta. In patients with mega-aortic syndrome, the stent graft will be free floating and will provide a landing zone for future interventions. In acute aortic dissections, the size of the stent graft should be equal to the size of the total aortic diameter. Oversizing can lead to a higher incidence of distal stent graft–induced new entry tears.
In chronic aortic dissections, the size of the true lumen is usually rather small. The purpose of the FET is to initially increase the diameter of the true lumen and also to promote positive aortic remodeling. Further, the FET allows an ideal landing zone for future interventions.
Regardless of the aortic pathology, the length of the stent graft has to be carefully chosen. A long stent carries a higher risk for spinal ischemia with subsequent paraparesis. As this is a detrimental complication, it should be obviously avoided at all costs. We generally prefer a stent length of only 10 cm beyond the origin of the left subclavian artery.
Seventh Commandment: Cerebral Protection
Total aortic arch replacement with the FET requires an episode of circulatory arrest due to the necessity of excluding the supra-aortic arteries. The cerebrum is extremely susceptible to ischemia due to its high metabolic rate. Hypothermia reduces the metabolic need of the brain. Hypothermic circulatory arrest described by Griepp and colleagues was the only and key component to allow such complex operations during the early days of cardiac surgery. 11
There are different degrees of hypothermia: (1) profound hypothermia <14 °C, (2) deep hypothermia 14.1 to 20 °C, (3) moderate hypothermia 20.1 to 28 °C, and (4) mild hypothermia 28.1 to 34 °C. Although it is possible to perform total aortic arch operations at profound hypothermia without any further protection strategies, it is more common nowadays to cool the patient to mild or moderate hypothermia and use concomitant cerebral perfusion.
Cerebral perfusion can be delivered in antegrade or retrograde fashion. Presumably, the most common form of cerebral perfusion is unilateral cerebral perfusion by cannulation of the right axillary artery. This requires an additional infraclavicular incision with dissection and exposure of this artery. Although this extends the operative time, it gives the benefit of a clear operative field. Unilateral cerebral perfusion relies on the perfusion of the contralateral brain by the circle of Willis.
Selective bilateral antegrade cerebral perfusion involves the insertion of catheters directly into the innominate and left carotid arteries. Obviously, it provides the benefit of active perfusion of both brain hemispheres. Some studies suggest that this brain perfusion strategy is safer compared with unilateral antegrade cerebral perfusion for extended circulatory arrest times. Retrograde cerebral perfusion relies on cannulation of the superior vena cava with subsequent perfusion with cold blood. It is nowadays less common.
Eighth Commandment: Risk of Intraluminal Thrombus Formation
The thrombosis of the perigraft lumen in aortic aneurysms and the thrombosis of the false lumen in acute dissections are desired effects after FET placement. Some centers, including our group, have reported intraluminal thrombus formation in the stent portion of the FET prosthesis. 12 Although the incidence of such events seems to be very low, it is a potentially life-threatening complication. The exact incidence and cause remain to be determined. Intraluminal thrombus formation can present as a solely radiologic accidental finding observed on a routine CTA scan without symptoms or as a thromboembolic event occluding visceral arteries with the need for emergent intervention. It does seem to be more common when using the Thoraflex Hybrid FET device (Terumo Aortic, Inchinnan, UK) in cases of mega-aortic syndrome, in which there is no landing zone and the FET stent “dangles” in the descending aorta. In these cases, initiation of anticoagulation prevents thrombus formation.
Ninth Commandment: Postoperative Care
Total aortic arch replacement with FET is a complex surgical operation. It is of the utmost importance to have an experienced surgeon as well as an entire team familiar and dedicated to this procedure. It has been shown that dedicated aortic centers may have more optimal outcomes than low-volume centers.
During the postoperative phase, the team on the intensive care unit plays a crucial role. Although most operations on the proximal aorta require a low to normal blood pressure goal, we believe that it might be beneficial to have a higher blood pressure goal after FET operations to maintain adequate spinal perfusion. Optimizing hematocrit and oxygenation are also believed to be beneficial. Further, the intensive care unit team needs to properly assess the patient with regular wake-up trials to detect any paraparesis. If this is the case, the insertion of a cerebrospinal fluid drain can be crucial. We do not advise a routine preoperative cerebrospinal fluid drain placement.
Tenth Commandment: Postoperative Imaging and Follow-Up
Regular follow-up after aortic surgery is recommended and may improve survival. Especially patients with syndromic disease or aortic dissection are more likely to experience future aortic events, which may require intervention.
After repair for acute aortic dissection, current guidelines recommend follow-up including imaging after 1, 6, and 12 months and then annually thereafter. We think that CTA is the most appropriate imaging modality, whereas MRI may be an alternative in younger patients as it avoids radiation or in patients with chronic kidney disease.
Conclusions
Total aortic arch repair with the FET procedure can simplify aortic arch surgery and may prevent future operations. This applies to both elective operations for aortic aneurysms and emergent surgery for aortic dissection. However, the FET procedure remains a complex and challenging operation with risks for complications, such as distal stent graft–induced new entry and intraluminal thrombus formation. Careful patient selection is highly recommended, and lifelong follow-up of patients after FET implantation is also recommended.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.