
Abstract
Objective:
Totally endoscopic mitral valve plasty (TEMVP) requires technical proficiency, which may be insufficient during the initial adoption phase. This study evaluated the learning curve and perioperative outcomes during the early experience with TEMVP, using operation time and complications as key metrics.
Methods:
We retrospectively analyzed 125 consecutive patients who underwent TEMVP between October 2021 and April 2025. Despite the early adoption phase, 40 patients met criteria for complex pathology (i.e., concomitant procedures, infective endocarditis, reoperation, narrow thoracic cage, or difficult aortic cross-clamping) and were defined as the complex group. The remaining 85 patients formed the control group. Surgical outcomes were compared between groups. The learning curve was assessed using operation time and risk-adjusted cumulative sum (RA-CUSUM) analysis based on predicted morbidity (Japan Score).
Results:
The complex group had longer operative times (335 ± 71 vs 282 ± 61 min, P < 0.001) and higher complication rates (17.5% vs 3.5%, P = 0.012). Two-year survival was 94.7% in the complex group and 100% in the control group (P = 0.03); freedom from reoperation was 100% and 94.2%, respectively (P = 0.30). Operation time significantly decreased over time in the overall and control groups but not in the complex group. RA-CUSUM analysis showed favorable cumulative trends below the predicted risk threshold, with no group exceeding the sequential probability ratio test decision limit of ±3.74.
Conclusions:
Despite the inclusion of complex cases, early TEMVP outcomes were favorable and within acceptable safety limits. RA-CUSUM and operation time analysis supported the presence of a manageable learning curve at our institution.
This is a visual representation of the abstract.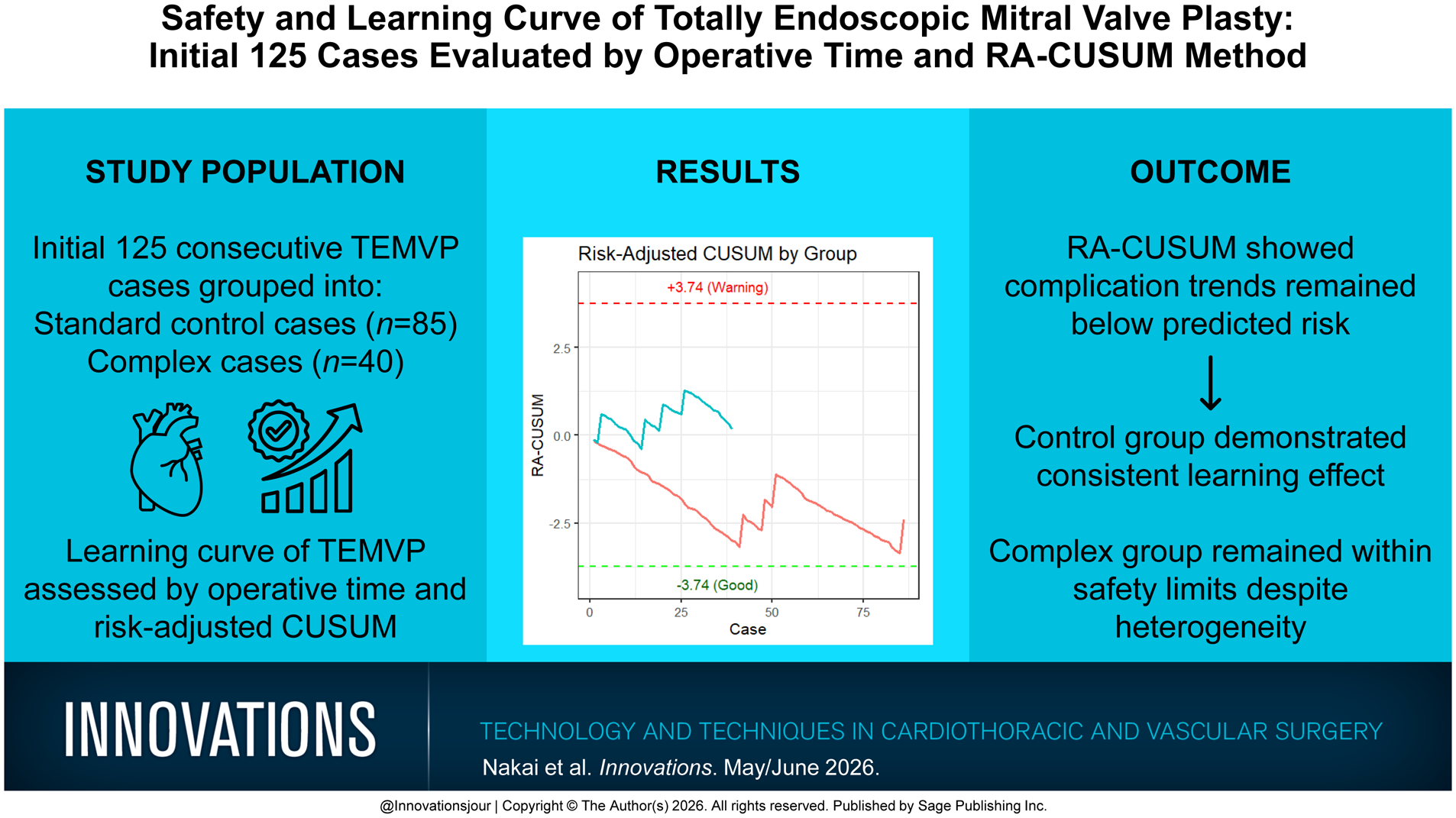
Keywords
Central Message
Early outcomes of TEMVP were favorable, even with complex cases included. Risk-adjusted CUSUM analysis effectively identified performance trends and validated the presence of a safe and achievable learning curve during the initial adoption phase, without exceeding predefined safety thresholds.
Introduction
Minimally invasive mitral valve plasty (MIMVP) has gained widespread adoption in Japan in recent years due to its advantages, including preservation of the sternum, improved cosmetic outcomes, shorter recovery time, and reduced invasiveness. 1 Among the various approaches to MIMVP, totally endoscopic mitral valve plasty (TEMVP) is increasingly recognized as a standard technique at experienced, high-volume centers.2,3
However, whether performed under direct vision or via totally endoscopic techniques, the safe introduction of MIMVP requires a thorough understanding of complication avoidance strategies, proficiency in operating through a limited field of view, and a dedicated surgical team—including perfusionists well-versed in cardiopulmonary bypass techniques. The need for specialized instruments and institutional readiness further complicates the learning curve, which is often reported to be steep, requiring 75 to 125 cases to achieve procedural maturity.4,5
Surgical indication for MIMVP should be approached cautiously in institutions with limited experience. This is particularly important because MIMVP tends to involve longer cardiopulmonary bypass times and presents challenges in complex cases. Procedures for patients with infective endocarditis or those undergoing reoperations remain technically demanding.6,7 Therefore, when choosing between MIMVP and median sternotomy, institutional expertise should be considered, and the benefits of a minimally invasive approach should clearly outweigh the risks.
At our institution, TEMVP has been adopted, and the cumulative case volume has now exceeded the learning threshold previously reported for MIMVP. Although complex and high-risk cases were included, we applied MIMVP only after careful multidisciplinary discussions involving cardiologists, nurses, and perfusionists and only when a clear clinical benefit was anticipated.
This study aimed to evaluate our institutional learning curve in the early phase of TEMVP adoption using 2 metrics: operation time as an indicator of technical proficiency and postoperative safety assessed via risk-adjusted cumulative sum (RA-CUSUM) analysis based on predicted morbidity from the Japan Adult Cardiovascular Surgery Database (JCVSD) dataset. 1
Methods
Study Design and Patient Selection
This retrospective study evaluated the early institutional experience with TEMVP, focusing on technical proficiency assessed by operation time and postoperative safety assessed using RA-CUSUM analysis based on predicted morbidity from the JCVSD. 1
Although conducted during the early adoption phase, several patients presented with complex pathologies or underwent combined procedures. To ensure appropriate evaluation of the learning curve and safety, patients were stratified based on preoperative and intraoperative risk factors. Cases with any of the following conditions were assigned to the complex group: concomitant procedures, active infective endocarditis, reoperation, narrow thoracic cage, or anticipated difficulty in aortic cross-clamping. All remaining cases were assigned to the control group for comparison.
We included 125 consecutive patients who underwent TEMVP between January 2021 and April 2025. All cases were scheduled for mitral valve repair. Patients preoperatively planned for valve replacement or with concomitant aortic valve replacement were excluded.
Preoperative Variables
The collected variables included age, sex, body surface area, left ventricular ejection fraction (LVEF), brain natriuretic peptide (BNP), chronic kidney disease (CKD), diabetes mellitus, hypertension, chronic obstructive pulmonary disease (COPD), atrial fibrillation, history of percutaneous coronary intervention or coronary artery bypass grafting, New York Heart Association class, Japan Score 2, and Japan Score morbidity. COPD was defined as forced expiratory volume in 1 s <70% and CKD as estimated glomerular filtration rate <45 mL/min/1.73 m2.
Surgical Technique
All procedures were performed by a single surgeon (Y.A.), who received off-site proctoring in TEMVP from his proctor, occasionally consulted him before individual cases, and adopted a technique that closely followed the approach described by Ito et al. 2
Patients were placed in the left lateral decubitus position with deflation of the right lung. A 3 to 4 cm right lateral thoracotomy was made in the fourth or fifth intercostal space, and an Alexis wound protector (Applied Medical, Rancho Santa Margarita, CA, USA) was used without metal retractors. A thoracoscopic camera port was inserted in the fourth intercostal space, and the left-hand instrument port was placed in the third intercostal space, completing a 3-port configuration.
Cardiopulmonary bypass was established via the right femoral vessels. The arterial line was placed in the femoral artery, and the venous cannula was advanced to the superior vena cava under intraoperative fluoroscopy. The right internal jugular vein was not routinely cannulated. In cases with significant atherosclerosis or calcification in the abdominal or thoracic aorta, right axillary artery or ascending aorta cannulation was added. 8 During bypass, the body temperature was lowered to 30 to 31 °C and to below 28 °C under ventricular fibrillation. A flexible aortic cross-clamp was used, and antegrade cardioplegia was delivered. All instruments, including the left atrial vent, cardioplegia cannula, and atrial retractor, were inserted through the main incision without accessory ports. Procedures were performed under full endoscopic vision, and mitral valve repair was principally based on the loop technique.
Because learning curve analysis is generally conducted as a time-sequential assessment, including complex cases may introduce distortion in the interpretation of procedural progress. Therefore, to validate the impact of case complexity, we categorized patients into subgroups based on predefined criteria. The first complex case was introduced at the 12th operation, which involved a narrow thoracic cage and infective endocarditis confined to the posterior leaflet. Although classified as complex, the pathology and technical aspects were considered relatively straightforward, and we judged them to be manageable.
Complex Group Definition
The complex group consisted of 40 patients meeting any of the following 5 criteria:
Concomitant procedures (n = 7): cases with tricuspid valve repair, maze procedure, or left atrial appendage (LAA) closure. These were defined as complex only when all procedures were performed simultaneously. Cases involving tricuspid annuloplasty with either maze or LAA closure alone were classified as control. These were expected to prolong operative and bypass times.
Active infective endocarditis (n = 7): only cases without abscess formation, in which valve repair could be completed without conversion to replacement, were included. Those with root abscess on preoperative computed tomography (CT) were treated via median sternotomy.
Reoperations (n = 12): required adhesiolysis and, in some cases, fibrillatory arrest due to difficult aortic clamping.
Narrow thoracic cage (n = 12): sternovertebral distance <75 mm; expected to restrict working space and prolong operation time.
Difficult aortic cross-clamping (n = 7): included 2 reoperations with adhesions; 5 cases with severe atherosclerosis of the ascending aorta, in which a minimally invasive approach was selected for mitral valve plasty for the reasons described above; 3 patients receiving prednisone ≥5 mg/day; 1 frail 87-year-old patient with osteoporosis; and 1 patient with poorly controlled diabetes (hemoglobin A1c >9). All underwent valve repair under hypothermic ventricular fibrillation. Details of these procedures have been reported previously. 9
Detailed case-by-case allocation criteria are provided in Supplemental Table 1.
Control Group Definition
The remaining 85 patients who did not meet any of the above criteria were assigned to the control group.
Clinical Outcomes and Analysis
We compared intraoperative parameters (operation time, cardiopulmonary bypass time, aortic cross-clamp time), postoperative outcomes (intensive care unit [ICU] stay, hospital stay, discharge to home), and complication rates (stroke, acute kidney injury, reexploration, pacemaker implantation) between the groups. Kaplan–Meier curves were used to evaluate overall survival and freedom from reoperation, with log-rank tests to compare groups.
Learning curves were assessed by plotting operation time against case sequence and performing linear regression analyses for the entire cohort and for each group separately.
In addition, the distribution of complex cases was evaluated by calculating their proportion within consecutive blocks of 10 cases. Furthermore, changes in cardiopulmonary bypass time, hospital length of stay, transfusion requirements, and the need for reintervention were also examined in relation to the cumulative number of cases performed.
RA-CUSUM Analysis
To evaluate surgical performance and learning trends based on complication rates, RA-CUSUM analysis was performed. The baseline failure rate (p0) was set at 6.55%, derived from national JCVSD data on major complications for mitral valve repair. 1 These complications included reexploration (2.3%), stroke (1.0%), wound/groin infection (0.1% each), prolonged ventilation >24 h (1.5%), acute kidney injury (1.6%), atrioventricular block (0.5%), and myocardial infarction (0.35%), totaling 7.45%. Considering the likelihood of overlap within a single patient, we applied a correction factor of 0.846 based on The Society of Thoracic Surgeons Adult Cardiac Surgery Database, in which the total summed incidence was 11.1% and major morbidity rate was 9.4%. 10 The adjusted morbidity rate was thus set at 6.30%, and by incorporating the 30-day mortality rate (0.05%) and in-hospital mortality rate (0.2%) reported by JCVSD, we finalized p0 as 6.55%.
SPRT and Statistical Thresholds
Decision limits of ±3.74 were defined using the sequential probability ratio test (SPRT) theory, based on p0 = 6.55% and an upper failure rate (p1) of 10.0%. Crossing +3.74 was interpreted as a statistically significant increase in failure beyond expected variance. 11 RA-CUSUM analysis thus enabled real-time detection of surgical performance changes during the learning phase. This method has been validated in cardiac surgery and is widely used to evaluate learning curves.5,11
Statistical Analysis
All analyses were performed using R version 4.5.1 (R Foundation for Statistical Computing, Vienna, Austria) and RStudio (Posit PBC, Boston, MA, USA). Continuous variables were analyzed using Student’s t test or Mann–Whitney U test and categorical variables using chi-square or Fisher’s exact test. A P value <0.05 was considered statistically significant.
Ethics Statement
This study was approved by the institutional review board (approval No. ethics 07-19). Informed consent was obtained from all patients or waived by opt-out disclosure, as appropriate for a retrospective study.
Results
Patient Characteristics
Baseline characteristics are summarized in Table 1. Compared with the control group, the complex group had a significantly lower LVEF (59.6% ± 8.6% vs 63.8% ± 7.2%, P = 0.005) and higher BNP levels (231 ± 493 vs 90 ± 125, P = 0.015). The prevalence of CKD was also higher in the complex group (27.5% vs 10.6%, P = 0.030). Both the Japan Score 2 (2.2 ± 2.8 vs 1.3 ± 1.4, P = 0.020) and Japan Score morbidity (11.7% ± 7.5% vs 7.8% ± 4.6%, P = 0.002) were significantly higher in the complex group, indicating an overall higher preoperative risk.
Baseline Characteristics of All Patients, Complex Group, and Control Group.
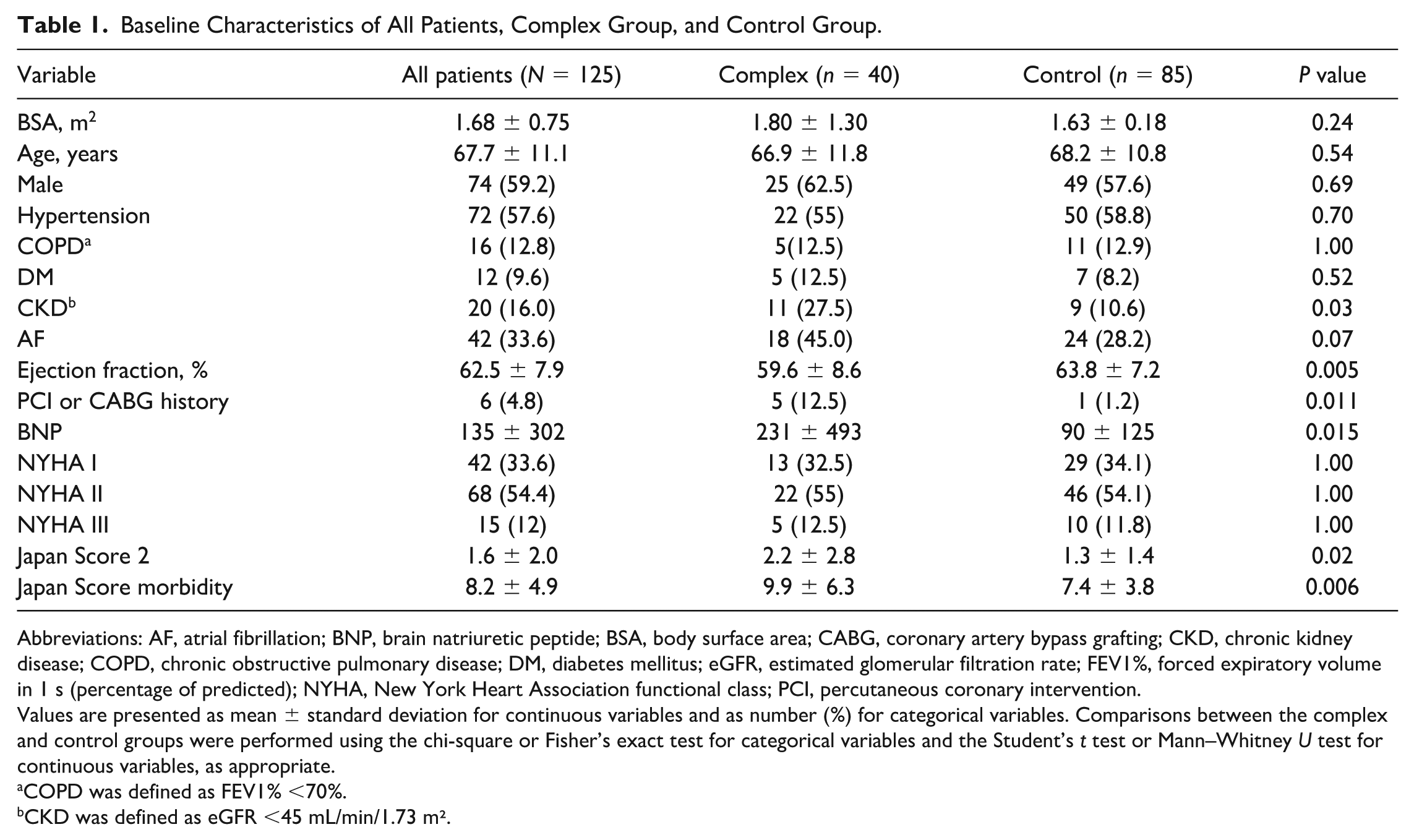
Abbreviations: AF, atrial fibrillation; BNP, brain natriuretic peptide; BSA, body surface area; CABG, coronary artery bypass grafting; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; DM, diabetes mellitus; eGFR, estimated glomerular filtration rate; FEV1%, forced expiratory volume in 1 s (percentage of predicted); NYHA, New York Heart Association functional class; PCI, percutaneous coronary intervention.
Values are presented as mean ± standard deviation for continuous variables and as number (%) for categorical variables. Comparisons between the complex and control groups were performed using the chi-square or Fisher’s exact test for categorical variables and the Student’s t test or Mann–Whitney U test for continuous variables, as appropriate.
COPD was defined as FEV1% <70%.
CKD was defined as eGFR <45 mL/min/1.73 m².
Etiology and Surgical Findings
Etiologic and operative findings are shown in Table 2. There were no major differences in leaflet involvement between the groups. Myxomatous degeneration was significantly less frequent in the complex group (72.5% vs 92.6%, P = 0.004). Infective endocarditis was present only in the complex group (15% vs 0%, P = 0.001). As for surgical techniques, patch plasty (15% vs 0%, P = 0.001) and leaflet resection (17.5% vs 3.5%, P = 0.01) were more commonly performed in the complex group, reflecting higher procedural complexity. Operation time (335 ± 71 min vs 282 ± 61 min, P < 0.001), cardiopulmonary bypass time (260 ± 69 min vs 212 ± 49 min, P < 0.001), and aortic cross-clamp time (165 ± 50 min vs 133 ± 32 min, P < 0.001) were all significantly longer in the complex group. In addition, transfusion was more frequently required in the complex group (67.5% vs 45.9%, P = 0.034).
Etiologies and Surgical Findings.
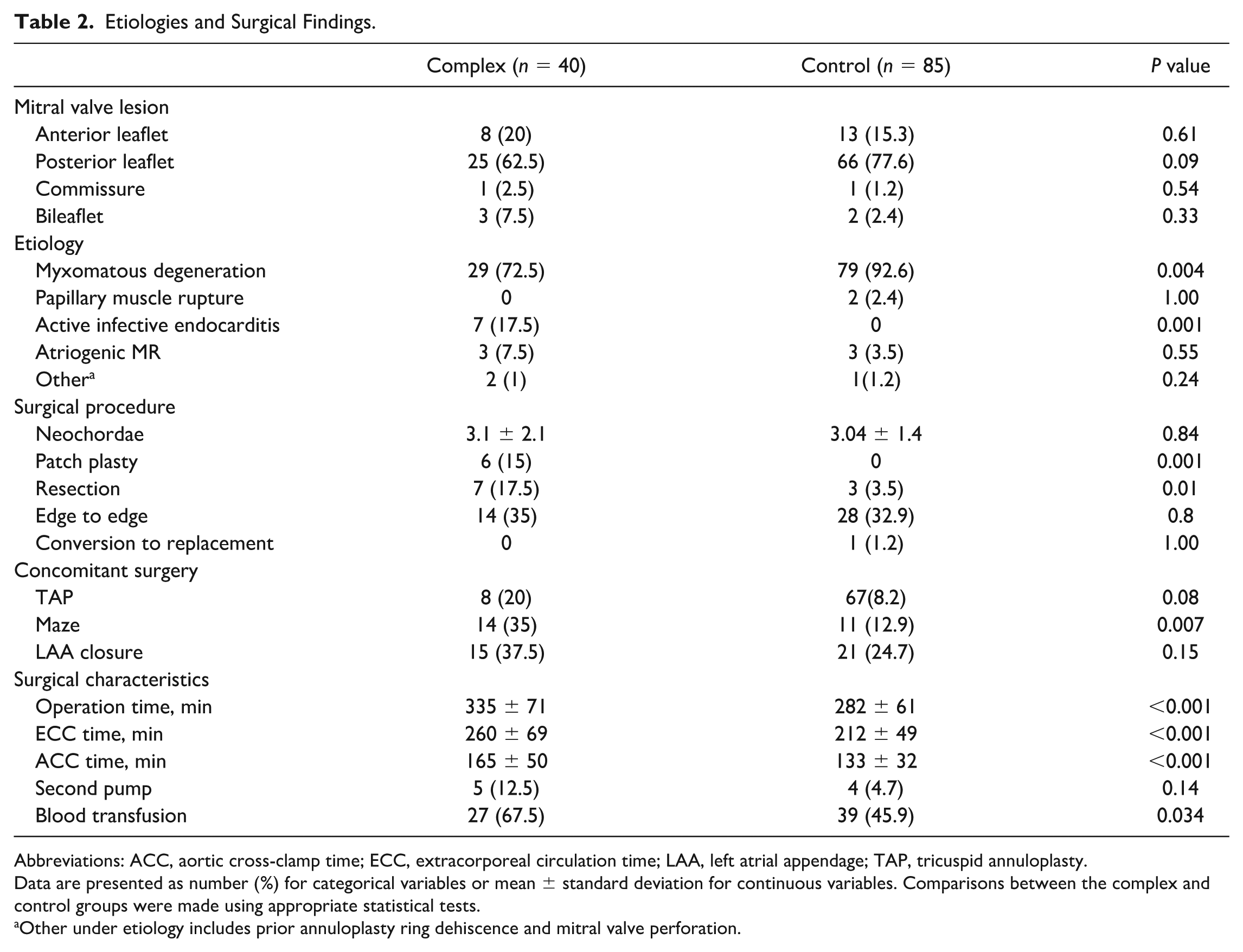
Abbreviations: ACC, aortic cross-clamp time; ECC, extracorporeal circulation time; LAA, left atrial appendage; TAP, tricuspid annuloplasty.
Data are presented as number (%) for categorical variables or mean ± standard deviation for continuous variables. Comparisons between the complex and control groups were made using appropriate statistical tests.
Other under etiology includes prior annuloplasty ring dehiscence and mitral valve perforation.
Early Postoperative Outcomes
Early outcomes are summarized in Table 3. The degree of postoperative mitral regurgitation (MR) was similar between groups: trace MR was seen in 80% of both groups and mild MR in 17.5% of the complex group versus 18.8% of the control group (P = 1.0). There was 1 in-hospital death (2.5%) in the complex group, with no significant difference between groups (P = 0.32). The deceased individual was a 55-year-old male patient on dialysis with infective endocarditis who had repeated embolic events and a splenic abscess before surgery. He died 2 months postoperatively from peritonitis and pancreatitis following worsening of the splenic abscess.
Early Postoperative Outcomes.
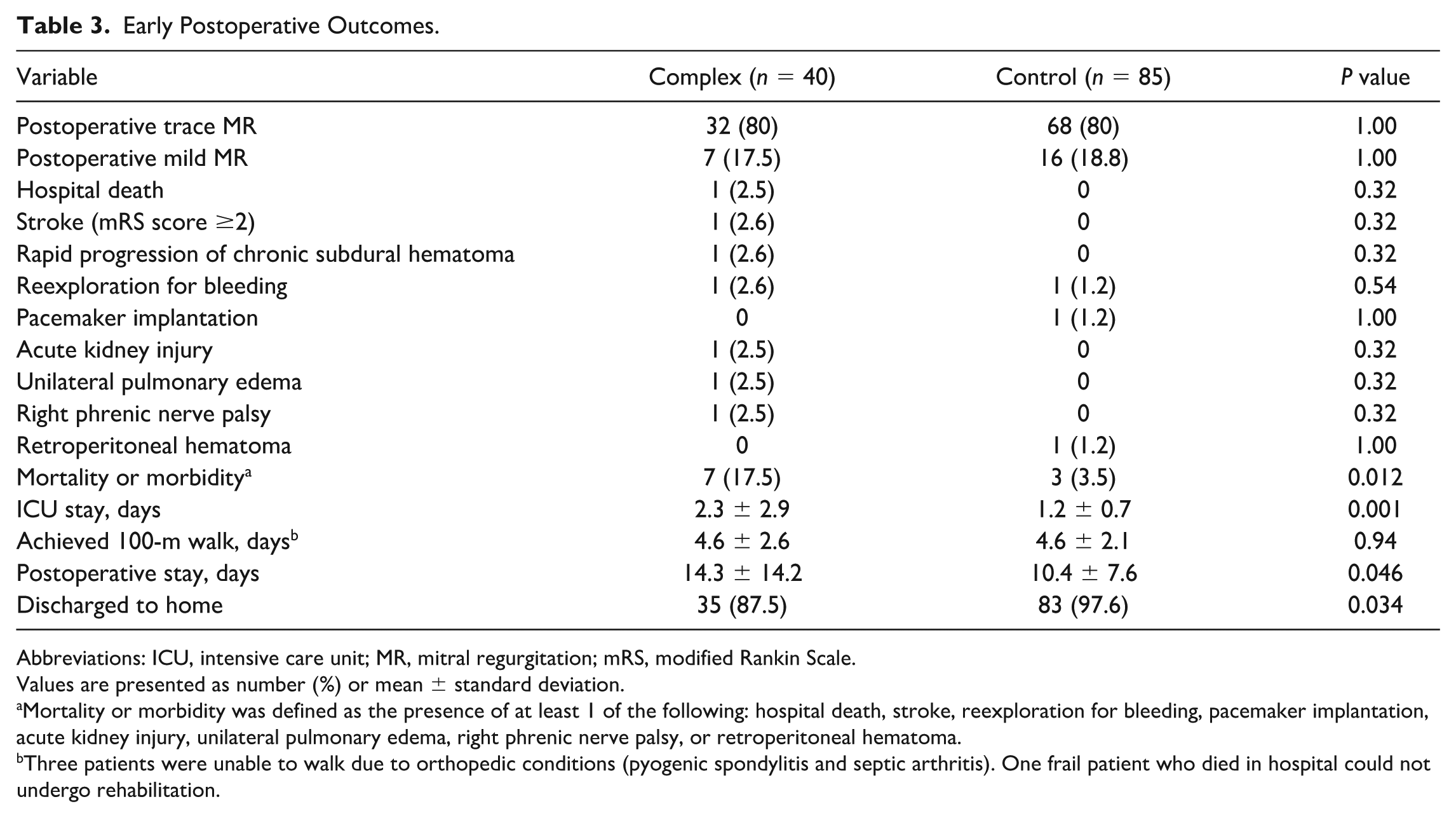
Abbreviations: ICU, intensive care unit; MR, mitral regurgitation; mRS, modified Rankin Scale.
Values are presented as number (%) or mean ± standard deviation.
Mortality or morbidity was defined as the presence of at least 1 of the following: hospital death, stroke, reexploration for bleeding, pacemaker implantation, acute kidney injury, unilateral pulmonary edema, right phrenic nerve palsy, or retroperitoneal hematoma.
Three patients were unable to walk due to orthopedic conditions (pyogenic spondylitis and septic arthritis). One frail patient who died in hospital could not undergo rehabilitation.
Major complications in the complex group included 1 case each of stroke, rapidly progressing chronic subdural hematoma, reexploration for bleeding, acute kidney injury, unilateral pulmonary edema, and right phrenic nerve palsy. In the control group, complications included 1 case each of pacemaker implantation and retroperitoneal hematoma. The combined mortality or morbidity rate was significantly higher in the complex group (17.5% vs 3.5%, P = 0.012). ICU stay was significantly longer in the complex group (2.3 ± 2.9 days vs 1.2 ± 0.7 days, P = 0.001), as was postoperative hospitalization (14.3 ± 14.2 days vs 10.4 ± 7.6 days, P = 0.046). The mean number of days to achieve a 100-meter walk was similar between groups (4.6 days, P = 0.94). The rate of discharge to home was lower in the complex group (87.5% vs 97.6%, P = 0.034).
Kaplan–Meier Analysis
The mean follow-up period for the cohort was 1.92 ± 1.16 years. Kaplan–Meier analysis demonstrated a 2-year overall survival of 98.4% (95% confidence interval [CI]: 96.1% to 100%). By group, 2-year survival was 100% (95% CI: 100% to 100%) in the control group and 94.7% (95% CI: 87.8% to 100%) in the complex group. The difference between the groups was statistically significant (log-rank test, P = 0.03; Fig. 1).
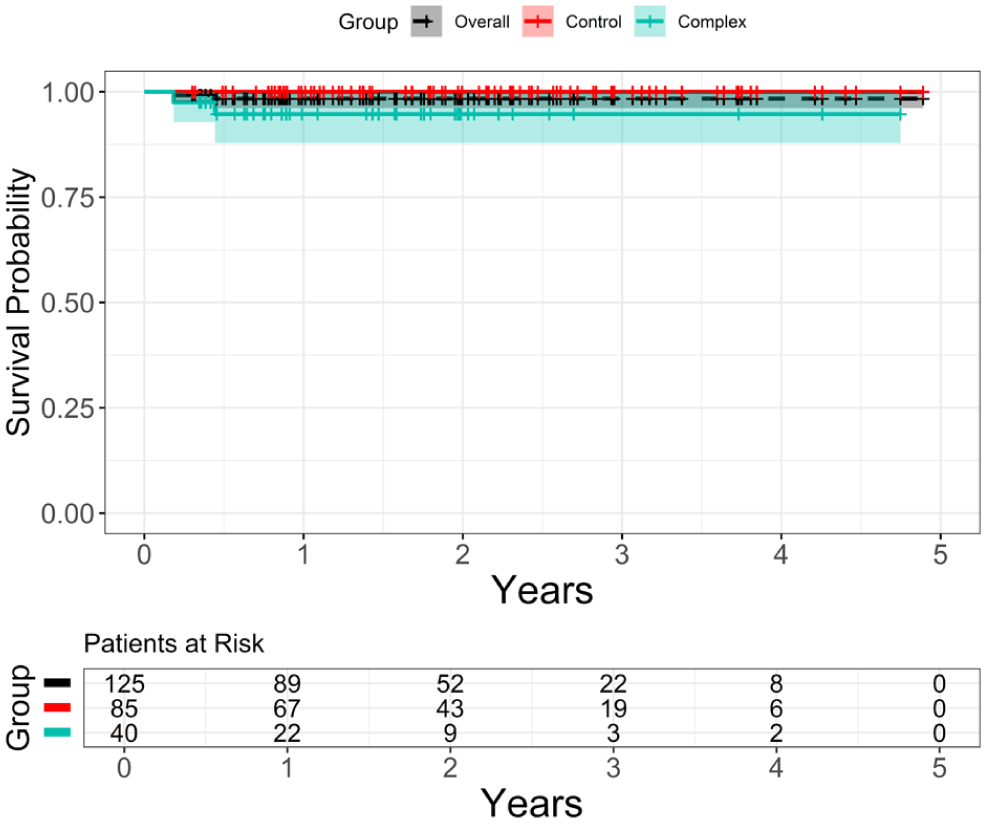
Kaplan–Meier survival curves comparing the control group (n = 85) and complex group (n = 40). The 2-year survival rate was 100% in the control group and 94.7% in the complex group (log-rank test, P = 0.03). The overall 2-year survival rate for the cohort was 98.4% (95% confidence interval: 96.1% to 100%). The black dashed line indicates the overall cohort.
Freedom from reoperation was also analyzed using Kaplan–Meier curves (Fig. 2). The 2-year rate for the overall cohort was 95.6% (95% CI: 90.9% to 100%). Group-specific rates were 94.2% (95% CI: 88.1% to 100%) for the control group and 100% (95% CI: 100% to 100%) for the complex group, with no significant difference between groups (P = 0.30).
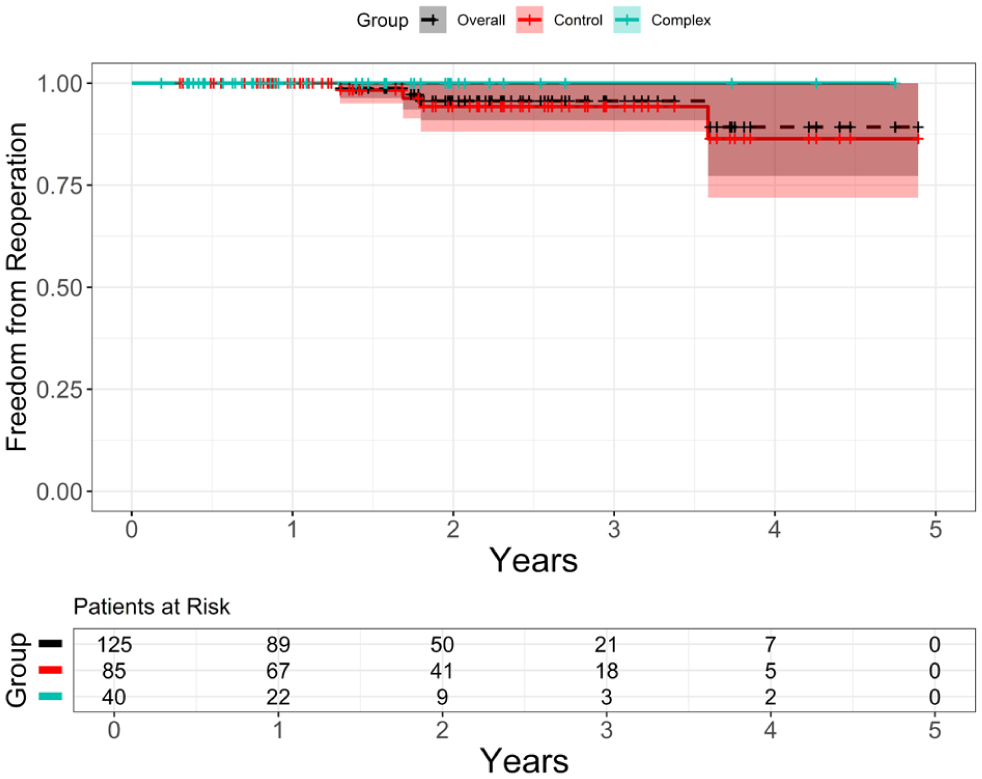
Kaplan–Meier curves showing freedom from reoperation for the control group (n = 85) and complex group (n = 40). The 2-year freedom from reoperation rate was 94.2% (95% CI: 88.1% to 100%) in the control group and 100% (95% CI: 100% to 100%) in the complex group (P = 0.30, log-rank test). The overall rate for the cohort was 95.6% (95% CI: 90.9% to 100%). The black dashed line indicates the overall cohort. CI, confidence interval.
Operative Time Learning Curve
The learning curve based on operation time is shown in Figure 3a. A significant decrease in operation time was observed with increasing case number (linear regression: R2 = 0.066, P = 0.004), although the overall variance remained substantial.
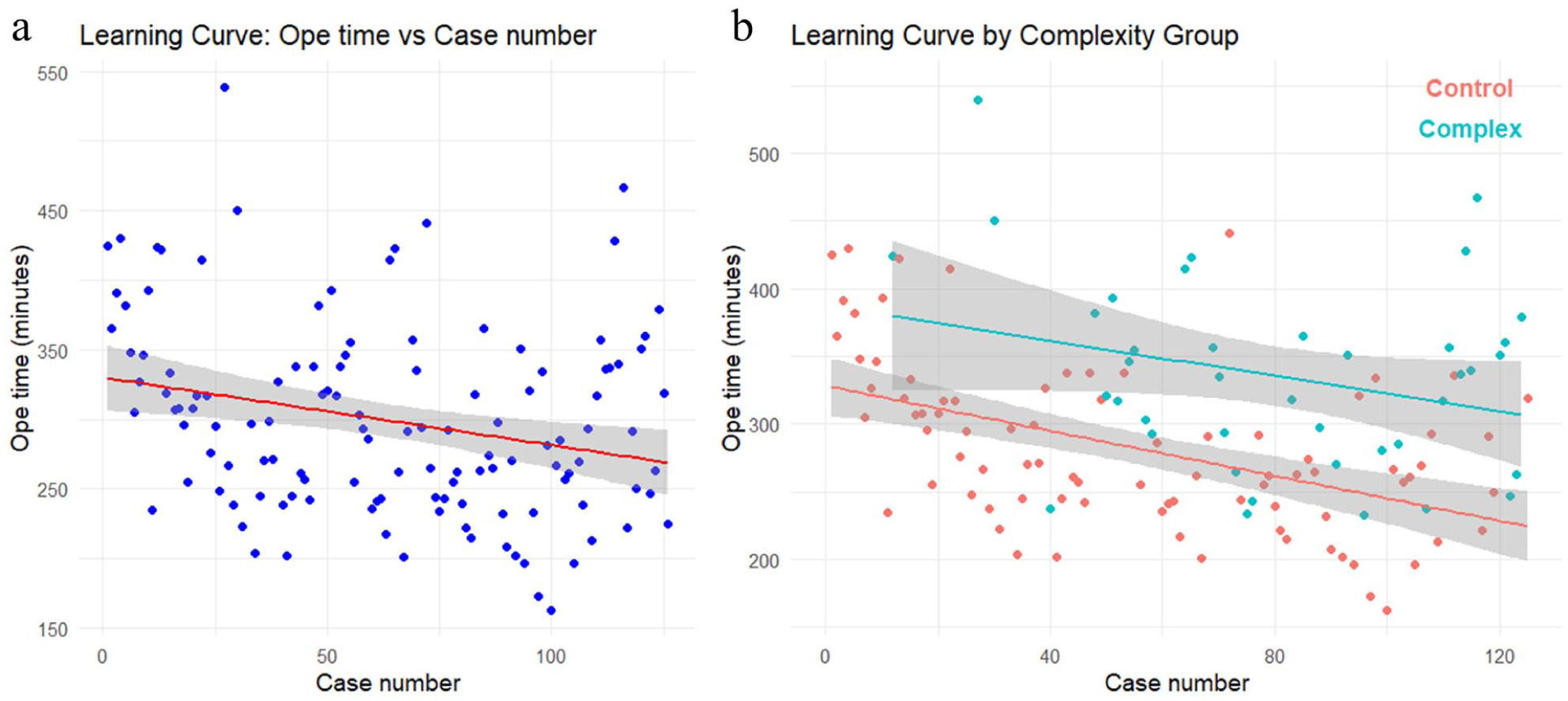
Scatter plots and linear regression lines showing the relationship between Ope time and sequential case number. (a) Overall trend for all 125 cases. Each case is plotted as a blue dot, and the regression line indicates a significant reduction in Ope time with increased experience (R2 = 0.066, P = 0.004), despite notable variability. (b) Group-specific analysis. Red dots represent the control group (n = 85), and cyan dots represent the complex group (n = 40). The control group demonstrated a significant learning curve with decreasing Ope time (regression coefficient = −1.68, R2 = 0.245, P < 0.001), whereas the complex group showed a nonsignificant downward trend (regression coefficient = −1.31, R2 = 0.076, P = 0.084). Ope, operation.
Figure 3b is plotted strictly in chronological case order, effectively functioning as a timeline. Control cases are shown in red and complex cases in cyan, demonstrating that complex cases began to appear from approximately the 12th case onward.
Group-specific regression analysis (Fig. 3b) showed a significant reduction in operation time in the control group (slope = −1.68, P < 0.001, R2 = 0.245). In the complex group, the slope was also negative (−1.31) but not statistically significant (P = 0.084), and the explanatory power was low (R2 = 0.076). Supplemental Figure 1 illustrates the proportion of complex cases by case block, which began to increase after approximately the 50th case.
Additional Learning Curve Analyses
Cardiopulmonary bypass time was analyzed using scatter plots and linear regression, but no significant temporal trend was observed (slope = −0.095, 95% CI: −0.391 to 0.202, P = 0.529; Supplemental Fig. 2). Similarly, the postoperative length of stay showed no significant association with case number (slope = −0.025, 95% CI: −0.075 to 0.026, P = 0.340; Supplemental Fig. 3).
For categorical outcomes, logistic regression analyses were performed. The transfusion requirement showed no significant association with case accumulation (odds ratio [OR] = 1.000, 95% CI: 0.991 to 1.010, P = 0.925), and reintervention likewise demonstrated no association (OR = 0.978, 95% CI: 0.947 to 1.011, P = 0.187).
RA-CUSUM Analysis
The RA-CUSUM analysis was performed using SPRT-based decision limits of ±3.74, with a baseline failure rate (p0) of 6.55% and an unacceptable failure rate (p1) of 10.0%. In the overall cohort (Fig. 4a), cumulative scores steadily decreased over time, although the lower decision boundary (−3.74) for statistical confirmation of good performance was not reached. Nevertheless, the overall trend remained below the predicted risk.
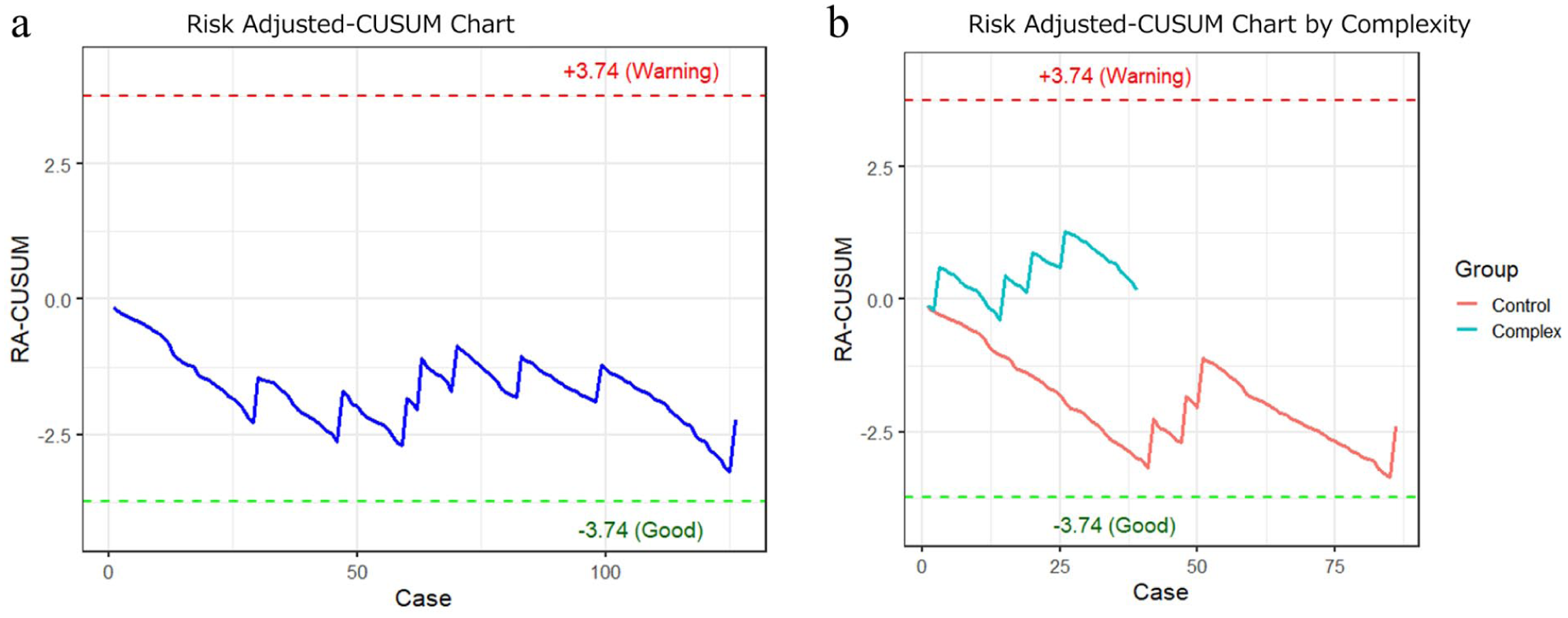
RA-CUSUM charts illustrating the temporal progression of postoperative outcomes based on predicted complication risk. An upward trend on the vertical axis reflects worse-than-expected outcomes, whereas a downward trend indicates better-than-expected performance. (a) RA-CUSUM chart for all 125 cases. The cumulative score gradually declined over time, suggesting outcomes were generally better than expected. However, the lower decision limit for statistically superior performance (−3.74) was not reached. (b) Group-specific RA-CUSUM charts. The control group showed a consistent decline in cumulative score, indicating favorable outcomes and learning progression. In contrast, the complex group exhibited relatively stable or slightly increasing scores but did not exceed the upper decision limit (+3.74), indicating acceptable safety throughout. RA-CUSUM, risk-adjusted cumulative sum.
Group-specific RA-CUSUM analysis (Fig. 4b) showed consistent score reduction in the control group, indicating good outcomes and progressive learning. In the complex group, cumulative scores remained mostly flat to slightly increasing but never exceeded the upper warning limit of +3.74 throughout the study period. These findings suggest effective learning and improved outcomes in the control group, whereas the complex group exhibited more variability, potentially due to smaller sample size and heterogeneous risk profiles.
Discussion
In this study, we quantitatively assessed the learning curve and safety of TEMVP during its early adoption using RA-CUSUM analysis. Conventional CUSUM evaluates binary outcomes but ignores patient-specific risk; therefore, we applied RA-CUSUM incorporating predicted morbidity from JCVSD via Japan Score morbidity. Although derived from sternotomy cases, Japan Score morbidity remains a practical benchmark in the absence of large minimally invasive cardiac surgery (MICS)–specific data in Japan.
Our RA-CUSUM analysis showed that cumulative scores stayed below predicted risk and did not approach the upper decision limit. The control group consistently exhibited negative scores, reflecting favorable outcomes and a stable learning effect. Even in the complex group, scores trended toward zero but remained within acceptable safety. Given the heterogeneity of complex cases, careful evaluation and individualized management remain crucial. Although inclusion of high-risk cases early may raise concerns, our practice emphasized thorough preoperative assessment and multidisciplinary discussion to ensure patient benefit.
Our results are consistent with prior reports from large centers. Holzhey et al. analyzed the early experiences of surgeons performing minimally invasive mitral valve surgery via right minithoracotomy and found that proficiency generally requires 75 to 125 cases. They also emphasized the need to maintain at least 1 case per week to preserve safety and noted substantial intersurgeon variability, advocating for structured monitoring and mentorship systems. 4 In our study, RA-CUSUM served as a real-time tool to continuously and objectively evaluate surgical performance based on complications.
Malik et al. proposed evaluating repair quality in mitral valve surgery via RA-CUSUM incorporating postoperative MR. They found that about 60 cases were needed to reduce residual regurgitation and up to 85 to stabilize overall outcomes, including complications. 5 Although our model did not include regurgitation due to difficulty in defining an objective threshold (p1), postoperative MR was well-controlled in our cohort. Future work will involve longitudinal echocardiographic assessment to integrate functional outcomes into performance analysis.
Other studies have highlighted the importance of institutional experience and team-based learning. Li et al. conducted a CUSUM failure analysis of 2,482 mitral repairs by 14 surgeons, showing that 50 to 200 cases were needed to achieve high repair success. 11 Institutional case volume had a positive spillover effect on individual learning curves. In their center, once overall experience passed a certain threshold, collective improvements in operation time and repair rates emerged, underscoring the value of shared expertise.
Successful implementation of TEMVP requires cumulative experience—not only in case volume but also in meeting qualitative goals such as minimizing residual regurgitation. Institutional knowledge transfer, potentially supported by structured mentorship (e.g., JMICS-certified proctorship), may further enhance surgeon development and procedural safety.
MICS procedures, including TEMVP, are generally associated with longer cardiopulmonary bypass times, especially in combined surgeries. Concomitant procedures such as tricuspid valve repair, maze, or left atrial appendage closure increase complexity and the risk of air embolism or incomplete deairing, potentially leading to neurologic complications. Stelzmueller et al. reported favorable outcomes for such complex endoscopic procedures, with a 30-day mortality of 0.7% and 10-year freedom from reoperation of 96.5%. 12 However, these results stem from high-volume centers and may not be generalizable. In our study, longer cardiopulmonary bypass and operative times were observed in the complex group. To mitigate ischemic time, retrograde cardioplegia was used when needed, and intraoperative reassessment guided decisions regarding concomitant procedures.
In infective endocarditis, MICS should be avoided if infection involves the aortic valve, annulus, or root. Our strategy was to select MICS only when preoperative CT and transesophageal echocardiography confirmed confinement to the mitral leaflets. Infective endocarditis often presents with fragile valve tissue and the need for complex repair. A systematic review by Shih et al. reported a repair rate of 32.4%, 30-day mortality rate of 9.4%, and reoperation rate of 9.3% in MICS for infective endocarditis, underscoring the technical challenge. 6 Careful selection and planning are crucial for safety in such cases.
For reoperations, the right minithoracotomy approach may reduce risks associated with adhesiolysis and graft injury compared with median sternotomy. Botta et al. demonstrated the feasibility of MICS reoperations, emphasizing the importance of minimizing adhesions and managing intraoperative risks such as air embolism and deairing. 7 In our series, although longer operative and cardiopulmonary bypass times were observed, serious complication rates were low. Proper case selection and intraoperative flexibility enabled safe reintervention via MICS.
Some reoperative cases or those with severe aortic calcification may preclude safe aortic cross-clamping. Salman et al. reported favorable outcomes using hypothermic ventricular fibrillation arrest as an alternative, with no significant difference in mortality or stroke rates compared with conventional methods. 13 We have adopted this technique in select patients and consider it a useful strategy when clamping is not feasible. However, its use should be limited to well-selected patients with good ventricular function, given uncertainties regarding myocardial protection.
In small-framed patients, limited intrathoracic space may impede visualization and instrument maneuverability. Shirasaka et al. reported that a sternovertebral distance of ≥80 mm on preoperative CT was associated with safe MICS outcomes. 14 We have successfully performed MICS in patients with distances <75 mm. Although technical challenges do exist, the endoscopic view generally allows adequate exposure of the mitral valve, making surgery feasible.
For all complex cases, our strategy involves thorough preoperative conferences with clinical engineers and operating room staff, with careful planning tailored to each patient. We also sought expert input from high-volume centers through direct consultation to support decision-making. Despite these efforts, the complex group exhibited a distinct learning curve. In Figure 3b, the reduction in operation time was not statistically significant (P = 0.084), and in Figure 4b, the RA-CUSUM trend, although within safety limits, differed from that of the control group. These findings may reflect the heterogeneity and technical demands of complex cases and underscore the value of structured team-based preparation and continued external guidance. Moving forward, we aim to strengthen this feedback system and enhance adaptability in complex TEMVP cases.
Limitations
This study has several limitations. First, it is a retrospective, single-center analysis of 125 patients and is susceptible to bias from case selection and evolving surgical techniques. Second, the baseline complication rate (p0) for RA-CUSUM was based on the JCVSD dataset, which primarily reflects conventional sternotomy and may not fully represent MICS-specific risk. Third, the complex group definition partially relied on subjective judgment, limiting generalizability. Fourth, learning curve assessment focused on operative time, complications, and RA-CUSUM, without addressing qualitative aspects such as intraoperative decision-making. Finally, the mean follow-up was relatively short (1.9 years), possibly limiting the evaluation of long-term outcomes such as reoperation or valve durability. Continued follow-up is needed.
Conclusions
Minimally invasive mitral valve repair, including TEMVP, requires attention to safety during early adoption. Using RA-CUSUM analysis, this study showed favorable early outcomes, with complication trends below predicted risk. The control group exhibited consistent learning, whereas the complex group remained within acceptable safety limits. These results suggest that with proper case selection and team coordination, TEMVP can be safely introduced even during early program phases.
Supplemental Material
sj-docx-1-inv-10.1177_15569845261447264 – Supplemental material for Safety and Learning Curve of Totally Endoscopic Mitral Valve Plasty: Initial 125 Cases Evaluated by Operative Time and RA-CUSUM Method
Supplemental material, sj-docx-1-inv-10.1177_15569845261447264 for Safety and Learning Curve of Totally Endoscopic Mitral Valve Plasty: Initial 125 Cases Evaluated by Operative Time and RA-CUSUM Method by Hidelazu Nakai, Akitoshi Yamada, Chihiro Okubo, Ryo Thoma and Yoshihisa Morimoto in Innovations
Supplemental Material
sj-tiff-2-inv-10.1177_15569845261447264 – Supplemental material for Safety and Learning Curve of Totally Endoscopic Mitral Valve Plasty: Initial 125 Cases Evaluated by Operative Time and RA-CUSUM Method
Supplemental material, sj-tiff-2-inv-10.1177_15569845261447264 for Safety and Learning Curve of Totally Endoscopic Mitral Valve Plasty: Initial 125 Cases Evaluated by Operative Time and RA-CUSUM Method by Hidelazu Nakai, Akitoshi Yamada, Chihiro Okubo, Ryo Thoma and Yoshihisa Morimoto in Innovations
Supplemental Material
sj-tiff-3-inv-10.1177_15569845261447264 – Supplemental material for Safety and Learning Curve of Totally Endoscopic Mitral Valve Plasty: Initial 125 Cases Evaluated by Operative Time and RA-CUSUM Method
Supplemental material, sj-tiff-3-inv-10.1177_15569845261447264 for Safety and Learning Curve of Totally Endoscopic Mitral Valve Plasty: Initial 125 Cases Evaluated by Operative Time and RA-CUSUM Method by Hidelazu Nakai, Akitoshi Yamada, Chihiro Okubo, Ryo Thoma and Yoshihisa Morimoto in Innovations
Supplemental Material
sj-tiff-4-inv-10.1177_15569845261447264 – Supplemental material for Safety and Learning Curve of Totally Endoscopic Mitral Valve Plasty: Initial 125 Cases Evaluated by Operative Time and RA-CUSUM Method
Supplemental material, sj-tiff-4-inv-10.1177_15569845261447264 for Safety and Learning Curve of Totally Endoscopic Mitral Valve Plasty: Initial 125 Cases Evaluated by Operative Time and RA-CUSUM Method by Hidelazu Nakai, Akitoshi Yamada, Chihiro Okubo, Ryo Thoma and Yoshihisa Morimoto in Innovations
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
This study was approved by the Institutional Review Board of Kita-Harima Medical Center (Approval No. Ethics 07-19). Informed consent was obtained or waived by opt-out disclosure, as appropriate for this retrospective study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.