
Abstract
Objective:
Octogenarians are sometimes excluded from mitral valve (MV) surgery due to increased morbidity and mortality. Sternal-sparing approaches (e.g., robotic MV surgery) have the potential to reduce these risks. We reviewed the outcomes of robotic totally endoscopic MV surgery in octogenarians.
Methods:
Of 600 patients undergoing elective robotic totally endoscopic MV surgery at our institution (September 2013 to December 2024), 40 patients were octogenarians. Early and midterm clinical and echocardiographic outcomes were analyzed. All procedures were performed using the da Vinci Si or Xi (Intuitive Surgical, Sunnyvale, CA, USA) with an endoscopic approach and an 8 to 10 mm working port.
Results:
The mean age was 83 ± 2.7 years, and 55% were female patients. The mean Society of Thoracic Surgeons risk was 4.4% ± 2.1%, 36 patients (90%) underwent MV repair, and 65% had concomitant procedures. Two patients had previous heart surgery. Cardiac arrest methods included endoballoon (62.5%), fibrillating heart (35%), or cross-clamp (2.5%). There was 1 (2.5%) conversion to sternotomy. The incidence of new postoperative atrial fibrillation was 15%, and 3 patients (7.5%) returned to the operating room for bleeding. There were no postoperative myocardial infarctions, strokes, or early mortalities. Mean intensive care unit and hospital length of stay were 1.5 ± 0.8 and 3.5 ± 1.5 days, respectively. Return to full activity occurred at a mean of 13 ± 9 days. Early postoperative echocardiography revealed 95% none to mild mitral regurgitation (MR). Clinical follow-up was complete in 100% of patients at a mean of 37 months. All-cause mortality occurred in 9 patients, and 1 was a cardiac-related death. At midterm echocardiography follow-up (mean 36 months), 90% had none to mild MR.
Conclusions:
These findings add to the growing evidence supporting the safety and efficacy of robotic totally endoscopic MV surgery and specifically recognize its benefits in older patients.
This is a visual representation of the abstract.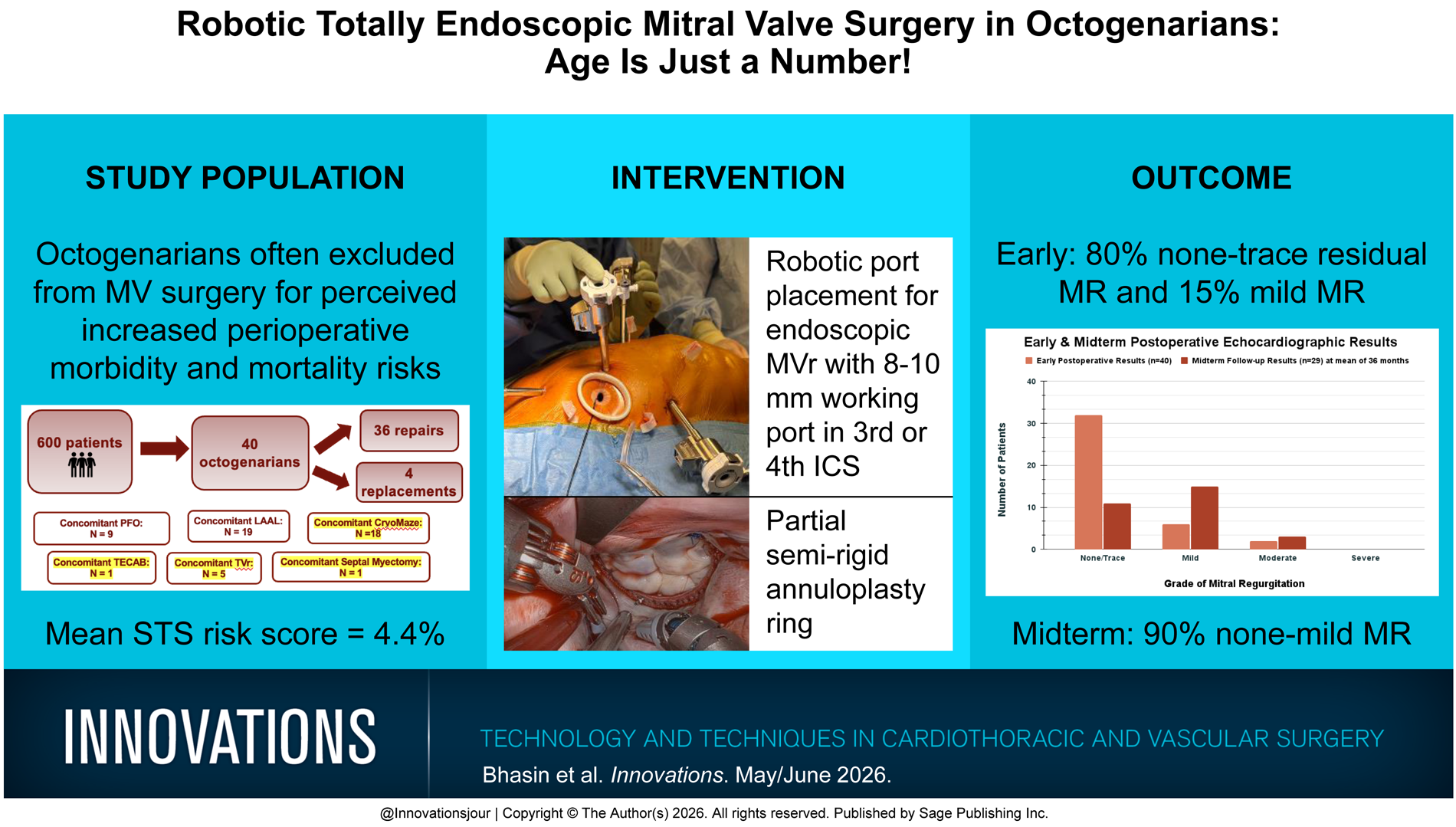
Central Message
In this study of 40patients, robotic totally endoscopic mitral valve surgery was found to be feasible, safe, and effective in octogenarians. Early outcomes and freedom from recurrent mitral regurgitation at midterm follow-up were satisfactory, providing benefits for this group of patients.
Introduction
The influence of age on outcomes in mitral valve (MV) surgery often results in many older patients, such as octogenarians, being excluded for consideration as candidates.1–3 Previous research details that the operative mortality risk quadruples between ages less than 50 years to that of 80 years and older, 4 making MV surgery sometimes considered an intervention not suitable for an older population. In studies focusing on octogenarian populations undergoing valve surgery in general, there has been a great emphasis on the fact that these patients can have considerable comorbidities, can likely require concomitant procedures, and in many cases have had previous surgical cardiac interventions on their valve, all highlighting that these cases are complicated and multifaceted. 5 Moreover, the incidence of complications such as postoperative atrial fibrillation, sepsis, and superficial and deep sternal wound infections has been recorded with higher prevalence in this subset of patients. 6 A robotic totally endoscopic approach offers an alternative that greatly lowers the probability of certain complications such as sternal wound infections due to the procedure’s nature as a minimally invasive and port-only technique.7,8
We believe that robotic MV surgery has the potential to mitigate some of the perioperative risks in an octogenarian population, allowing there to be a safe and effective option for older and higher-risk patients needing intervention. In this report, we review a series of 40 octogenarian patients who underwent robotic MV surgery and evaluated their early and midterm outcomes.
Methods
Study Population
We retrospectively reviewed all patients who underwent robotic totally endoscopic MV surgery at our institution between 2013 and 2024. A total of 600 patients underwent MV procedures, with 40 of these patients being octogenarians. Preoperative factors, along with intraoperative and postoperative data, were analyzed. Midterm clinical follow-up was conducted over the phone by contacting all patients or their cardiologist, and the latest echocardiographic results were analyzed.
Selection Criteria and Preoperative Evaluation
Patients were referred to our robotic cardiac surgery program by their cardiologist or were self-referred seeking a sternal-sparing approach. All patients suitable for MV repair or replacement were considered candidates for the robotic approach regardless of the etiology of disease. Previous sternotomy or minimally invasive cardiac surgery via right minithoracotomy was not an exclusion criterion. Contraindications to this elective procedure included emergency surgery, right lung adhesions due to previous major right lung surgery, severe coronary artery disease, and severe left ventricular dysfunction in addition to frailty and poor functional status. Preoperative echocardiographic evaluation was used to assess left ventricular function. As part of routine workup, all patients received a left heart catheterization to assess for coronary artery disease. In addition, aorto-iliac-femoral computed tomography angiography was performed to evaluate the size and pathology of the ilio-femoral vessels and aorta for peripheral cannulation.
Surgical Approach
Our operative approach for robotic endoscopic MV surgery with an 8 to 10 mm working port in the third or fourth intercostal space using soft-tissue retraction (XX-small Alexis, Applied Medical, Rancho Santa Margarita, CA, USA) has been previously described (Fig. 1).9,10 The use of the robot allows this procedure to be performed totally endoscopically and without any rib spreading in patients with a wide variety of body habitus and redo statuses. In patients undergoing MV replacement, the working port was enlarged to accommodate the prosthetic valve. General anesthesia was administered using a single-lumen endotracheal tube. Cardiac arrest was achieved using the endoballoon approach in 62.5% of patients, fibrillatory arrest for 35%, and the cross-clamp was used in 1 patient (2.5%). Although the endoballoon is our preferred method for cardiac arrest, fibrillatory arrest is used as the next option in cases in which a patient has severe peripheral vascular disease and therefore would not be a suitable candidate for cannulation for the endoballoon. In patients with peripheral vascular disease, arterial perfusion was performed using axillary cannulation. A semirigid partial annuloplasty ring was implanted using a running continuous mattress stitch (Supplemental Fig. 1).

Port placement for endoscopic mitral valve repair with 8 to 10 mm working port between the third and fourth intercostal spaces.
Results
Patient Demographics
Of 1,883 patients who underwent robotic endoscopic cardiac surgery at our institution between 2013 and 2024, 600 patients had robot-assisted MV surgeries, and of those, a total of 40 were performed in octogenarians and were the focus of this review. The mean age of the patients was 83 years, 55% were female, and 5% had previously undergone heart surgery. Of the 2 patients who underwent previous heart surgery, 1 was done via sternotomy. Prior percutaneous coronary intervention was completed in 10% of patients, and 10% had a prior MitraClip (Abbott Structural Heart, Santa Clara, CA, USA). Hypertension, hyperlipidemia, and diabetes mellitus were present in 88%, 75%, and 13%, respectively. Rates of peripheral vascular disease, history of smoking, and sleep apnea were 5%, 35%, and 13%, respectively. A total of 33% had congestive heart failure, 8% had chronic obstructive pulmonary disease, and 53% of patients had preoperative atrial dysrhythmia. Preoperative permanent pacemaker was present in 10% of patients. Prior cerebrovascular accidents had occurred in 4 patients, and 1 patient had a prior myocardial infarction. Mitral stenosis was present in 8% of patients, and 98% of patients had mitral regurgitation (MR). Degenerative MV disease was present in 87.5% of patients, whereas in the remaining 12.5% of patients, MV disease was attributed to infective endocarditis, rheumatic fever, or functional reasons. The average Society of Thoracic Surgeons (STS) predicted risk of mortality was 4.4% (range: 0.95% to 10.1%). Complete demographic information is listed in Supplemental Table 1.
Perioperative Results
Forty octogenarians had MV surgery, and 65% underwent an additional procedure, including left atrial appendage ligation (47.5%), tricuspid valve repair (12.5%), patent foramen ovale closure (22.5%), totally endoscopic coronary artery bypass (TECAB; 2.5%), ventricular septal myectomy (2.5%), and CryoMaze (45%). Of the CryoMaze procedures, 83% were localized to the left atrium, with the remaining procedures being biatrial. The mean operative time was 183 ± 52 min. There was 1 conversion to sternotomy. Intraoperative red blood cell (RBC) transfusions occurred in 18%, and inotrope usage was present in 10%. All intraoperative information is shown in Table 1.
Intraoperative Data.
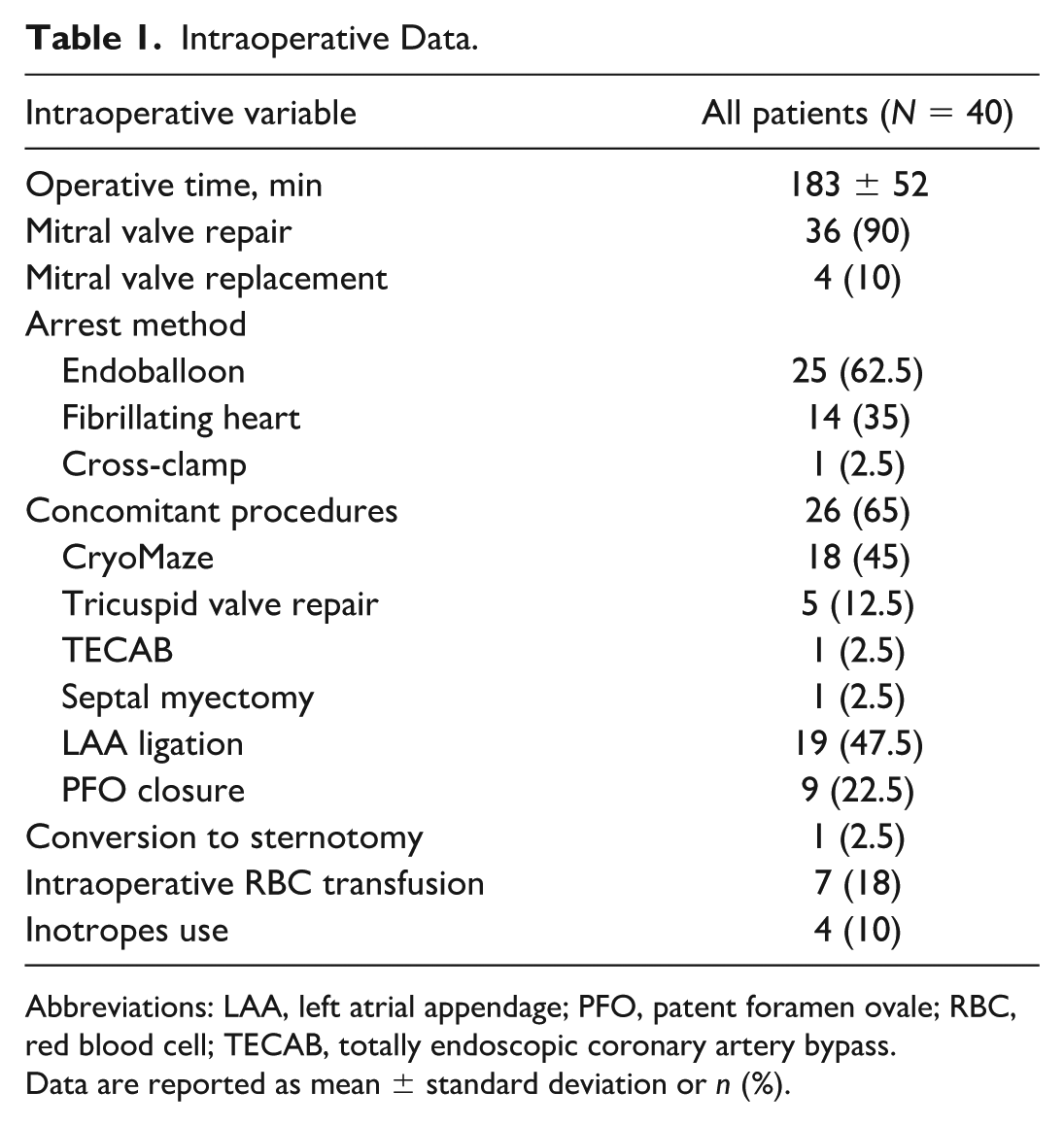
Abbreviations: LAA, left atrial appendage; PFO, patent foramen ovale; RBC, red blood cell; TECAB, totally endoscopic coronary artery bypass.
Data are reported as mean ± standard deviation or n (%).
MV repair occurred in 90% of patients, and 4 patients had a tissue valve replacement. Postoperatively, 55% of patients were extubated within 6 h and 33% within 24 h. Prolonged intubation (>24 h) occurred in 13% of patients, and 5% required reintubation. Postoperative RBC transfusion occurred in 35% of patients. Mean hospital and intensive care unit lengths of stay were 3.5 and 1.5 days, respectively. Discharge conditions included 70% of patients being discharged to home, and 30% were discharged to an acute or long-term rehabilitation facility. There were no hospital mortalities. Early postoperative outcomes can be found in Table 2.
Postoperative Outcomes.
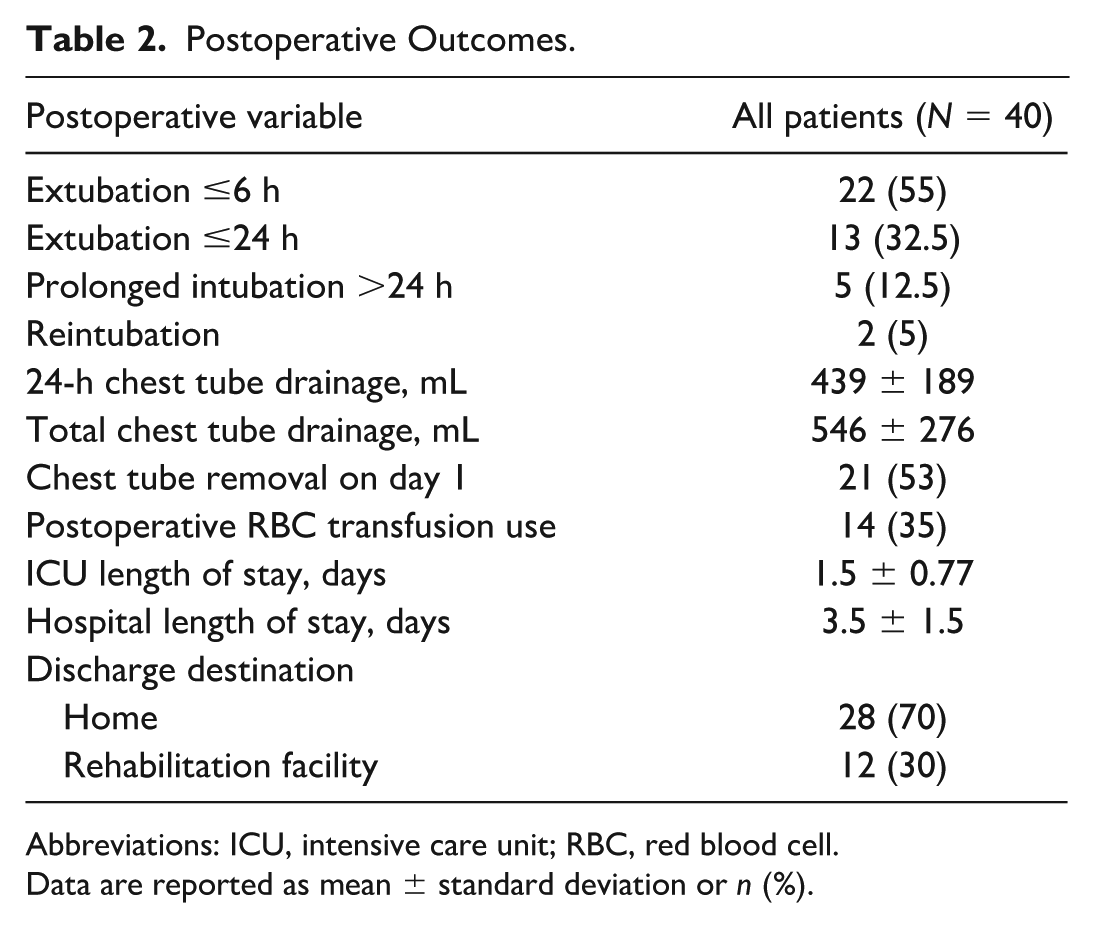
Abbreviations: ICU, intensive care unit; RBC, red blood cell.
Data are reported as mean ± standard deviation or n (%).
New incidence of atrial fibrillation was present in 15% of patients, and 5% of patients required new permanent pacemakers. There was no incidence of postoperative wound infections, pleural effusions, pericarditis, deep vein thrombosis, pulmonary embolism, or unilateral lung edema. Postoperative acute kidney injury, heart failure, pneumonia, and tracheostomy each occurred in 2.5% of patients. One patient was placed on extracorporeal membrane oxygenation (ECMO). Three patients returned to the operating room for bleeding. There was no incidence of postoperative myocardial infarction or stroke, nor were there any patient readmissions. All postoperative complications are shown in Table 3.
Postoperative Complications.
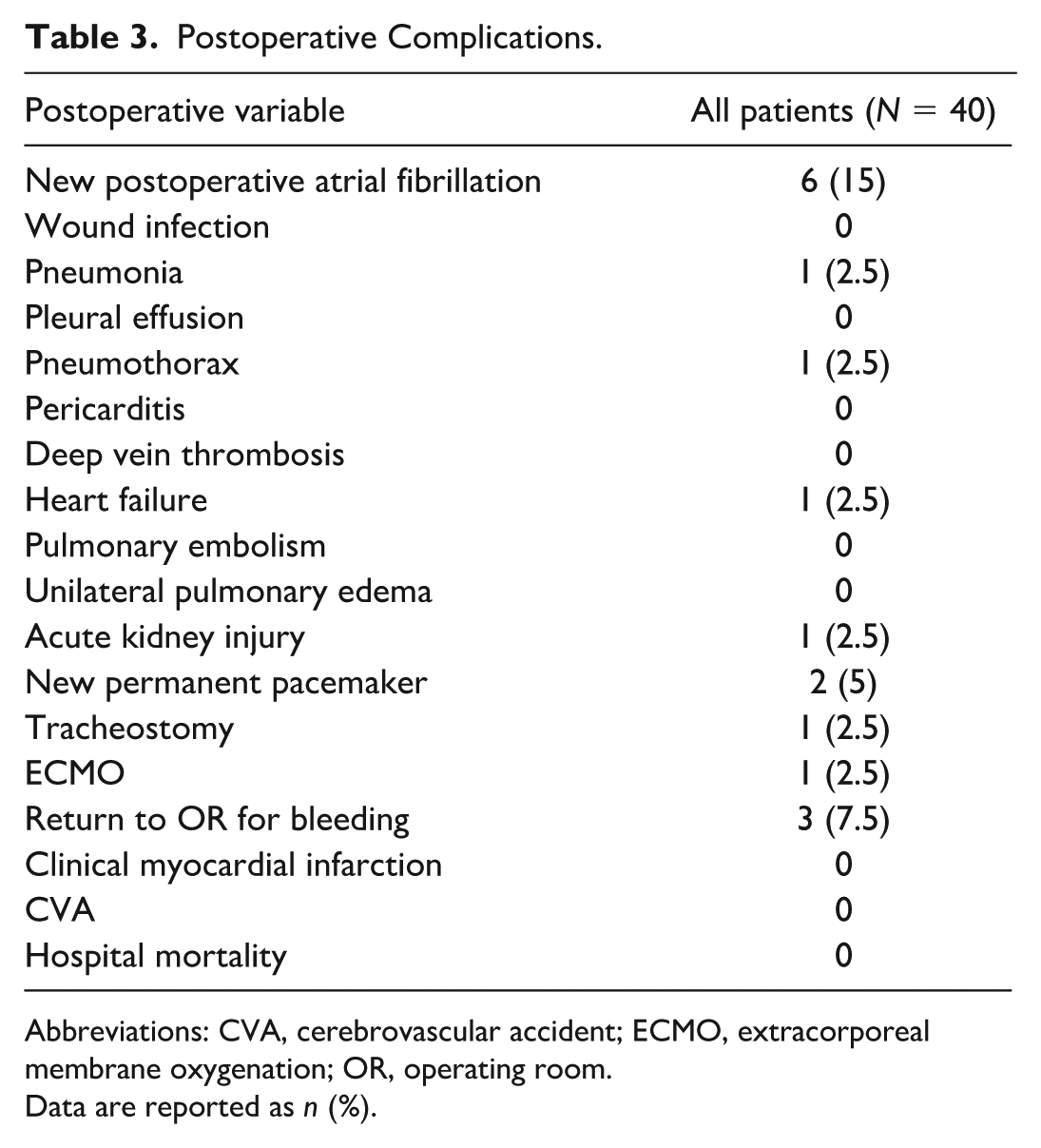
Abbreviations: CVA, cerebrovascular accident; ECMO, extracorporeal membrane oxygenation; OR, operating room.
Data are reported as n (%).
The mean time for patients to return to normal activities was 13 days. The use of opioid pain medication was discontinued by patients at a mean of 1 day after discharge. Patients were seen for follow-up in the outpatient clinic 4 to 6 weeks postoperatively, at which time an echocardiogram and chest X-ray were obtained, and surgical incisions were assessed (Fig. 2). Early postoperative echocardiography revealed none to trace residual MR in 32 patients (80%) and mild residual MR in 6 patients (15%). Moderate MR was present in 2 patients.

Incision healing at a follow-up clinic visit at 4 to 6 weeks postoperatively.
Midterm Results
Clinical follow-up was completed in 100% of patients at a mean of 37 months from surgery. All-cause mortality occurred in 9 patients (23%), 8 of which were noncardiac deaths secondary to septic shock, subarachnoid hemorrhage, brain lesion, and unknown. There were no repeat cardiac surgeries or MitraClip placements noted at this time. Follow-up echocardiography results were available for 29 patients (73%) at a mean of 36 ± 25 months, showing none to mild recurrent MR in 26 patients (90%). The mean MV gradient was found to be 3.2 ± 0.64 mm Hg for patients who underwent MV repair and 4 ± 1 mm Hg for patients who underwent MV replacement. Figure 3 displays both the initial postoperative and follow-up echocardiographic outcomes for MR. Other information on midterm outcomes from clinical follow-up is listed in Supplemental Table 2.
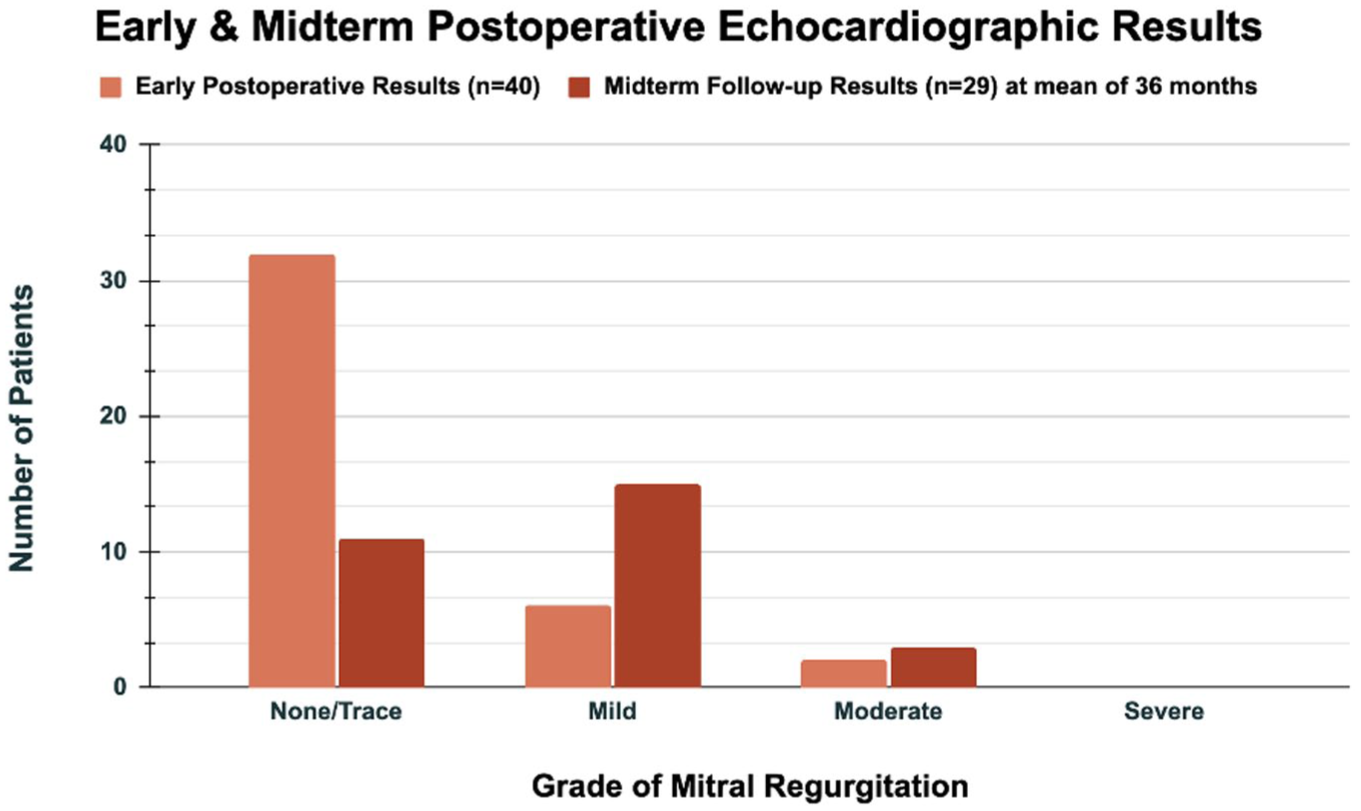
Early echocardiographic results obtained at approximately 30 days postoperatively from procedure, and midterm echocardiographic outcomes assessed at a mean follow-up of 36 months.
Discussion
Although MV surgery has been established as a safe, effective, and commonly performed procedure across many cardiac surgical programs, octogenarians can frequently be excluded from both MV repairs and replacements due to the greater number of associated perioperative risk factors. 11 This trend has been accentuated with the advent of percutaneous transcatheter interventions, which may carry less risk but are also perhaps less efficacious. In this series of 40 octogenarians undergoing robotic endoscopic MV surgery, we have demonstrated good early outcomes including no early mortalities, a mean hospital length of stay of 3.5 days, and 95% freedom from moderate or worse postoperative residual MR. Of note, 65% of these patients also underwent an additional procedure including 18 concomitant CryoMaze procedures, 1 concomitant TECAB, and 1 concomitant septal myectomy. We have previously reported our outcomes in concomitant and isolated tricuspid valve surgery, 12 and within this series, we had a total of 5 patients who underwent concomitant MV and tricuspid valve repairs. Our results compare favorably with previous studies in the literature, which have shown greater operative mortality rates with MV surgery in octogenarians, especially in cases of concomitant procedures, such as coronary artery surgery, and in cases with an increased aortic cross-clamping time. 13 A unique aspect of our robotic MV approach is that it is endoscopic with no rib spreading, which we believe minimizes postoperative pain and allows for early recovery and discharge. The 1 conversion to sternotomy in this series of patients was due to an aortic dissection, which was successfully repaired, and the patient recovered with short-term ECMO support. As part of our postoperative outcomes, we measure prolonged postoperative ventilation times as being longer than 24 h after surgery. Although this was noted in 5 patients, 3 of these patients had undergone concomitant procedures with a longer operative time, and the remaining 2 patients had a history of chronic renal insufficiency and chronic obstructive pulmonary disease. In this series, 70% of patients were discharged to home, with only 30% discharged to a rehabilitation facility. We do not feel that this number is too large given that this cohort consisted of octogenarians with a mean age of 83 years and an STS risk profile of 4.4% predicted risk. Most were discharged to acute rehab because they lived alone and did not have family support to be discharged directly home.
We are liberal with the use of nonaortic manipulation techniques for cardiac arrest, including ventricular fibrillatory arrest, which we believe minimizes perioperative complications. This approach was used in 35% of patients in this series as opposed to 21% in our recent publication describing our whole cohort of robotic MV patients over a 10-year period. 8 In that publication, we described our algorithm for choice of cannulation and arrest technique, which favors ventricular fibrillatory arrest to avoid aortic manipulation in patients with any risk factor for vascular complications, which are likely to be more prevalent in octogenarians.
Although there have been multiple studies of longer and midterm survival and reoperation outcomes to support MV repair versus replacement in patients with degenerative MV disease, 14 there has been less discussion of long-term outcomes of these procedures specifically in relation to an octogenarian population. Our clinical follow-up at a mean of 3 years shows no repeat cardiac surgeries or MitraClips, with no cardiac events and 1 cardiac-related mortality. Midterm echocardiographic data collected at a mean of 36 months postoperatively for 73% of patients also showed 90% of those patients to have none or mild residual MR. These midterm postoperative clinical and echocardiographic results speak to the effectiveness of the robotic, totally endoscopic surgical repair and its efficacy over time, for this high-risk and older population when conducted by an experienced robotic team and in the context of a multispectrum robotic cardiac program. We believe that this is important because many of the patients in this age group present with concomitant disease and/or previous cardiac surgery, which may require concomitant robotic procedures and/or reoperative surgery, as demonstrated in our series.
Limitations
This was a retrospective, single-institution study with all of the inherent biases therein. We did not have a control group for this series. In addition, the results reported in our study may not be transferable to other programs with a less experienced team in robotic cardiac surgery.
Conclusions
Our study demonstrates that robotic totally endoscopic MV surgery is feasible, safe, and effective in an octogenarian population. Our series demonstrates good early and midterm outcomes, showing the benefits this minimally invasive approach holds for higher-risk and older patients. Further studies are warranted to assess long-term data for robot-assisted MV repairs and replacements in octogenarians.
Supplemental Material
sj-docx-1-inv-10.1177_15569845261452666 – Supplemental material for Robotic Totally Endoscopic Mitral Valve Surgery in Octogenarians: Age Is Just a Number!
Supplemental material, sj-docx-1-inv-10.1177_15569845261452666 for Robotic Totally Endoscopic Mitral Valve Surgery in Octogenarians: Age Is Just a Number! by Riya Bhasin, Sarah Nisivaco, Hiroto Kitahara, Yazan AlJamal and Husam H. Balkhy in Innovations
Supplemental Material
sj-docx-2-inv-10.1177_15569845261452666 – Supplemental material for Robotic Totally Endoscopic Mitral Valve Surgery in Octogenarians: Age Is Just a Number!
Supplemental material, sj-docx-2-inv-10.1177_15569845261452666 for Robotic Totally Endoscopic Mitral Valve Surgery in Octogenarians: Age Is Just a Number! by Riya Bhasin, Sarah Nisivaco, Hiroto Kitahara, Yazan AlJamal and Husam H. Balkhy in Innovations
Supplemental Material
sj-png-3-inv-10.1177_15569845261452666 – Supplemental material for Robotic Totally Endoscopic Mitral Valve Surgery in Octogenarians: Age Is Just a Number!
Supplemental material, sj-png-3-inv-10.1177_15569845261452666 for Robotic Totally Endoscopic Mitral Valve Surgery in Octogenarians: Age Is Just a Number! by Riya Bhasin, Sarah Nisivaco, Hiroto Kitahara, Yazan AlJamal and Husam H. Balkhy in Innovations
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Balkhy is a proctor for Intuitive Surgical. All other authors have nothing to disclose.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.