
Abstract
Objective:
To evaluate the surgical outcomes of the modified right vertical infra-axillary thoracotomy (MRVIAT) technique for the treatment of various congenital heart diseases (CHDs) across all age groups.
Methods:
A retrospective analysis was performed on 1,513 patients with CHD who underwent surgery using the MRVIAT technique between January 2022 and June 2024. Incisions were 2 to 5 cm, and peripheral extracorporeal circulation was not used. Twelve primary surgical procedures were executed across all age groups.
Results:
All 1,513 patients successfully underwent surgery without the need for conversion to a median sternotomy or any in-hospital mortality. The median patient age was 1.1 years (range, 0.1 to 57 years), with 62 patients aged 18 years or older. The median weight was 9 kg (range, 1.8 to 101.6 kg), with 859 patients (56.8%) weighing ≤10 kg, 588 patients (39.9%) weighing between 10 kg and 50 kg, and 66 patients (4.4%) weighing ≥50 kg. Two patients (0.1%) required early reoperation: 1 (0.1%) due to third-degree atrioventricular block and 1 (0.1%) due to postoperative bleeding. Other postoperative complications included mild residual shunt in 20 patients (1.3%), pneumothorax in 2 patients (0.1%), wound infection in 3 patients (0.2%), and pulmonary infection in 4 patients (0.3%). The median follow-up period was 1.3 years (range, 0.3 to 2.5 years). During follow-up, no surgery-related thoracic deformities were noted.
Conclusions:
The MRVIAT technique is a safe and viable method for treating CHD patients across all age groups. This technique, which involves a smaller, less prominent incision, offers a promising alternative to median sternotomy methods.
This is a visual representation of the abstract.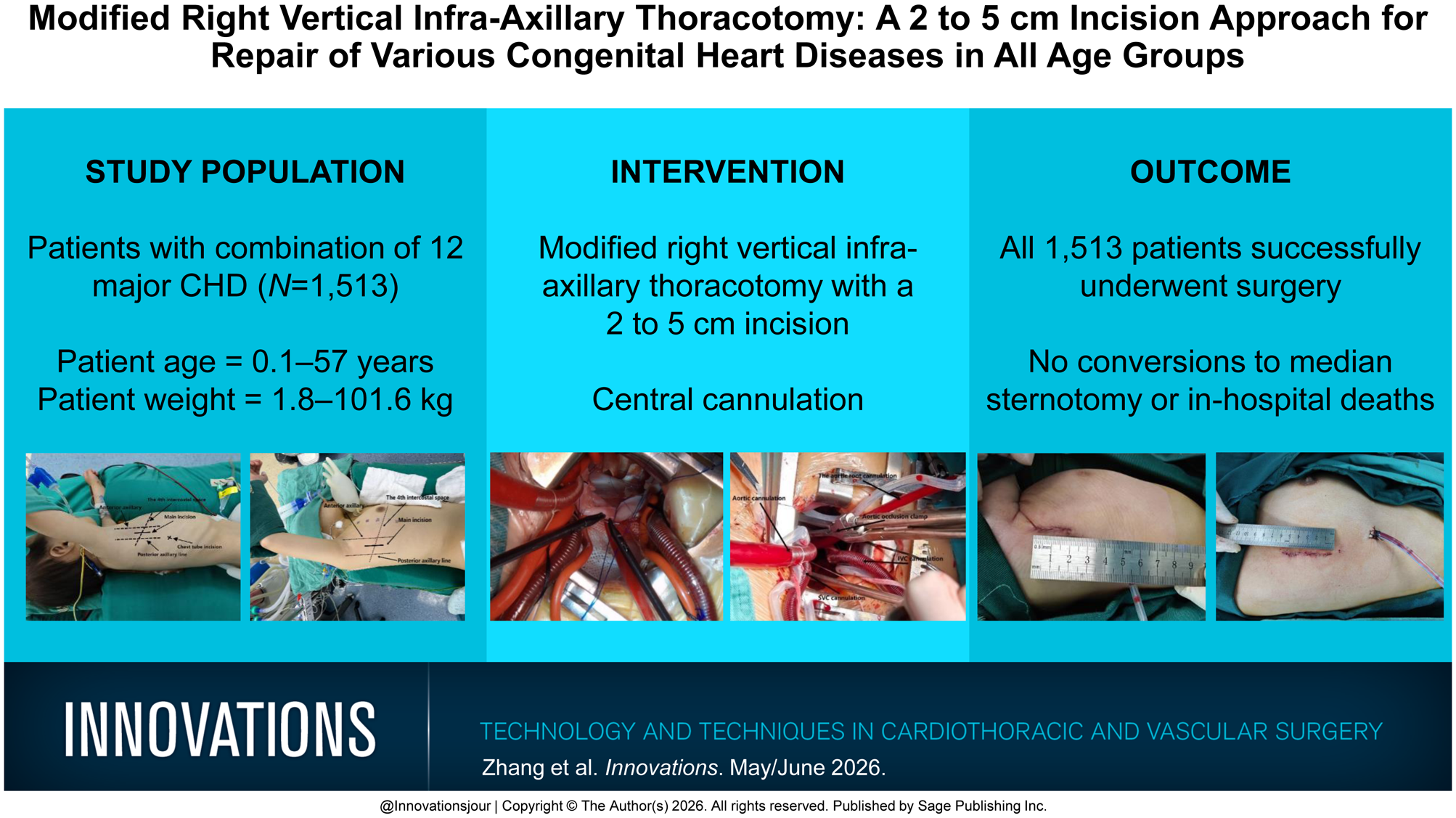
Keywords
Central Message
Modified rightvertical infra-axillarythoracotomy repairwas used to treatvarious congenitalheart diseasesacross all agegroups. Basedon postoperativeand follow-upoutcomes, thistechnique with asmaller incisionwas effectiveand safe.
Introduction
Median sternotomy has traditionally been the standard approach for correcting congenital heart disease (CHD), with well-established effectiveness. However, its esthetic drawbacks, notably the long, visible sternotomy scar, often lead to psychological distress, particularly in young female patients. 1 Consequently, minimally invasive techniques that can deliver cardiac repair outcomes comparable with median sternotomy are highly desirable. Minimally invasive cardiac surgery represents an innovative technique performed through small incisions, reducing tissue trauma relative to traditional median sternotomy. This approach minimizes hospital stay, blood product use, postoperative pain, and neurologic complications, thus improving recovery and clinical outcomes.2–4 Various minimally invasive incisions have been introduced for CHD repair, including lower sternum incisions, right submammary incisions, anterolateral and posterolateral incisions, right axillary incisions, intercostal transverse incisions, and total thoracoscopic.5–11 Among these, the right vertical infra-axillary thoracotomy (RVIAT) approach is one of the most frequently used, showing encouraging results. However, it still has certain limitations, such as restrictions in patient indications, age, weight, and methods of extracorporeal circulation. In recent years, our center has advanced this technique by developing a modified RVIAT (MRVIAT) technique, integrating the traditional RVIAT with total thoracoscopic technique and improved surgical instruments and methods of aortic occlusion. This modification has broadened the indications for the right axillary incision, making it suitable for CHD repairs that were previously limited to median sternotomy. This improved method requires only a 2 to 5 cm incision and eliminates the need for peripheral cannulation. It has successfully facilitated the repair of 12 major congenital defects, including doubly committed subarterial ventricular septal defect (VSD), Warden procedure, tetralogy of Fallot (TOF), and atrial myxoma with favorable outcomes. This retrospective study examined the short-term clinical outcomes and surgical experience associated with the MRVIAT technique.
Methods
Patient Selection and Data Collection
This observational, retrospective, single-center study included 1,513 patients with various CHDs who underwent surgery using the modified RVIAT technique between January 2022 and June 2024. All surgeries were performed by a single surgeon. Routine preoperative assessments included airway computed tomography (CT) and coronary artery evaluation to rule out any airway or coronary anomalies. All 1,513 patients met the surgical inclusion criteria.
Surgical Techniques
Following induction of anesthesia with both intravenous and inhalational agents, endotracheal intubation was performed. The patient was positioned in the left lateral decubitus position, with the right arm abducted, elbow flexed, and secured to the headrest to ensure optimal exposure of the axillary region (Fig. 1). Once draping and disinfection were complete, the right arm was released from fixation, allowing it to fall naturally A vertical incision approximately 2 to 5 cm in length was made along the midaxillary line between the third and fourth ribs, and the subcutaneous tissue was dissected. After temporarily suspending ventilation, access was gained through the third or fourth intercostal space, and an incision protector was positioned with chest retraction (Fig. 2a). The pericardium was incised longitudinally, approximately 2 cm anterior to the right phrenic nerve, and then suspended around the superior vena cava, right atrium, inferior vena cava, and ascending aorta to provide clear exposure of the heart, with an additional gauze pad to protect the lung (Fig. 2b). In adult patients or those with larger body mass (typically ≥50 kg), an additional 5 mm horizontal incision was made between the fifth and sixth intercostal spaces for thoracoscope insertion. Following heparin administration, purse-string sutures were placed on the ascending aorta and both the superior and inferior vena cavae. Aortic cannulation and metal right-angle venous cannulation were conducted, followed by insertion of venous lines for extracorporeal circulation. The sutures were securely tied around the cannulas with a venous clamp, ensuring an unobstructed surgical field (Fig. 2c, Fig. 2d). With the flow reduced, the ascending aorta was clamped (Fig. 3a, Fig. 3d, Fig. 4d). A del Nido/HTK/High K+ myocardial protective solution was then infused at the aortic root to induce cardiac arrest. The right atrium was opened, and left heart drainage was achieved through the foramen ovale. Surgical repair of the relevant congenital heart defects was then performed using established techniques (Supplemental Video 1). Using the right atrium–tricuspid valve approach, a bovine pericardial patch of appropriate size was applied to close the atrial septal defect (ASD) and membranous VSD with continuous 5-0 Prolene sutures. For doubly committed subarterial VSD, a longitudinal incision was made in the main pulmonary artery or right atrium–tricuspid valve approach. Additional procedures, including right ventricular outflow tract (ROVT) reconstruction, subvalvular aortic membrane resection, and valve repair may also have been performed as necessary. Details of the TOF correction can be found in Supplemental Video 2. The foramen ovale was closed with continuous sutures, and after thorough air removal, circulation was reestablished. Once the aortic cross-clamp (ACC) was opened, the heart typically resumed beating in sinus rhythm on its own. Post-bypass transesophageal echocardiography confirmed the absence of residual shunting and aortic valve regurgitation. Afterward, a chest drain was inserted through the thoracoscopic port on the right side (Fig. 4f). Finally, after the conventionally closed thorax, the patient was subsequently transferred back to the intensive care unit (ICU).
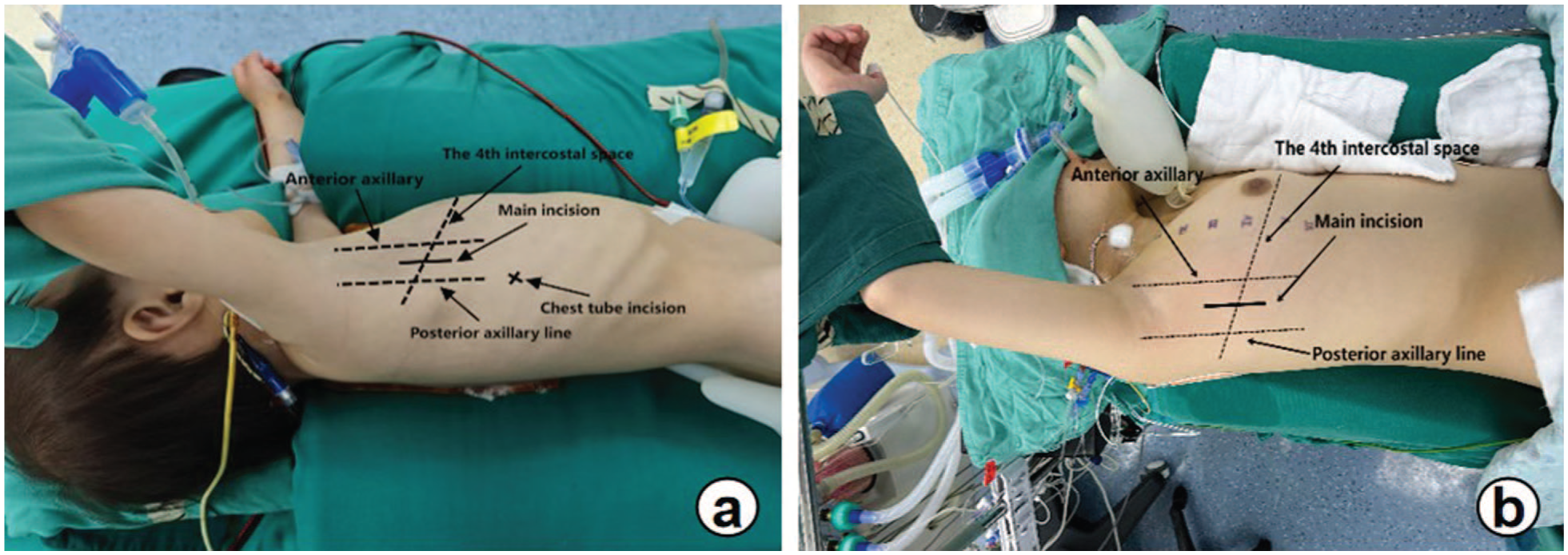
Preoperative positions and incision locations for (a) infants and (b) adults.
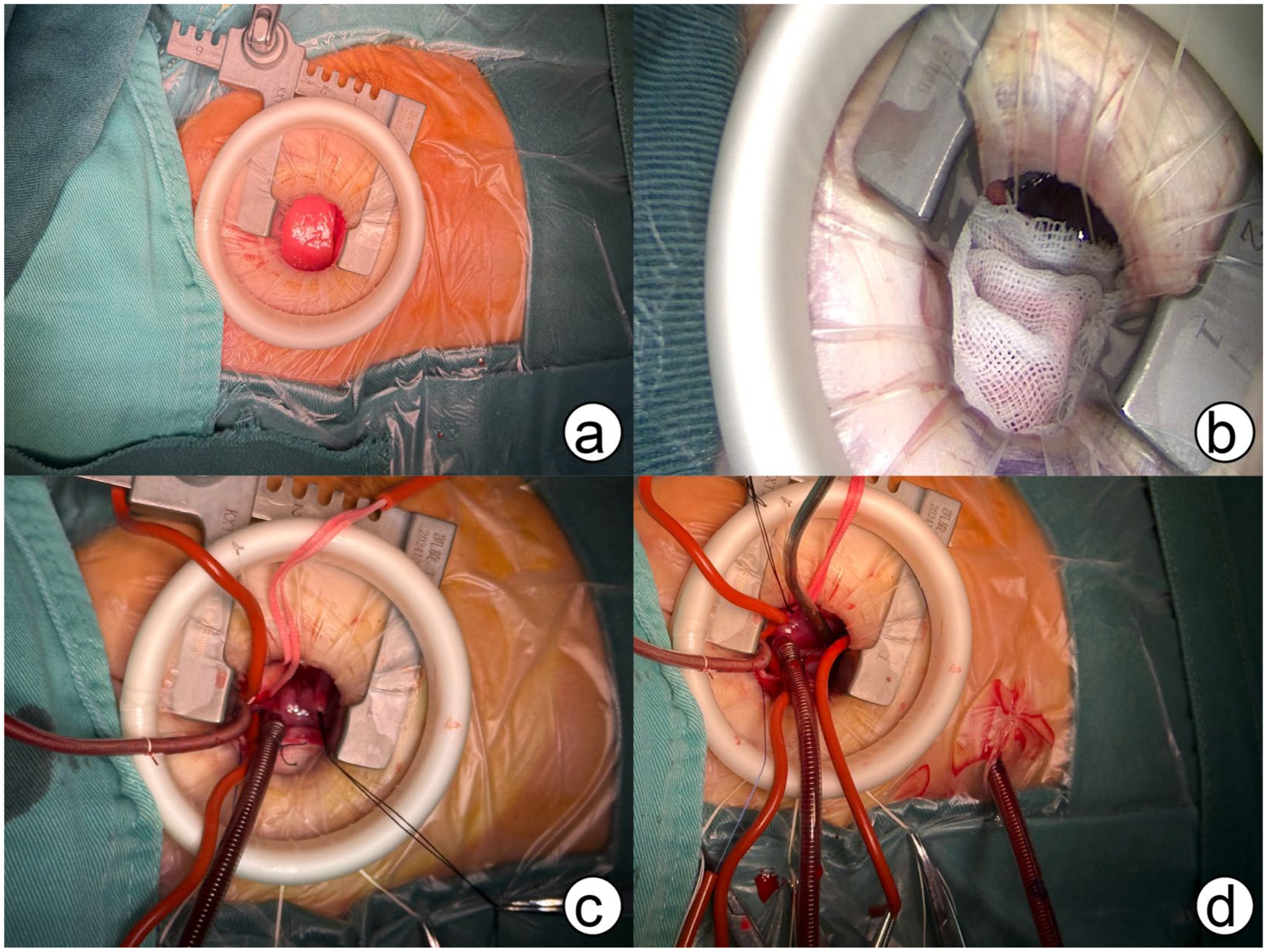
Some details of the operation.
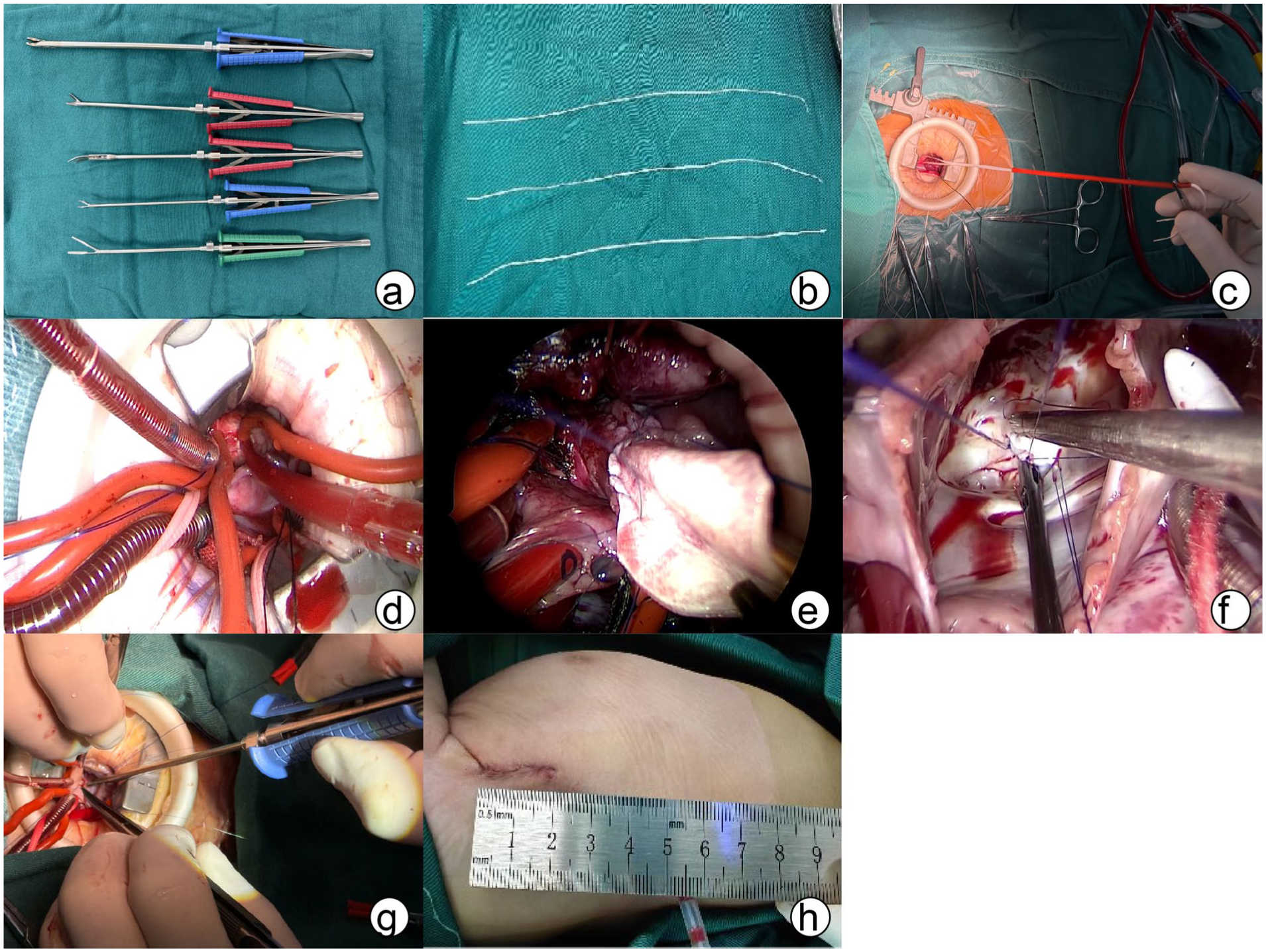
(a)(b)(c)(d) Pediatric surgical incisions and corresponding minimally invasive instruments and methods of aortic occlusion. (e) Widening of the right ventricular outflow tract. (f) Partial atrioventricular septal defect repair. (g)(h) Repair of muscular ventricular septal defect, with incision length of approximately 2 cm.
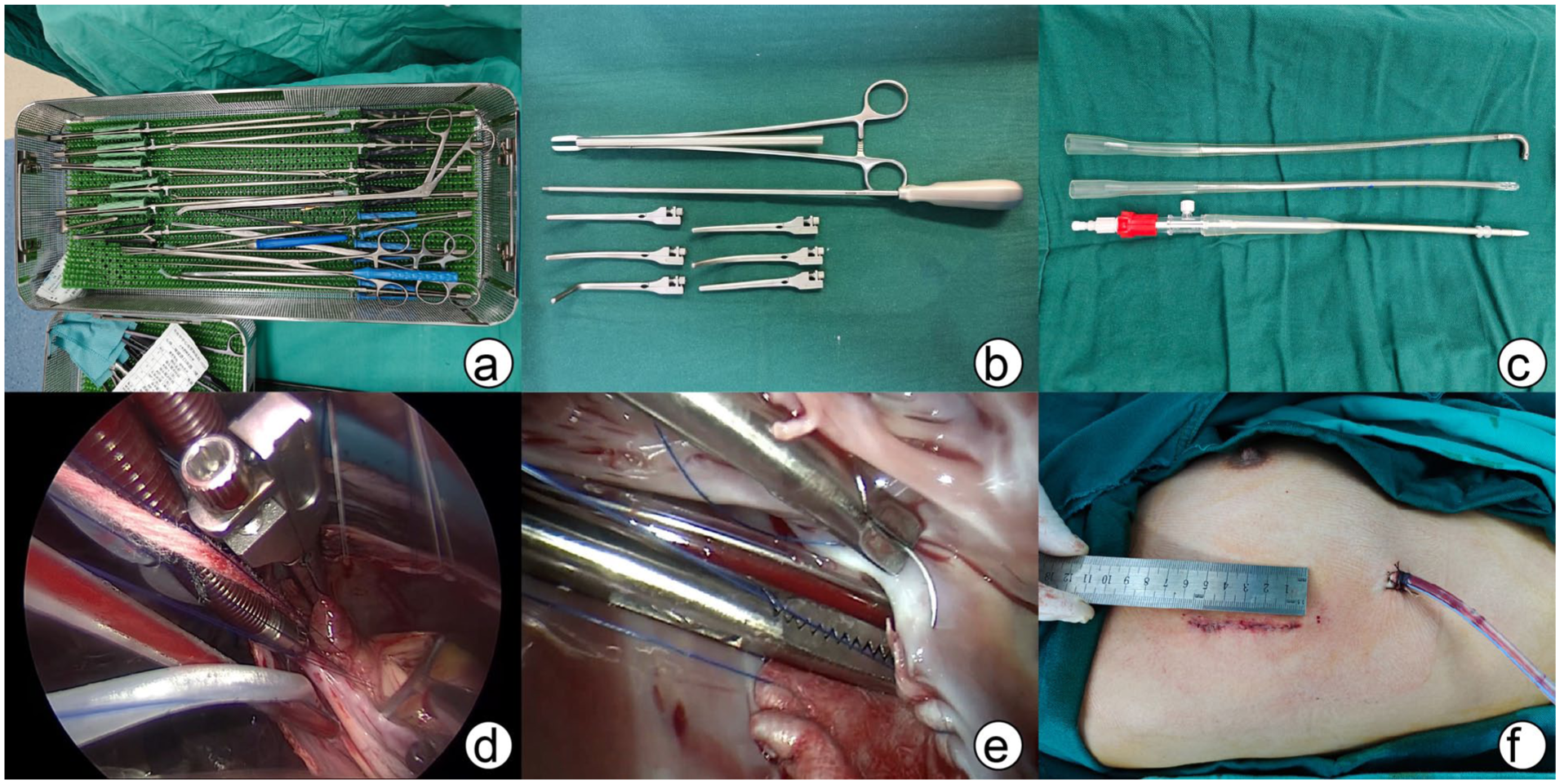
(a)(b)(c) Surgical incisions and corresponding minimally invasive instruments for patients weighing ≥50 kg. (d) Application of split-type blocking forceps during the operation. (e) Atrial septal defect repair. (f) Incision length of approximately 5 cm.
Modified Strategy
Modified surgical instruments
For patients requiring deep intracardiac operations, such as muscular VSD, partial atrioventricular septal defects, and adult CHD, long-handled minimally invasive instruments are selected for surgical operations, which can satisfy the operator in performing delicate operations in a deeper thoracic cavity. In addition, due to the thinner and longer handle, smaller incisions do not limit intraoperative operations (Fig. 3a, Fig. 3e–g, Fig. 4a).
Modified blocking method
Because traditional blocking instruments often occupy the field space when used, we modified the blocking method by using arterial blocking bands (usually ≤30 kg) to block the aorta in infants and children (Fig. 3b–d) and by using split blocking forceps to block the aorta in adults or patients with a large body mass (usually ≥50 kg) (Fig. 4b, Fig. 4d). These 2 methods of occlusion can be used in patients of all ages, greatly reducing the need for occlusion devices to occupy the intraoperative operating space and providing the operator with sufficient room to work.
Improved application strategy for extracorporeal circulation
The cannula is selected according to the theoretical basis of peripheral extracorporeal circulation, and in children, a smaller cannula is usually selected than the conventional cannula with negative pressure suction. The aortic cannula (19#) and the metal right-angle superior vena cava cannula (20#) and inferior vena cava cannula (20#) must be aspirated at the appropriate negative pressure to achieve the flow rate required for adult transfer. For aortic cannulation, an imported femoral cannula with a blunt tip (Fig. 4c) is preferred to reduce the risk of puncturing the posterior wall of the aorta during the cannulation maneuver.
Statistical Analysis
Continuous data, which were non-normally distributed, are presented as medians with interquartile ranges. Categorical data are shown as counts and percentages. Statistical analyses were conducted using IBM SPSS Software (IBM Corp., Armonk, NY, USA).
Results
Baseline Data
From January 2022 to June 2024, a total of 1,513 patients with CHD underwent correction using the MRVIAT technique (Table 1). The median age was 1.1 years (range, 0.1 to 57 years), with 738 male patients (48.8%). The median weight was 9 kg (range, 1.8 to 101.6 kg), with 154 patients (10.2%) weighing ≤5 kg, 859 patients (56.8%) weighing ≤10 kg, 588 patients (39.9%) weighing between 10 kg and 50 kg, and 66 patients (4.4%) weighing ≥50 kg. The median preoperative left ventricular ejection fraction was 68% (range, 57% to 79%). Of the 1,513 patients, 1,000 (66.1%) underwent VSD repair, including 171 (17.1%) for doubly committed subarterial VSD and 9 (0.9%) for muscular VSD. Other procedures included ASD repair in 235 patients (15.5%), TOF repair in 144 (9.5%), partial anomalous pulmonary venous (PAPVC) connection repair in 27 (1.8%), partial atrioventricular septal defect repair in 29 (1.9%), correction of tricuspid atresia in 9 (0.6%), double-chambered right ventricle resection in 14 (0.9%), double outlet right ventricle repair in 14 (0.9%), aortic valve repair in 9 (0.6%), mitral valve repair in 46 (1.6%), and atrial myxoma resection in 1 (0.1%). Additional concurrent procedures included valve repair, ROVT reconstruction, ligation of a patent ductus arteriosus, subvalvular aortic membrane resection, and others. Preoperatively, moderate or severe mitral regurgitation was observed in 53 patients (3.5%), moderate or severe tricuspid regurgitation in 62 patients (4.1%), and moderate or severe aortic regurgitation in 12 patients (0.8%).
Baseline Characteristics of Patients.
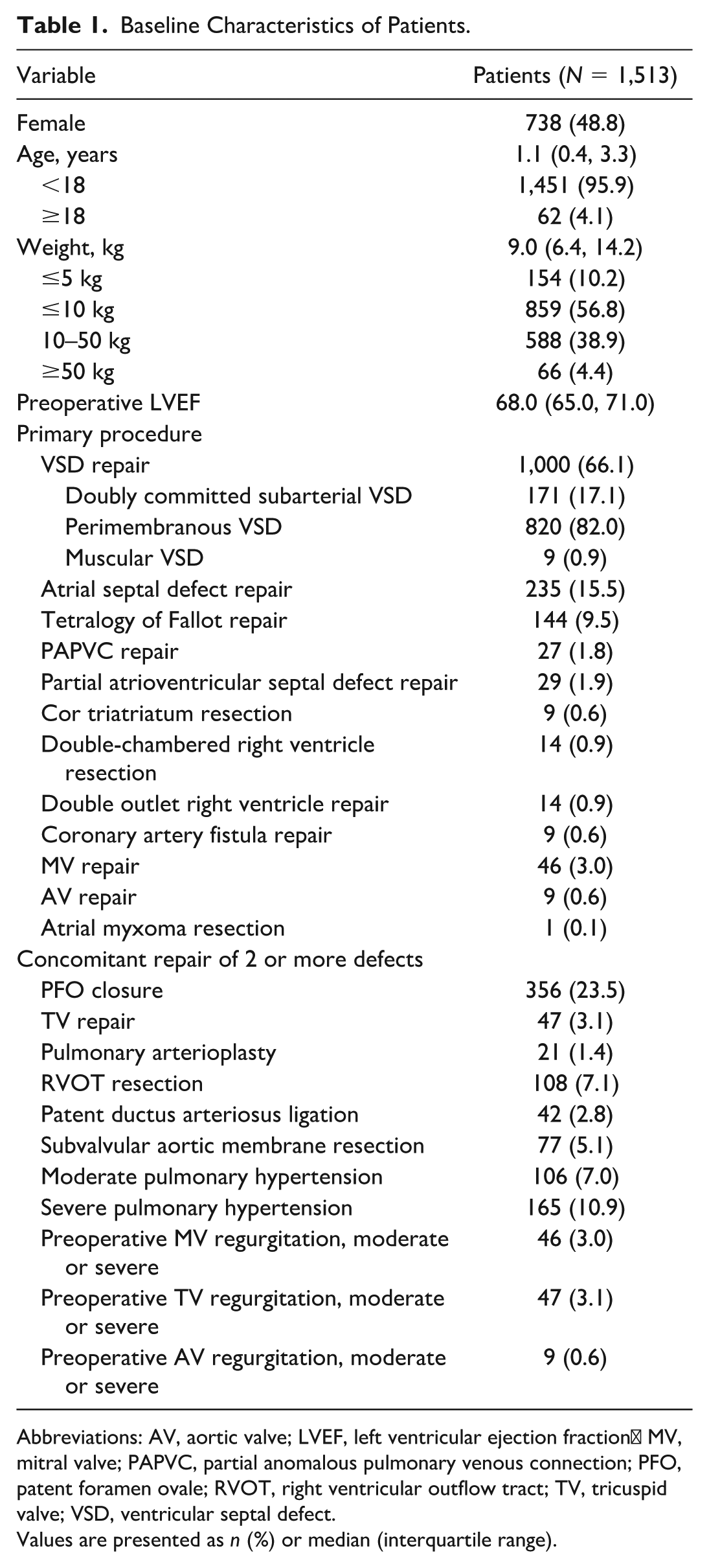
Abbreviations: AV, aortic valve; LVEF, left ventricular ejection fraction; MV, mitral valve; PAPVC, partial anomalous pulmonary venous connection; PFO, patent foramen ovale; RVOT, right ventricular outflow tract; TV, tricuspid valve; VSD, ventricular septal defect.
Values are presented as n (%) or median (interquartile range).
Perioperative Data and Complications
All 1,513 patients successfully completed the procedure without in-hospital mortality or the need for conversion to median sternotomy (Table 2). The median cardiopulmonary bypass (CPB) time was 54 min (range, 16 to 158 min), and the median ACC time was 32 min (range, 5 to 108 min). Detailed CPB and ACC times for each primary procedure are provided in the Supplemental Figure. Postoperatively, the median hospital stay was 7 days (range, 5 to 19 days), the median duration of mechanical ventilation was 0.3 days (range, 0.3 to 5 days), and the median ICU stay was 1.7 days (range, 0.3 to 6.1 days). Two patients (0.1%) required early reoperation. One patient developed third-degree atrioventricular block unresponsive to medical antiarrhythmic treatment. A second surgery via the original approach was performed to adjust the suture position, resolving the arrhythmia and restoring sinus rhythm. Another patient experienced postoperative bleeding, which was controlled through a second surgery via the original incision to achieve hemostasis. Additional postoperative complications included mild residual shunting in 20 patients (1.3%, all related to VSD repair), pneumothorax in 2 patients (0.1%), wound infection in 3 patients (0.2%), and pulmonary infection in 4 patients (0.3%). There was no recurrent left ventricular outflow tract obstruction, and all complications were managed successfully through debridement, wound closure, chest tube drainage, and antibiotic treatment, with all patients recovering and discharged in stable condition.
Perioperative Results.
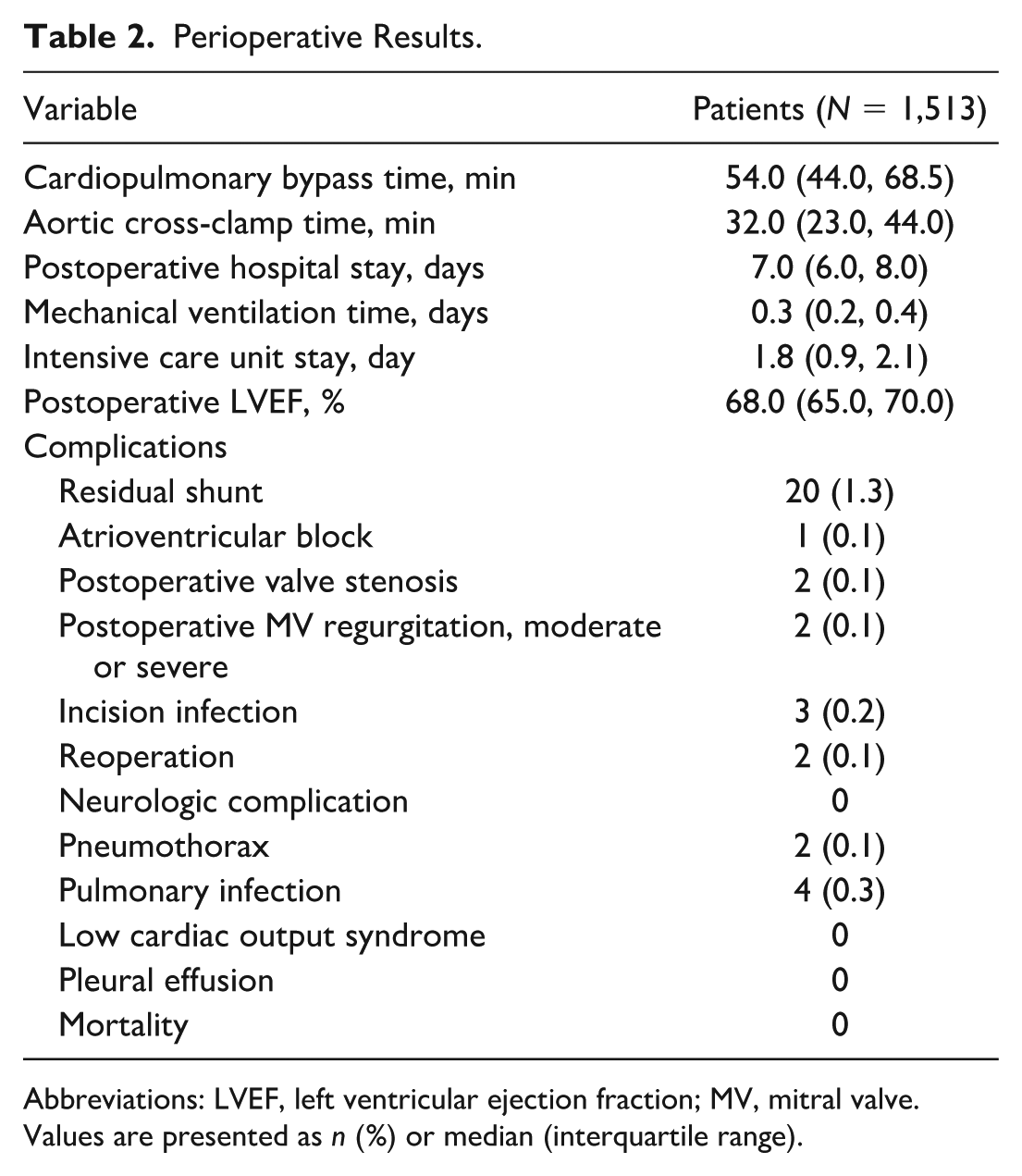
Abbreviations: LVEF, left ventricular ejection fraction; MV, mitral valve.
Values are presented as n (%) or median (interquartile range).
Outcomes of Postoperative Follow-Up
Follow-up was conducted in person at the outpatient clinic or by telephone. Routine echocardiographic evaluations were performed at 1, 3, 6, and 12 months postoperatively and annually thereafter. The median follow-up duration was 1.3 years (range, 0.3 to 2.5 years). No surgery-related chest deformities were observed during follow-up, and postoperative scar photographs of infants, adolescents, and adults are shown in Figure 5. Two patients (0.1%) who underwent repair for TOF developed pulmonary stenosis and were treated successfully with balloon pulmonary valvuloplasty, showing favorable outcomes at follow-up. In addition, 2 patients (0.1%) with moderate mitral regurgitation continued to require regular follow-up.
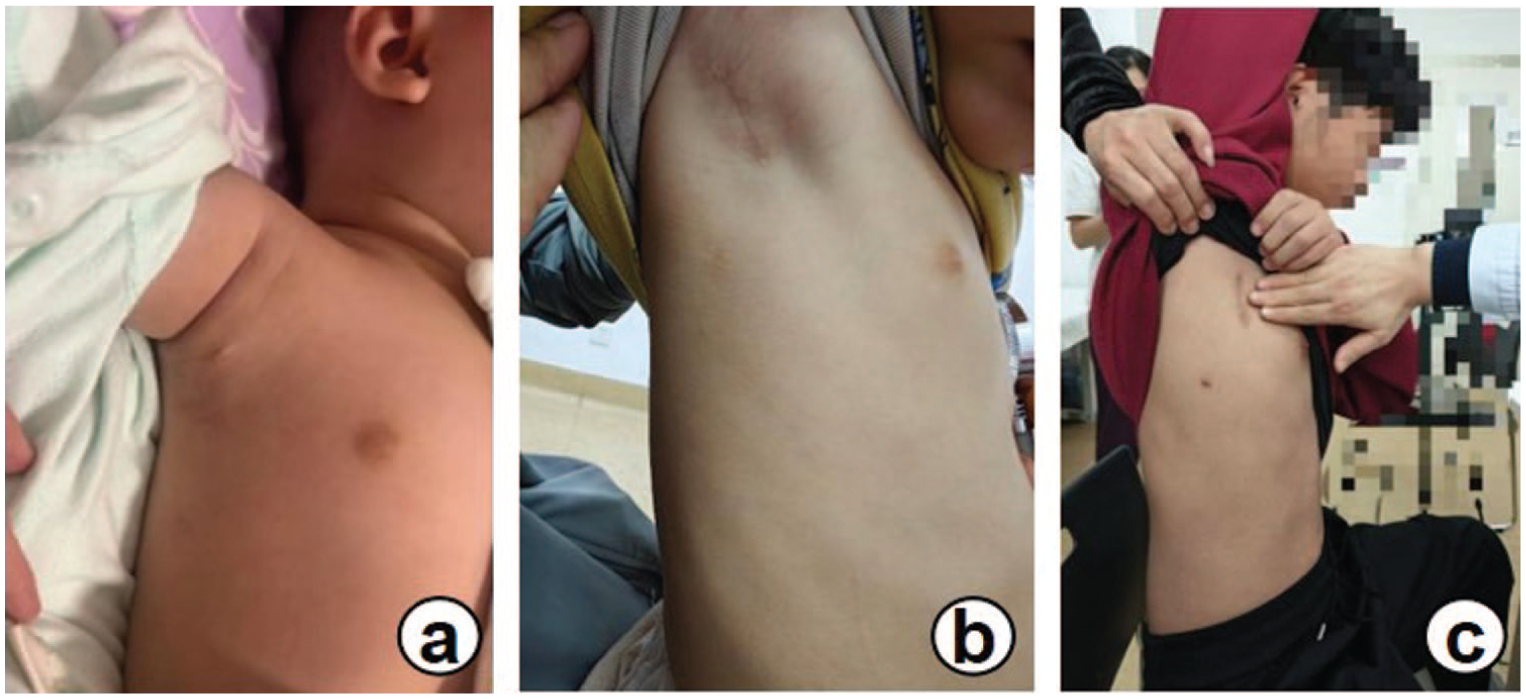
The incision scar “disappears” 3 months after surgery.
Discussion
The traditional median sternotomy, a well-established approach in cardiovascular surgery, offers excellent exposure for various cardiac procedures. However, it also entails substantial trauma, significant blood loss, prolonged hospital stays, an elevated risk of wound infections, and prominent scarring, which can significantly affect patients psychologically.12,13 As cardiac surgery safety advances, there is an increasing emphasis on reducing surgical trauma and improving cosmetic results. In clinical practice, many patients and their families seek minimally invasive incisions to improve esthetic outcomes and lessen psychological effects, particularly in children. The use of minimally invasive techniques in CHD surgery has primarily aimed to improve cosmetic outcomes, reduce postoperative pain, shorten recovery time, and decrease hospital stays.5–11 Of these, the cosmetic benefits are the most objectively measurable, providing clear advantages in patient satisfaction. 14 Initially, the RVIAT was primarily used in children and adolescents for ASD and membranous VSD repairs. With advancements in the technique and smaller right axillary incisions, indications have expanded to include valve repairs, TOF, PAPVC, and other conditions. 15 However, reports have also noted longer incisions, extended CPB times, and limitations related to patient age, weight, and disease type.6,12,16,17 Currently, most centers employ peripheral CPB strategies for adult patients or those with higher body weights in CHD surgery.17–19 Despite the widespread adoption of peripheral cannulation techniques, most cardiac surgeons continue to prefer cannulation of the ascending aorta. Peripheral cannulation, although well established, carries risks such as retrograde dissection, embolism, and limb ischemia, especially with femoral cannulation. One study noted a stroke incidence of 1.17% associated with femoral cannulation.2,20 Additional reports indicate that femoral arterial cannulation without preventive measures may lead to limb ischemia, potentially affecting survival rates or long-term functional outcomes. 21 A follow-up study by Xu et al. on 62 patients who underwent total thoracoscopic ASD closure at our institution found that 2 patients expressed dissatisfaction with the scar length resulting from femoral cannulation. 22 In adults, the depth of the thoracic cavity and reduced rib flexibility present additional challenges for surgical exposure compared with pediatric cases. Consequently, individuals weighing more than 30 kg were initially considered unsuitable for this approach. 12 However, with increasing experience and improvements in surgical instrumentation, greater body weight is no longer seen as a contraindication. Our study supports this, including a patient weighing up to 101.6 kg (Fig. 4h). Furthermore, advancements in technology have enabled fully thoracoscopic heart surgery to be conducted without the need for the da Vinci system (Intuitive Surgical, Sunnyvale, CA, USA). Total thoracoscopic techniques now require only 3 small incisions (1.0 to 2.5 cm). 23
We have integrated key technical insights from RVIAT and thoracoscopic approaches, combining the traditional RVIAT with thoracoscopic instruments to establish the MRVIAT technique. This approach offers several advantages:
Minimally invasive incision. The incision is small, vertical, and situated near the axilla, providing significant cosmetic benefits (Fig. 5a–c).
Central CPB. All procedures used central CPB, avoiding complications associated with peripheral CPB cannulation.
Broad applicability. The technique overcomes limitations typically associated with age, body weight, and defect type. Although most studies focus on VSD and ASD repair, our series includes repairs of 12 major heart defects, with patients ranging from 0.1 to 57 years old and weighing between 1.8 and 101.6 kg.
Short learning curve. This technique is relatively easy to master, with minimal disruption to the surgical habits of cardiac surgeons specializing in CHD. Central CPB via this incision is no more challenging than with the median sternotomy. With practice, the operative time may be shorter than median sternotomy, as it avoids complex chest opening and closure as well as extended hemostasis.
No postoperative deformities. This approach does not require sternal division and avoids damage to breast tissue, preserving normal breast development and eliminating postoperative breast or sternal deformities often seen with other approaches.
Reduced postoperative pain. Chest muscles and nerves are preserved, with only partial muscle dissection. The intercostal space is only slightly widened, with the soft-tissue retractor facilitating the expansion, minimizing postoperative pain. In addition, serratus anterior muscle nerve blocks are administered before or after surgery to further ease discomfort.
Our findings indicate that the MRVIAT technique is a safe and effective treatment for CHD across all age groups, with no early or late mortality and no cases requiring conversion to median sternotomy, aligning with outcomes reported globally.6,12,16,17,19,24 The RVIAT has also been successfully adopted by several other centers (Supplemental Table).6,12,16,17,19,24 Compared with previous studies, our MRVIAT technique offers a broader range of indications, effectively overcoming traditional age and weight limitations. With a single 2 to 5 cm incision and central CPB, we can address a wide spectrum of congenital heart defects, not only ASD and VSD, but also concurrent conditions, such as mitral valve repair, tricuspid valve repair, aortic valve repair, RVOT, and subvalvular aortic membrane resection, in a single procedure. Our incisions are significantly shorter than those used by most other centers, and there is no requirement for peripheral CPB. This is largely attributable to the following factors:
Improved surgical instruments and methods of aortic occlusion. These instruments (Fig. 3a, Fig. 4a) provide excellent exposure, essential for the successful repair of deep-seated heart defects, particularly in patients with a larger body mass. In addition, we use occlusion bands and split-type occlusion clamps (Fig. 3b, Fig. 4b) to block the aorta, which improves visibility and avoids the suboptimal exposure often associated with traditional clamps.
Thoracoscopic assistance. In patients with a larger body mass, the depth of the thoracic cavity and limited rib elasticity make adequate exposure challenging, as headlamps alone may not provide sufficient lighting. To address this, we use a thoracoscope inserted between the sixth and seventh ribs, which illuminates the chest cavity and greatly improves visibility for precise, intricate procedures. When the surgery nears completion, a drainage tube can be positioned through this port.
Use of surgical sutures, nerve hooks, and auxiliary exposure tools. Effective use of these tools is critical for optimal exposure. For example, during the repair of doubly committed subarterial VSD, we typically use sutures to suspend the tricuspid valve leaflets and pulmonary artery, reducing the need for the assistant’s hand and ensuring that the incision remains minimal while maintaining clear exposure. This technique promotes both procedural safety and a minimal incision size. We now routinely apply the modified right axillary vertical small incision approach to treat most congenital heart defects. However, certain limitations remain. For example, in children with TOF and an underdeveloped pulmonary artery (McGoon ratio <1.5), as well as in cases of complete atrioventricular septal defect and total anomalous pulmonary venous connection, we generally prefer a median sternotomy for optimal repair, particularly when a secondary surgery may be required to ensure the best surgical outcomes. Notably, for TOF repairs using the MRVIAT technique, we prioritize preserving the native pulmonary valve whenever possible. Current follow-up results are promising, with only 2 cases of postoperative pulmonary valve stenosis. Both patients achieved normal pulmonary valve velocities following balloon dilation, and follow-up has shown stable, normal velocities. RVIAT is increasingly becoming a standard approach for CHD repair. Continued refinement and optimization of RVIAT will help reduce surgical complexity, enabling more CHD patients to benefit from excellent surgical outcomes with minimal scarring, truly advancing the goals of minimally invasive cardiac surgery.
Conclusions
The MRVIAT technique is a safe and viable method for treating CHD patients across all age groups. This technique, which involves a smaller, less prominent incision and avoids peripheral extracorporeal circulation, offers a promising alternative to median sternotomy methods.
Supplemental Material
sj-docx-1-inv-10.1177_15569845261453374 – Supplemental material for Modified Right Vertical Infra-Axillary Thoracotomy Technique: A 2 to 5 cm Incision Approach for Repair of Various Congenital Heart Diseases in All Age Groups
Supplemental material, sj-docx-1-inv-10.1177_15569845261453374 for Modified Right Vertical Infra-Axillary Thoracotomy Technique: A 2 to 5 cm Incision Approach for Repair of Various Congenital Heart Diseases in All Age Groups by Heqi Zhang, Hua Cao, Weijie Liang, Haoju Dong, Shubo Song and Taibing Fan in Innovations
Supplemental Material
sj-docx-2-inv-10.1177_15569845261453374 – Supplemental material for Modified Right Vertical Infra-Axillary Thoracotomy Technique: A 2 to 5 cm Incision Approach for Repair of Various Congenital Heart Diseases in All Age Groups
Supplemental material, sj-docx-2-inv-10.1177_15569845261453374 for Modified Right Vertical Infra-Axillary Thoracotomy Technique: A 2 to 5 cm Incision Approach for Repair of Various Congenital Heart Diseases in All Age Groups by Heqi Zhang, Hua Cao, Weijie Liang, Haoju Dong, Shubo Song and Taibing Fan in Innovations
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Henan Province Medical Science and Technology Research Project, China (Grant Nos. SBGJ202502021 and SBGJ202001005).
Ethics Statement
Our study was conducted in accordance with the ethical principles outlined in the WMA Declaration of Taipei, and the study was approved by the ethics committee of Zhengzhou University Central China Fuwai Hospital (institutional review board approval date August 14, 2024, approval code: [2024] Lun Shen 64). Being a retrospective observational study, no interventions or modifications were made to the standard clinical practice during the data collection process. All procedures adhered to ethical guidelines for the collection, storage, and use of research data for scientific purposes. Due to the retrospective nature of this study, patient informed consent was waived.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.