
Abstract
Objective:
Video-assisted thoracoscopic surgery (VATS), via multiportal and uniportal approaches, has largely replaced thoracotomy for lung cancer surgery. However, the comparative effectiveness of these techniques in optimal lymph node dissection remains under active investigation.
Methods:
A retrospective review included 763 patients who underwent lung resection for primary lung cancer between October 2001 and January 2024. Demographic, clinical, and pathological data were collected. Patients were stratified into 3 VATS learning phases: early (2001 to 2016), intermediate (2017 to 2020), and late (2021 to 2024). Propensity score matching (PSM; 1:1) was performed based on age, gender, tumor-node-metastasis staging, and preoperative mediastinal staging status. The number of dissected lymph nodes among groups was compared using the Kruskal–Wallis test.
Results:
Six hundred patients (78.3%) were male, with a mean age of 61.28 ± 10.18 years. In this cohort, 469 patients (61.2%) underwent thoracotomy, 147 (19.2%) multiportal VATS, and 150 (19.6%) uniportal VATS. The mean number of dissected lymph nodes was 22.1 ± 17.2 for thoracotomy, 16.8 ± 11.1 for multiportal VATS, and 12.8 ± 10.8 for uniportal VATS (P < 0.001). After PSM, mean lymph node counts were 21.0 ± 18.5, 17.4 ± 11.5, and 13.4 ± 11.1 for thoracotomy, multiportal, and uniportal VATS, respectively (P < 0.001). In the late phase, thoracotomy had a higher mean lymph node count (P = 0.006); however, after PSM, differences were not statistically significant (P = 0.158).
Conclusions:
Thoracotomy allows more extensive lymphadenectomy in lung cancer patients. However, following the learning curve, multiportal and uniportal VATS approaches may yield comparable outcomes.
This is a visual representation of the abstract.
Central Message
Lymph node dissection quality remains a key focus in thoracic surgery. Although thoracotomy achieved higher lymph node counts, the difference with VATS diminished in the late learning phase. These findings suggest that adequate lymph node dissection is attainable with sufficient experience in VATS techniques.
Introduction
Since the first report of lobectomy via video-assisted thoracoscopic surgery (VATS) performed by McKenna, 1 this technique has been demonstrated as safe, feasible, and comparable to thoracotomy in terms of oncologic outcomes. 2 Over the following years, given its association with fewer complications, improved quality of life, shorter hospital stays, and better compliance with adjuvant treatment,3–5 VATS has increasingly replaced thoracotomy in most cases of lung cancer surgery.6,7
Thorough lymph node dissection is a cornerstone of oncologic integrity in lung cancer surgery, playing a critical role in staging, prognostication, and guiding adjuvant therapy. With the increasing adoption of VATS for anatomical lung resections, concerns have been raised regarding the adequacy of lymphadenectomy compared with traditional thoracotomy. Although VATS offers significant advantages in terms of reduced postoperative pain, shorter hospital stays, and faster recovery, its minimally invasive nature poses potential limitations in achieving comprehensive nodal evaluation. Several studies have investigated the quality of lymph node dissection in VATS, focusing on parameters such as the number of stations sampled, total nodes retrieved, and the adherence to established guidelines.8,9 After more than 30 years of experience with VATS lobectomy, there is still discrepancy regarding the quality of lymph node dissection achieved by VATS.8–11 Moreover, uniportal VATS, which is a less invasive method with surgical and oncologic outcomes equivalent to the multiportal approach, has also been a subject of investigation regarding lymph node dissection.12,13
In this study, we aimed to evaluate the trend in lymph node dissection throughout the learning curve of multiportal and uniportal VATS in our institution, in comparison with thoracotomy.
Methods
A total of 763 patients who underwent lung resection with the diagnosis of lung cancer in our institution between October 2001 and January 2024 were retrospectively reviewed. The recorded variables included age, gender, surgical approach, preoperative mediastinal staging status, pathological tumor-node-metastasis (TNM) staging, and the number of dissected lymph nodes or lymph node pieces as reported in the pathology report. The 8th edition of the TNM staging was used. 14 Patients with T1–4N0–1M0 non-small cell lung cancer (NSCLC) and selected cases with brain or adrenal oligometastasis (M1a) were operated. According to our institutional strategy, we did not operate on patients with N2 to N3 disease pathologically proven by preoperative invasive mediastinal staging without oncologic treatment. An endobronchial ultrasound-guided transbronchial needle aspiration, videomediastinoscopy, or videomediastinoscopic mediastinal lymphadenectomy was performed to assess mediastinal lymph node involvement in patients with cT2 to cT4 and/or cN1 to cN3 NSCLC. Thoracotomy was performed using either a posterolateral or muscle-sparing approach with placement of a Finochietto retractor. Multiportal VATS was performed through 2 or 3 ports including a 4 cm utility incision, depending on the surgeon’s preference. Uniportal VATS was performed through a 4 to 5 cm incision at the anterior axillary line at the fifth intercostal space without rib spreading. All patients underwent systematic nodal sampling or dissection in compliance with European Society of Thoracic Surgeons guideline. 15
The VATS program was initiated in 2011, and the uniportal VATS approach was introduced in our institution in 2014, with increasing adoption after 2016. A total of 6 surgeons were responsible for the cases, all of whom were senior surgeons; 1 surgeon exclusively performed the uniportal VATS approach, whereas the others preferred the multiportal VATS technique. All patients were stratified into 3 categories according to the learning phases of VATS: early phase (2001 to 2016), intermediate phase (2017 to 2020), and late phase (2021 to 2024). The early learning phase in our study included 58 multiportal and 31 uniportal VATS cases. In the intermediate phase, the cumulative numbers amounted to 97 multiportal and 94 uniportal VATS cases. With the accumulation of 97 multiportal and 94 uniportal cases in the intermediate phase, increasing proficiency enabled us to manage more complex cases. Later, a propensity score matching (PSM) analysis was applied matching for age, gender, TNM staging, and preoperative surgical mediastinal staging status, in a 1:1 ratio for thoracotomy and VATS groups. The number of dissected lymph nodes across the 3 groups was compared using the Student’s t test and the Kruskal–Wallis test. A P value <0.05 was considered statistically significant.
Results
In this cohort, 597 patients (78.2%) were male, and the mean age was 61.2 ± 10.1 years. Most patients underwent preoperative surgical mediastinal staging (n = 485, 63.6%), and thoracotomy was the most commonly preferred surgical approach (n = 469, 61.5%). A total of 83 patients (10.8%) had neoadjuvant systemic chemotherapy. The mean number of dissected lymph nodes during resectional surgery was 19.3 ± 16.0 in the overall cohort. The demographic and clinical features of all patients are summarized in Table 1.
Demographic and Clinical Features.
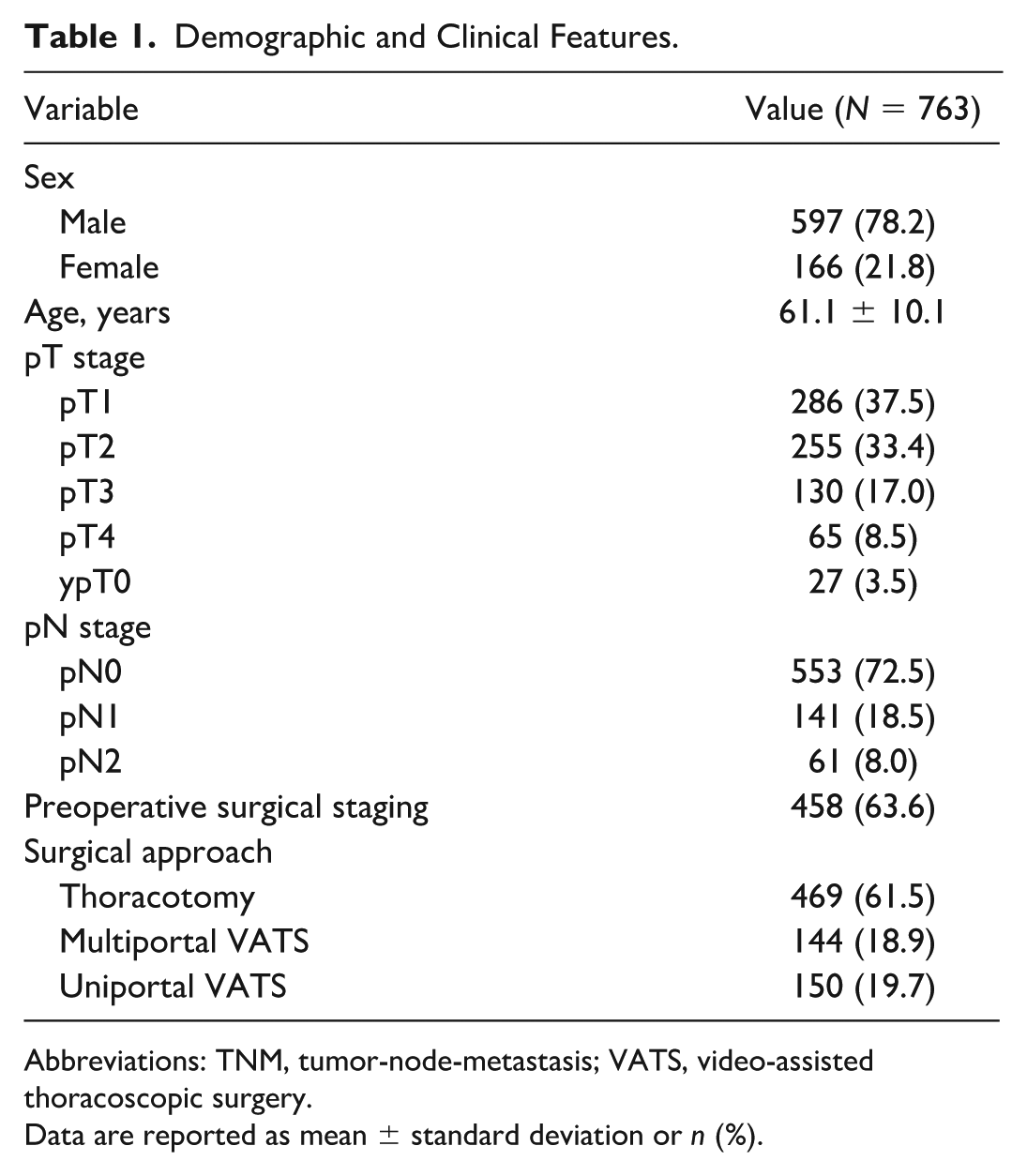
Abbreviations: TNM, tumor-node-metastasis; VATS, video-assisted thoracoscopic surgery.
Data are reported as mean ± standard deviation or n (%).
The mean number of dissected lymph nodes in the thoracotomy group was 22.1 ± 17.2, 16.8 ± 11.1 in the multiportal VATS group, and 12.8 ± 10.8 in the uniportal VATS group (P < 0.001). The early learning phase group included 426 patients (55.8%), followed by 179 (23.5%) in the intermediate phase group, and 158 (20.7%) in the late phase group. Figure 1 shows the percentage distribution of surgical approaches among learning phases. In all phases, the mean number of dissected lymph nodes was significantly higher in the thoracotomy group (P = 0.001, P < 0.001, and P = 0.006, respectively; Fig. 2a).
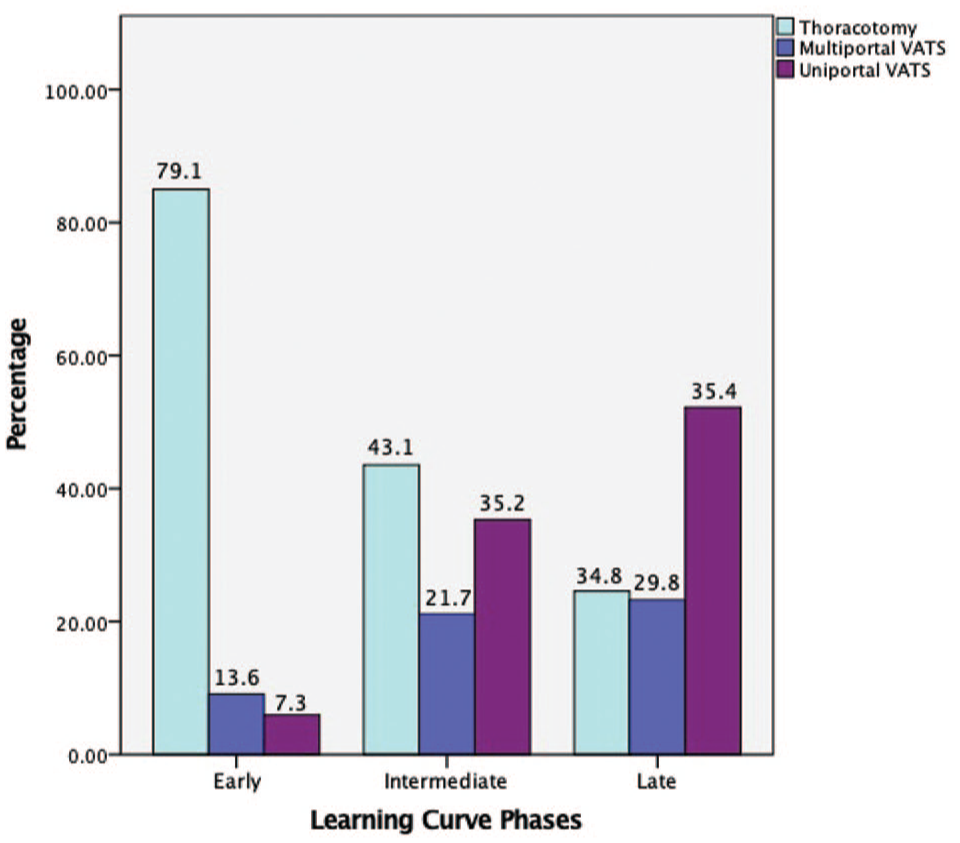
Proportions of surgical approaches in different learning phases. VATS, video-assisted thoracoscopic surgery.
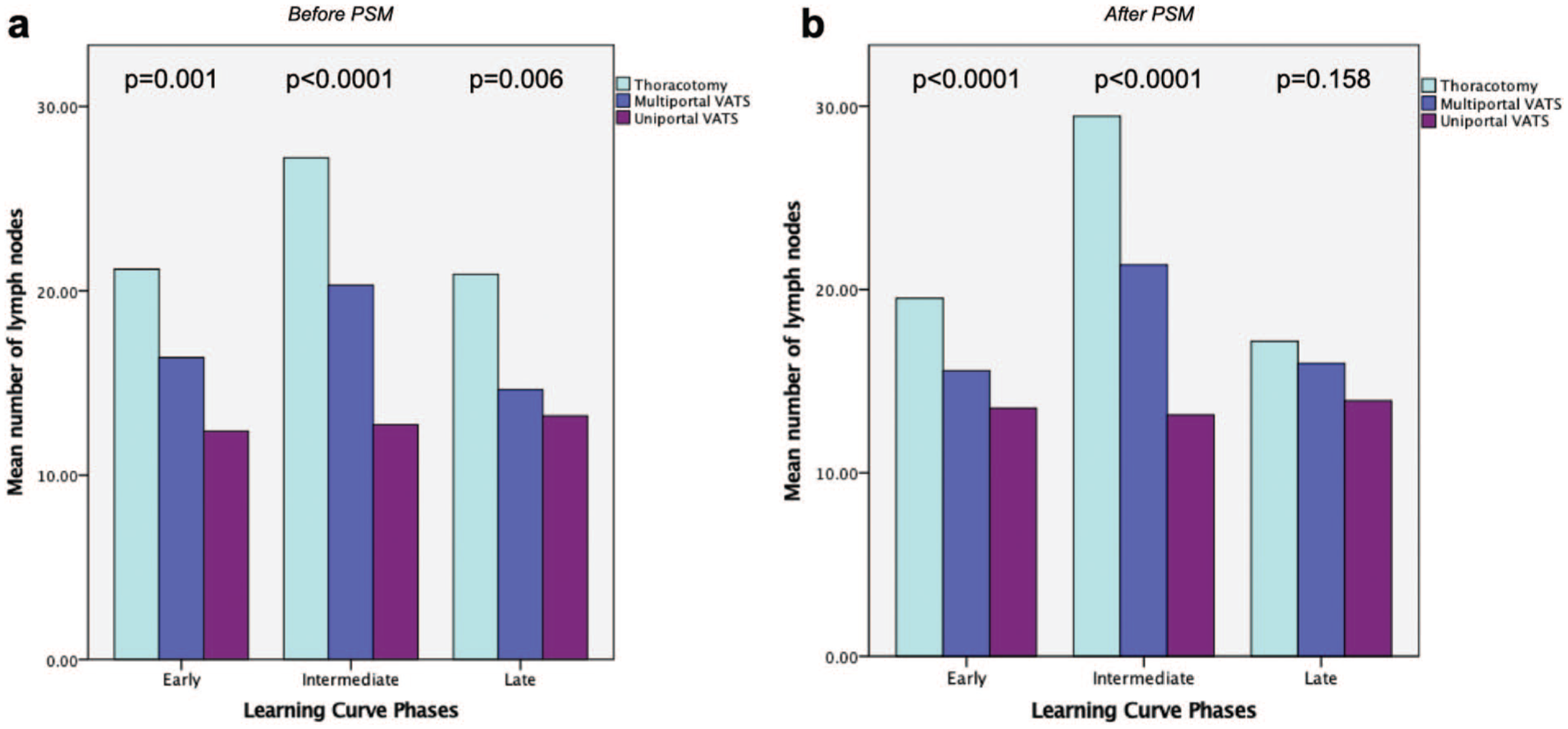
Mean number of lymph nodes dissected among different surgical approaches and learning phases (a) before and (b) after PSM analysis. PSM, propensity score matching; VATS; video-assisted thoracoscopic surgery.
After applying the PSM analysis based on age, gender, TNM staging, and preoperative surgical mediastinal staging status, a total of 474 patients were matched. The thoracotomy group included 237 patients (50.0%), the multiportal VATS group included 114 patients (24.1%), and the uniportal VATS group included 123 patients (25.9%). The demographic and clinical features were well balanced between the groups (Table 2). In the matched cohort, the mean number of dissected lymph nodes was 21.0 ± 18.5, 17.4 ± 11.5, and 13.4 ± 11.1 in the thoracotomy, multiportal VATS, and uniportal VATS groups, respectively (P < 0.001). The statistical significance of this difference was sustained in the early and intermediate phases, but it was attenuated and lost significance in the late phase (P < 0.001, P < 0.001, and P = 0.158, respectively; Table 3, Fig. 2b). No significant difference in terms of nodal upstaging between the groups was observed with 8.3% in uniportal VATS, 10.0% in multiportal VATS, and 13.6% in thoracotomy (P = 0.448). The additional analysis comparing uniportal VATS, multiportal VATS, and thoracotomy across the 3 learning periods demonstrated that the upstaging rates were 7.8%, 5.9%, and 5.0% in the early phase (P = 0.869); 8.0%, 9.5%, and 21.6% in the intermediate phase (P = 0.248); and 11.8%, 20.0%, and 8.3% in the late phase (P = 0.560), respectively. Although clinically meaningful differences were observed between the groups in some periods, statistical significance might not have been reached due to the limited number of patients in each period.
Demographic and Clinical Features Among Groups Before and After PSM Analysis.
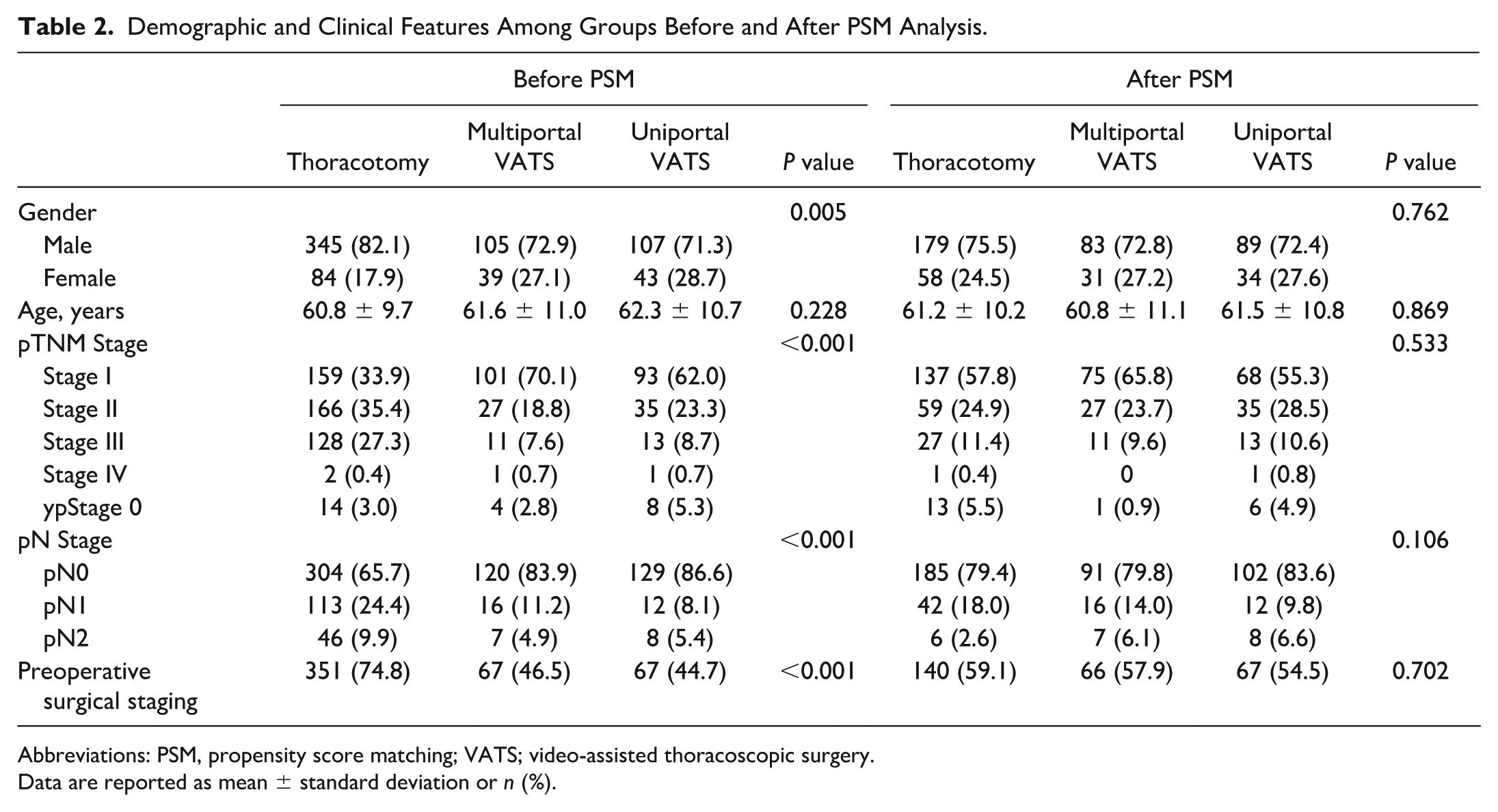
Abbreviations: PSM, propensity score matching; VATS; video-assisted thoracoscopic surgery.
Data are reported as mean ± standard deviation or n (%).
Mean Number of Lymph Nodes Dissected Among Groups Before and After PSM Analysis.
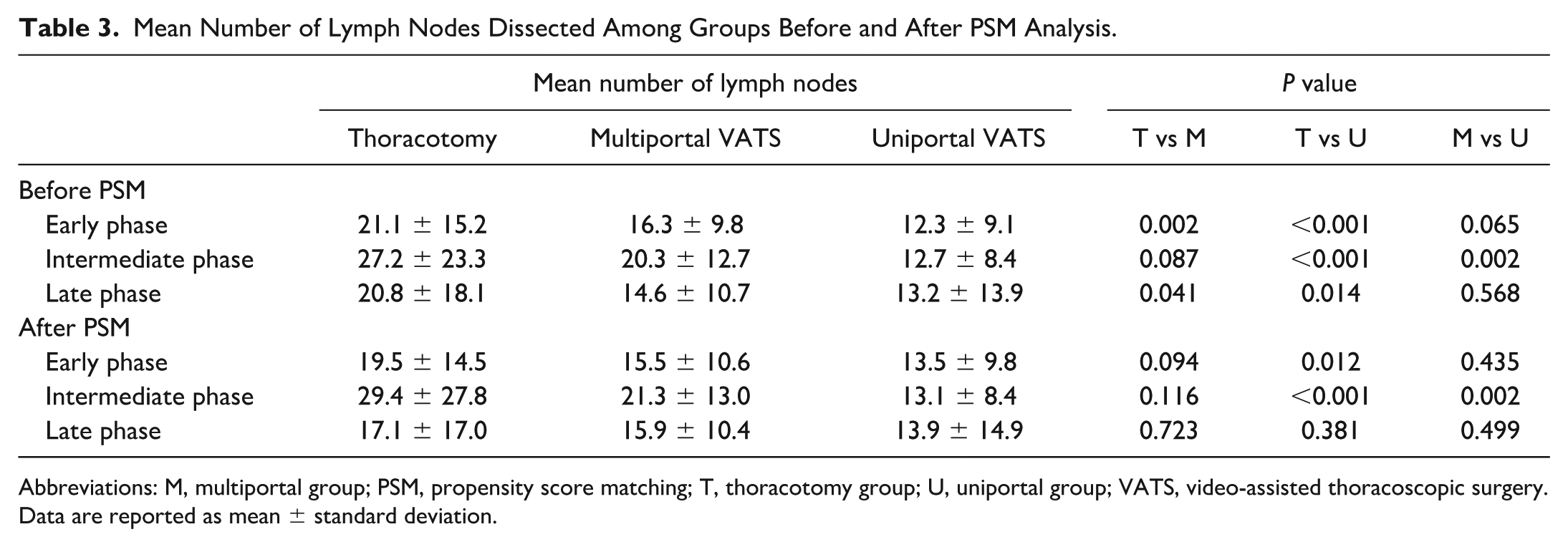
Abbreviations: M, multiportal group; PSM, propensity score matching; T, thoracotomy group; U, uniportal group; VATS, video-assisted thoracoscopic surgery.
Data are reported as mean ± standard deviation.
Discussion
The introduction of VATS has shifted lung cancer surgery toward improved perioperative comfort, better quality of life, and less pain for patients, while offering enhanced visualization and technical challenges for surgeons.3–5 In addition, uniportal VATS has contributed to the advancement of minimally invasive techniques, while raising concerns about oncologic adequacy. 16 Although uniportal and multiportal VATS are well-established approaches for lung cancer,2,16 nuances in lymph node dissection quality between surgical techniques continues to be a subject of investigation.
It can be hypothesized that enhanced visualization of the surgical field by VATS enables more thorough dissection of lymph nodes particularly adjacent to the blood vessels and trachea. One of the early studies comparing the open approach and thoracoscopy reported a higher number of total and N2 lymph nodes dissected in the thoracotomy group. 17 In contrast, a later retrospective study reported comparable outcomes between VATS and thoracotomy regarding the number of lymph nodes and stations sampled. 18 A secondary analysis of the American College of Surgeons Oncology Group Z0030 randomized trial also demonstrated a similar number of lymph nodes retrieved in both approaches. 19 Amid inconsistent findings in the current literature, a meta-analysis reported a higher total number of harvested lymph nodes with thoracotomy compared with VATS, whereas the number of lymph node stations was similar between the groups. 9
In our study, a greater number of lymph nodes were dissected in the thoracotomy group compared with the multiportal and uniportal VATS groups within the matched cohort. Moreover, multiportal VATS enabled more extensive lymph node dissection than the uniportal approach. However, these differences diminished in the late learning phase of VATS. This equalization between groups might be attributed to increasing experience with VATS, including technical advancements and better patient selection. In a single-center study investigating the adoption of VATS lobectomy, lymph node dissection was found to be more extensive without compromising safety after completion of a learning curve with 50 cases. 20
Dissection of the subcarinal lymph node station (station 7) during uniportal VATS lobectomy presents a unique technical challenge due to the limited access and constrained angles inherent to the single-incision approach. Unlike multiport VATS or open thoracotomy, uniportal VATS offers a narrower operative corridor, which may restrict instrument maneuverability, particularly when attempting to access the deep and posteriorly located subcarinal space. This difficulty is further amplified in left-sided resections, where anatomical barriers such as the aorta, esophagus, and left main bronchus complicate exposure. Adequate visualization and safe dissection of subcarinal nodes require a high level of surgical expertise and careful coordination of the thoracoscopic instruments. Despite these challenges, experienced surgeons have reported that with appropriate patient selection and advanced technical proficiency, complete and oncologically sound subcarinal lymphadenectomy can be achieved via the uniportal approach.
Starting from the consensus on VATS lobectomy recommending 50 cases for completing the learning curve, 21 subsequent studies have proposed a range of 30 to 60 cases to achieve procedural proficiency.22,23 In line with this, as our surgical experience accumulated, we were able to move beyond the early phase of the learning curve and gradually manage more complex cases. Furthermore, reflecting the cumulative global experience, Altorki et al. reported an increasing number of dissected lymph nodes over time in a retrospective, multicenter trial, which resulted in similar survival outcomes in the late period despite larger tumors and more fragile patients. 24 The adoption of less invasive techniques, such as biportal and uniportal VATS, was associated with a significantly higher number of harvested lymph nodes during the proficiency stage.25,26 Consistent with these results, in a recent meta-analysis, uniportal VATS was reported to have better perioperative outcomes and comparable oncologic efficacy including similar performance on lymph node dissection compared with multiportal VATS. 27
Our study is subject to several limitations, including its retrospective design and the relatively small sample size, which may limit the generalizability of the findings. In addition, the number of lymph node pieces, rather than the actual number of lymph nodes, was reported in the pathology records, as nodes may be fragmented during dissection or specimen handling. Although this may overestimate the number of dissected lymph nodes, we believe that the count of lymph node pieces still reflects the relative extent of lymphadenectomy. The choice of surgical approach based on surgeon preference may also represent a potential confounding factor. Nonetheless, the standardized surgical strategies employed in our center, aligned with guideline recommendations, is expected to mitigate the impact of this issue. Finally, the definition of learning phases was arbitrary, which may introduce subjective bias and influence the interpretation of surgical outcomes.
Conclusions
Our findings suggest that although the open approach enables more extensive lymph node dissection, with sufficient experience and adherence to standardized protocols, both multiportal and uniportal VATS can achieve comparable outcomes. This highlights the need for structured mentorship and training pathways that support the safe and effective adoption of minimally invasive approaches in thoracic oncology.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
Ethical approval was waived due to the retrospective nature of the study.