
Abstract
Objective:
As alternatives to conventional coronary artery bypass grafting (CABG), robot-assisted CABG (R-CABG) and percutaneous coronary intervention (PCI) offer less invasive treatments for coronary artery disease (CAD). However, data comparing outcomes of R-CABG versus PCI are limited.
Methods:
Databases were systematically searched for studies comparing R-CABG versus PCI. Random-effects models were used to calculate pooled odds ratios (ORs) with 95% confidence intervals (CIs), both overall and stratified by left main or multivessel (LM+MV) or isolated left anterior descending artery (LAD) disease. Kaplan–Meier curves were digitally extracted to reconstruct individual participant data (IPD), from which hazard ratios (HRs) were estimated for survival analyses.
Results:
Six retrospective studies, including 1,896 patients (R-CABG: 894, 47.1%), were analyzed. The mean age was 63.8 ± 11.3 years, and 78.7% were male patients. Follow-up ranged from 2 to 8 years. Overall, R-CABG was associated with a lower odds of target vessel revascularization (TVR; OR = 0.50, 95% CI: 0.27 to 0.93, P = 0.03) and myocardial infarction (MI; OR = 0.44, 95% CI: 0.26 to 0.76, P < 0.01), with no significant difference in all-cause mortality. Among patients with LM+MV disease, R-CABG reduced TVR and MI. In LAD lesions, R-CABG significantly lowered the likelihood of MI (OR = 0.18, 95% CI: 0.04 to 0.71) as well as major adverse cardiovascular events (MACE; OR = 0.51, 95% CI: 0.28 to 0.93). Time-to-event analysis from reconstructed IPD demonstrated significantly improved freedom from reintervention (HR = 0.31, 95% CI: 0.16 to 0.60) and MACE (HR = 0.24, 95% CI: 0.15 to 0.60) with R-CABG, whereas no significant difference was found for all-cause mortality.
Conclusions:
R-CABG was associated with less TVR and MI compared with PCI in CAD patients, with no difference in all-cause mortality.
This is a visual representation of the abstract.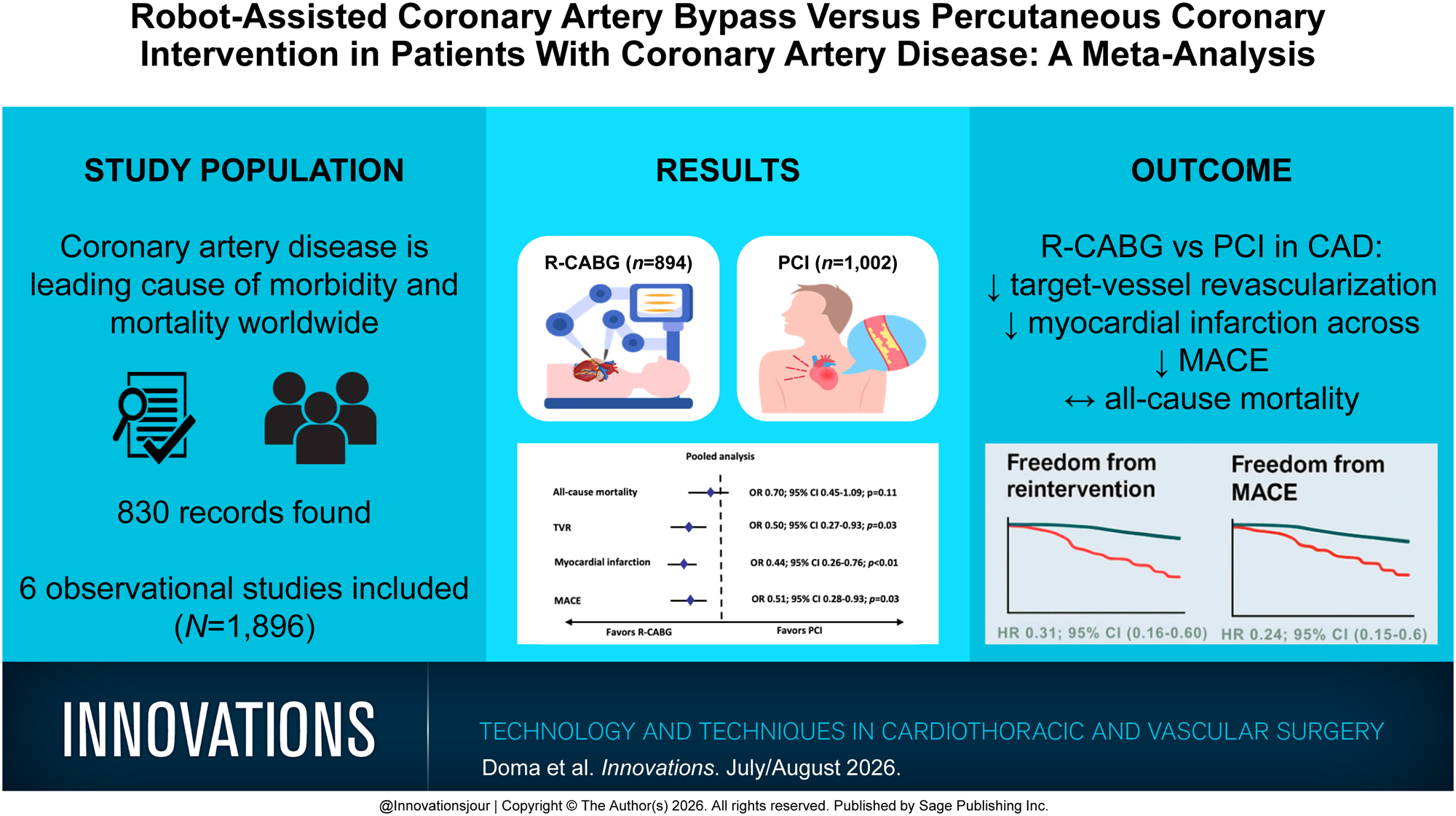
Keywords
Central Message
Across 6 retro-spective studies,robot-assisted CABGreduced repeatrevascularization andMI compared withPCI, including in theLM+MV and LADdisease subgroups,with improvedreintervention-freeand MACE-freesurvival fromreconstructed IPD.All-cause mortalitywas not statisticallydifferent.
Introduction
Coronary artery disease (CAD) remains a leading cause of morbidity and mortality worldwide. 1 The optimal management of patients with multivessel (MV) disease, left main (LM) disease, and isolated left anterior descending artery (LAD) CAD presents ongoing clinical challenges.2,3 The selection of revascularization strategies is based on lesion complexity, comorbidities, anatomical considerations, and patient preferences.
Robot-assisted coronary artery bypass grafting (R-CABG) has emerged as a minimally invasive alternative to conventional CABG, aiming to reduce surgical trauma while preserving the durability of arterial grafts.4–6 The use of robotic surgery enables improved precision in artery harvesting and smaller incisions, resulting in lower rates of perioperative complications, shorter hospital stays, and faster recovery compared with open surgery.7–9 As robotic technology has advanced, R-CABG has been increasingly adopted for isolated LAD lesions and selected MV or hybrid procedures.10,11
Percutaneous coronary intervention (PCI) remains a widely used revascularization approach, particularly for patients with single-vessel CAD.12–15 Advances in drug-eluting stents, bifurcation techniques, and adjunctive imaging have improved PCI outcomes.15,16 Several studies have compared PCI with conventional CABG, often showing comparable mortality but higher rates of repeat revascularization and myocardial infarction (MI), specifically in patients with complex CAD anatomy.16–18 Direct comparisons between PCI and R-CABG remain limited, and differences in patient selection, lesion characteristics, and procedural expertise complicate interpretation.
Therefore, we conducted the present study to compare clinical outcomes between R-CABG and PCI through a systematic review and meta-analysis. Building on prior work,19,20 this analysis incorporates reconstructed individual patient-level time-to-event data from Kaplan–Meier curves, subgroup analyses by lesion anatomy, and updated evidence to provide a more detailed comparison of these 2 revascularization strategies.
Methods
This systematic review and meta-analysis was performed and reported following the Cochrane Collaboration Handbook for Systematic Reviews of Interventions and the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Statement guidelines (Supplemental Table 1, Supplemental Table 2). 21 The protocol for this study was registered in the International Prospective Register of Systematic Reviews (PROSPERO ID CRD420250638623).
Data Source and Search Strategy
PubMed, Scopus, and the Cochrane Central Register of Controlled Trials were searched systematically from database inception to May 20, 2025. Search strategies combined terms related to R-CABG techniques (e.g., “MIDCAB,” “TECAB”), PCI (e.g., “PCI,” “stenting”), and CAD anatomic subtypes (e.g., “LAD,” “CTO”). The full search syntax is provided in Supplemental Table 3. After removal of duplicate citations, 2 reviewers independently screened all titles, abstracts, and full texts against predefined eligibility criteria. Disagreements were resolved by discussion with a senior author. Reference lists of included studies were also manually reviewed to identify additional eligible articles.
Eligibility Criteria
Studies that compared R-CABG with PCI and reported on relevant clinical outcomes were included. Studies were excluded if they lacked a control group, involved concomitant or hybrid procedures, or enrolled 10 or fewer patients. Conference abstracts and studies with overlapping patient populations were also excluded. In cases of suspected population overlap, corresponding authors were contacted to clarify study cohorts to avoid duplication.
Definitions and Procedural Characteristics
The included studies evaluated patients treated with either R-CABG or PCI, but the criteria for study enrollment varied. Some studies used coronary anatomy, such as isolated LAD or MV disease, whereas others relied on clinical judgment without standardized definitions. For the purposes of this analysis, R-CABG was defined as any coronary bypass procedure performed with robotic assistance, including totally endoscopic coronary artery bypass (TECAB) and robot-assisted minimally invasive direct CABG (RA-MIDCAB) techniques, performed either on-pump or off-pump. Procedural details, including robotic platforms, conduit selection, and stent types, were inconsistently reported across studies; these are summarized in Supplemental Table 4 and Supplemental Table 5. Given this procedural variability, heterogeneity in outcomes was qualitatively considered when interpreting the pooled results.
Data Extraction
Two authors independently extracted the following data: study inclusion and exclusion criteria, follow-up period, baseline patient characteristics, endpoint data, and endpoint definitions. Disagreements were resolved in a panel discussion with the senior author. Baseline characteristics were reported as the mean ± standard deviation for continuous variables and as percentages for binary variables.
Endpoints, Subgroup Analyses, and Sensitivity Analyses
Outcomes of interest included all-cause mortality, target vessel revascularization (TVR), MI, and major adverse cardiovascular events (MACE). Endpoints were defined differently by individual studies. Detailed endpoint definitions are provided in Supplemental Table 6.
Subgroup analyses were performed, stratifying by lesion location at the study level: complex CAD (LM and MV disease) and isolated LAD disease. To assess the robustness of the findings, a leave-one-out sensitivity analysis was conducted by excluding 1 study at a time. Between-study heterogeneity was evaluated using the I2 statistic, with a two-tailed P < 0.05 considered statistically significant.
In addition, a correlation analysis to examine the relationship between follow-up duration and treatment effect was conducted for all-cause mortality, TVR, MI, and MACE. Repeat revascularization (of any vessel) and cardiac-specific mortality were examined during data extraction; however, these outcomes were not consistently reported across studies, as detailed in Supplemental Table 6.
Quality Assessment
Two authors independently conducted the risk of bias assessment. Disagreements were resolved through consensus discussion. Nonrandomized studies were assessed using the Risk Of Bias In Non-Randomized Studies - of Interventions (ROBINS-I) V2 tool. 22 Each study was evaluated in 7 domains, including confounding, selection of participants, classification of interventions, deviations from intended interventions, missing data, measurement of outcomes, and selection of reported results. Each domain was assessed according to predefined criteria, and the overall risk of bias was categorized as low, moderate, serious, or critical. Funnel plots were generated to visually assess for potential publication bias.
In addition, Grading of Recommendations Assessment, Development and Evaluation (GRADE) assessment was performed to evaluate the certainty of evidence for each outcome, considering risk of bias, inconsistency, indirectness, imprecision, and publication bias. The overall certainty of evidence was categorized as high, moderate, low, or very low. 23
Statistical Analysis
Binary endpoint data were aggregated using Mantel–Haenszel random-effects models to generate odds ratios (ORs) with 95% confidence intervals (CIs). The restricted maximum likelihood estimate was used to calculate heterogeneity variance (tau2). Heterogeneity was assessed with Cochrane’s Jackson method I2 statistics. The consistency of the studies was determined based on I2 values of 0%, ≤25%, ≤50%, and >50%, indicating no observed, low, moderate, and substantial heterogeneity, respectively. 24 Analyses were conducted using R software, version 4.3.2 (R Project for Statistical Computing, Vienna, Austria) with the extension packages “meta” and “dmetar” used for all calculations and graphics.25,26
Survival Analyses Using Reconstructed Time-to-Event Data
Individual participant data (IPD) were reconstructed by digital extraction from published Kaplan–Meier curves and number-at-risk tables for studies reporting all-cause mortality, repeat revascularization, and MACE. IPD for MI were not reconstructed due to insufficient data. Reconstructed datasets were merged across studies. Survival time and event status variables were standardized, and treatment was modeled as a categorical variable. Unadjusted comparisons between groups were visualized using Kaplan–Meier survival curves, with log-rank P values reported. Cox proportional hazards models were fitted to estimate hazard ratios (HRs), and both fixed-effects models and frailty models with study-level random effects (gamma-distributed) were applied to account for study heterogeneity. 27 Proportional hazards assumptions were visualized using Schoenfeld residuals and were tested using the Grambsch–Therneau test. 28 In cases of potential nonproportionality, treatment effects were also evaluated using restricted mean survival time (RMST) analyses truncated at the maximum common follow-up time. 29 RMST differences and corresponding CIs were derived to estimate the average treatment effect over time. Survival analyses were performed using R version 4.3.2 packages including “survival,” “survminer,” “survRM2,” “gtsummary,” “rms,” and “cowplot.”
Results
Study Selection and Characteristics
The initial database search identified 820 records, of which 287 were duplicates and were removed before screening. A total of 533 unique records were screened by title and abstract, and 17 full-text articles were assessed for eligibility (Fig. 1). Finally, 6 nonrandomized, retrospective studies met the inclusion criteria and were included in the analysis.30–35 Across the included studies, a total of 1,896 patients were analyzed: 894 (47.1%) underwent R-CABG and 1,002 (52.9%) underwent PCI. The mean age of the participants ranged from 58.1 to 67.3 years, with an overall mean of approximately 63.8 ± 11.3 years (R-CABG 63.1 ± 11 years vs PCI 64.5 ± 11.6 years). Among studies with available data, approximately 78.7% were male patients. A summary of baseline characteristics for each study population, including comorbidities, is presented in Table 1.
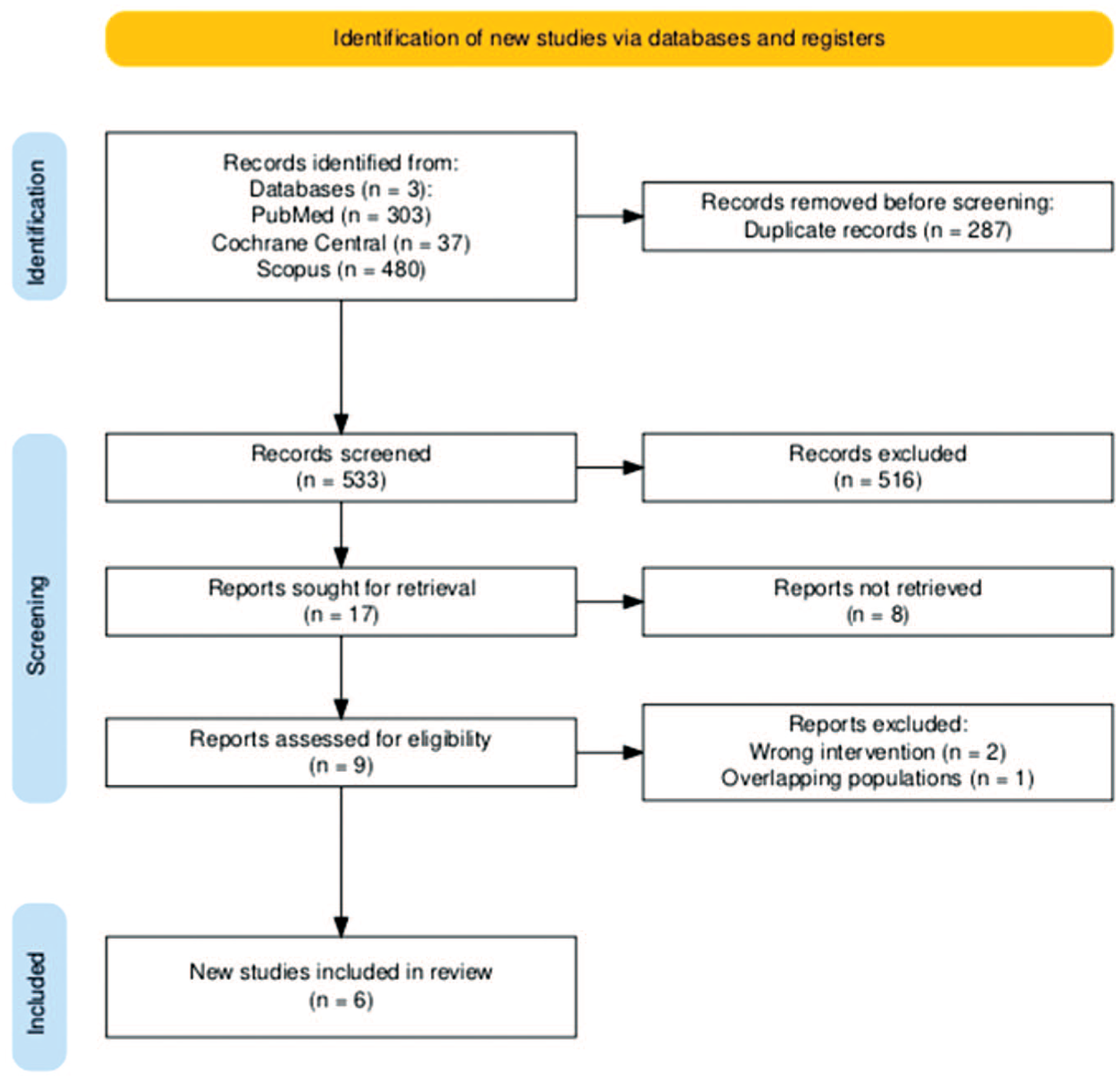
PRISMA flow diagram illustrating the process of study identification, screening, eligibility assessment, and inclusion.
Baseline Characteristics of the Included Studies.
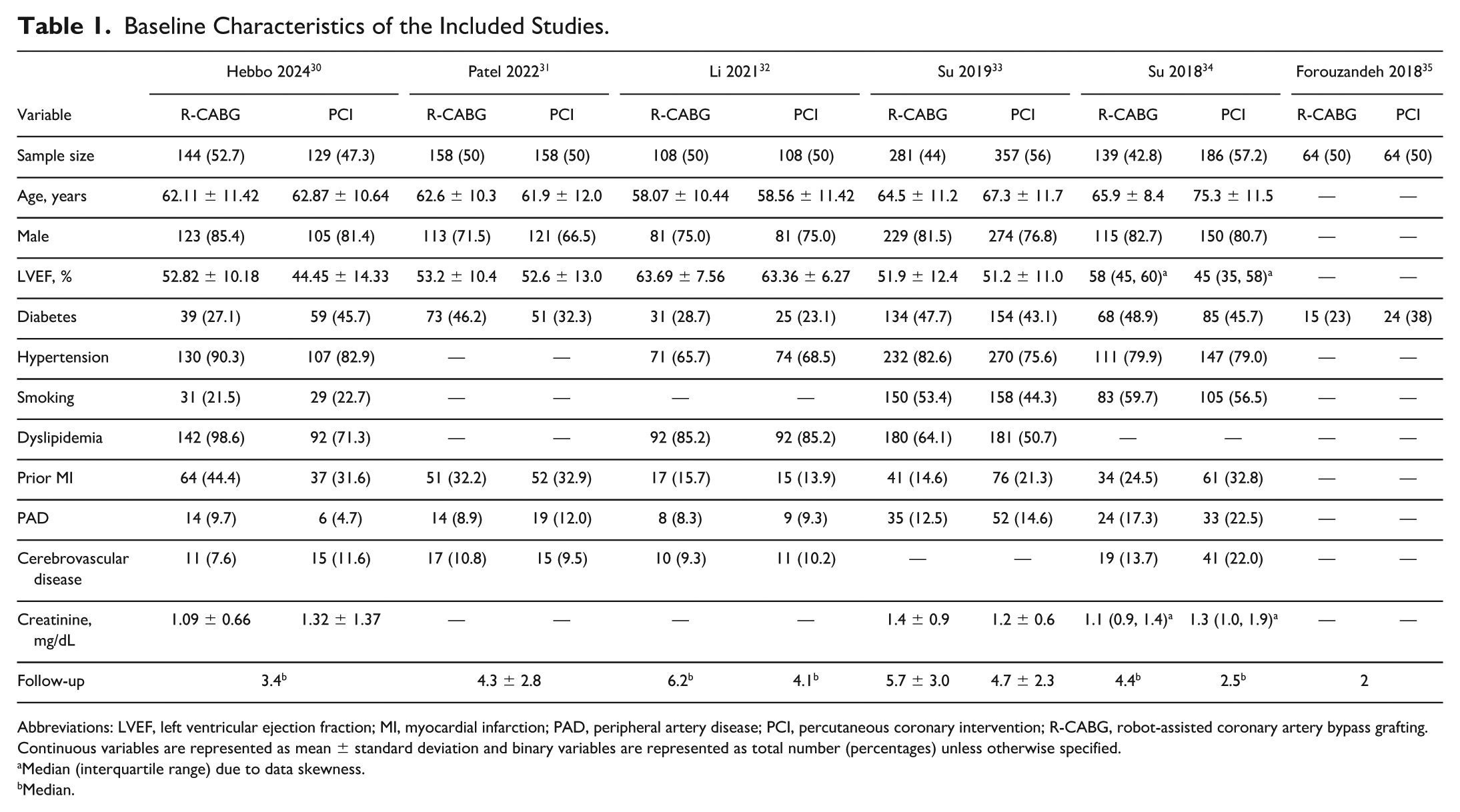
Abbreviations: LVEF, left ventricular ejection fraction; MI, myocardial infarction; PAD, peripheral artery disease; PCI, percutaneous coronary intervention; R-CABG, robot-assisted coronary artery bypass grafting.
Continuous variables are represented as mean ± standard deviation and binary variables are represented as total number (percentages) unless otherwise specified.
Median (interquartile range) due to data skewness.
Median.
Pooled Analysis
Across all included studies, there was no statistically significant difference in all-cause mortality (very low certainty of evidence) between R-CABG and PCI (Fig. 2a). However, R-CABG was associated with a significantly lower risk of TVR compared with PCI (OR = 0.50, 95% CI: 0.27 to 0.93, P = 0.03, I2 = 53%, moderate certainty of evidence; Fig. 2b). The incidence of MI was also significantly reduced with R-CABG (OR = 0.44, 95% CI: 0.26 to 0.76, P < 0.01, I2 = 0%, low certainty of evidence; Fig. 3a). MACE data were reported by only 3 studies of isolated LAD lesions; in pooled analysis, R-CABG was associated with a significantly lower risk (OR = 0.51, 95% CI: 0.28 to 0.93, P = 0.03, I2 = 20%, low certainty of evidence; Fig. 3b).
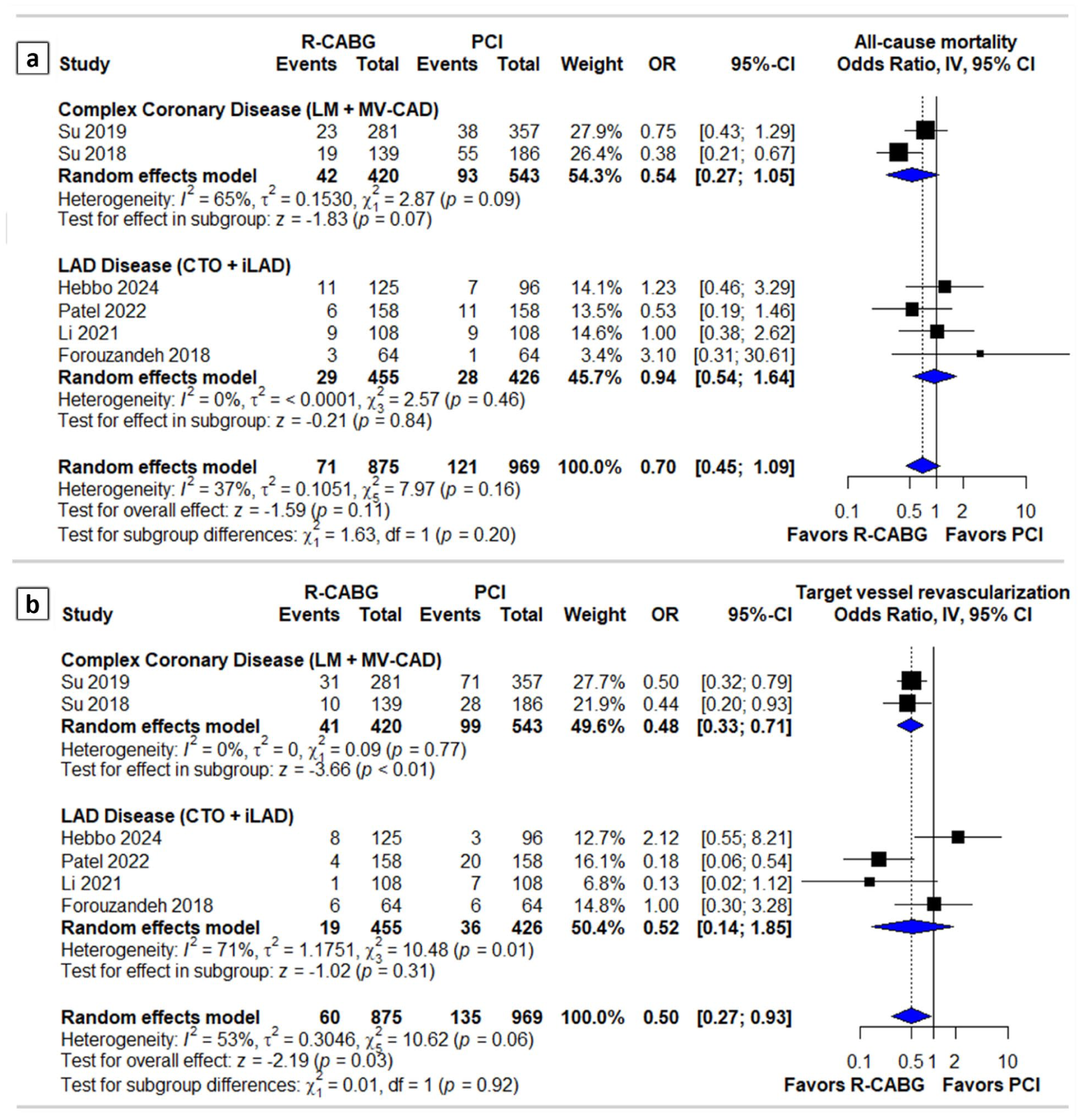
Forest plots showing ORs with 95% CIs for (a) all-cause mortality and (b) target vessel revascularization in patients with CAD undergoing R-CABG versus PCI. Analyses are stratified by disease subtype: LM + MV-CAD and LAD (CTO + iLAD). CI, confidence interval; CTO, chronic total occlusion; iLAD, isolated LAD disease; LAD, left anterior descending artery; LM, left main; MV-CAD, multivessel coronary artery disease; OR, odds ratio; PCI, percutaneous coronary intervention; R-CABG, robot-assisted coronary artery bypass grafting.
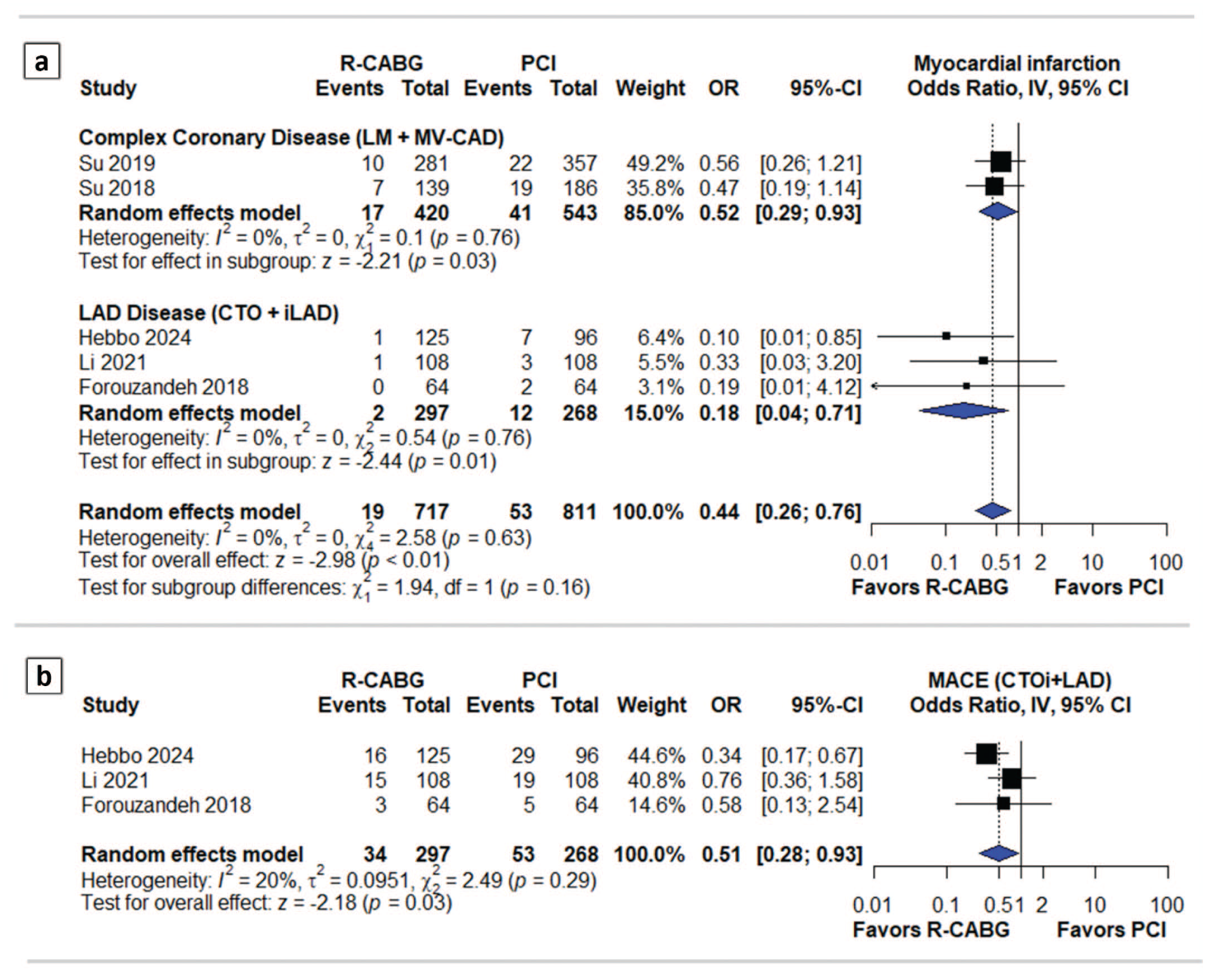
Forest plots showing ORs with 95% CIs for (a) myocardial infarction and (b) MACE in patients with coronary artery disease undergoing R-CABG versus PCI. Analyses are stratified by disease subtype: LM + MV-CAD and LAD (CTO + iLAD). CI, confidence interval; CTO, chronic total occlusion; iLAD, isolated LAD disease; LAD, left anterior descending artery; LM, left main; MACE, major adverse cardiovascular events; MV-CAD, multivessel coronary artery disease; OR, odds ratio; PCI, percutaneous coronary intervention; R-CABG, robot-assisted coronary artery bypass grafting.
Subgroup Analyses
In patients with complex coronary disease (LM or MV CAD), there was not a significant difference in all-cause mortality between R-CABG and PCI (very low certainty of evidence; Fig. 2a). R-CABG significantly reduced the likelihood of TVR (OR = 0.48, 95% CI: 0.33 to 0.71, P < 0.01, low certainty of evidence; Fig. 2b) and MI (OR = 0.52, 95% CI: 0.29 to 0.93, P = 0.03, low certainty of evidence; Fig. 3a), with no heterogeneity observed in either outcome.
Among patients with isolated LAD disease, there were no significant differences between R-CABG and PCI in all-cause mortality (very low certainty of evidence; Fig. 2a) or TVR (very low certainty of evidence; Fig. 2b). However, R-CABG was associated with a significantly lower odds of MI (OR = 0.18, 95% CI: 0.04 to 0.71, P = 0.01, moderate certainty of evidence; Fig. 3a). In addition, R-CABG demonstrated a significant benefit for MACE, reported exclusively in LAD-focused studies (Fig. 3b) as reported above.
Sensitivity Analyses
The leave-one-out sensitivity analysis demonstrated stable pooled estimates across all evaluated outcomes. For all-cause mortality, TVR, MI, and MACE, no single study had a disproportionate influence on the overall effect size or heterogeneity. The findings remained consistent both in the full cohort and in the subgroup analyses, confirming the robustness of the primary results. A summary of the leave-one-out sensitivity analyses is presented in Supplemental Figure 1.
Follow-Up Correlation With Overall Effect Size
The relationship between follow-up duration and treatment effect size was assessed using scatter plots of log ORs against median follow-up time for each outcome (Supplemental Fig. 2). For all-cause mortality and MI, a visual trend suggested that the relative benefit of R-CABG may attenuate slightly over longer follow-up, although the CIs were wide and no formal correlation testing was possible. In contrast, effect sizes for MACE appeared stable across follow-up durations, whereas for TVR, a slight negative slope was observed, suggesting that the benefit of R-CABG may persist over time. These findings are exploratory, descriptive, and should be interpreted cautiously as they do not reflect formal meta-regression models.
Time-to-Event Analyses
Kaplan–Meier survival analyses were conducted using reconstructed IPD for overall survival, freedom from MACE, and freedom from TVR. No significant difference in overall survival was observed between R-CABG and PCI, and the Cox model confirmed the absence of a meaningful difference (Fig. 4). In contrast, R-CABG was associated with significantly greater freedom from TVR (HR = 0.31, 95% CI: 0.16 to 0.60, P < 0.001; Fig. 5a) and a lower hazard of MACE (HR = 0.24, 95% CI: 0.15 to 0.60, P < 0.001; Fig. 5b).
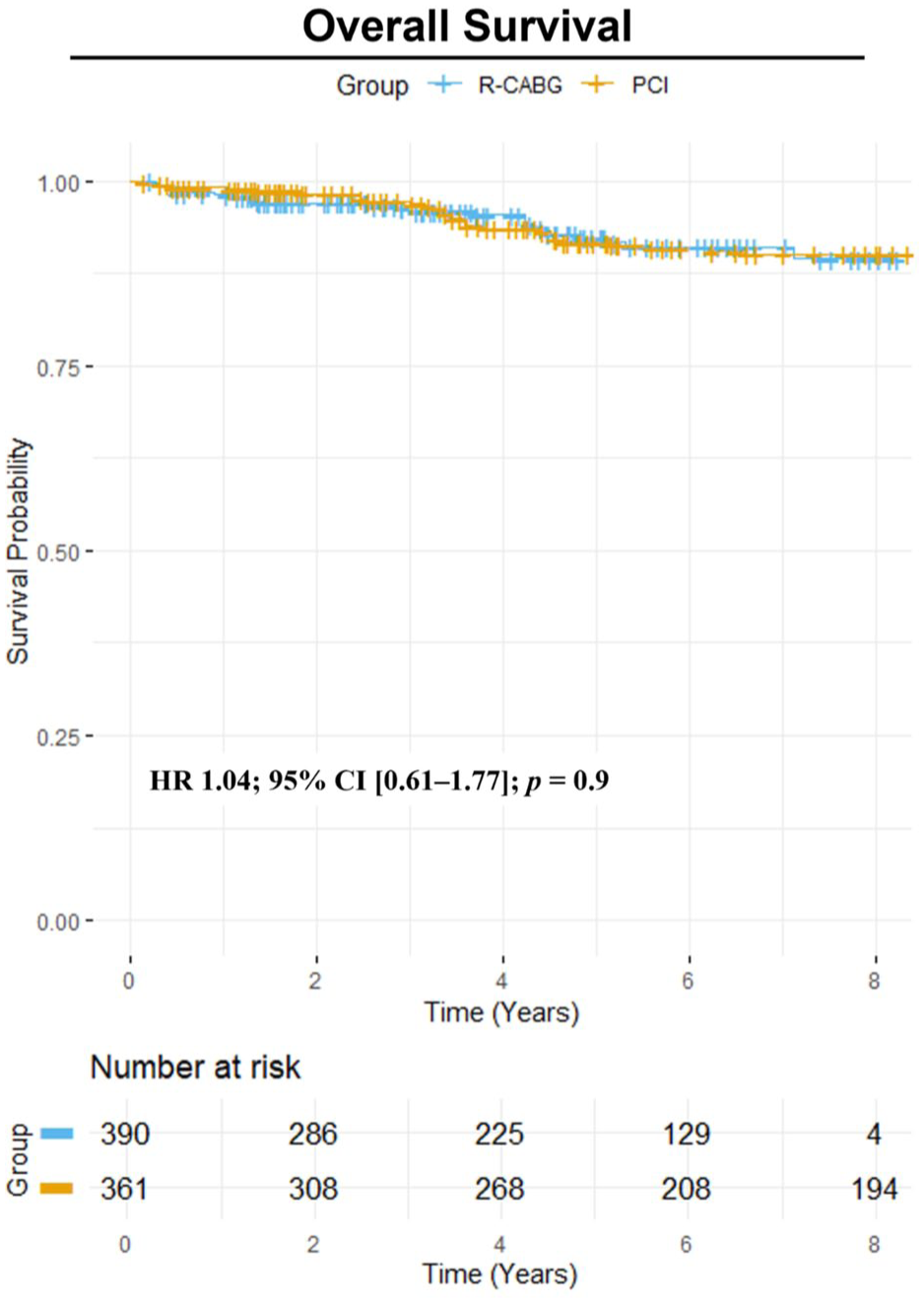
Kaplan–Meier survival curve comparing overall survival in patients with coronary artery disease undergoing R-CABG versus PCI. CI, confidence interval; HR, hazard ratio; PCI, percutaneous coronary intervention; R-CABG, robot-assisted coronary artery bypass grafting.
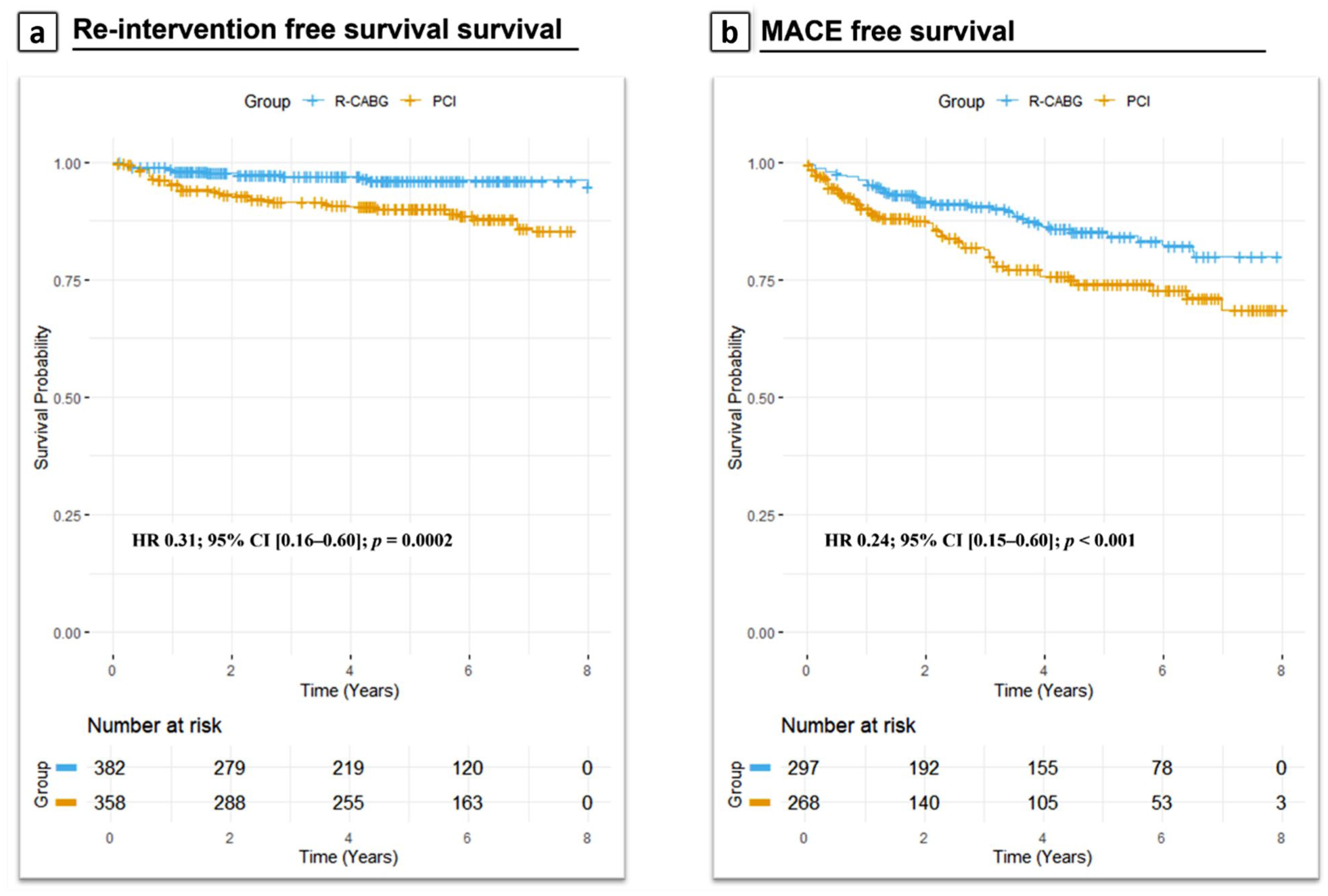
Kaplan–Meier survival curves comparing (a) reintervention-free survival and (b) MACE-free survival in patients with coronary artery disease undergoing R-CABG versus PCI. CI, confidence interval; HR, hazard ratio; MACE, major adverse cardiovascular events; PCI, percutaneous coronary intervention; R-CABG, robot-assisted coronary artery bypass grafting.
Schoenfeld residual plots were examined to assess the proportional hazards assumption for both outcomes. Although some deviations were noted toward the tail end of follow-up, the residuals for both treatment and study covariates remained largely within the confidence bounds over time. These plots suggest that the proportional hazards assumption was reasonably met for the fitted Cox models (Supplemental Fig. 3).
In addition, RMST analyses were performed using truncation points that reflected the maximum common follow-up duration across the reconstructed survival curves for each outcome. For all-cause mortality and TVR, RMST was estimated over a 5-year truncation interval; for MACE, RMST was estimated over a 2-year interval. The corresponding RMST values were 4.82 versus 4.83 years for all-cause mortality, 4.88 versus 4.66 years for TVR, and 1.91 versus 1.83 years for MACE (Supplemental Fig. 4). Although longer event-free survival with R-CABG was reported for TVR and MACE, no significant difference was noted for all-cause mortality. These RMST estimates provide a time-based perspective on treatment effect, broadly consistent with the direction of effect observed in the reconstructed HRs.
Quality Assessment
Risk of bias was evaluated across 7 domains using the ROBINS-I V2 tool. As illustrated in the traffic light plot (Supplemental Fig. 5), 4 studies were judged to have an overall critical risk of bias, primarily due to a lack of confounding adjustment and concerns about participant selection as well as selective reporting and missing data. Only Hebbo et al. (2024) and Patel et al. (2022) achieved overall moderate and low risks of bias, respectively, supported by their use of propensity matching and more complete outcome data.30,31 Funnel plots for all 4 outcomes (all-cause mortality, TVR, MI, and MACE) are presented in Supplemental Figure 6. Overall, although some visual asymmetry was noted for all-cause mortality and TVR, the small number of included studies limits definitive conclusions regarding publication bias.
The GRADE assessment showed moderate to very low certainty of evidence across outcomes. For all-cause mortality, the certainty was very low in all subgroups; however, TVR and MI data showed moderate to low certainty, including in the subgroup analyses. The detailed GRADE assessment is reported in Supplemental Table 7, Supplemental Table 8, and Supplemental Table 9.
Discussion
We conducted a meta-analysis of 6 nonrandomized studies to compare clinical outcomes between R-CABG and PCI. The main findings of the study can be summarized as follows: (1) there was no significant difference in all-cause mortality between R-CABG and PCI, (2) R-CABG was associated with a lower risk of MI and TVR compared with PCI, and (3) this benefit was consistent in patients with complex coronary disease (LM+MV), whereas in isolated LAD lesions, R-CABG significantly reduced MI and MACE but not TVR or mortality.
This meta-analysis suggests that there is no statistically significant difference in all-cause mortality between revascularization with R-CABG and PCI in patients with LM disease and MV CAD. This finding is consistent with several previous meta-analyses that have also demonstrated no significant difference in mortality between sternotomy CABG and PCI.16,36,37
Over the past 2 decades, robotic coronary surgery has progressed from experimental feasibility to a clinically mature, reproducible approach at specialized centers. Advances such as articulated EndoWrist instruments (Intuitive Surgical, Sunnyvale, CA, USA), intrathoracic stabilizers, and 3-arm beating-heart TECAB systems have enabled complete arterial revascularization without sternotomy. The introduction of automated distal anastomotic devices, including the Cardica C-Port Flex-A, further improved precision and reduced operative times, helping flatten the learning curve for new programs. Large contemporary single-center experiences have reported procedural completion in 98% to 99% of TECAB cases and early graft patency around 97%,38,39 confirming the safety and durability of these methods. This is also supported by the largest MIDCAB series to date, which reported excellent early outcomes and durable 20-year survival in 2,667 patients. 40 Similarly, the largest contemporary TECAB series, involving 874 patients with up to 10-year follow-up, demonstrated high graft patency, low perioperative mortality, and sustained freedom from major adverse events. 41 Increasing adoption of dedicated training curricula and high-volume robotic programs worldwide supports that R-CABG is now a clinically established, minimally invasive alternative to conventional CABG rather than an emerging technology.
However, certain factors must be taken into account. In the study by Su et al. (2018), patients in the R-CABG group showed more favorable baseline characteristics. 34 In contrast, the PCI group had higher rates of advanced age, acute coronary syndrome, chronic kidney disease (CKD), peripheral artery disease, prior cerebrovascular accident, previous MI, prior PCI, prior CABG, lower left ventricular ejection fraction (LVEF), cardiogenic shock, and cardiac arrest. Multivariable logistic regression analysis identified age, diabetes mellitus, LVEF, statin use, and CKD as independent predictors of long-term mortality. 34 Therefore, the findings showing that patients undergoing PCI experienced more than twice the rate of all-cause mortality and TVR compared with the R-CABG group may be largely attributed to differences in baseline characteristics. In addition, in both the Su et al. (2018) 34 and Su et al. (2019) 33 studies, the choice of revascularization modality was partially left to physician discretion, potentially introducing selection bias. Patients selected for surgery underwent either R-CABG or C-CABG based on comorbidities, patient preference, and financial considerations, which may have further contributed to bias.
The LM coronary artery supplies a substantial portion (75% to 100%) of the LV myocardium; consequently, significant LM stenosis places the left ventricle at considerable risk. Most LM disease involves the left main bifurcation, and this anatomical location has significant implications for performing PCI compared with lesions located in the ostial or mid-shaft segments of the vessel. 42 The natural history of medically managed LM disease is associated with a 15-year mortality rate of up to 73%. 43
Current revascularization guidelines provide a Class I, Level B-R recommendation for CABG in patients with significant LM CAD to improve survival. 44 PCI is also reasonable (Class IIa, Level B-R) when similar outcomes to CABG can be achieved. 44 This recommendation is based on a network meta-analysis demonstrating that the survival benefit of PCI over medical therapy was similar to that observed with CABG. 45
In our analysis, outcomes of R-CABG in LM disease were consistent with these recommendations, suggesting that minimally invasive approaches can preserve the established survival advantage of surgical revascularization while reducing operative morbidity. From a procedural standpoint, in both Su et al. (2019) and (2018),33,34 the decision to employ a 1-stent or 2-stent technique, as well as the choice between drug-eluting and bare-metal stents, was operator dependent. Among the 2-stent strategies, the double-kiss (DK) crush technique has demonstrated lower rates of TVR compared with the culotte technique. 46 However, as reported by Su et al. (2018), 34 86% of patients were treated with a 2-stent strategy, 92% of whom underwent the culotte technique and only 5.5% the DK-crush technique, which may partly explain the higher rates of TVR and all-cause mortality observed.34,40,45,46 Several studies support revascularization as the preferred treatment strategy for patients with chronic total occlusion (CTO).47–49 However, the evidence base for the treatment of CTOs has been hindered by inconsistent descriptive and quantitative terminology used to define lesion characteristics.50,51 Growing evidence suggests that, in appropriately selected patients, successful PCI for a CTO may lead to a significant reduction in symptom burden and functional ischemia. 51 In our study, we found no significant difference in TVR or all-cause mortality among patients with CTO involving the isolated LAD. These findings differ from a previous meta-analysis, which demonstrated that, compared with CABG, PCI was associated with lower all-cause and cardiac mortality but with a higher incidence of MI and repeat revascularization. This showed that the results in Wang et al. may be attributed to the routine use of internal thoracic artery grafts in the CABG cohort, which are known to provide superior long-term patency rates. 52 However, certain specific methodological aspects within the included studies warrant consideration. It is well established that a history of prior CABG may reflect a more aggressive atherosclerotic burden and more complex comorbidities. 53 Post-graft CTOs are often more complex, typically associated with higher J-CTO scores and lower rates of technical success. In the study by Hebbo et al., no patients in the CABG group had a history of prior CABG. 30 In contrast, 16% of patients in the PCI group had previously undergone LAD revascularization, with more than 50% of those presenting with either occluded or severely diseased grafts. In addition, LAD bifurcation PCI was common in the PCI group (26%). These differences may have led to an underestimation of the potential clinical benefit in favor of PCI. On the other hand, in the study by Forouzandeh et al., patients in the R-CABG group had significantly more severe baseline characteristics compared with those in the PCI group. 35 Patients in the R-CABG cohort demonstrated higher J-CTO and SYNTAX scores as well as a greater frequency of proximally located LAD lesions.
R-CABG was associated with a significantly reduced rate of MI compared with PCI, both in patients with complex CAD and those with isolated LAD involvement. These findings are consistent with the study by Aluthman et al., which compared conventional CABG with R-CABG and reported no MI events in the R-CABG group. 10 Similarly, another study conducted by Halkos et al., showed a low MI incidence of 1.6% among patients undergoing R-CABG. 54 However, Koefler et al. found no significant difference in MI rates and noted similar long-term outcomes between R-CABG and conventional CABG. 55 These variances may be attributed to differences in study design, patient selection, and surgical techniques, because most of them compared R-CABG with conventional CABG instead of PCI, which also reinforces the importance of this meta-analysis.
Regarding MACE, a recent meta-analysis conducted by Hwang et al., which included 39 studies, reported a high rate of long-term MACE-free survival and great overall graft patency among patients undergoing R-CABG, reinforcing the clinical value of the technique. 9 Similarly, in the study by Aluthman et al., robot-assisted hybrid coronary revascularization observed no MACE events. 10 Although they employed a hybrid strategy, their findings further support the clinical safety and effectiveness of robot-assisted approaches. These results align with our own, in which pooled data from 3 studies demonstrated a significantly lower risk of MACE in the R-CABG group compared with PCI. As shown in Figure 5b, the MACE-free survival hazard ratio was 0.24 (95% CI: 0.15 to 0.60, P < 0.001), indicating a substantial reduction in adverse cardiovascular outcomes with R-CABG. This further reinforces the long-term benefits highlighted by Hwang et al.
The results of this meta-analysis are consistent with the established evidence base demonstrating the long-term superiority of CABG over PCI in durability and freedom from repeat revascularization. Importantly, this study extends that evidence to the robotic era, showing that such benefits can now be achieved through a minimally invasive, beating-heart approach. As robotic programs mature and procedural reproducibility increases, R-CABG has the potential to redefine surgical revascularization by combining the long-term advantages of bypass grafting with the reduced invasiveness traditionally associated with PCI.
Clinical Applicability and Future Directions
This meta-analysis supports the growing role of R-CABG as a minimally invasive yet durable revascularization option. As robotic platforms improve in precision, automation, and integration with intraoperative imaging, the feasibility of wider adoption of R-CABG is increasing. These technologies may allow surgical revascularization to extend its established survival advantage while reducing perioperative morbidity and recovery time. However, wider implementation of R-CABG remains constrained by institutional learning curves, capital cost, and the need for multidisciplinary team experience. Ongoing multicenter registries and cost-effectiveness analyses will be critical to inform guideline inclusion and resource allocation. In contrast, while robotic PCI remains technically feasible and has been shown to reduce operator radiation exposure and enhance procedural precision, the original Corindus systems were ultimately withdrawn from the market due to high cost and limited commercial viability. 56 Currently, there is no robotic PCI system approved for clinical use in the United States, and only 1 (R-One, Robocath, Rouen, France) is available in Europe and China. 56 Future efforts may focus on developing more affordable and versatile systems, including those capable of telerobotic operation. Comparative studies examining not only traditional outcomes (e.g., mortality, MI, TVR) but also operator ergonomics, patient-centered endpoints such as recovery and quality of life, and hybrid strategies combining robotic CABG with manual or future robotic PCI approaches will be essential. Ultimately, the integration of robotics across surgical and interventional domains may still reshape revascularization for anatomically complex but physiologically stable patients, pending significant technological and economic breakthroughs. These findings also underscore the importance of large prospective collaborations, such as The Society of Thoracic Surgeons Robotic Registry and The International Society for Minimally Invasive Cardiothoracic Surgery multicenter initiatives, in establishing standardized outcome reporting and informing patient selection. Continued registry-based evidence will be critical to guide the design of future randomized trials that can definitively define the role of robotic CABG within contemporary coronary revascularization strategies.
Strengths and Limitations
This study has several notable strengths, including comprehensive risk-of-bias and certainty assessments using ROBINS-I V2 and GRADE methodologies and the inclusion of reconstructed time-to-event data for detailed survival analysis. Stratified subgroup analyses by CAD anatomy added details on how treatment effects varied with follow-up duration, offering additional insight. These methodological strengths enhance both the rigor and clinical applicability of the findings.
However, important limitations remain. All included studies were retrospective and nonrandomized, with potential for confounding and selection bias. In addition, although the definition of R-CABG was standardized across studies for this analysis, the included procedures spanned TECAB and RA-MIDCAB techniques with the variable use of cardiopulmonary bypass, which may influence perioperative outcomes. Although subgroup analysis was not feasible due to limited reporting, this heterogeneity reflects the real-world diversity of R-CABG practice and underscores the need for standardized procedural reporting in future studies. Repeat revascularization and cardiac-specific mortality could not be analyzed because they were inconsistently reported in the source studies. Future prospective registries with standardized outcome definitions would enable a more comprehensive comparison of procedural durability. Furthermore, cerebrovascular events were rarely reported; only 1 study provided stroke-specific data, precluding expansion of MACE to MACCE. As such, intertechnique comparisons of stroke risk could not be reliably performed. Moreover, even lesions categorized similarly, such as LAD or LM disease, can differ substantially in anatomical complexity, lesion morphology, and technical difficulty, which complicates comparisons across studies and may introduce unmeasured confounding in treatment outcomes. Finally, access to robotic surgical platforms remains limited, especially in developing countries, where cost, infrastructure, and training requirements may restrict widespread adoption and generalizability of these findings.
Conclusions
In this meta-analysis of 6 nonrandomized studies, R-CABG was associated with similar all-cause mortality but a significantly lower risk of TVR, MI, and MACE compared with PCI, both in patients with complex CAD and isolated LAD lesions. These findings suggest that R-CABG may offer durable revascularization benefits with a favorable safety profile in selected patients. Beyond comparative outcomes, the broader implication of this work lies in demonstrating that robotic CABG can extend the long-term benefits of bypass grafting while improving recovery and patient acceptance. However, real-world dissemination still depends on the establishment of dedicated robotic programs, multidisciplinary team training, and institutional investment in specialized infrastructure. As technology, automation, and training pathways continue to evolve, R-CABG may become a central component of modern coronary revascularization strategies, bridging surgical durability with minimally invasive delivery. However, given the observational nature of the data, procedural heterogeneity, and variability in lesion characteristics, even within similar anatomical categories, future randomized trials are needed to validate these results and to define optimal patient selection criteria for robot-assisted revascularization.
Supplemental Material
sj-docx-1-inv-10.1177_15569845261457424 – Supplemental material for Robot-Assisted Coronary Artery Bypass Versus Percutaneous Coronary Intervention in Patients With Coronary Artery Disease: A Meta-Analysis
Supplemental material, sj-docx-1-inv-10.1177_15569845261457424 for Robot-Assisted Coronary Artery Bypass Versus Percutaneous Coronary Intervention in Patients With Coronary Artery Disease: A Meta-Analysis by Mohamed Doma, Edmundo Damiani Bertoli, Gustavo Rovari, Adham Ramadan, Luena Seferasi, Mangesh Kritya, Ghazal Sanadgol, Ibrahim Kamel, Shanmukh Sai Pavan Lingamsetty, Yehia Karara, Lucas Cael Azevedo Ramos Bendaham, Motahar Hosseini, Arnar Geirsson, Chase R. Brown and Andrew M. Goldsweig in Innovations
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Geirsson is a consultant for Edwards Lifesciences, Medtronic, and enableCV. Dr Goldsweig reports speaking for Philips and Boston Scientific as well as consulting for Abbott, Occlutech, and Conformal Medical. None of these relationships are relevant to the submitted manuscript. No other authors report relationships with industry to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.