
Abstract
Research of intimate partner abuse has not adequately assessed the role of gender in situational couple violence (SCV). This research examines gendered effects of SCV on outcomes using longitudinal data from the United States National Survey of Family and Households. Results show gender asymmetries in physical health, depression, and fear outcomes of respondents exposed to SCV. Women exposed to physical SCV are less likely to report good physical health and more likely to report depression and fear than control-group women. No significant relationships are found for men. Implications suggest inclusion of outcomes when assessing gender symmetry in intimate partner abuse.
Keywords
Introduction
Within research of heterosexual intimate partner abuse (IPA), there is a heated debate over the role of gender in abusive relationships. Some research indicates that men and women use violence at approximately equal rates (Archer, 2000; Dutton, 2006; Fiebert, 2004; Straus, Gelles, & Steinmetz, 2006). This “gender symmetrical violence” is typically found by researchers who identify with the “family violence perspective” (Johnson, 2006, p. 1004). Other research indicates that heterosexual IPA is gender asymmetrical and primarily a problem of males who assault or kill female partners (Belknap & Melton, 2005; Sillito & Salari, 2006; Tjaden & Thoennes, 2000b). This “gender asymmetrical violence” is often found by researchers who follow the “feminist perspective” (Johnson, 2006, p. 1004). Although it is acknowledged that not all research can be clearly classified as “family violence” or “feminist” research, it is important to study the two perspectives generally to gain a better understanding of the overall gender debate in IPA.
Researchers from both perspectives have attempted to reconcile the differences in findings between groups. One prominent theory explains that differences in sample selection have led the two groups to study two types of violence (Johnson, 1995, 2008). Specifically, research from the family violence perspective generally examines samples of low-level violence (referred to as “situational couple violence”), whereas research from the feminist perspective generally examines samples of severe violence (“intimate terrorism”).
However, sample selection is not the only methodological difference influencing results of the two groups; research instruments and measurements also influence the conflicting outcomes. This research first examines methodological differences between family violence and feminist research, and then uses empirical research to examine whether methodological changes reveal gender asymmetries among couples experiencing low-level violence.
Review of Literature
Methodological and Conceptual Differences Between Groups
As was mentioned in the introduction, current theory assumes that differences in family violence and feminist research findings are due to sample selection. Family violence sampling techniques typically lead to research of couples experiencing situational couple violence (SCV). Johnson, (2005) first coined the term, but it is similar in meaning to terms couple fights (Stark, 2007, p. 234), or minor violence (Gelles, 2007, p. 406) used by other researchers. This research uses Johnson’s term to refer to violence that is used by both men and women, is generally not severe, results in low rates of injuries, and does not escalate over time. SCV usually takes place in the context of an argument, rather than in the context of a pattern of controlling behavior in the relationship. Some researchers believe it is the most common form of intimate partner abuse (Johnson, 2006, 2008; Johnson & Ferraro, 2000).
Research and theory (Johnson, 2008; Kimmel, 2002; Stark, 2007) have identified that situational couple violence is often studied through the use of population surveys. Stark explains that,
The majority of incidents population surveys identify as domestic violence are properly understood as fights in which one or both partners use force to address situationally specific conflicts [wherein] neither [partner] is sufficiently fearful to seek outside assistance, both partners view the use of force as a legitimate (if not necessarily desirable) form of conflict resolution, and injury is very rare (Stark, 2007, p. 234).
Family violence research of “family conflict” (Kimmel, 2002, p. 1338) typically focuses on situational couple violence. Although some family violence research focuses on small samples of young adults or college students, where IPA is more common and less gendered (Romans, Forte, Cohen, Du Mont, & Hyman, 2007), family violence research typically focuses on large national samples of “family conflict.” Due to the nature of large telephone samples, these studies often undercount severe violence (Anderson et al., 2008; Brush, 1990; Salari & Baldwin, 2002). However, because large national samples often place family conflict into the context of an argument, these samples are ideal for identifying and studying “couple fights” or “SCV” in large samples.
In contrast, feminist research often examines research samples from domestic violence shelter populations, domestic violence service providers, police data, or medical facilities servicing IPA victims (Das Dasgupta, 2007; Melton, 1999; Ristock, 2003; Stark & Flitcraft, 1996). These sampling techniques lead to an oversampling of severe violence (Johnson, 2006, 2008; Johnson & Ferraro, 2000). Countless research studies by feminist authors have identified females to be the primary victims, and males the primary perpetrators of severe violence in these samples. Although typical feminist samples are best for examining injuries and severe violence, they are not ideal to study SCV because clients in these agency samples are not likely to be experiencing mild violence.
Sample size explains a portion of the conflicting findings between family violence and feminist research. Nonetheless, this explanation is contradicted by findings of gender asymmetries in several large research samples. For example, research using the National Violence Against Women Survey (NVAWS) found asymmetrical gendered violence even though researchers were using a large national sample (Tjaden & Thoennes, 1998, 2000b). The same is true of the National Crime Victimization Survey (NCVS; Catalano, 2007). In addition, national crime statistic analysis identifies that a majority of intimate partner homicide victims are female (Bureau of Justice Statistics, 2007). The difference between the NVAWS, NCVS, and large surveys typically used in family violence research is that the NVAWS and NCVS include broader measurements of violence than do typical family violence surveys. The NVAWS, NCVS, and other similar crime-victim surveys include measures of sexual violence, violence from previous partners, violence frequency, violence severity, and injury. Moreover, these studies do not assume that violence always happens in the context of an argument. Instead, the studies examine violence that respondents perceive to be a crime (Kimmel, 2002). By so doing, SCV may be underreported in these samples, whereas severe violence may be reported more frequently. This is evidenced by differences in reported rates of violence in the two types of national surveys. The NVAWS, NCVS, and other similar surveys often have lower rates of family violence but higher rates of severe violence reported. In contrast, typical family violence surveys, including the National Family Violence Survey, have higher reported percentages of violence in families, but lower rates of severe violence or injuries (Caetano, 2008; Kimmel, 2002; Tjaden, 1998).
Furthermore, when SCV is examined by feminist researchers, it is not necessarily examined for gender differences. For example, Johnson and Leone (2005) compared physical health and psychological health outcomes for victims of intimate terrorism and SCV using the NVAWS. They found that victims of intimate terrorism experienced poorer outcomes than did victims of SCV. While their research showed significant differences in outcomes for victims of intimate terrorism compared to victims of SCV, the sample was limited to outcomes of married women. The exclusion of male outcomes did not allow for assessment of gender differences in outcomes. In addition, the research compared victims of intimate terrorism to victims of SCV, but did not account for poor outcomes of SCV compared to non-violence-exposed individuals. This did not allow researchers to examine whether or not SCV can have a negative effect on outcomes when compared to a control group. Although Johnson and Leone’s research was monumental in examining the differences between intimate terrorism and SCV, it was unable to provide crucial information about gender in SCV outcomes. Further research is needed to determine gender differences and to examine the effects of SCV compared to a control group. Because Johnson and Leone’s research was cross-sectional, longitudinal research could indicate whether poor outcomes and violence are correlated or whether there is a causal relationship between the two.
Although the focus of this research is not to delineate differences among surveys, it is important to recognize that current theory identifying sample size and selection as the reason for differences in family violence and feminist findings is incomplete. This is an indication that in addition to sample size or selection, methodologies and conceptualizations of key terms contribute to differences in findings (Melton & Belknap, 2003).The principal methodological difference between family violence and feminist research is that family violence research primarily relies on use of the “Conflict Tactics Scale” (CTS) to measure IPA. The CTS assumes that violence is in the context of an argument and focuses on the rates of men and women who have used violence over a 1-year period with a current partner (Straus, 1979; Straus, Hamby, Boney-McCoy, & Sugarman, 1996). By measurement of violence with the CTS, “Any couple where either the husband hit the wife, or the wife hit the husband—even if it was ‘just’ a slap or push—was counted as having been violent that year” (Straus et al., 2006, p. 205). To reiterate, any time a respondent reports that he or she has ever hit, pushed, grabbed, shoved, slapped, or tried to hit another person, he or she is regarded as a violent aggressor or perpetrator (Dowd, 2001; Dutton, 2006; Straus, Gelles, & Steinmetz, 1986).
The CTS, as it is presently used, can identify if a partner has ever used violence, but it cannot identify if that violence was actually “symmetrical” because it does not account for context, identify self-defense, or quantify the force or extremity of the violence. Moreover, the CTS neglects assessment of violence from previous partners, stalking, violence prior to the past 12 months, sexual violence, homicide, or nonviolence coercion or control tactics in the relationship. Each of these unmeasured forms of IPA is more likely to be perpetrated by males who harm females (Davies, Ford-Gilboe, & Hammerton, 2009; Dobash, Dobash, Cavanagh, & Lewis, 2004; Melton & Belknap, 2003; Tjaden & Thoennes, 1998). By using the CTS alone (which assesses only a small part of the abuse spectrum), family violence research has a tendency to overestimate gender symmetry in SCV.
The CTS is the most widely used instrument for measuring IPA (Smith, Earp, & DeVellis, 1995), and feminist research cannot entirely avoid use of the CTS if examining existing data. An important distinction is that feminist research samples do not rely heavily on the CTS. Feminist research that does employ the CTS acknowledges the shortcomings of the CTS (Das Dasgupta, 2002; Kimmel, 2002). When possible, feminist research uses additional research instruments that measure violence outcomes, violence frequency, violence severity, injuries, stalking, sexual violence, or violence from previous partners. Instead of relying strictly on frequencies of violence reporting, feminist research often uses qualitative assessments of violence, and contextualizes meanings, motives, and outcomes behind violent acts (Houry et al., 2008; Johnson, 2005, 2006; Leone, Johnson, & Cohan, 2007; Melton & Belknap, 2003; Stark, 2006).
Conceptual and theoretical differences between family violence and feminist research may also contribute to differences in methodologies and research findings. The family violence research perceives couple violence in the context of disagreements or arguments, wherein violence is used mutually by males and females. From this perspective, it is understood that some violence is acceptable for solving disagreements and that social learning of violence is a primary social cause of IPA (Gelles et al., 2007). IPA is researched in conjunction with other forms of family violence, and gender is seen as one of many contributing factors explaining conflict in families (Dutton, 2006; Dutton & Golant, 1995; Gelles, 1984; Gelles et al., 2007; Straus et al., 2006). These conceptualizations of the gender and violence are compatible with use of the CTS because the CTS measures violence in the context of an argument, and results using the CTS indicate that men and women are both involved in family conflict (Fiebert, 1997).
On the other hand, feminist research conceptualizes violence as result of the gendered nature of society. Male violence is backed by a history of legal and social sanctions that legitimize patriarchal control over women (Dobash & Dobash, 1979; Pleck, 2004). In a classic feminist writing, Brownmiller explained that there is a “Conscious process of intimidation by which all men keep all women in a state of fear” (1975, p. 7). Although she was referencing violence through rape, her explanation is key to understanding that the patriarchal supremacy creates an environment wherein male violence is qualitatively different from female violence.
In addition to male advantage through historical dominance, men are often socially paired with women who are physically smaller and economically more vulnerable than themselves. Furthermore, men receive encouragement to be violent, and socialized training in violence use, where women are socially barred from its use (Anderson, 2005; Anderson & Umberson, 2001). This creates a male advantage in the ability to perform violence when it is used. Assuming that partner violence can be “symmetrical” assumes that all other things are equal, which they are not. Until gender equality is a reality, gender symmetrical violence cannot exist because of the gender inequalities that precede violence use or victimization. Feminist conceptualizations of gendered violence and gender symmetry are less compatible with the CTS, and often necessitate choosing samples and research instruments that can address gender, context, and outcomes of violence in a way that is not possible with the CTS alone.
It is problematic that family violence and feminist research study different types of violence, using different methodologies and different conceptualizations of violence. Low rates of injuries in SCV, coupled with high rates of “mutual violence” in research using the CTS, have led to the assumptions that situational couple violence is somehow less gendered than other types of intimate partner abuse (Fiebert, 2004; Prospero, 2008; Straus et al., 2006a). Because there is little research crossover between the two groups, it is unknown whether the finding of “gender symmetry” in SCV is a factor of methodologies, or if this type of violence is truly less gendered than other IPA.
Although empirical and theoretical contributions by feminists have been essential in illuminating the gendered nature of more severe intimate partner abuse, a crucial weakness remains: neither feminist nor family violence research has sufficiently challenged the assumption that SCV is less gendered than other types of IPA. Feminist research has claimed that gender symmetry in situational couple violence is “mythical” and the result of a “meaningless measure of symmetry” (Johnson, 2008, p. 108), yet feminist research to this point has not sufficiently studied gender within this type of violence, presumably because of typical data limitations in existing samples of SCV. By neglecting analysis of SCV using a feminist perspective, research has largely failed to identify asymmetries that may exist among couples experiencing SCV. If feminists were to address the issue of SCV, and if asymmetries were found, it would further strengthen the feminist argument that IPA is gendered, and that females are its primary victims.
Examining SCV through the feminist research perspective is difficult because of the aforementioned shortcomings in data of existing SCV samples. It is not entirely possible to overcome the shortcomings of existing SCV data. Yet there are ways to examine the data using a feminist research perspective. As was mentioned above, feminist research often focuses on gender, meanings, motives, and outcomes of violent acts (Houry et al., 2008; Johnson, 2005, 2006; Leone et al., 2007; Melton & Belknap, 2003; Stark, 2006) rather than on frequencies of reported violence. This research focuses on gender and violence outcomes (specifically physical health, depression, and fear) in SCV; previous research has identified poor physical health, depression, and fear as negative outcomes of IPA victimization. This analysis of symmetry of outcomes, as opposed to symmetry of measured violence frequencies, may correct for “gender symmetry” measurement tendencies typical of SCV research.
Physical Health Effects of IPA
Until recently, the health risk of IPA was primarily assessed as a direct result of injuries associated with physical violence. However, research now indicates that intimate partner abuse victimization can serve as a catalyst for both direct and indirect health problems (Coker et al., 2002; Coker, Smith, Bethea, King, & McKeown, 2000). Negative health effects can be the result of physical violence, sexual violence, or emotional abuse (Centers for Disease Control [CDC], 2008; Coker et al., 2000, 2002). In addition to the health risks associated with injuries, exposure to abuse is associated with higher rates of diabetes, arthritis, current asthma, current activity limitations, and heart disease for women. It has also been correlated with higher rates of current asthma, and current activity limitations for men (CDC 2008). For both males and females, physical victimization has been linked to increased risk of self-reported current poor health, or developing chronic disease (Coker et al., 2002). While no typology has proven effective to identify perpetrators of intimate partner abuse, Cronholm theorizes that perpetrators of violence “may appear more normal and healthy in contrast to their partners who have been devastated by victimization” (Cronholm, 2006, p. 210). This research will examine self-reported current poor health.
In studying SCV, identification of health outcomes may be especially helpful because the current measures of the CTS do not account for context of violence. It is not possible to know from reported rates of violence alone whether someone was using violence in aggression or in self-defense. Yet, by identifying exposure to abuse, and combining the information on health effects of IPA on victims and perpetrators, health outcomes resulting from SCV can be used to classify primary victims in intimate partner abuse. These theories and findings suggest that victims may report more negative health outcomes, while perpetrators may appear healthier than victims (Cronholm, 2006).
Emotional Health Effects of IPA: Depression and Fear
In addition to negative physical health outcomes associated with IPA, victims are at higher risk of depression, fear, and other negative emotional health problems than nonvictims are. Depression is one of the most common mental health consequences of intimate partner abuse (Campbell, 2002). Women who experience IPA show more depressive symptoms than nonabused women (Campbell, 1997). IPA has been associated with increased risk of depressive symptoms for both male and female victims (Coker et al., 2002; Fergusson, Horwood, & Ridder, 2005). Whereas some women may experience depression before abuse, there is evidence that even in women who did not report depression before violence exposure, intimate partner abuse can trigger depression. Moreover, long-term depression decreases as intimate partner abuse declines (Campbell, 2002; Campbell & Soeken, 1999; Silva, McFarlane, Soeken, Parker, & Reel, 1997).
There may be a gendered relationship between depression and IPA. Although research has indicated that women often suffer depression because of abuse victimization (Campbell, 2002; Golding, 1999), aggression is one of the best predicting symptoms for major depressive disorder in men (Palsson, Sigurasson, Aevarsson, & Olafsdottir, 2009). Moreover, depression is often a precursor to aggression (as opposed to a result of aggression) for men (Dietmar, Edda, & Siegfried, 2005). Unfortunately, it is not possible to identify the cause of depression in this research. This research can, however, identify whether or not there is a significant relationship between physical violence and depression, and whether or not there are gender differences in this relationship.
The literature suggests that increased fear is another consequence of intimate partner abuse victimization. Reports indicate that almost 12% of female victims, and almost 2% of male victims, feared an intimate partner to the extent that the fear prevented them from reporting victimization (Tjaden & Thoennes, 2000a). Other studies have indicated that IPA is more likely to cause fear for women than for men; females who have experienced IPA in their lifetime report significantly higher levels of emotional distress and fear than do men (Campbell & Lewandowski, 1997) or nonabused women (Lipsky & Caetano, 2007).
Although Johnson (2008) associated fear with exposure to severe violence, by another author’s definition, “battering involves a systematic pattern of using violence . . . to induce fear” (Osthoff, 2002, pp. 1526-1527). Within this definition, fear is associated not only with severe violence but also with repeated violence, which is not necessarily severe. It is possible that victims of situational couple violence will also experience higher fear than do nonvictims. This possibility will be examined in the research presented in this article.
Conclusions
In conclusion, a review of current literature indicates that methodological and conceptual differences between family violence and feminist research have left a gap wherein gendered violence has not been adequately assessed among couples in population-based samples. Differences in sample size, sample selection, and research instruments have led to conflicting findings in family violence and feminist research. Assessing outcomes of violence as a measure of symmetry allows researchers to test the current assumption of gender symmetry in low-level couple violence. In an effort to better understand gender in SCV, this research will examine gender symmetry in physical health, depression, and fear outcomes.
Research Question and Hypotheses
This research addresses whether or not there are gender symmetries in physical health, fear, and depression outcomes for respondents experiencing situational couple violence. It focuses on gender and violence outcomes (as opposed to focus on violence frequencies), as is typical of the feminist research perspective. The research question is as follows: “Are there gender differences in physical health, depression, and fear resulting from exposure to SCV?”
Hypothesis 0 (H0): There are no measurable gender differences in physical health, depression, or fear resulting from exposure to physical intimate partner abuse in SCV.
Hypothesis 1 (H1): There are measurable gender differences in physical health, depression, or fear resulting from exposure to physical intimate partner abuse in SCV.
Please note that findings supporting the null hypothesis would not necessarily indicate “symmetrical violence” in SCV. Instead, null findings would indicate that inadequacies of the data do not allow for full assessment of SCV. This would signify a need for feminist research to collect data that can assess SCV using more complete measures of the meanings and motives of violence, in addition to a thorough examination of violence from previous partners, sexual abuse, homicide, and other types of violence unmeasured by the CTS. On the other hand, findings supporting the alternative hypothesis would signify the possibility that feminist research may examine existing data samples of SCV for evidence of gender asymmetries resulting from abuse exposure.
Method
Data
This research uses the U.S. National Survey of Family & Households (NSFH), a large nationally representative data set that surveyed respondents across the United States from 1987 to 2003. As such, the NSFH is primarily composed of the reports of couples experiencing no partner violence, or situational couple violence (Johnson, 1995, 2008; Stark, 2007). In addition, the NSFH contains responses by both members of couples, which family violence research has identified as an important factor in measuring violence (Bohannon, Dosser, & Lindley, 1995). These data are similar to data used in family violence research that often show gender symmetry in violence.
Violence indicators in the NSFH are measured using a modified CTS. It may seem counterintuitive to examine a sample that uses a modified CTS when the focus of the research is on inadequacies of current SCV research. However, the NSFH is ideal for measuring SCV because it assumes that violence is in the context of an argument. By studying SCV using the feminist perspective, and by including assessment of longitudinal violence outcomes, this research is innovative in avoiding the previous research technique of reducing SCV to frequency counts. This research attempts to move beyond surface-level assessments of sex-frequencies of violence to examine how this violence affects outcomes within the context of a gendered social system.
The NSFH is a panel data set with three waves; the first wave began in 1987, and the last wave ended in 2003 (Bumpass & Sweet, 2003). Although these data are older than is generally preferred, the research goal is not to identify current trends or rates of violence; the research focus is only on whether or not there are measurable asymmetries in outcomes related to exposure to SCV. This makes the relatively older data acceptable for this research.
The NSFH began with a sample of 13,007 individuals in 9,637 households in the first wave. Only heterosexual couples were included in the research. In the second wave, 87% of initial respondents were interviewed (the overall response rate was 81.7%). More than 80% of the spouses and 70% of former spouses were also interviewed. Because of funding shortages, the sample size of the third data wave was reduced, and only 72% of the original sample was interviewed (Bumpass & Sweet, 1988, 1994, 2003).
The NSFH includes data on individuals who are married, divorced, remarried, widowed, cohabiting, and never married. The research sample is restricted to individuals who were not widowed due to the potentially negative effects widowhood can have on health (Lee & Carr, 2007). The NSFH asks a range of questions about violence exposure to those who are married or cohabiting, but information on violence exposure is very limited for unmarried or noncohabiting respondents. Because of this, the study sample is restricted to individuals who were married or cohabiting in at least two points of the data. In addition, the sample is restricted to individuals with responses to model variables in at least two of the three waves, and individuals younger than 70 at the first wave.
One factor that makes the NSFH unique is that it includes assessments of both partner violence and individual health outcomes, along with traditional demographic variables that are often collected in survey research. These variables, coupled with the longitudinal nature of the data, make it possible to assess whether or not there are gendered differences in physical health, depression, and fear outcomes when respondents are exposed to intimate partner abuse.
Gender stratification
It is notable that models are stratified by gender in all analyses of this research. This is done for several reasons. Because physical health, fear, and depression may be reported differently by males and females (Duetz, Abel, & Niemann, 2003; Gorman & Read, 2006), stratifying by gender allows for analyses without including complex interaction variables between gender and other variables. Including gender as an independent variable would not adequately acknowledge that health and outcomes might be experienced or reported differently by each group due to the nature of gender rather than the nature of violence.
By comparing each gender to itself, the research is able to control for immeasurable effects of gender on outcomes. Traditional measurements of “male” or “female” as independent variables fail to capture the complexity of what it really means to be a “man” or a “woman” in a gendered society. Sex as an independent variable “ignores the complex ways in which gender operates in social interactions” (Anderson, 2005, p. 856). In other words, using sex as an independent variable would assume that sex is only an individual characteristic and would assume that when research controls for gender, it holds all other things equal. However, gender is much more than an individual characteristic of respondents; it is a characteristic of social interactions (Anderson, 2005; Kimmel, 2008). For example, society perceives, administers, and teaches violence differently by gender. Men’s violence is interpreted as “masculine” when used against other men; women’s violence is often perceived as being gender inappropriate, or as being less threatening than male violence (Anderson 2005). Simplifying “gender” to a report of sex ratios cannot contextualize the complexity of the relationship between gender and all other variables.
Because of this, research attempting to capture “gender” rather than “sex frequencies” may stratify samples by gender (Anderson, 2005). This stratification allows assessment of the effects of violence and other factors when holding gender as a constant in each model. This provides for a thorough assessment of the effects in the context of a gendered social system instead of a simple count of sex frequencies (Anderson, 2005). By stratifying the models by gender, this research removes the assumption that the only difference between the groups is sex identification of “male” or “female.” By comparing males to males and females to females, gender is held as a constant in each analysis.
This is not the traditional way that family violence research has examined the effect of gender on violence. Stratification by gender creates a complexity in comparing results or assessing “symmetry” and “asymmetry” of outcomes. In essence, what this research can do is determine if violence affects outcomes for females, and determine if violence affects outcomes for males. Then, because each gender stratified model contains the same independent and dependent variables, the stratified results are compared to determine if outcomes are the same, or “symmetrical,” for men and women. If violence significantly affects outcomes for both males and females, this indicates some level of “symmetry.” If results vary for males and females, this indicates some level of “asymmetry.” Although this is not a perfect measure of symmetry, it allows for an analysis of gender, which has largely been left out of current analyses of SCV (Anderson, 2005).
Dependent variables: Physical health, depression, fear
The dependent variables for the logistic regression analyses in this study are physical health, depression, and fear. Each measure was self-reported. To measure physical health, the NSFH asked respondents the following question:
Now I’d like to ask you some questions about your health. Compared with other people your age, how would you describe your health? Would you say it is very poor, poor, fair, good, or excellent? (Bumpass & Sweet 2005)
1
Although this measure is reliant on self-report of respondent rather than health care records, the use of self-reported health to measure morbidity is common in epidemiological research, and agreement between self-reported and medical record health is high for many measures of morbidity (Barber, Muller, Whitehurst, & Hay, 2010). In the random effects logistic regression analysis, those with good health or better (coded “1”) are compared to those with fair health or worse (coded as “0”).
The division was made between good and fair health because it was the best way to split the groups into somewhat similar portions, while maintaining categories that made sense. It would not seem logical to divide “excellent” health from “good health or worse.” Nor would it make sense to place “fair” health with those reporting good health. Because the majority of respondents report their health as good or better (each mean score was above 3.0, which is “fair,” indicating the majority of respondents said they had good health or better), this division will allow for examination of whether or not those exposed to violence experience poorer health than the average. In each random effects logistic regression model, self-reported health of women exposed to IPA is compared with those who do not report IPA exposure. The same is done for men.
Depression and fear were also self-reported in the NSFH. Respondents were asked, “On how many days (during the past week) did you feel depressed?” (Bumpass & Sweet, 2005). Responses ranged from 0 to 7 days. Respondents were also asked, “On how many days (during the past week) did you feel fearful?” (Bumpass & Sweet, 2005). Again, responses ranged from 0 to 7 days. Depression and fear are dummy coded in the random effects logistic regression models. If a respondent reported depression one or more days, it was coded as “1.” If the respondent did not report depression on any day, it was coded as “0”. The same coding is used for fear.
Predictor variable: IPA exposure
The predictor variable, or focal independent variable, in each model is physical IPA exposure. In the survey, respondents and partners were asked to identify several forms of physical aggression. Respondents were asked the following questions:
How often do you end up hitting or throwing things at each other (seldom, sometimes, very often, or always)?
Sometimes arguments between partners become physical. During the last year has this happened in arguments between you and your partner (yes, no)?
During the past year, in how many of these arguments did your partner become physically violent with you (0, 1, 2, 3, 4 or more)?
During the past year, in how many of these arguments did you become physically violent with your partner (0, 1, 2, 3, 4 or more)? (Bumpass & Sweet, 2005) 2
If either the respondent or partner reported experiencing any of these types of violence in any wave of the data, it was coded as “1.” If neither the respondent nor partner reported experiencing violence at any time in the survey data, it was coded as “0.” The rates of males and females who reported using physical violence, or who report being victims of partner physical violence, are reported in univariate analyses. The distinction between “perpetration” or “victimization” is not included in regression analyses to avoid classifying victims who use violence in self-defense as “perpetrators,” or classifying perpetrators as “victims” when they are harmed by someone using self-defense “victims.” Being exposed to violence, or not, is the only variable included in regression analyses. It is important to note that these measures of abuse are extremely limited by the data’s use of a modified CTS. The measures of violence do not include homicide, verbal aggression, sexual violence, rape, violence from previous partners, violence toward pets or other family members, stalking, or nonviolent forms of abuse (such as coercion, or control). These limitations mean that violence was likely underreported in the data set; it is unknown how many respondents in the data set experienced one (or more) of these nonmeasured forms on intimate partner abuse.
Control variables
Several demographic factors (including age, race, education, and income) influence health outcomes and are used as control variables in the models. Age is a necessary control variable when assessing health outcomes. Each respondent reported age at each wave. This is reported as a continuous variable. Previous research indicates that self-reported measures of health differ by race, ethnicity (Fletcher, 2009), and socioeconomic status (Demakakos, Nazroo, Breeze, & Marmot, 2008; Duetz et al., 2003; Matthews, Manor, & Power, 1999; Read & Gorman, 2006). In general, minority groups report poorer health than Whites (Read & Gorman 2006). In this research, race is dummy coded as “White, non-Hispanic” (1) compared to “non-White or Hispanic” (0).
In addition, persons of lower SES report worse health than those with higher SES (Demakakos et al., 2008). Education and income are used to measure SES in the data. Education is reported as the highest level of education achieved by the primary respondent, and is measured linearly as years of education. Individual income is coded as a continuous variable. Individual income (as opposed to household income) was used in analyses. Because the focus of this research is on gender instead of resources, it is important to measure income by individual gender, rather than by household resources. Although female income is lower than male income, the stratification by gender allows for inclusion of individual income in the analysis. When individual income was missing, the missing response was replaced with the sample mean of the given wave, and a dummy variable was included to indicate if the mean had been imputed for a missing variable.
It would have been preferable to differentiate between cohabiting and married couples; however, fewer than 5% of the study sample reported nonmarital cohabitation, so these groups were combined. Research indicates that health differences between married and cohabiting couples are nonsignificant (Zheng, Penning, Pollard, & Hart, 2003). Unfortunately, most of the violence questions were not asked of respondents who were not in a current relationship. Future research should be conducted on divorced or separated couples experiencing SCV. In addition to the above control variables, a linear time control is included. Period specific intercepts are included in each random effects logistic regression model to control for time at each of the three waves.
It is notable that each of these control variables could be examined as either a focal independent variable or a potential confounder. However, because the primary focus of this research is the relationship between violence exposure and the dependent variable, physical violence exposure is examined as the focal independent variable in each model. It is my hypothesis that exposure to physical intimate partner violence in SCV can cause poorer physical health outcomes and increased depression and fear. Age, race, education, and income, and a time control (wave) are selected as control variables because previous research has identified that each can affect physical and emotional health outcomes. Future research should consider assessing the effects of emotional abuse, sexual abuse, or control on health outcomes using similar control variables.
Statistical Analysis
This research uses panel data analysis. Panel data are a form of longitudinal data, where the same respondents are contacted at different points in time and repeatedly asked to respond to questions they were given at earlier time points. Construction of the data set is such that respondents may appear multiple times in the data if they responded to the survey at multiple time points. Panel data allow for comparison between time points for individual respondents and for comparison between respondents (Yaffee, 2003).
Random effects logistic regression models (xtlogit command in Stata 9 software) are used to examine whether or not violence exposure has an effect on the dependent variables in each model when controlling for age, race, education, earnings, and time. A random effects logistic regression model uses a form of logistic regression to analyze panel data. It is different from cross-sectional logistic regression because it can account for the panel-level variance of individual respondents, and it allows for between-case comparisons using all three waves of the NSFH (Allison, 2009).
There are several advantages to using random effects models over fixed effects models for the analyses in this research. The primary advantage is that using random effects models allows for between-case comparisons. Respondents who report violence exposure in the study period may have also experienced IPA prior to the study; any negative consequences of IPA exposure may already be taking place for violence-exposed respondents. Comparing respondents who experienced violence with those who did not (as is done in random effects models) allows for identification of ways violence affects health over time. This type of analysis is not possible with within-case analysis of fixed effects models. Moreover, random effects models include respondents who experienced no “change” in violence status over time. What this means is that if respondents never experienced IPA in any of the waves, or experienced IPA at all waves, they are included in random effects models. A fixed effects model requires only inclusion of cases that experienced a change in violence status. Because research interests lie in the differences between groups, as well as the differences between individuals who experienced a change in violence status, random effects models are preferred. Finally, random effects models allow for analysis of time-invariant variables (including gender and education), whereas fixed effects models do not provide coefficients for time-invariant variables (Allison, 2009; Garson, 2010).
Before conducting regression analyses, each variable was examined for distribution normality. Age and income are skewed in the data, but logging the variables resolved the problem. Results were substantively the same in models with age and income unlogged as in the logged models. Because of this, the unlogged variables are used in the reported models for ease of interpreting the results of the random effects logistic regression models. Other variables either follow a normal distribution or are dummy coded.
An overall likelihood ratio test and a test of the likelihood ratio of rho are used to insure that models are adequate fit for the data. The overall likelihood ratio test is a chi-squared test (calculated by Stata 9.1) in which at least one of the coefficients of the regressors is not equal to zero (Garson 2010). Significant findings for this test (prob. χ2 < .05) indicate a good fit for the model. rho is a measure of panel-level variance. A significant result (prob. chi bar < .5) indicates that the panel data model is better able to predict the dependent variable than the cross-sectional models (Gayle, 2003). This means when rho does not equal zero, the panel component is important. If rho is zero, the panel-level variance component is unimportant.
Results
Univariate and Descriptive Statistics
When the three waves of data for the sample are combined into one panel data set, about 41% of the sample was male and 59% of the sample was female. About 11% of the males and just above 9% of the females reported experiencing some form of physical IPA in the study period (see Table 1). Note that these numbers do not identify the gender of the victims or perpetrators of violence. Within the sample, respondents were asked if they had used violence against a partner, but reporting rates were low for both genders. Reports from respondents and partners indicated that 4.57% of men and 4.17% of women in the sample used physical violence against a partner. Almost 4% of women and 5% of men report a partner’s use of physical violence. These rates do indicate that a similar portion of men and women were reported to use violence, and to be victims of violence, in the year prior to sample collections.
Descriptive Statistics for Primary Respondents in Sample
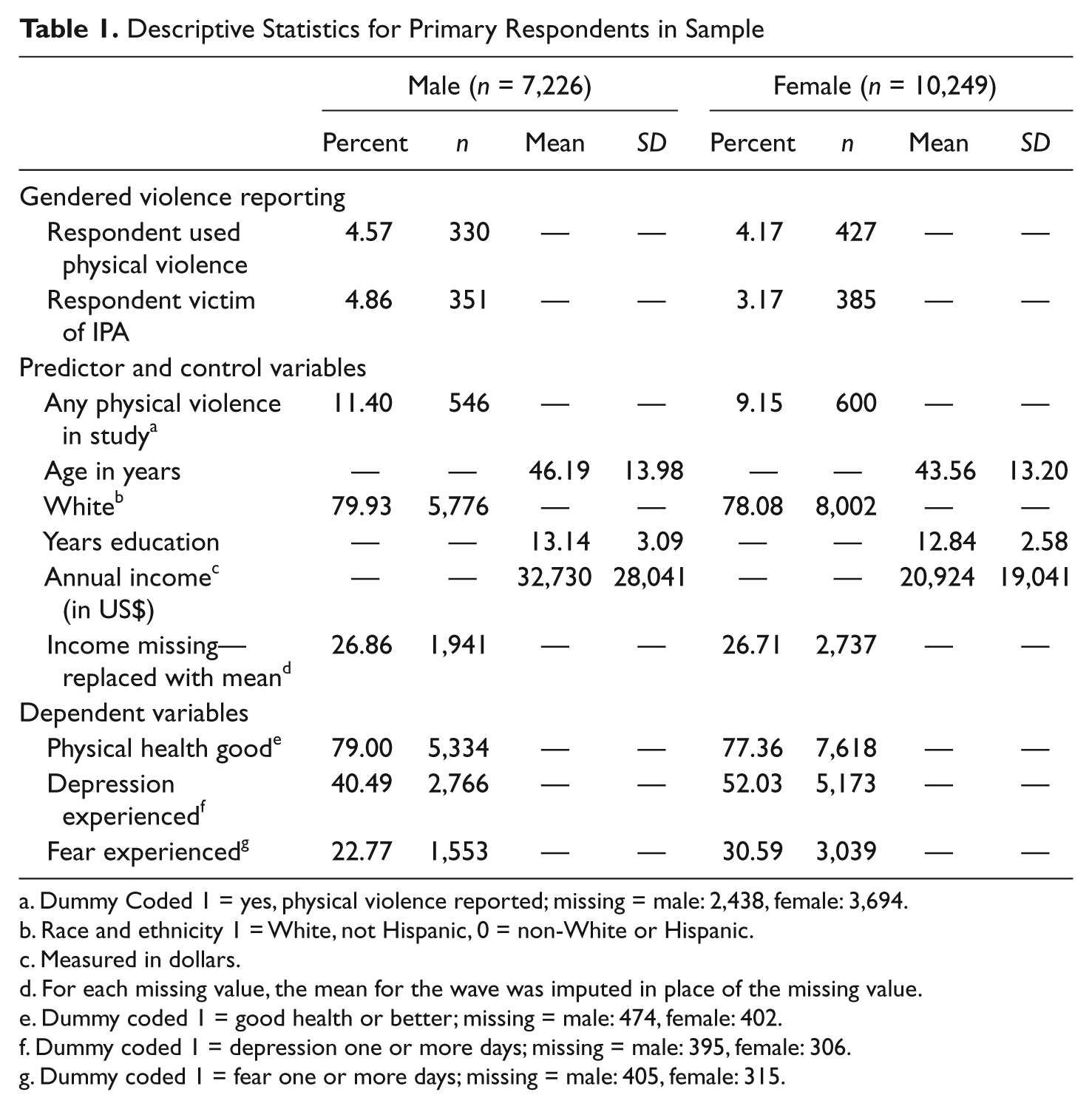
Dummy Coded 1 = yes, physical violence reported; missing = male: 2,438, female: 3,694.
Race and ethnicity 1 = White, not Hispanic, 0 = non-White or Hispanic.
Measured in dollars.
For each missing value, the mean for the wave was imputed in place of the missing value.
Dummy coded 1 = good health or better; missing = male: 474, female: 402.
Dummy coded 1 = depression one or more days; missing = male: 395, female: 306.
Dummy coded 1 = fear one or more days; missing = male: 405, female: 315.
Within the sample, men averaged 46 years old, whereas women were between 2 and 3 years younger at an average age of between 43 and 44 years. Close to 80% of men and 78% of women in the sample were non-Hispanic White. Men averaged just above 13 years of education, whereas women averaged just under 13 years of education. The average annual income was about US$11,800 more for men than it was for women. For both males and females, missing data for income were replaced with the mean income from each wave in almost 27% of the cases.
Univariate analyses of dependent variables show that men and women have very similar self-reported physical health in the study. About 79% of men and about 77% of women report having good health or better in the study. More women reported being depressed and experiencing fear than did men in the study sample; about 12% more women experience depression (52% for women compared to 40% for men), whereas about 8% more women experienced fear than men in the sample (23% of men compared to 31% of women experienced fear. These differences in rates by gender signify that it is important to stratify regression models by gender to account for differences in health, depression, and fear outcomes that are gender specific.
Random Effects Logistic Regression Models
Physical health outcomes
Random effects logistic regression models are used to assess the physical health effects of being exposed to physical IPA in the study sample. Models were stratified by gender. The dependent variable was modeled as “good health or better” (coded as “1”) compared to “fair health or worse.” Any physical IPA was the predictor variable in the model. Predictor variables and predictor variables outcomes are bold in Tables 2, 3 and 4 for ease of reading the tables. In addition to the predictor variable, variables to control for age, race, education, income, and time are included. Overall likelihood ratio tests of the models indicated that at least one of the coefficients was not equal to zero (male: LR = 190.01, p < .001; female LR = 137.70, p < .001). In addition the likelihood ratio of rho test indicates that the panel level variance is significantly better at predicting outcomes than cross-sectional models would be (male rho LR = 235.2, p < .001; female: rho LR = 324.36, p < .0001). These tests indicate that the data were a good fit for the models.
Results of the gender-stratified models indicate that for men, there is no significant difference in health outcomes if respondents are reported to experience physical IPA in the study period (see Table 2). Conversely, women who experience IPA have 53% lower odds (OR =.47, p < .001) of reporting good health or better than do women who are not exposed to IPA. For both men and women, a majority of the control variables are also significant in predicting physical health outcomes.
Physical Health Outcomes: Random Effects Logistic Regression a
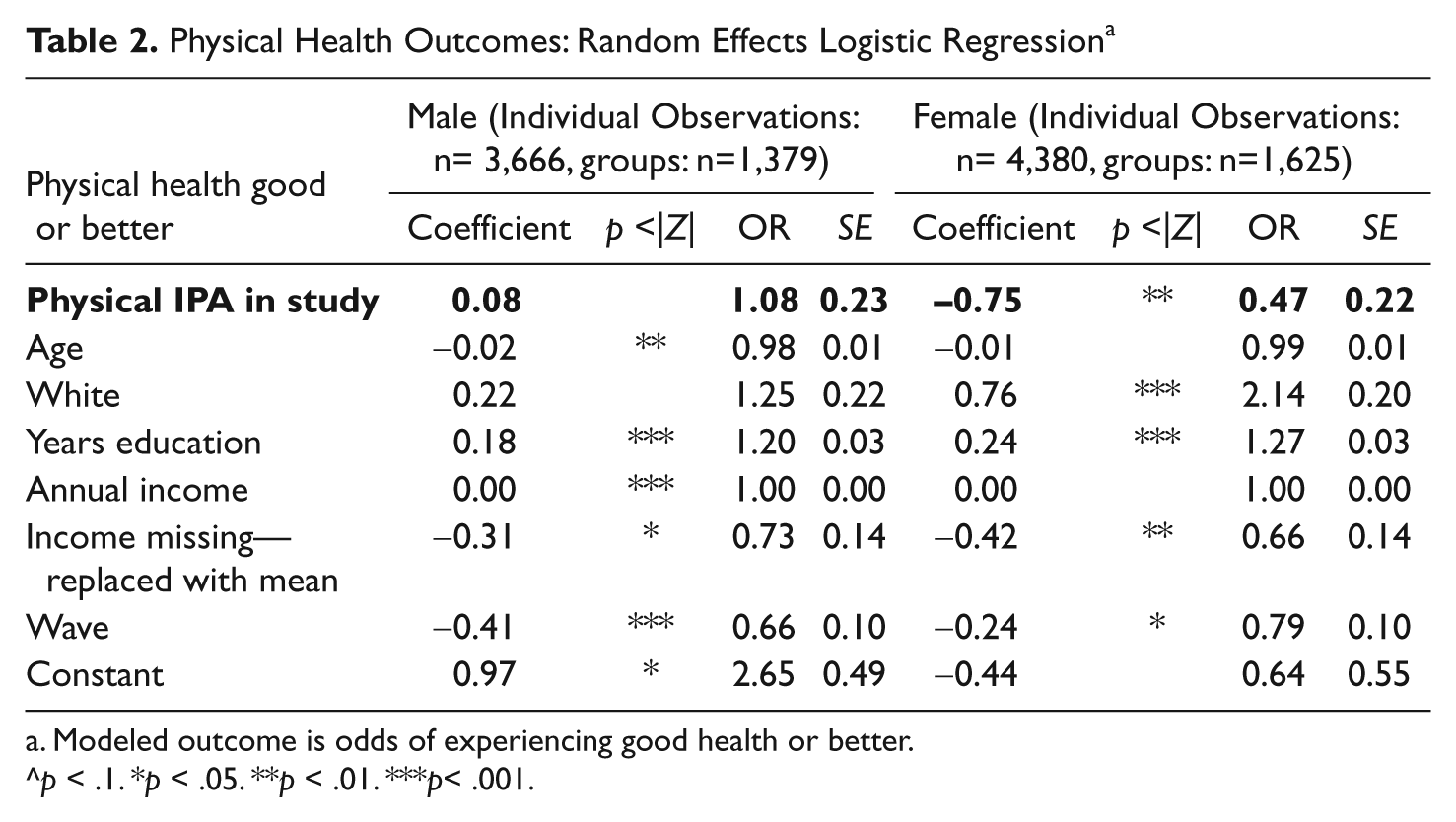
Modeled outcome is odds of experiencing good health or better.
p < .1. *p < .05. **p < .01. ***p< .001.
Depression: Random Effects Logistic Regression a
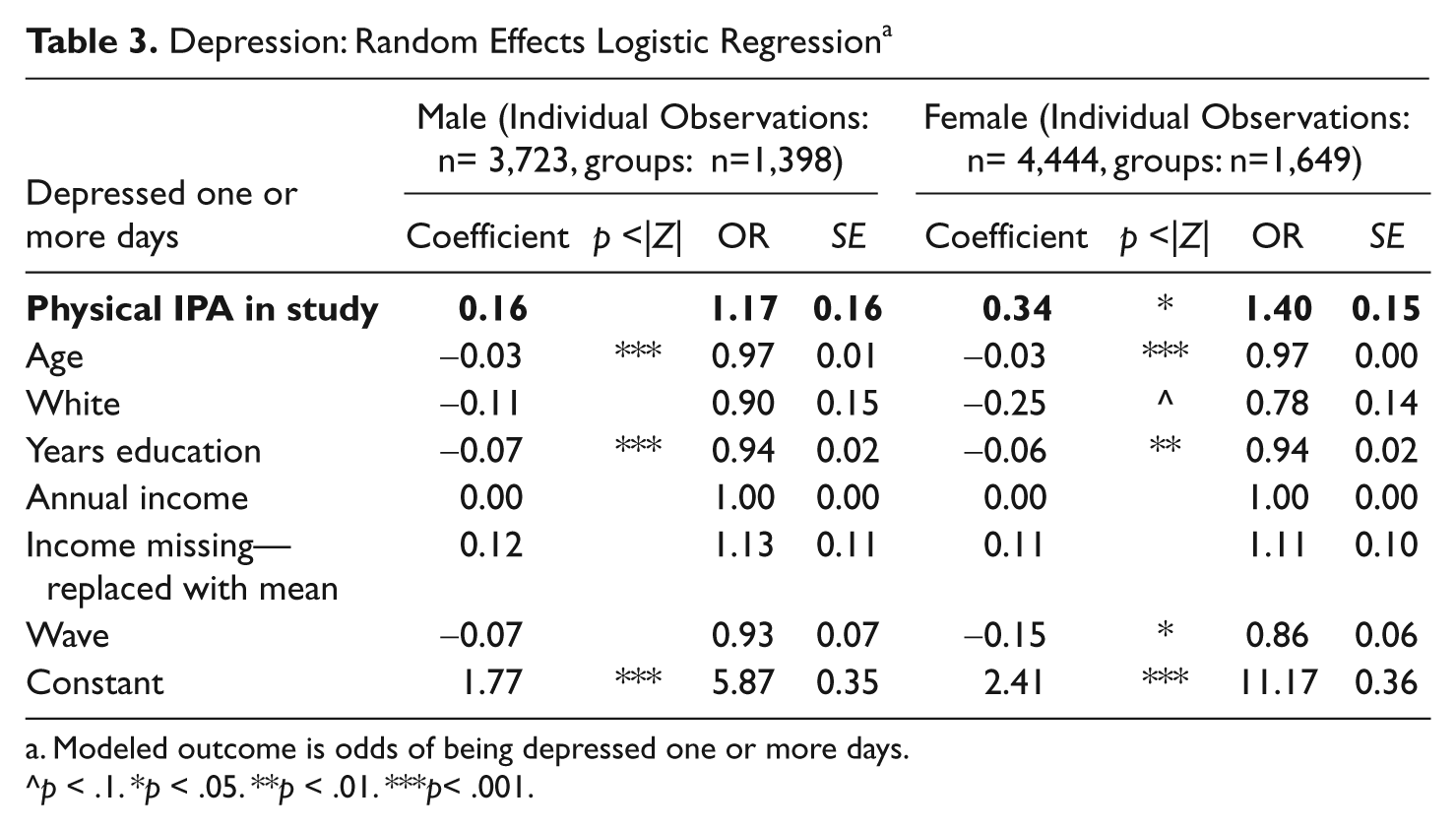
Modeled outcome is odds of being depressed one or more days.
p < .1. *p < .05. **p < .01. ***p< .001.
Fear: Random Effects Regression a
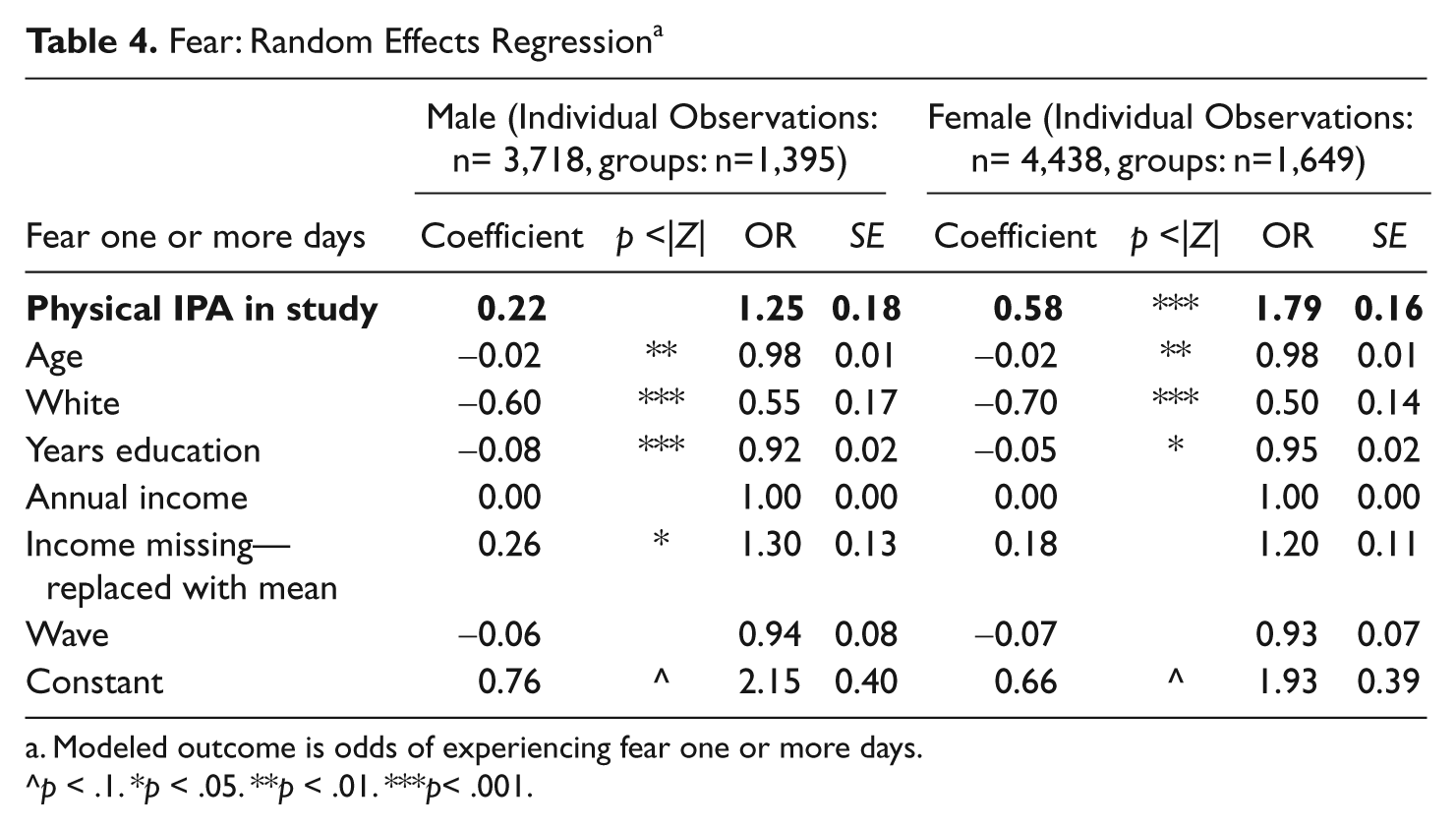
Modeled outcome is odds of experiencing fear one or more days.
p < .1. *p < .05. **p < .01. ***p< .001.
It is interesting to note that these findings indicate age as an insignificant factor leading to health outcomes for women. It is likely that this is due to the nature of the survey question assessing physical health outcomes. Because the question asks respondents to describe their health compared to others their same age, individuals with good health compared to others at younger ages may remain in good health compared to others their same age in later surveys.
Depression outcomes
Random effects logistic regression models are completed to assess depression outcomes in the study sample. Physical IPA exposure was the predictor variable in the model. In addition to the predictor variable, variables to control for age, race, education, income, and time are included in the gender-stratified models. Overall likelihood ratio tests of the models indicated that at least one of the coefficients was not equal to zero (male: LR = 79.43, p < .001; female LR = 128.03, p < .001). In addition, the likelihood ratio of rho test indicates that panel level variance is significantly better at predicting outcomes than cross-sectional models would be (male rho LR = 158.10, p < .001; female: rho LR = 117.51, p < .0001).
Results indicate that there was no significant relationship between physical IPA and depression for men (see Table 3). Conversely, if women reported experiencing IPA in the study period, they experienced 40% higher odds of reporting depression (OR = 1.4; p < .05) compared to women who reported no exposure to IPA in the study. Several control variables were also significant in identifying depression outcomes.
Fear outcomes
Random effects logistic regression models are used to assess self-reported fear when exposed to physical IPA in the study sample (see Table 4) Models were stratified by gender. The dependent variable in the model was modeled as “fear one or more days” (coded as “1”) compared to “fear no days.” Physical IPA was the predictor variable in the model. In addition to the predictor variable, variables to control for age, race, education, income, and time are included in the models. Overall likelihood ratio tests of the models indicated that at least one of the coefficients was not equal to zero (male: LR = 82.51, p < .001; female LR = 60.38, p < .001). In addition, the likelihood ratio of rho test indicates that the panel level variance is significantly better at predicting outcomes than cross-sectional models would be (male rho LR = 196.41, p < .001; female: rho LR = 124.05, p < .0001). These tests both indicate a good fit of the data with the models.
Results of random effects logistic regression models indicate that there is not a significant relationship between fear and exposure to IPA for men in the study sample. The same is not true for women. Women exposed to IPA in the study period had 79% higher odds of reporting fear in the week prior to survey collection (OR = 1.79, p < .001). Several control variables were also significant in identifying fear outcomes.
Discussion
The research presented in this article indicates support for the alternative hypothesis: There are gender differences in physical health, depression, and fear resulting from exposure to SCV. This is a breakthrough in identifying gender asymmetries in outcomes of situational couple violence. Although theory previously identified sample selection and the conflict tactics scale as barriers to finding asymmetries in this type of violence, the results of this research are evidence to the contrary. The CTS and sample choice are barriers to a complete assessment of gendered violence in SCV, but when gender and violence outcomes are placed central in the analysis, females are identified as primary victims of situational couple violence.
Females exposed to SCV were significantly less likely to experience good health when exposed to SCV, but men were not. These findings can be used to identify females as primary victims in situational couple violence. The results also indicate that there are gender differences in physical health outcomes that result from exposure to SCV. This supports previous research indicating that although both men and women use violence in relationships, females primarily sustain harm from abuse (Jacobson & Gottman, 1998; Melton & Belknap, 2003; Miller, 2005). Moreover, Cronholm’s theory explains that perpetrators do not experience the same negative health effects as their victims (Cronholm, 2006); the null finding for men’s physical health outcomes could actually be an indication of primarily male perpetration in SCV. This idea should be examined in future research of SCV.
When depression was examined in the data, females exposed to SCV had a higher likelihood of reporting depression, but for males there was not a significant relationship between SCV exposure and depression outcomes. This result conflicts with previous findings indicating that depression was related to violence for both men and women (Coker et al., 2002). However, when taken into the context of what gender may mean by gender, it could be possible that men who experienced depression as a precursor to aggression (Dietmar et al., 2005) may not have reported depression at the time of the survey. Females, who are more likely to experience depression as a result of violence (Campbell, 2002; Golding, 1999), may have still felt the effects of the depression when the survey was taken. Future research may consider assessing depression and violence exposure at closer intervals to better determine the relationship between the two.
Females exposed to SCV were significantly more likely to experience fear, but the same was not true for men. Previous research has indicated that women are more likely to fear their partners because husbands have a unique ability to use violence to produce fear (Jacobson & Gottman, 1998; Sokoloff & Dupont, 2005). Although both men and women were reported to have used similar levels of violence in this research (see Table 1), this finding is an indication that the outcomes of that violence are asymmetrical. This support’s Brownmiller’s conclusion that because men have a unique ability to create fear by use of violence, female use of violence can never be seen as equal to male use of violence (Brownmiller, 1975). Female violence does not have the same effect on males.
In Tables 2, 3, and 4, income was reported as a nonsignificant factor affecting female physical health and emotional outcomes. For physical health outcomes, this finding is explained by the significant finding on missing income being replaced by the mean. In other words, a significant portion of the female sample did not report income, and so the replaced mean had a significant effect on the outcomes. Another explanation for physical health and emotional outcomes is that this finding results from income being measured as individual income rather than household income. Traditional gender roles may lead to higher male income, and thus the female income may not be as influential as the male income. Future research focused on gender differences in resource access and resource allocation can help identify the reasons for these differences.
This research supports and strengthens the feminist theoretical argument that gender is the central risk factor for IPA victimization by showing that gender affects outcomes, even in situational couple violence, which many researchers previously assumed was nongendered. This research suggests that there are qualitative differences in male and female violence. Males exposed to female violence do not experience poorer physical health, increased depression, or increased fear. Conversely, females exposed to male violence experience significantly poorer physical health, depression, and fear outcomes. Although both men and women reported being victims of partner violence, the unquantifiable differences, or contextual differences, in male and female violence make male violence more harmful than female violence. Perhaps it is the context of SCV within a gendered system that makes SCV a danger for women. Future research should further address these issues.
The implications of these results include the need for an increased emphasis on study of situational couple violence. Through additional research of gender asymmetries in couples experiencing SCV, feminist research could gain a better understanding of the effects of intimate partner abuse and how those effects vary by gender. Future research samples of SCV should include an analysis of violence from previous partners, context of violence (including self-defense), sexual violence, nonviolent control tactics, and a better measure of violence frequency and severity. In addition, future research should attempt to identify the mechanisms through which IPA can lead to poor health outcomes.
Research Limitations
There are several limitations to the research presented in this study. Limitations lie primarily in the data and instruments. The NSFH does not account for nonviolent forms of abuse, control, sexual abuse, or for context of abuse within the relationship. Without assessment of context, sexual violence, or nonviolent abuse, the outcomes are severely limited. Because the NSFH does not ask who instigated the violence, nor if there was a motive of self-defense, results cannot indicate which gender perpetrates violence, only which gender experiences the most severe outcomes. Future research studies should include measures indicating motives behind violent acts. The NSFH did not ask noncohabiting or nonmarried respondents a full range of questions about violence. Although the data is longitudinal and follows individuals over 15 years, there is no measurement of violence before this time point. If an individual experienced violence between the waves, but not during the past year (Bumpass & Sweet, 2003), the violence was not reported in the data. This means that many individuals may have experienced IPA that was unaccounted for because the NSFH did not collect data frequently enough, and responses were limited to violence that occurred in the 1-year prior each wave of data collection.
Assessments of emotional outcomes were also limited. Measures of fear and depression asked respondents about experience with these emotional outcomes only in the week prior to data collection. This is problematic because the survey asked about violence in the past year. This means that if physical violence took place 11 months before the survey, fear or depression measured only the week before survey collection may not have captured the relationship between physical abuse and emotional outcomes. Moreover, fear and depression questions were not asked in the context of violence. Reported fear could have been fear from victimization, fear of being caught using violence, or fear unrelated to violence use. Depression could have preceded violence or could have been the result of violence. Future research should contextualize fear, depression, and violence to understand the relationship between these variables and SCV better.
Another limitation typical of IPA research is that IPA is difficult to study because of social desirability effects. It is impossible to know how many individuals in the sample were not truthful about IPA perpetration or victimization or how many victims chose not to participate in the surveys due to abuse.
Conclusions
This research examined how family violence and feminist research differ methodologically and conceptually, and then used empirical research as evidence that SCV in large samples may not be nongendered, as was formerly assumed. Previous practices of claiming “symmetry” based on frequencies of violence reported by sex have been shown to be greatly inadequate through this research of SCV. The results and discussion point toward the importance of contextualizing violence by gender and incorporating assessments of outcomes in measures of symmetry. This research asserts that females are at greater risk of negative physical health consequences, increased depression, and increased fear resulting from SCV, which was previously thought to be “gender symmetrical.” These results call for reconsideration of the role of gender in SCV. The findings of this research indicate evidence of asymmetries exists in current research samples of SCV. Researchers may consider reassessing large national samples, focusing on gender or violence outcomes, to determine if other samples also show evidence of asymmetry in SCV.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.