
Abstract
Background:
Acute pancreatitis (AP) is frequently linked to metabolic syndrome (MetS) and its individual components. Coronary artery calcium (CAC) score is also associated with MetS. This study aims to investigate the relationship between CAC and the occurrence of AP.
Methods:
This retrospective, single-center, case-control study included 352 patients admitted to a tertiary medical referral center between January 2017 and December 2023. Patients were divided into AP (case) and non-AP (control) groups, with controls matched to cases based on sex and age.
Results:
The prevalence of MetS was significantly higher among AP patients (38.2%) compared to controls (13.3%) (OR: 2.66, 95% CI: 1.72–4.32; P < 0.001). Similarly, CAC was more common in the AP group (35.5%) than in controls (10.8%) and was significantly associated with AP (OR: 3.47; 95% CI: 1.99–4.93, P < 0.001). Multivariate logistic regression, adjusted for smoking, alcohol use, gallstone history, CAC, and MetS components, confirmed associations between AP and smoking (OR: 2.23; 95% CI: 1.78–4.98, P < 0.001), alcohol consumption (OR: 1.78; 95% CI: 1.07–2.76, P = 0.027), gallstones (OR: 22.93; 95% CI: 18.22–49.82, P < 0.001), and positive CAC score (OR: 3.47; 95% CI: 1.99–4.93, P < 0.001).
Conclusions:
MetS and CAC score are significantly associated with admission for AP. Further studies are needed to explore potential causative mechanisms.
Introduction
The coronary artery calcium (CAC) score is a test used for gauging the risk of coronary artery disease. In recent years, it has become an essential predictive tool for assessing an individual’s likelihood of developing a heart attack by detecting atherosclerosis.1–5 Cardiac computed tomography (CT), through techniques such as multidetector-row CT or electron beam tomography, enables the detection and measurement of coronary calcium—a key marker of atherosclerosis. 3 Research analyzing baseline data have consistently linked CAC scores with other coronary heart disease (CHD) risk factors, including age, male sex, and diabetes duration. 4 Moreover, CAC may be an independent predictor of subclinical atherosclerosis, particularly in those with a history of metabolic syndrome (MetS) and diabetes.3–9
Several components of MetS have been independently correlated with CAC, such as abdominal obesity, insulin resistance, hypertension, and elevated fasting serum glucose. Additionally, CAC scores tend to be inversely related to high-density lipoprotein (HDL) levels. 9
Acute pancreatitis (AP) is an inflammatory disorder that can lead to severe, life-threatening complications from the inflammatory response of the pancreas. 10 Epidemiological surveys indicate that the incidence of AP has doubled over the past few decades, presenting a major health burden and significantly contributing to medical costs.11,12 The primary causes of AP are gallstones and excessive alcohol intake, though additional factors such as smoking and genetic predisposition also play causative a role. 12 While the detailed mechanisms involved in the development of AP remain unclear, there are numerous research studies seeking to ascertain potential triggers.
MetS is characterized by four interrelated factors: hyperglycemia, hyperlipidemia (especially elevated triglycerides [TGs] and low HDL cholesterol), obesity, and hypertension. 13 Despite the absence of a universally accepted explanation for MetS, prevailing evidence suggests that its components are linked through shared physiological mechanisms, including insulin resistance, visceral adiposity, atherogenic dyslipidemia, and endothelial dysfunction.14,15 As the clinical conditions characterizing MetS often co-occur beyond chance, MetS is best described as an overarching condition. It predisposes individuals to a chronic inflammatory state associated with diseases such as venous thrombosis and psoriasis.15–17 As there is a known connection between MetS and inflammation, we hypothesize that MetS may contribute to the development of AP.15–17 While some studies have linked MetS to AP severity, data with regard to it having a causative effect on AP remain scarce.10–18 Most existing research focuses on individual components of MetS, such as obesity or hyperglycemia, rather than treating it as a unified condition.
To address these gaps, we aim to investigate: the relationship between MetS and AP, the association between each MetS component and AP, and the correlation between CAC score, closely linked to MetS components, and AP.
Methods
A hospital-based case–control study was conducted at a tertiary medical referral center, where participants were classified into two groups: an AP group and a control group (without AP).
Based on the 2012 revised Atlanta classification, AP was diagnosed if at least two of the following three criteria were met: (1) an episode of acute severe upper abdominal pain; (2) serum amylase or lipase levels elevated to at least three times the upper normal limit; and (3) imaging findings consistent with AP.
Only patients experiencing their first AP episode were included, while those with recurrent or chronic pancreatitis were excluded. Controls were matched to cases based on sex and exact age. Individuals with a history of AP were excluded from the control group, and participants with a history of cardiovascular disease (excluding hypertension) were excluded from both study groups. Additionally, we only included in the study group those who had a CAC score and diagnosis of AP within 6 months of one another. Further exclusion criteria included individuals under 18 years of age, pregnant women, those who had undergone surgery within the past month, and individuals with a history of cancer.
Data were extracted from electronic case records, including the following variables: sex, age, smoking status, alcohol consumption (>14 drinks per week for women and >21 drinks per week for men), history of biliary stones, hepatitis B or C, body mass index (BMI), and blood pressure. Laboratory test results included total cholesterol (TC), TG, HDL, low-density lipoprotein, apolipoprotein A, apolipoprotein B, and fasting plasma glucose (FPG). BMI was calculated as weight (kg) divided by height squared (m2).
MetS was defined using the National Cholesterol Education Program Adult Treatment Panel III criteria, modified by the Asia–Pacific guidelines. The diagnostic criteria included:
The CAC score was assessed using cardiac multidetector CT. Coronary calcification was defined as a high-density lesion >130 Hounsfield units, following the Agatston method. CAC scoring was categorized into four stages:
The study was approved by the Institutional Review Board of Shaare Zedek Medical Center, with informed consent waived due to its retrospective and noninterventional design.
Statistical analysis
Quantitative data were expressed as mean ± standard deviation or median with interquartile ranges (25th and 75th percentiles). Independent sample t-tests were used to compare normally distributed continuous variables, while nonnormally distributed variables were analyzed using the Mann–Whitney U test. Qualitative data were presented as frequencies (n) and percentages (%), with comparisons made using Fisher’s exact test or the chi-square test.
Univariate logistic regression analysis was conducted to assess whether individual variables were predictive of AP occurrence. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. Further evaluation of OR values was performed using univariate and multivariate logistic regression models. The accuracy of predictive markers for AP occurrence was analyzed using receiver operating characteristic curves. A P-value <0.05 was considered statistically significant. Statistical analyses were performed using IBM SPSS v22 (SPSS, Chicago, IL, USA) and MedCalc software version 10 (MedCalc, Mariakerke, Belgium).
Results
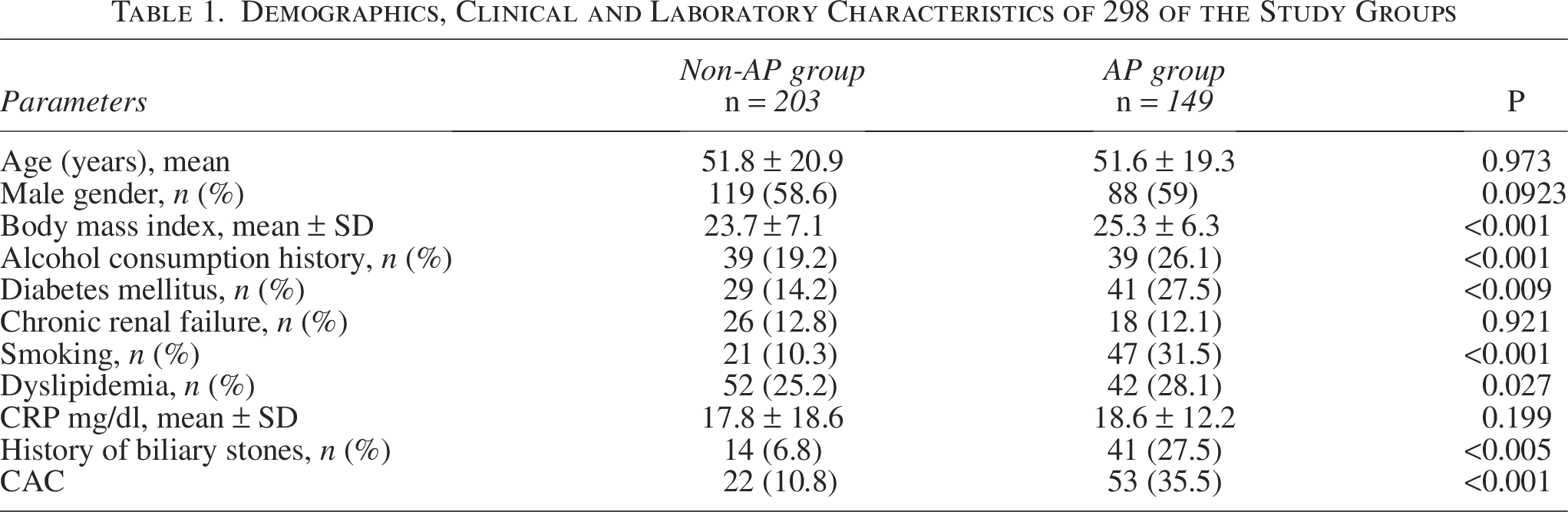
A total of 352 participants were included in the study, with 149 (42.3%) assigned to the AP group and 203 (57.7%) to the control group. No significant differences were found between the groups in terms of age (P = 0.973) or gender distribution (P = 0.923). However, AP was significantly associated with cigarette smoking (P < 0.001), a history of biliary stones (P < 0.001), diabetes (P < 0.001), and dyslipidemia (P = 0.027).
CAC was significantly more prevalent in the AP group, with 53 (35.5%) individuals testing positive for CAC compared to 21 (10.3%) in the control group (P < 0.005). Additional baseline characteristics of the study groups are detailed in Table 1.
Demographics, Clinical and Laboratory Characteristics of 298 of the Study Groups
Effect of CAC and MetS on AP
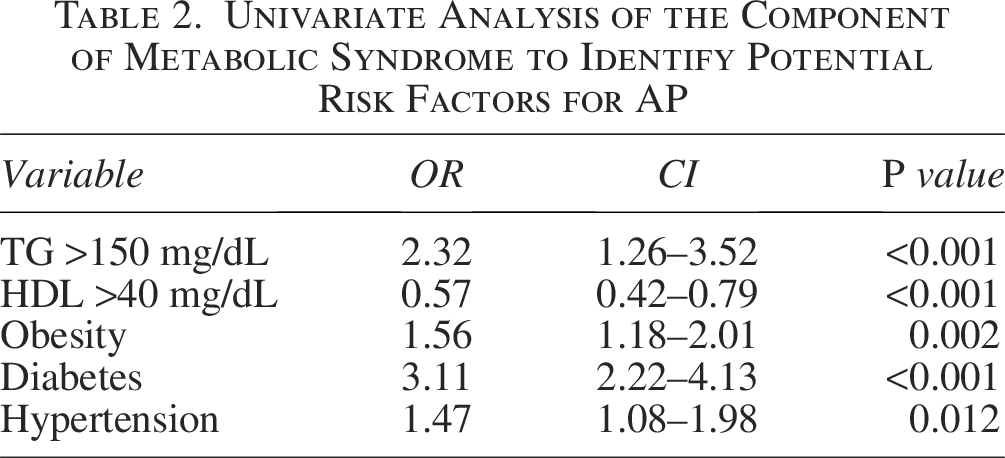
Univariate analysis indicated that increased CAC, elevated TG levels, and decreased HDL levels were significantly associated with AP occurrence (OR: 2.32; 95% CI: 1.26–3.52, P < 0.001; OR: 1.63; 95% CI: 1.18–2.16, P = 0.002; OR: 1.49; 95% CI: 1.09–1.97, P = 0.013). Additionally, obesity, diabetes, and hypertension were significant risk factors for AP (OR: 1.56; 95% CI: 1.18–2.01, P = 0.002; OR: 3.11; 95% CI: 2.22–4.13, P < 0.001; OR: 1.47; 95% CI: 1.08–1.98, P = 0.012). A detailed breakdown of univariate analyses for MetS components is provided in Table 2.
Univariate Analysis of the Component of Metabolic Syndrome to Identify Potential Risk Factors for AP
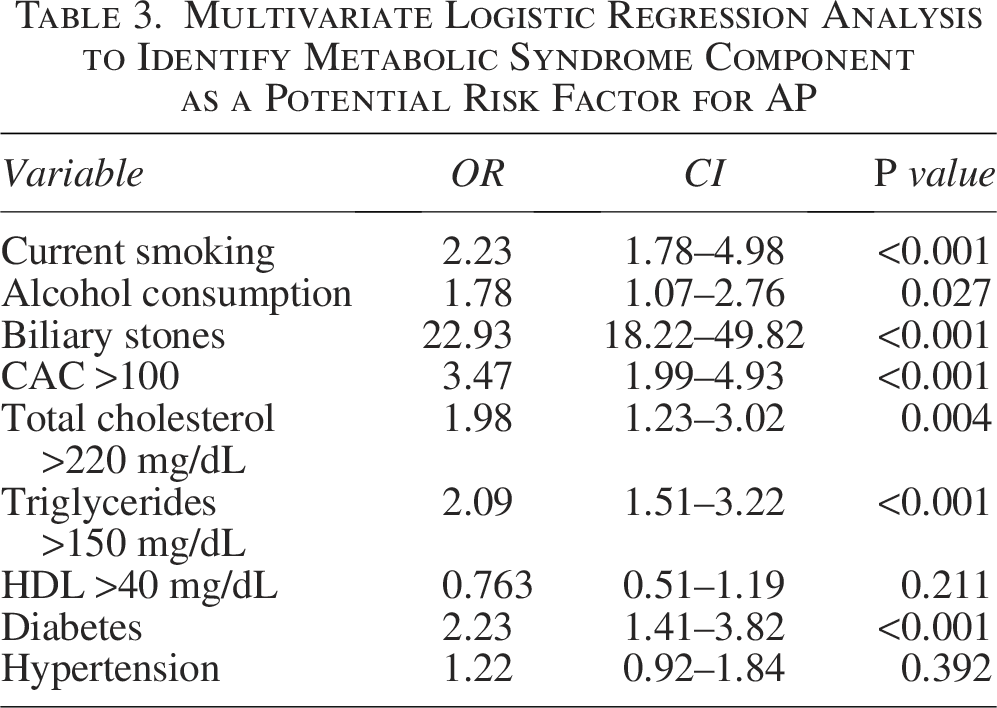
Multivariate logistic regression analysis, adjusted for smoking, alcohol consumption, gallstone history, CAC, and MetS components, showed that AP was significantly associated with smoking, alcohol consumption, gallstones, and CAC (OR: 2.23; 95% CI: 1.78–4.98, P < 0.001; OR: 1.78; 95% CI: 1.07–2.76, P = 0.027; OR: 22.93; 95% CI: 18.22–49.82, P < 0.001; OR: 3.47; 95% CI: 1.99–4.93, P < 0.001).
Regarding MetS components, AP was linked to elevated TG and TC levels, as well as hyperglycemia. The multivariate analysis results are summarized in Table 3.
Multivariate Logistic Regression Analysis to Identify Metabolic Syndrome Component as a Potential Risk Factor for AP
When assessing the relationship between AP and MetS (as defined by the ATP III criteria), MetS was identified in 57 (38.2%) individuals in the AP group compared to 27 (13.3%) in the control group (OR: 2.66; 95% CI: 1.72–4.32, P < 0.001).
Among AP patients, increased TG levels, MetS, and CAC were significant predictors of AP (P < 0.001, P < 0.001, and P < 0.001, respectively), with corresponding AUC values of 0.760, 0.692, and 0.621.
Discussion
To our knowledge, this is the first case–control study to examine the association between CAC and both the occurrence and severity of AP. Our findings indicate that an elevated CAC score is independently associated with an increased likelihood of developing AP, regardless of the presence of MetS.
MetS and its components have long been linked to AP, as demonstrated in previous research.17–19 Similarly, our data confirm a significant association between MetS and AP. However, no prior studies have reported a higher incidence of AP among individuals with increased CAC scores. Our analysis revealed a strong positive correlation between CAC and AP (OR: 3.47; 95% CI: 1.99–4.93, P < 0.001).
The exact biological mechanisms underlying the relationship between MetS, its components (such as hyperglycemia), and AP remain unclear. However, several hypotheses have been proposed. Elevated blood glucose levels contribute to mitochondrial oxidative stress by promoting reactive oxygen species production and lipid oxidation, mediated by cytosolic Ca2+ accumulation.20–22 Additionally, beta-cell dysfunction and hyperinsulinemia may reduce sensitivity to somatostatin, a hormone that plays a regulatory role in pancreatic function, potentially contributing to AP. 22 Moreover, insulin resistance, a central contributor to hyperglycemia, triggers inflammatory responses in the body via pathways involving nuclear factor-kappaB, tumor necrosis factor-alpha, amylin, and interleukin-6, all of which have been associated with the pathogenesis of AP.23–25
Hypertriglyceridemia and obesity, both key components of MetS, are well recognized as contributing to increased morbidity and mortality associated with AP.26–29 Our study found a significantly higher prevalence of CAC among the AP group (35.5%) compared to the control group (10.3%). Multivariate logistic regression analysis, adjusted for smoking, alcohol consumption, gallstone history, CAC, and MetS components, demonstrated that AP was strongly linked to smoking, alcohol use, gallstones, and CAC (OR: 2.23; 95% CI: 1.78–4.98, P < 0.001; OR: 1.78; 95% CI: 1.07–2.76, P = 0.027; OR: 22.93; 95% CI: 18.22–49.82, P < 0.001; OR: 3.47; 95% CI: 1.99–4.93, P < 0.001). These findings suggest that CAC is associated with AP independently of MetS. Previous studies have reported a high prevalence of AP in individuals with MetS, which is known to increase the risk of coronary artery disease, as reflected by CAC scores.18–20 Additionally, our study highlights an independent association between fatty liver and CAC, irrespective of MetS status.
Limitations
Several limitations should be acknowledged. First, this was a retrospective, single-center, hospital-based case–control study, which limits the ability to establish causation. Prospective studies are needed to determine whether CAC plays a direct causal role in AP. Second, while we found a strong association between CAC and AP, our study did not assess the impact of treatments for coronary artery disease or MetS components on AP risk, which may influence the results.
Strengths
Despite these limitations, our study has several strengths. Notably, this is the first investigation to establish a relationship between CAC and the development of AP, contributing novel insights into potential risk factors for the disease.
Conclusion
Our findings demonstrate that MetS, its components, and CAC scores are significantly associated with AP. Further research is necessary to explore the underlying mechanisms and potential clinical implications of these associations.
Authors’ Contributions
All authors made substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; and drafted the work/reviewed it critically for important intellectual content; and provided final approval of the version to be published.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.