
Abstract
Background:
Lymphedema is a potential chronic degenerative secondary condition of oncologic treatments. Complex decongestive therapy (CDT) is the only treatment. Quantitative dimensional characterization of lymphedema is a topic of great clinical interest that has not been sufficiently analyzed yet. We aimed to develop statistical models that evaluate lymphedema’s local spatial distribution and the effectiveness of CDT.
Methods and Results:
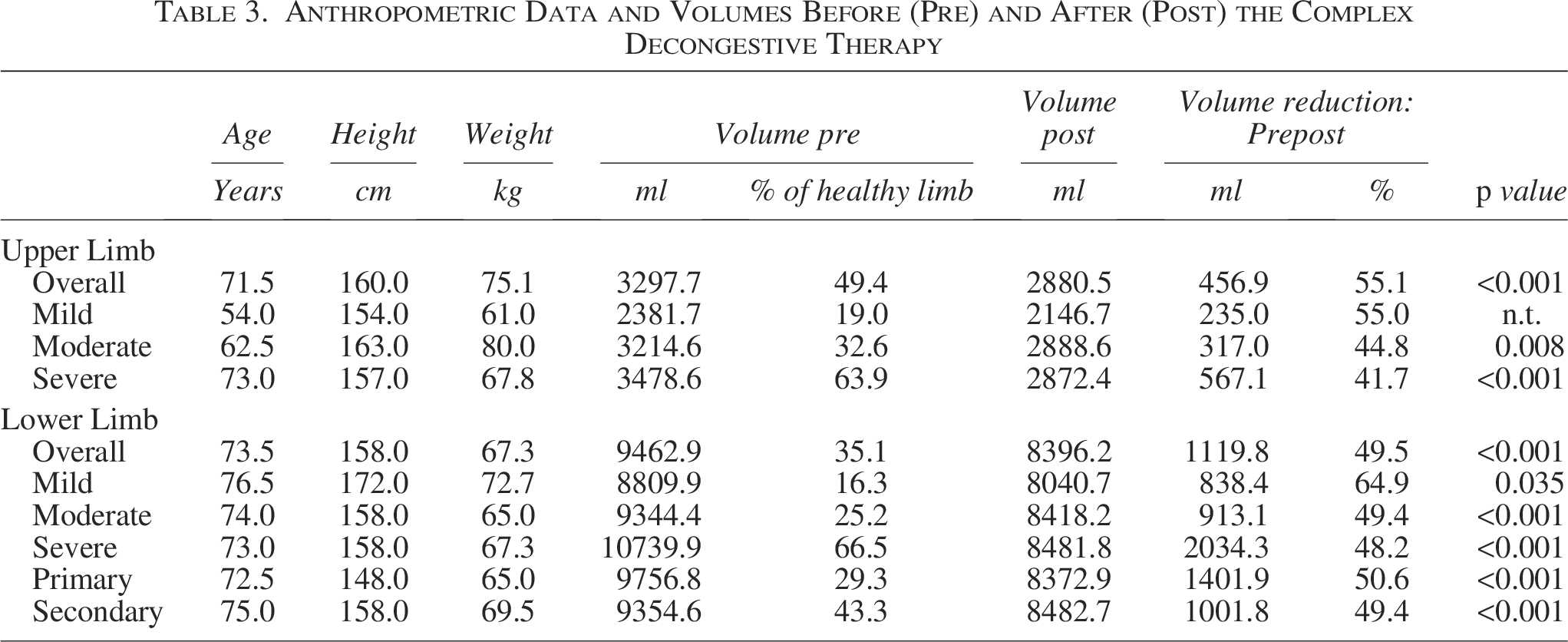
Retrospective observational analysis of 74 individuals (220 medical records) with unilateral upper or lower limb lymphedema who completed at least one cycle of the first phase of CDT. Statistical mixed-effects models were used to quantify the local distribution of lymphedema through the circumference of eight detection points and the efficacy of CDT according to the entity and the etiology of lymphedema. The coefficients of the models considered both fixed (i.e., the effect at the population level) and random (i.e., subject) effects. All points significantly reduced between pre- and posttreatment. Lymph stagnation occurred in the forearm and below the knee. The dimensions and effective treatment were similar between primary and secondary lymphedema and between mild and moderate lymphedema. The median global volume reduction of the upper limb was 55.1%, while it was 55%, 44.8%, and 41.7% in mild, moderate, and severe lymphedema; 50.6% and 49.4% in primary and secondary lymphedema. The median global volume reduction of the lower limb was 49.5%, while it was 64%, 49.4%, and 48.2% in mild, moderate, and severe lymphedema.
Conclusion:
A modeling of lymphedema distribution was provided, finding a dysmorphic pattern driven by the gravitation effect, with lymphedema accumulating on the lower part of the limbs, which is also the part that mostly responded to CDT. The response to CDT was assessed locally and not in terms of global volume change. A new segmental proportional technique was proposed that allows making comparisons between and within subjects.
Keywords
Introduction
Lymphedema is a chronic and degenerative condition caused by a low-output failure of the lymphovascular system to transport lymph. It differentiates into primary (due to congenital lymphatic dysplasia) and secondary (acquired after node sampling, radical operative dissection like extensive axillary, retroperitoneal node removal, irradiation or trauma). The final pathway is the manifestation of tissue edema whenever lymph formation exceeds lymph absorption, provoking an increase in the volume of the affected limb.1–5
Swelling quantification (volumetric limb measure and/or measurements of the circumference of the limb) can be used for staging and testing the treatment of lymphedema. Functional severity assessment has utilized excess percentage volume differences between the affected and unaffected limbs. According to the International Society of Lymphology (ISL), 1 lymphedema is classified as mild (5%–20% increase in limb volume), moderate (20%–40%), or severe (>40%). These volume differentials are most commonly determined using circumferential measurement due to wide availability and low cost, and the truncated cone formula is utilized for calculating volume. 1
Besides tissue swelling, lymphedema is also associated with adipose tissue remodeling and collagen deposition in the superficial skin lymphatics, causing skin layers to change its structural composition and mechanical properties, leading to skin stiffness.4,6
According to the guidelines, the main treatment of lymphedema is the complex decongestive therapy (CDT).1,7–9 CDT involves a two-stage treatment program: the first “intensive” phase consists of skincare, a specific light manual lymphatic drainage, compression typically applied with multi-layered bandage wrapping, and muscle pumping exercises. The second “maintenance” phase consists of daily compression by a low-stretch elastic stocking or sleeve to be initiated promptly after the intensive phase to conserve and optimize the results. The assessment of limb volumes should be made before, during, and after CDT treatment to quantify the efficacy of the therapy. There is no doubt that CDT effectively reduces the volume of affected limbs, but results are traditionally reported as global limb volume/circumference.10–14,15 To date, a general quantitative description of the distribution of lymphedema within the limb at a local level is unavailable due to practical measurement issues: (1) limb plethysmographic measurements or 3D body scanners are not commonly used in clinical practice, and (2) circumferential measurements are traditionally made at specified segment lengths and not at proportional standardized distances. The consequence is the impossibility to make comparisons among different subjects because of the different absolute anatomical lengths. The local analysis of volume would improve the knowledge of the anatomical distribution of lymphedema. This would better quantify and optimize the effect of CDT by localizing the points that would need more drainage and/or compressive bandaging.
The aims of this study were: (1) to shift the attention from global to local evaluation of lymphedema by developing a statistical model of the lymphedema distribution and the CDT effectiveness; (2) to consider two clinical classifications in the analysis, namely the entity of lymphedema (mild, moderate, and severe) and the etiology (primary vs. secondary); and (3) to propose a segmental circumferential measurement based on proportional standardized distances that allows comparison among subjects.
Materials and Methods
This was a single-center retrospective observational study using patients’ medical records between January 2010 and December 2022. Inclusion criteria: individuals with unilateral upper or lower limb lymphedema who completed at least one cycle of the first phase of CDT and were over 18 years of age. Exclusion criteria: missing values in the medical records included in the analysis.
The use and analysis of the database were approved by the Clinical Research Ethics Committee of Politecnico di Milano (Decision number: 07/2023).
Complex decongestive therapy
All patients underwent two and a half hours of the first phase of CDT, consisting of skin care, specific manual lymphatic drainage (1-hour duration), multi-layered bandage wrapping, and muscle pumping exercises. The treatment was administered daily, 5 days a week for 2 weeks, with the multi-layered bandage wrapping maintained during the weekend to guarantee therapeutic continuity.
Measurement of the limb circumferences
Circumferential measurements were made at standardized distances by fractioning the limb’s length with a defined constant proportion. This segmental proportional technique identifies the points for circumferential measurements by dividing the limb lengths into proportional parts (Fig. 1). The limb circumferences were measured by the same operator (a physiotherapist expert in lymphedema treatment) using a double dynamometric tape measure (a dynamometer at each extreme (Italian patent number 1417397—European patent EP2.986.176 A1) so that measurements were made with uniform tension.
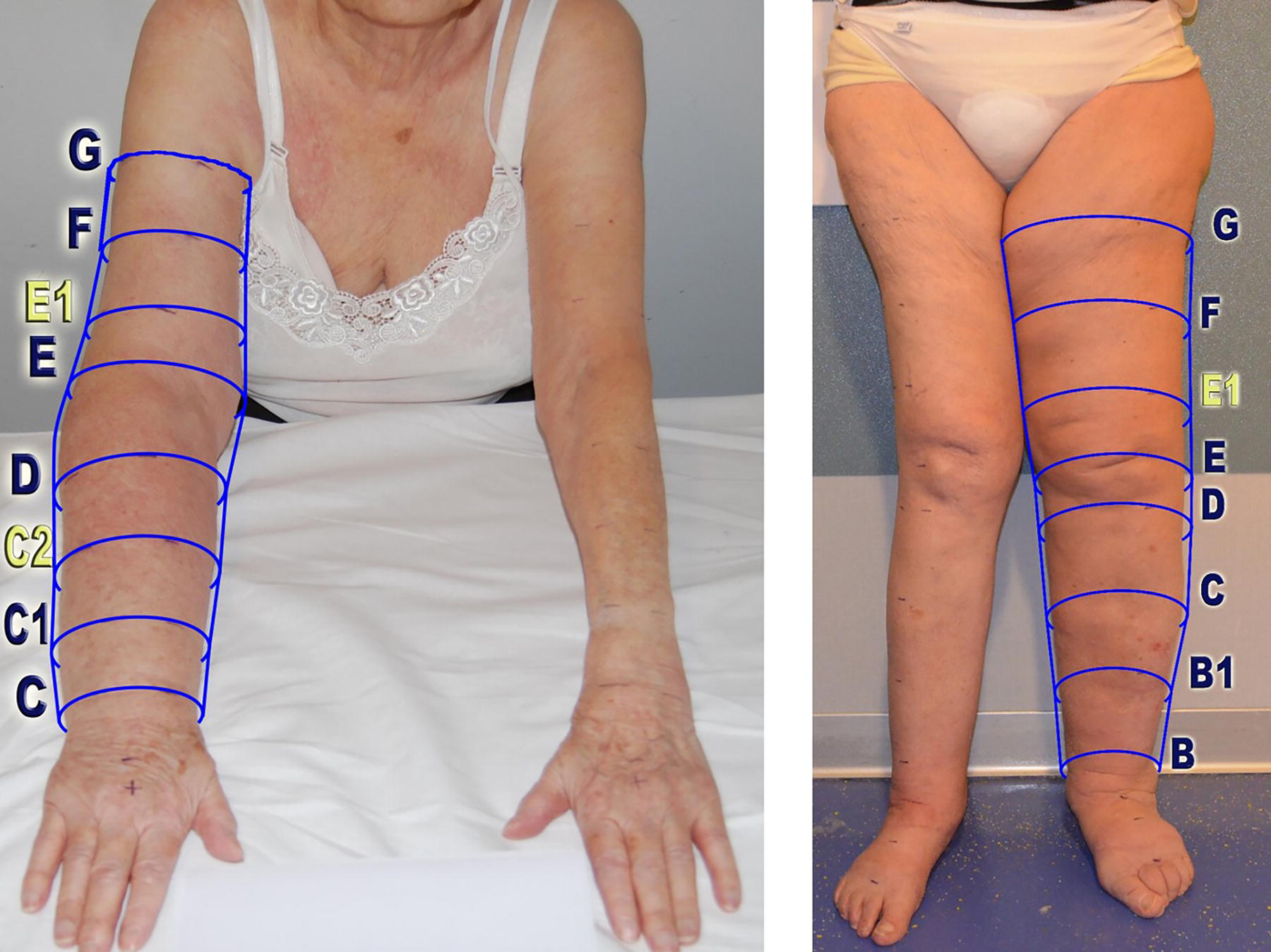
Upper (left panel) and lower (right panel) limb detection points identified using the segmental proportional technique. More in detail, the forearm length was defined as the distance between the distal wrist crease (point C) and the main elbow flexion skin crease (point E). The forearm length was then divided into four equal parts, identifying points C1 (i.e., 25% of forearm length), C2 (i.e., 50% of forearm length), and D (i.e., 75% of forearm length). The arm length was defined as the distance between the main elbow flexion skin crease (point E) and the axilla skin crease (point G). The arm length was then divided into three equal parts, identifying points E1 (i.e., 33% of arm length) and F (i.e., 66% of arm length). The leg length was defined as the distance between the narrowest circumference over the malleolus (point B) and the main popliteus flexion skin crease (point E). Point C was identified as the largest calf circumference. B1 was defined as the 50% distance between points B and C. Point D is defined as the medial popliteus skin crease. Finally, the thigh length was defined as the distance between the main popliteus flexion skin crease (point E) and the gluteal sulcus (point G). The thigh length was then divided into three equal parts, identifying points E1 (i.e., 33% of forearm length) and F (i.e., 66% of forearm length). In this way, the points were identified according to anatomical points and in proportion to the length so that different individuals could be compared. The patients signed written informed consent for the publication of their photos.
When the distribution of lymphedema was considered, the outcome measurement was the difference between the affected and unaffected limbs divided by the latter to normalize the circumference variations (expressed as percentage differences relative to the unaffected limb). Measurements were collected for each of the eight detection points on the first day (i.e., pretreatment (ΔPRE) and the tenth day (i.e., posttreatment [ΔPOST]).
When the CDT effectiveness was considered, the outcome measurement was the (ΔPRE-ΔPOST/ΔPRE) to normalize the circumference variations (expressed as percentage changes from the pretreatment).
Global limb volume was calculated using the truncated cone formula.
Statistical analysis: Mixed effects models
Considering the structure of the data, we developed mixed-effects models that allowed analyzing of longitudinal data in which the observations were not independent of each other. These were statistical models in which the coefficients were expressed as the sum of both fixed effects and random effects. The latter collects the characteristics of each cluster (e.g., subject) for which several observations were measured. The former describes the effect at the population level, i.e., the part common to all clusters. Estimations were made using the restricted maximum likelihood approach, while the goodness-of-fit of the model was analyzed using as R-squared Marginal and Conditional. The model returned Fixed Effect Omnibus Tests that assessed the statistical significance of the fixed effect at the global level using Student’s t-tests and the Fixed Effects Parameter Estimates. For random effects, their variance was returned, which captured the variation between/among clusters. Post hoc tests between fixed effects were performed, for which marginal means were estimated and represented graphically. The normal distribution of the residuals and their heteroskedasticity were observed to assess how close they were to the model’s optimal assumptions (The Jamovi® project, version 2.3, Computer Software, 2022).
The analysis was conducted for the overall population and according to lymphedema etiology and to severity (as indicated by ISL). 1
Results
Seventy-nine patients were included in the study for a total of 220 records analyzed (the same patients underwent treatment several times).
Overall patients
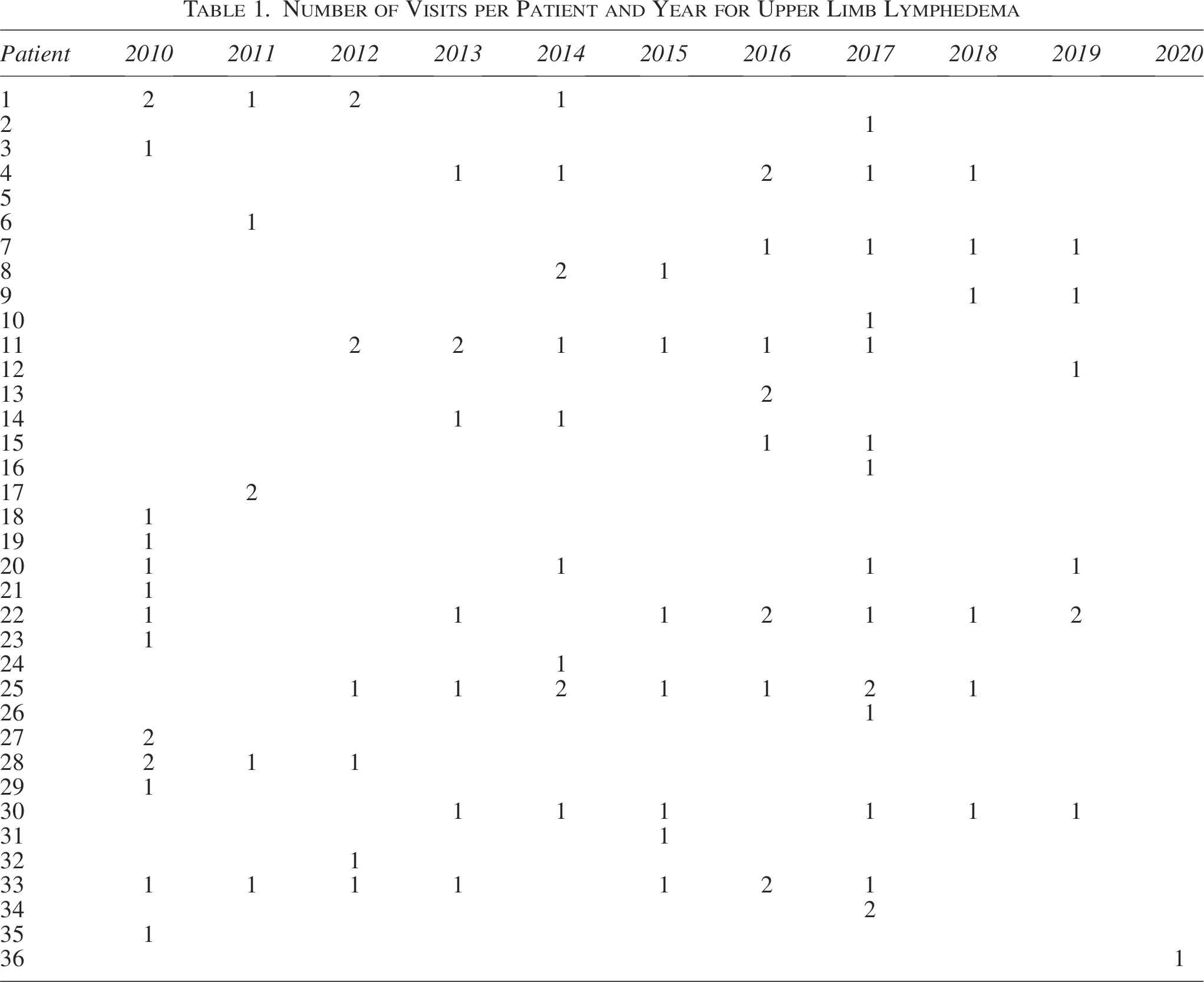
Thirty-six patients were affected by upper extremity lymphedema (98 visits, Table 1). Lymphedema was mainly located in the forearm, with the most severely affected points being C1, C2, and D (Fig. 2). The treatment was effective in all points, with an average circumference reduction of around 8%. The most reduced points were C1 (12.1%), C2 (10.7%), and D (9.9%).
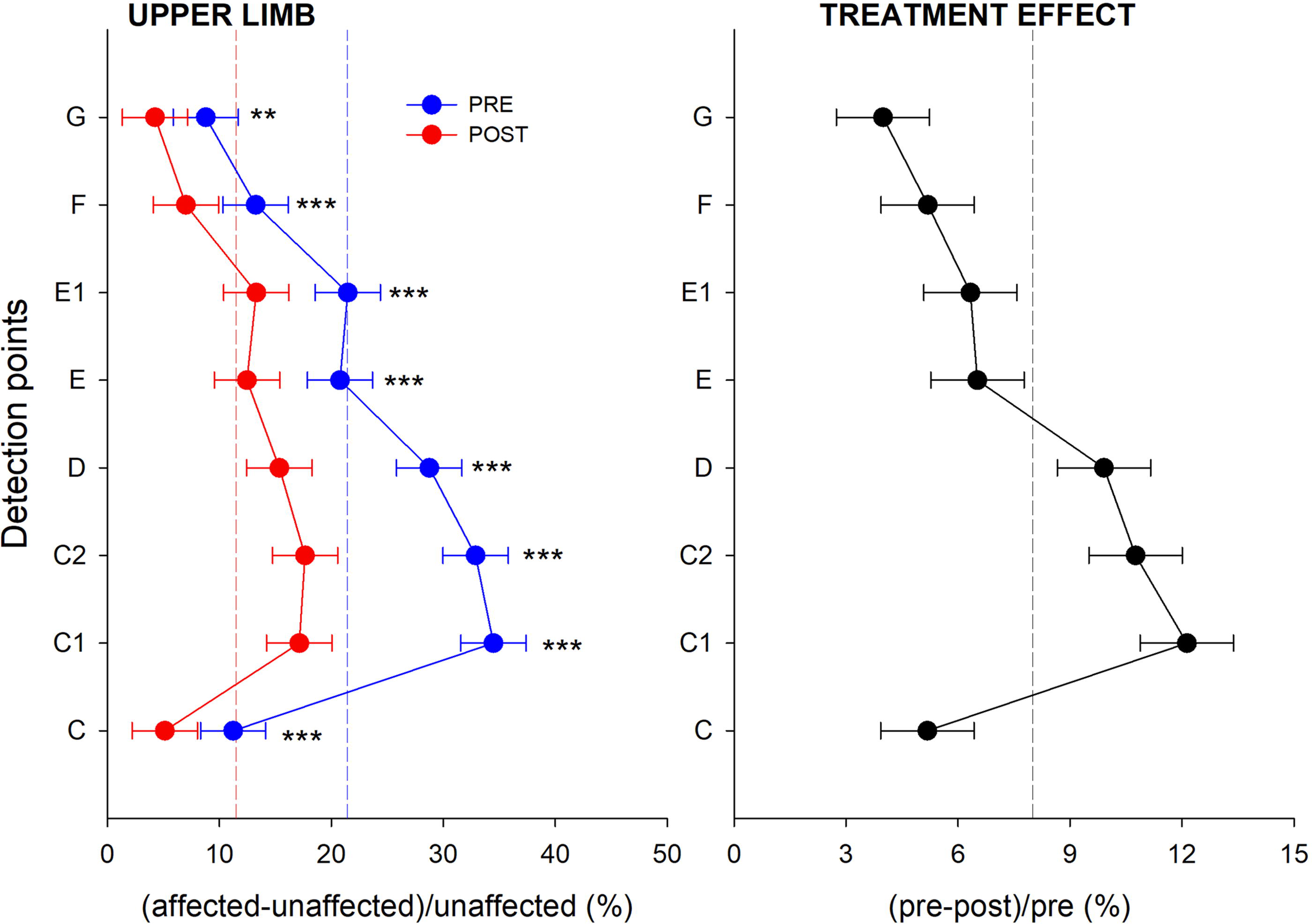
Estimated marginal means (symbols) and 95% confidence interval (whiskers) of the percentage circumference difference (x-axis) between the edematous upper limb and the healthy contralateral limb measured pretreatment (left panel, blue symbols) and posttreatment (left panel, red symbols) and of the percentage circumference difference (x-axis) of the edematous upper limb measured pre- and posttreatment (right panel) of all the detection points (y-axis). Vertical dotted lines indicate the average values. *, **, ***: p < 0.05, 0.01, 0.001 pre versus post.
Number of Visits per Patient and Year for Upper Limb Lymphedema
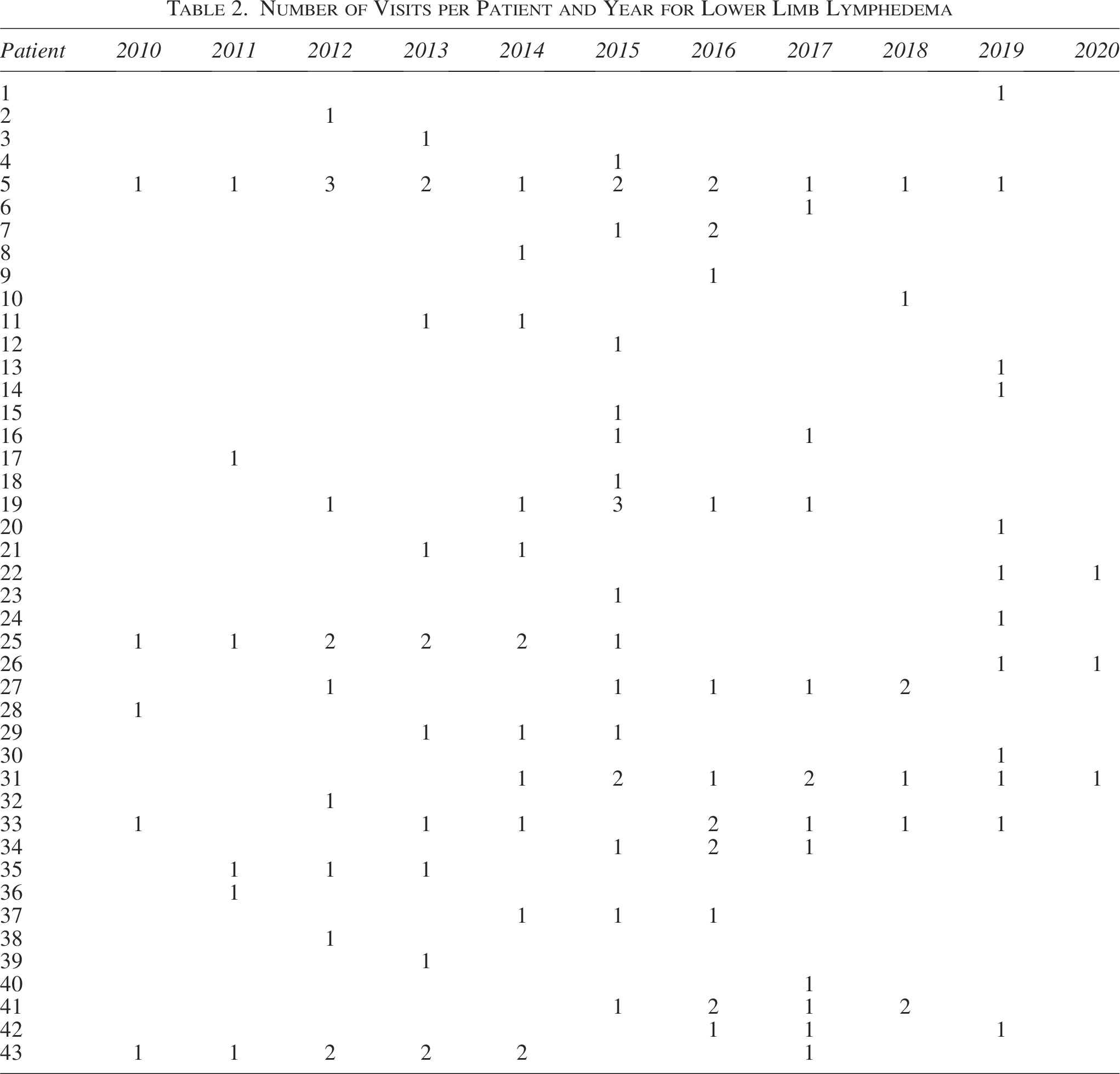
Forty-three patients were affected by lower extremity lymphedema (122 visits, Table 2). Before treatment, the lymphedema was mainly located below the knee (points B, B1, C, and D), exceeding the dimension of the healthy lower limb by 30%. All points benefited from treatment, with an average reduction in circumference of 7%. The most reduced points were B (10.7%), B1 (13.3%), and C (10.3%), as shown in Figure 3.
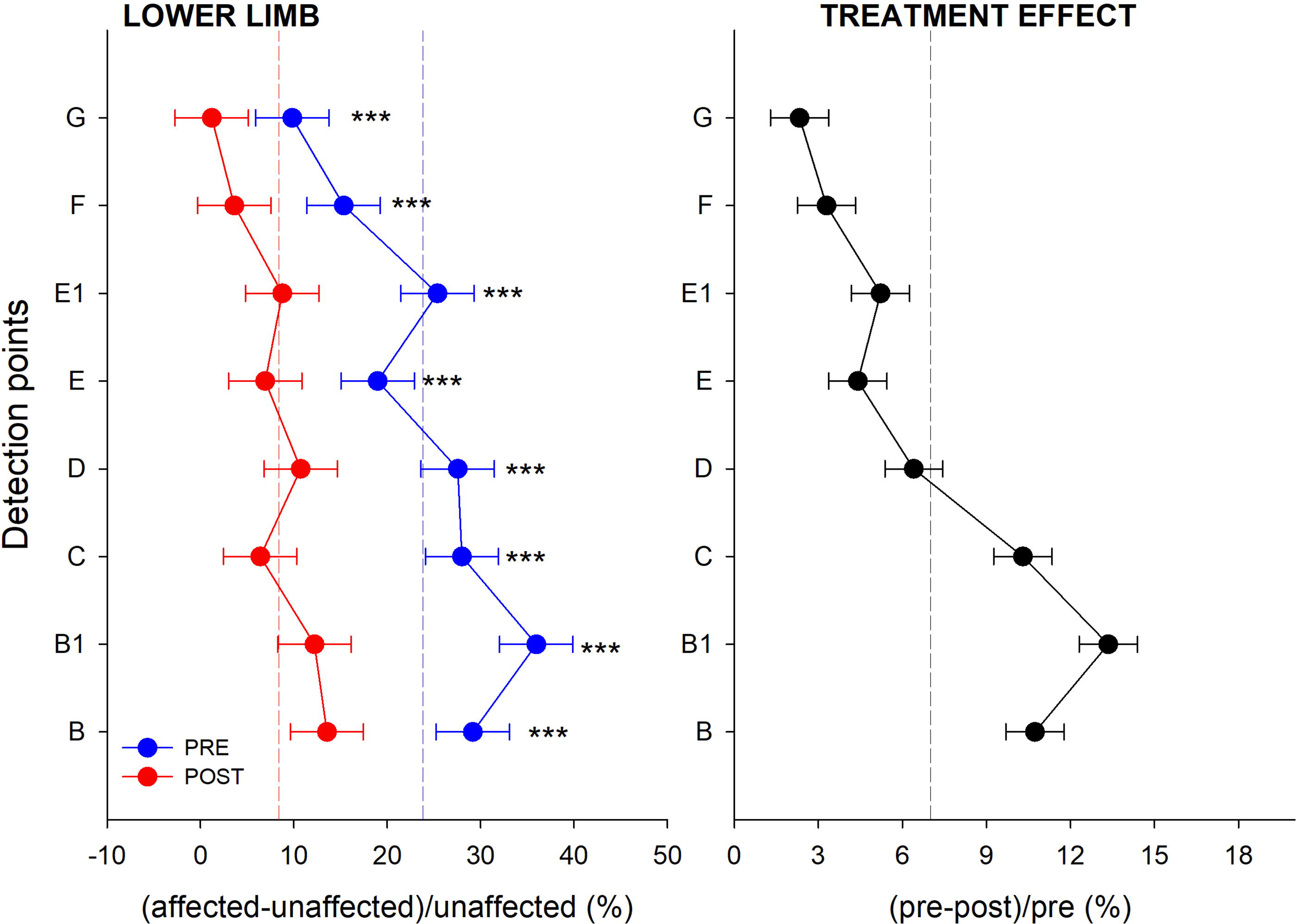
Estimated marginal means (symbols) and 95% confidence interval (whiskers) of the percentage circumference difference (x-axis) between the edematous lower limb and the healthy contralateral limb measured pretreatment (left panel, blue symbols) and posttreatment (left panel, red symbols) and of the percentage circumference difference (x-axis) of the edematous lower limb measured pre- and posttreatment (right panel) of all the detection points (y-axis). Vertical dotted lines indicate the average values. *, **, ***: p < 0.05, 0.01, 0.001, pre versus post.
Number of Visits per Patient and Year for Lower Limb Lymphedema
The entity of lymphedema: Mild, moderate, and severe
Twenty (57 visits) upper limb lymphedemas were classified as severe, 15 (38 visits) as moderate, and 3 (3 visits) as mild. Severe patients showed a marked significant difference between moderate and mild at points C1, C2, and D. CDT managed to reduce the dimension of the affected limb overall in points C1, C2, D, and E in the comparison between severe and moderate (Fig. 4).
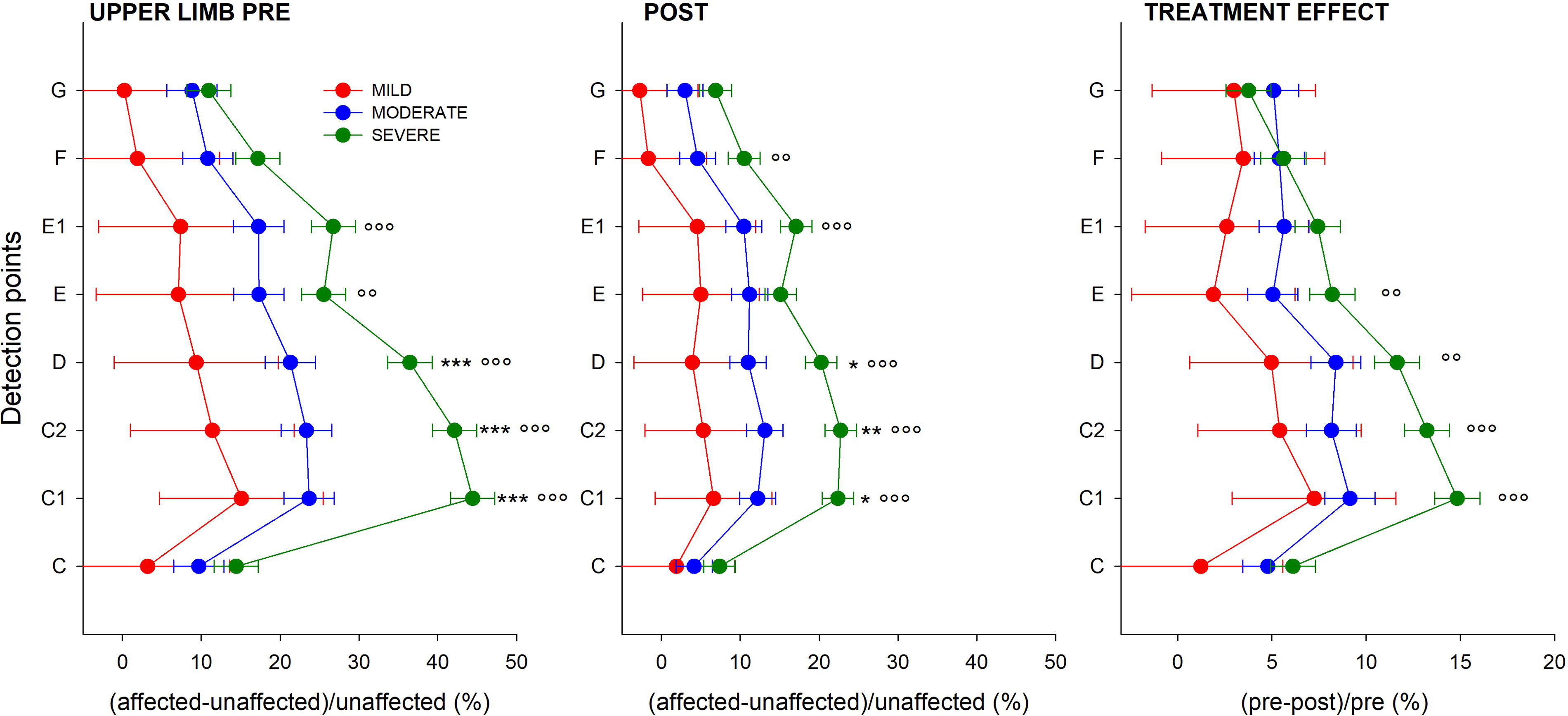
Estimated marginal means (symbols) and 95% confidence interval (whiskers) of the percentage circumference difference (x-axis) between the edematous upper limb and the healthy contralateral limb measured pretreatment (left panel), posttreatment (middle panel) and of the percentage circumference (x-axis) of the edematous lower limb measured pre- and posttreatment (right panel) of all the detection points (y-axis) according to lymphedema entity: severe (green), moderate (blue), and mild (red). *, **, ***: p < 0.05, 0.01, 0.001, Severe versus Mild; °, °°, °°°: p < 0.05, 0.01, 0.001 Severe versus Moderate.
Eight (39 visits) lower limb lymphedemas were classified as severe, 18 (70 visits) as moderate, and 12 (13 visits) as mild. Before and after the treatment, the dimensions of mild and moderate lymphedema were similar, while almost all points of severe lymphedema were higher than mild and moderate. In the posttreatment, there was an overall decrease in the estimated point means in the three groups compared to pretreatment. The best treatment benefit of the severe group compared to the mild and moderate (which are very similar) occurred at points C, D, and E (Fig. 5).
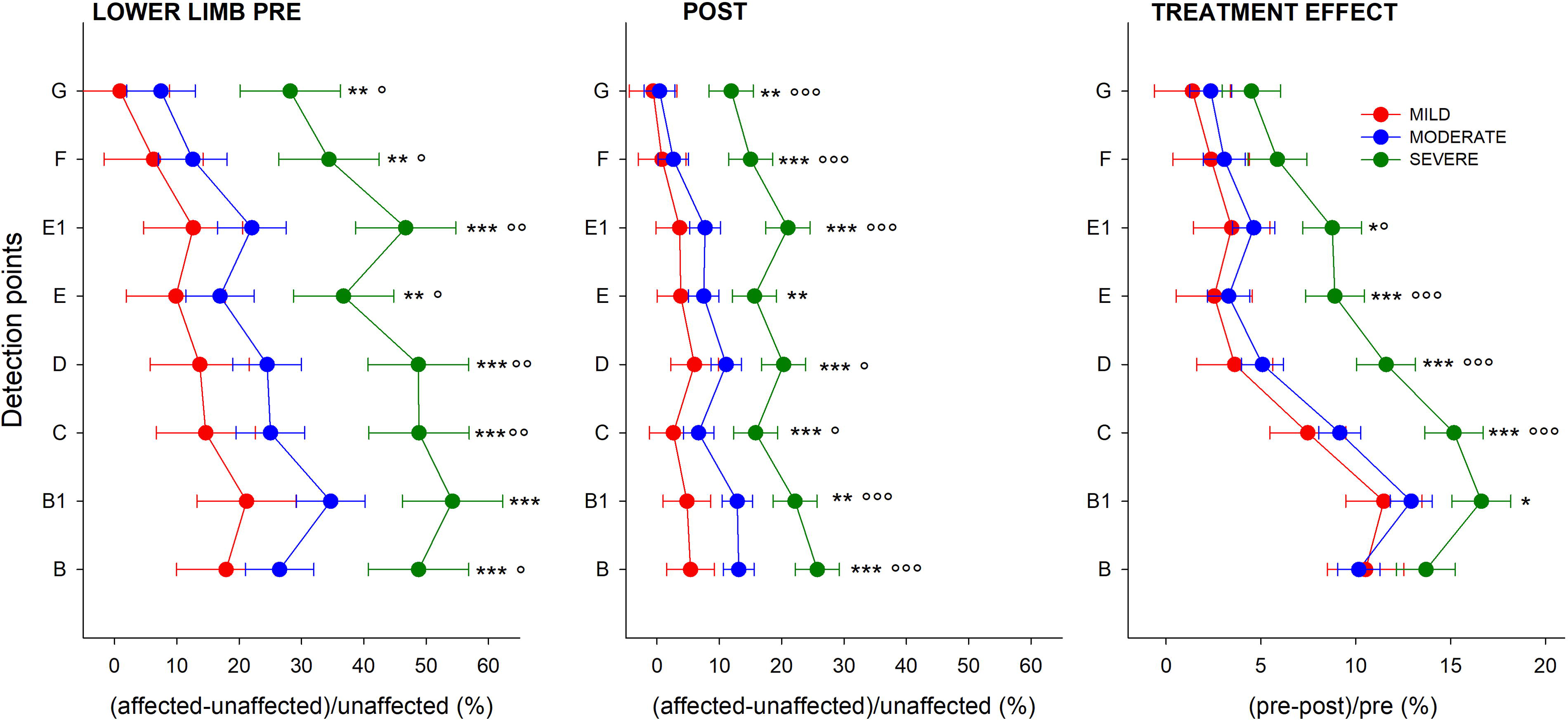
Estimated marginal means (symbols) and 95% confidence interval (whiskers) of the percentage circumference difference (x-axis) between the edematous lower limb and the healthy contralateral limb (divided by the latter) measured pretreatment (left panel), posttreatment (middle panel), and of the percentage circumference (x-axis) of the edematous lower limb measured pre- and posttreatment (right panel) of all the detection points (y-axis) according to lymphedema entity: severe (green), moderate (blue), and mild (red). *, **, ***: p < 0.05, 0.01, 0.001, severe versus mild; °, °°, °°°: p < 0.05, 0.01, 0.001, severe versus moderate.
Etiology: Primary vs. secondary
All the upper limb lymphedemas were secondary to breast cancer treatment. The etiology analysis was therefore performed only for the lower limb. Thirteen (49 visits) lower limb lymphedemas were primary, and 25 (73 visits) were secondary. No differences emerged between the two groups (Fig. 6).
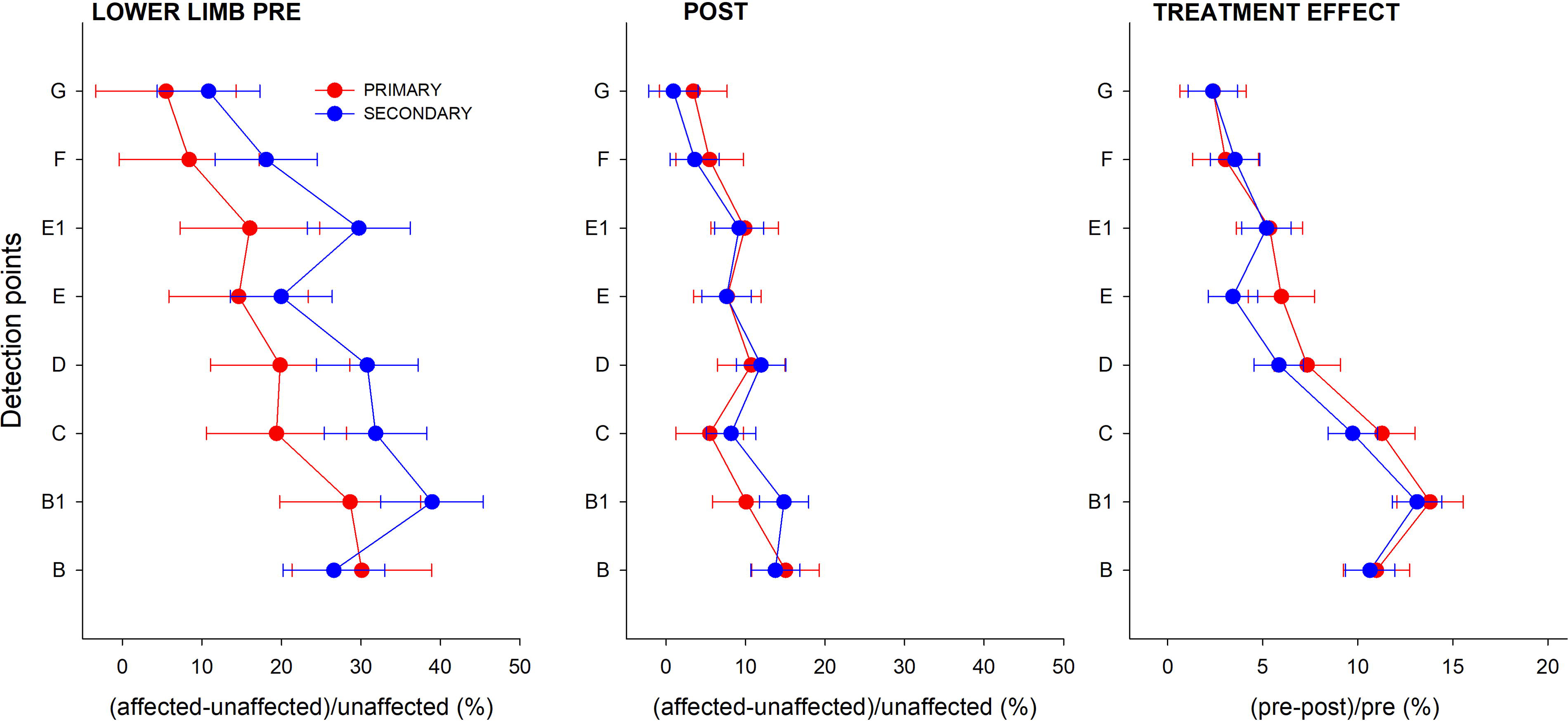
Estimated marginal means (symbols) and 95% confidence interval (whiskers) of the percentage circumference difference (x-axis) between the edematous lower limb and the healthy contralateral limb (divided by the latter) measured pretreatment (left panel), posttreatment (middle panel), and of the percentage circumference (x-axis) of the edematous lower limb measured pre- and posttreatment (right panel) of all the detection points (y-axis) according to lymphedema etiology: primary (red) and secondary (blue).
Overall anthropometric data and volumes before and after the CDT are reported in Table 3.
Anthropometric Data and Volumes Before (Pre) and After (Post) the Complex Decongestive Therapy
Discussion
This was the first attempt to model the lymphedema distribution in a representative population. We have shown that lymph accumulated following a gravitational gradient, with swelling primarily located in the forearm and below the knee. We have confirmed the effectiveness of the first phase of CDT by quantifying and localizing the distribution and the reduction of the circumferences. We have also shown that mild and moderate lymphedema seemed comparable in size and treatment effectiveness. We have confirmed that CDT’s dimensions and effect were similar between primary and secondary lymphedema. Finally, we have proposed a proportional segmental technique for circumferential measurements that made different individuals comparable.
The last decade has seen an explosive growth of insights into and approaches to the problem of lymphedema, probably due to increased cases of secondary lymphedema and the greater survival of oncological patients and a greater prevalence of the chronicity of lymphedema. Measuring lymphedema and its progression is still an important issue. Manual circumference and volume measurements are the most portable and readily accessible noninvasive methods to assess the extent of lymphedema by measuring the difference between the dysmorphic and the contralateral limb or between the baseline condition and the end of the treatment. However, these absolute differences are poorly informative if not related to the starting point. The same absolute reduction value might be a tremendous or a poor result, according to the reference.
Although the objective measure used to identify and quantify lymphedema is total limb volume change, it does not provide information on the distribution of lymphedema. A possible solution is to consider segmental volume changes, i.e., measuring limb volume at different segments of the limb. 16 Circumferences can be measured at constant or standardized distances. The fixed distance method is the most used in clinical practice. In 2006, Taylor and coauthors found greater accuracy of circumferential measurements based on anatomical landmarks than on fixed distances, as the measurements at relative lengths produce segments more similar to truncated cones. 17 Most importantly, such measurements can be used to compare patients with different limb lengths. It is therefore better to take circumferential measurements at standardized (and not fixed) distances. One strength of the present study was the use of a segmental proportional technique to take measurements at standardized distances and according to anatomical points. The measurement points paralleled those taken for the compression garment to provide consistency between CDT and the compression therapy. The proposed segmental measurement technique was validated against water displacement, the traditional gold standard, proving to be accurate in measuring limb volume with a mean error of 0.86%. 18
Thanks to the segmental proportional technique and to referring the circumferences to the healthy limb or baseline condition before CDT, it was possible to quantify the distribution of the lymph along the limb in a representative population (and not the single patient). This was the main strength of the study. A modeling of the spatial distribution of lymphedema along the affected limb was presented for the first time. Although every lymphedema is peculiar and unique, we found a representative dysmorphism (indicated by the relatively narrow confidence interval) that seemed driven by the gravitational effect. We have shown lymphedema accumulating on the lower part of the limbs (i.e., in the forearm for the upper limb and below the knee for the lower limb). These parts were also the most responsive to the CDT. Points C1, C2, and D for the upper limb and B, B1, and C for the lower limb deserved special attention, being the points where lymphedema was mainly localized and the CDT more effective. Knowing the points of most lymph accumulation and therapy response might help to optimize the CDT and to design compression garments.
Another important strength of the study was the development of statistical mixed-effects models that allow researchers to fully model all the sources of variability in the data, including repeated measures on the same subject and across time. They also provide interactions between fixed and random factors, allowing for exploring the difference between effects within and between groups. 19
Random factors made possible to consider that there was nonindependence in the data because some patients were visited repeatedly. They also have their flexibility in dealing with missing values and uneven spacing of repeated measurements (in our case, different number of visits and timing). Fixed factors are the levels of interest that allow for comparing pre- versus posttreatment and the different entity and etiology of lymphedema. For these reasons, we believe that the analysis with Linear Mixed-Effects Models is an important strength of our work, as it allows us to include the entire database.
We also confirmed CDT to reduce the affected limb significantly.8,10,12,13,20–31 While the effectiveness of CDT has always been reported in terms of global volume, we have quantitatively evaluated the reduction of lymphedema at the local level. We have also modeled lymphedema according to its entity. Interestingly, the three (mild, moderate, and severe) dysmorphic patterns were similar, but rescaled, to the global one. Limbs with severe lymphedema, which deviated more from the healthy limb, benefited more from treatment. Limb dimensions and treatment effectiveness were similar in patients with mild and moderate lymphedema, suggesting that these two entities might be unified. However, the numerosity of mild lymphedema was low, particularly for the upper limb (3 visits). Larger-scale studies should confirm whether mild and moderate lymphedema were comparable in size and treatment effectiveness.
Finally, we have also considered etiology as a fixed factor, but only for the lower extremity, finding no differences pre- and post-CDT and in the circumference reduction. This conclusion was in line with Abakay et al., who found no difference in the amount of lymphedema in both groups, reported as global volume changes. 10
Another strength of the study was presenting data on both limbs. Considering monolateral lymphedema was a limit because after cancer treatment both limbs may be affected. Another limitation was the relatively low sample size due to the single-center nature of the study. Extending our analysis to other databases would be important to verify if mild and moderate lymphedema could be grouped into a single entity. With a vast database, it could also be possible to investigate if different dysmorphic patterns can be identified to allow a more tailored treatment. In addition, it would be possible to compare the treatment strategies of different clinical centers to determine the best technique of CDT for the patients. Finally, measuring the circumferences at standardized heights would also permit extended local analysis of CDT response during the maintenance phase.
Since the incidence of the pathology is constantly increasing, the implementation of standard and effective protocols is necessary. Recent reviews have highlighted the lack of methodological rigor, standardized protocols, and controlled studies capable of comparing available treatments.13,16,32,33 The proposed segmental proportional technique seems to be appropriate to allow comparison between individuals with different characteristics. To provide a more comprehensive evaluation of lymphedema, external volume measurements should be combined with imaging (i.e., standard ultrasound or Magnetic Resonance Imaging (MRI)) to characterize the internal composition of the swelling in terms of fluid or fat. While standard ultrasound imaging may differentiate fat and fluid and only quantify the thickness of the dermal and subcutaneous layers; MRI can differentiate various tissue components and measure their volume. Using 3 MRI images to separate the tissue components of interest (muscle, fat, and fluid), Borri and coauthors showed that the volume of fat was predominant in most of the 13 women analyzed with unliteral breast cancer-related lymphedema. 34 They did not observe muscle hypertrophy due to advanced lymphedema. In line with our modeling, they found predominant involvement of the distal portions of the upper arm, further away from the original axillary damage. In addition to our results, they showed that fluid seems to collect mainly around the forearm and elbow region, whereas fat mainly contributes to upper arm swelling. 34 Combining our external segmental measurements information with the spatial distribution of the composition of the different tissues deriving from the image could better tailor guide the therapeutic approaches in terms of: (1) identifying the optimal site for drainage massage; (2) optimizing the design of compression garments, and (3) better evaluating the response to CDT.
To conclude, a modeling of lymphedema distribution in a sample population was provided, finding a dysmorphic pattern driven by the gravitation effect. The response to CDT was assessed at the local level and not in terms of global volume. An accurate segmental proportional technique for circumferential limb measurements was proposed. From a therapeutic point of view, it seemed useless to distinguish patients according to the etiology while it should be verified if mild and moderate classification can be unified. Therapists should learn to deal with practical measurement issues (the points for the circumferential measurements, their longitudinal separation, the volume calculation, and the reproducibility of the reference marks). They should also be trained to report the results in percentages and not as absolute values.
Footnotes
Author Disclosure Statement
G.F. is the owner of the double dynamometric tape measure patent (Italian patent number 1417397-European patent EP2.986.176 A1). The other authors certify that there is no conflict of interest with any financial organization regarding the material discussed in the article.
Funding Information
No funding was received for this article.