
Abstract
Background:
Case management models (CMM) have proven effective in improving cancer patients’ transition from hospitals back into the community. However, whether a CMM has long-term effects in improving cancer patients’ health requires further investigation. Therefore, this study aimed to evaluate the short-term and long-term effects of a nurse-led CMM on upper limb function and the incidence of affected limb complications among postoperative breast cancer patients.
Methods and Results:
A non-concurrent, quasi-experimental design was used to compare upper limb function and the incidence of affected limb complications between two groups: a care as usual group (CAU; control group) and a CMM group (intervention group). This study was conducted in the largest department for breast cancer in south China, where women newly diagnosed with breast cancer (N = 157) were assigned to either the CMM group (n = 77, recruited from June to July 2017) or the CAU group (n = 80, recruited from June to July 2016). Data on limb function—including objective shoulder range of motion (ROM), muscle strength, and the subjective Functional Evaluation Scale of the Ipsilateral Shoulder and Arm Function (FESISA)—were collected at baseline (upon admission), and at 3, 6, and 12 months after surgery. Additionally, the incidence of limb pain, paresthesia, and lymphedema was measured at 3, 6, and 12 months postoperatively. The results showed that affected limb function decreased for more than one year, and the incidence of upper limb complications in both groups declined over time, except for lymphedema in the CAU group. Furthermore, patients in the CMM group demonstrated significantly better limb function and a lower incidence of limb complications compared to those in the CAU group.
Conclusion:
The nurse-led CMM is a feasible and effective approach to improve the short-term and long-term quality of care and patient outcomes among patients with breast cancer.
Introduction
Breast cancer is the most common malignant tumor in women and seriously threatens the health of women in China and around the world.1–3 Standard comprehensive treatment for patients with breast cancer includes surgery, chemotherapy, radiotherapy, endocrine, and/or target therapy. 4 However, surgery and radiotherapy can often cause neuromusculoskeletal tissue and lymphatic system damage in the affected side of the chest and axilla, which can lead to limb complications and dysfunction.5–7 Limb function refers to the ability of human limbs to perform daily activities such as combing one’s hair, putting on clothes, and lifting or carrying heavy objects. Limb dysfunction refers to reduced function of the upper limb during daily activities. Signs of decreased limb function are decreased range of motion (ROM) of the shoulder joint and or a reduction in muscle strength. Previous studies have shown that the prevalence of restricted ROM was between 12% and 24%,8–10 and a reduction in muscle strength was between 8.5% and 13%.8,11,12 Moreover, the postoperative ROM of the shoulder joint and a reduction in muscle strength decreased for more than 1 year.13–14 Limb complications can manifest as pain, paresthesia, and lymphedema. According to previous studies, the prevalence of upper limb complications varies considerably (6–70%) depending on the symptoms assessed, the evaluation period, and the measurement.13–20 Affected upper limb dysfunction and limb complications reduce survivors’ quality of life and can delay their return to work. 21 Thus, mitigating postoperative limb function impairment and limb complications is integral for breast cancer survivors’ rehabilitation.
Current guidelines and clinical practices state that systematic, individualized, multidisciplinary, coordinated, and continuous care of upper limb function should be provided to breast cancer survivors.22–23 Case management models (CMMs) are one way in which these areas have been brought together. A CMM is a case manager-led, multidisciplinary-supported care delivery models that provide patient-centered and continuous care to patients to ensure treatment integrity, a reduction in complications, and an improvement in quality of life,24–25 which have been effective in improving cancer patients’ transition from hospitals and back into the community.26–32 The case manager plays the role of a clinical practitioner, manager, educator, consultant, and coordinator in the CMM. 33 The model was developed in the 19th century and popularized in western countries as well as in Hong Kong and Taiwan26,32,34–37 and has been employed as an effective care delivery model for cancer patients in previous research,32,35,37–39 including breast cancer studies.34,40–42 Such studies suggested that the CMM could improve limb function in patients with breast cancer 2–6 months after surgery. A randomized clinical trial in the United States suggested that the CMM was more likely to help elderly female patients with breast cancer obtain normal or near to normal range of arm motion 2 months after surgery. 41 A study in China showed that the CMM can improve a patient’s postoperative subjective limb function score 6 months after surgery. 42 However, there is limited evidence concerning the long-term effects of CMMs on postoperative upper limb function.
In China, the majority of patients with breast cancer receive upper limb rehabilitation education during their inpatient period, while home-based care is entirely absent. As primary care is in its initial stage in China, hospitals have a responsibility to provide continuous care. The CMM is a relatively new concept in mainland China. Healthcare in China faces insufficient oncological resources, a large population of cancer patients, and an immature primary health system. Thus, we aimed to adapt a CMM for Chinese patients with breast cancer to investigate its effectiveness on postoperative upper limb function rehabilitation over a long period of evaluation.
Methods
Design
A quasi-experimental, nonrandomized, and nonconcurrent design was conducted. The control group received care as usual (CAU group) and was recruited from June to July 2016, and the intervention group received extra care using the adapted CMM (CMM group) and was recruited from June to July 2017. The two groups were compared with evaluate the effectiveness of each approach.
Sample and setting
The sample size of the CMM group and the CAU group was set as 1:1. Sample size was estimated based on the expected change in the Functional Evaluation Scale of the Ipsilateral Shoulder and Arm Function (FESISAF) scores. 42 At least 84 patients (42 in each group) were required to detect the between-group difference, with a power of 90% at the 5% level of statistical significance, plus a 50% loss rate.
Participants were recruited using convenience sampling at a breast cancer department at the largest cancer center in South China. The inclusion criteria were: (1) newly diagnosed with stage I to III breast cancer based on pathology or histology reports; (2) had been informed of their cancer diagnosis; (3) 18 years or older; (4) could complete the issued questionnaires independently; (5) could communicate in Mandarin or Cantonese; (6) agreed to telephone and or face-to-face interviews. The exclusion criteria were: (1) patients with a past or present history of mental illness; (2) other life-threatening diseases or serious systemic infections; (3) were participating in other clinical trials; (4) preoperative shoulder joint dysfunction, lymphedema, periarthritis of the shoulder and or any other disease or symptoms that may affect upper limb function; (5) had a peripherally inserted central catheter implanted in the upper limb; (6) diagnosis with bilateral breast cancer. The elimination criteria were: (1) cancer metastasis and recurrence during follow-up; (2) death from any cause; (3) voluntarily withdrew from the study.
The study protocol was approved by the ethics committee of our hospital. Written informed consent was obtained from all participants.
Intervention program
The CAU group
The patients in the CAU group received routine inpatient care. Nurses assessed patients, established nursing plans, and introduced the ward environments when patients were enrolled. In the perioperative period, nurses provided patients with information about their surgery and taught patients a range of upper limb rehabilitation exercises. A brochure was also provided to each patient to guide upper limb rehabilitation. The length of stay in the hospital lasted approximately 10 days. Patients were told about the time of return for outpatient review and the procedure of adjunctive treatment before discharge. Patients were responsible for their own follow-up visits and transitions between clinical departments.
The CMM group
The patients in the CMM group were provided with the nurse-led case-management approach in addition to the usual care. Care was provided to patients from diagnosis to 1 year after surgery. The case manager conducted regular visits at planned timepoints to provide patients with assessments, planning, counseling, health education, evaluations, coordinated resources from different specialties, and organized a multi-disciplinary team meeting. The case manager of this program was a full-time senior nurse with a master’s degree and over 5 years of oncology experience. Completion of a 3-month training course for the case managers was also a prerequisite. The case management services started at admission and ended 5 years after surgery (the details of the 1-year follow-up are discussed here only). The implementation of the CMM group is shown in Table 1. Meanwhile, the case manager gave her mobile phone number or social media contact to patients and their caregivers to ensure timely guidance as and when needed.
Nursing Care Provided by the Case Manager in the CMM Group
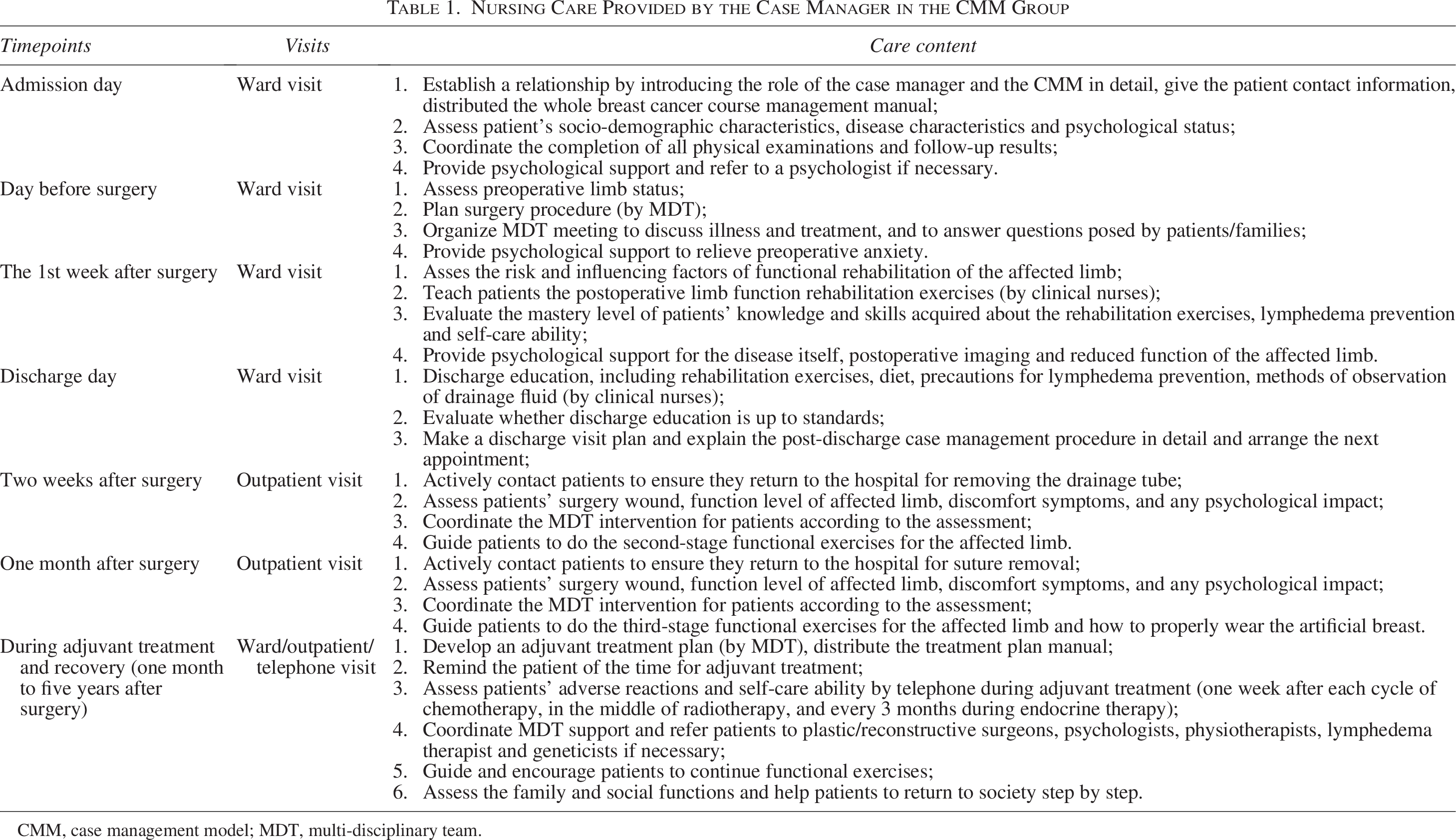
CMM, case management model; MDT, multi-disciplinary team.
Measurements
Sociodemographic and clinical characteristics
Sociodemographic characteristics included gender, age, education level, work status, marital status, economic status, and medical burden. Clinical characteristics included surgical method, clinical cancer stage, pathological subtypes, and medical regimen.
Affected upper limb function
Objective indicators: degree of shoulder ROM and muscle strength
The angles of the shoulder’s ROM in terms of forward flexion, backward extension, adduction and abduction were measured using a goniometer. Normal ROM were defined as follows: 43 forward flexion: 160°−180°; backward extension: 50°−60°; adduction: 60°−70°; and abduction: 170°−180°. Muscle strength was graded using Lovett’s manual muscle testing levels one to five. 44
Subjective indicators: Functional evaluation scale of the ipsilateral shoulder and arm function score
FESISAF is a self-reported questionnaire, which measures upper limb ability when performing common functional activities. FESISAF is a reliable and valid measure and is widely used in international studies.45–46
This scale was translated into Mandarin Chinese in 2007.
47
It is a 10-item, 5-point Likert scale scored from “0 = completely incapable” to “4 = completely capable.” The total score is the sum of all items’ scores, ranging from 0 to 40. Higher scores indicate better limb function. Cronbach’s
Affected upper limb complications
Affected upper limb complications were assessed by the incidence and the severity of limb pain, paresthesia, and lymphedema. Patients were asked to report whether they had limb pain and paresthesia. Diagnosis and clinical stage of lymphedema were classified in accordance with the International Society of Lymphology’s stage scale: 0, I, IIa, IIb, III. 48 The severity of their lymphedema was ranked as mild (Stage 0–I), moderate (Stage IIa), or severe (Stage IIb–III).
Data collection
Data collectors in this study were blind to the results. Sociodemographic and clinical characteristics were only collected during admission (baseline, T0) before the case manager had contact with the patients. Incidents of limb pain, paresthesia, and lymphedema were assessed at 3 months (T1), 6 months (T2), and 12 months (T3) after surgery, respectively. ROM, FESISA, and muscle strength scores were measured at four timepoints. Patients’ sociodemographic characteristics were collected during face-to-face interviews; clinical characteristics were collected from medical records; and the other data were obtained from the measurement methods. Patients were notified 1 week before their scheduled follow-ups. Patients who did not come back for the study’s follow-ups within 2 weeks were reminded twice by telephone.
Data analysis
Descriptive analysis was used to depict the patients’ demographic characteristics, clinical characteristics, ROM, muscle strength, FESISAF scores, and limb complications. The t-test, chi-square, and one-way analysis of variance (ANOVA) were used to compare the differences in demographic characteristics, clinical characteristics, ROM, FESISAF scores, muscle strength, and limb complications between the two groups, respectively. The repeated-measure ANOVA was used to analyze the changes in ROM and FESISAF scores. The separate effect analysis was used to further compare the difference of ROM and FESISAF scores between the two groups when time-intervention interaction existed. The general estimation equation was used to analyze the changes in muscle strength and limb complications. A p value of 0.05 (two-sided) was considered statistically significant. All statistical analyses were performed with Statistical Product and Service Solutions software version 20.0 (SPSS Inc., Chicago, IL, USA).
Results
Participant characteristics
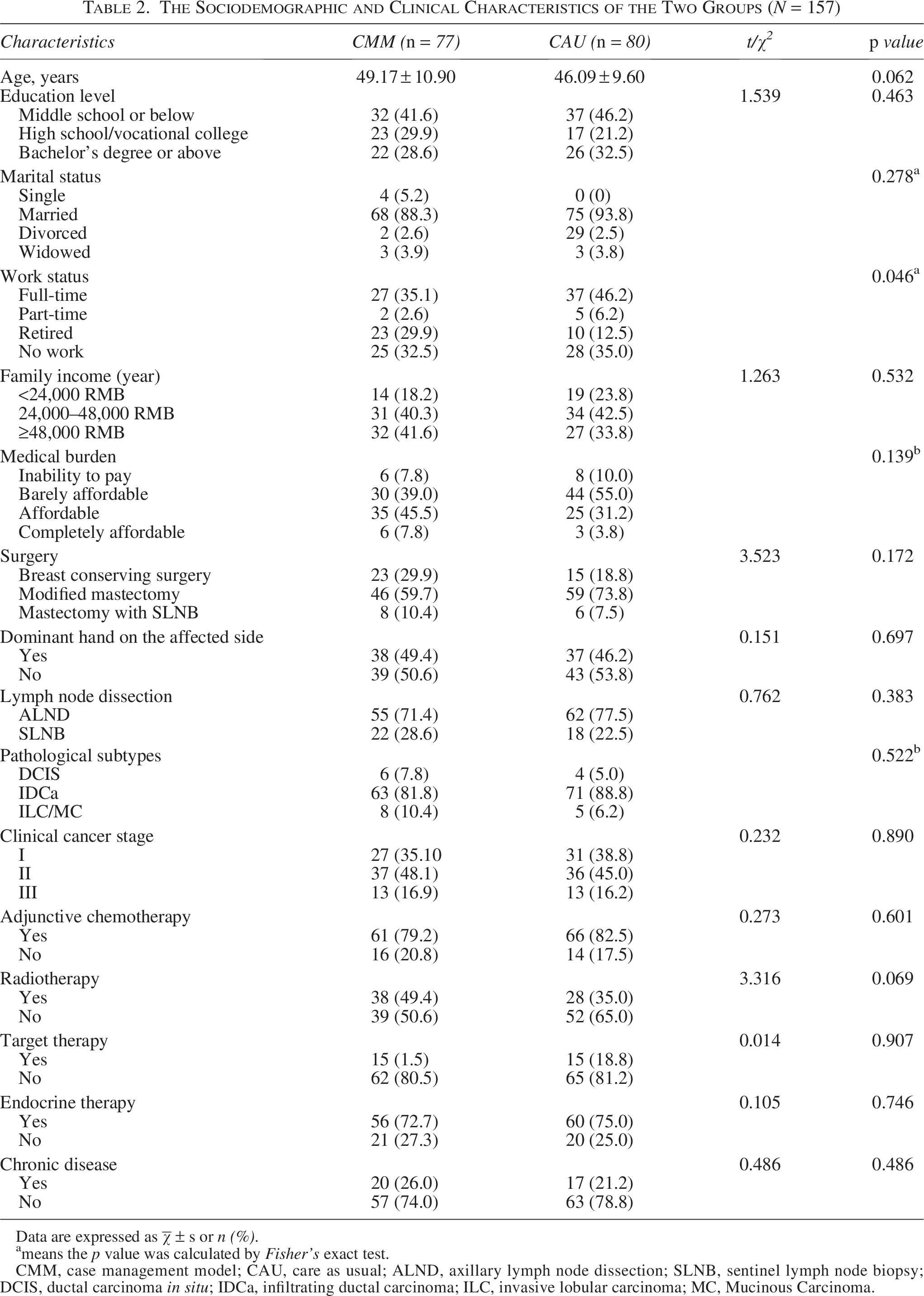
The total number of patients with breast cancer who provided written informed consent form at T0 was 166, with 83 in each group. In the CAU group, 80 patients completed all the assessments, with a loss rate of 3.61%. In the CMM group, 77 patients received interventions and completed all the assessments, with a loss rate of 7.23%. The flowchart for the study is shown in Figure 1. There were no significant differences in patients’ baseline sociodemographic and clinical characteristics between the two groups (p > 0.05), except for work status (p = 0.046) (Table 2). Therefore, work status at baseline was controlled for in the multivariate analyses.
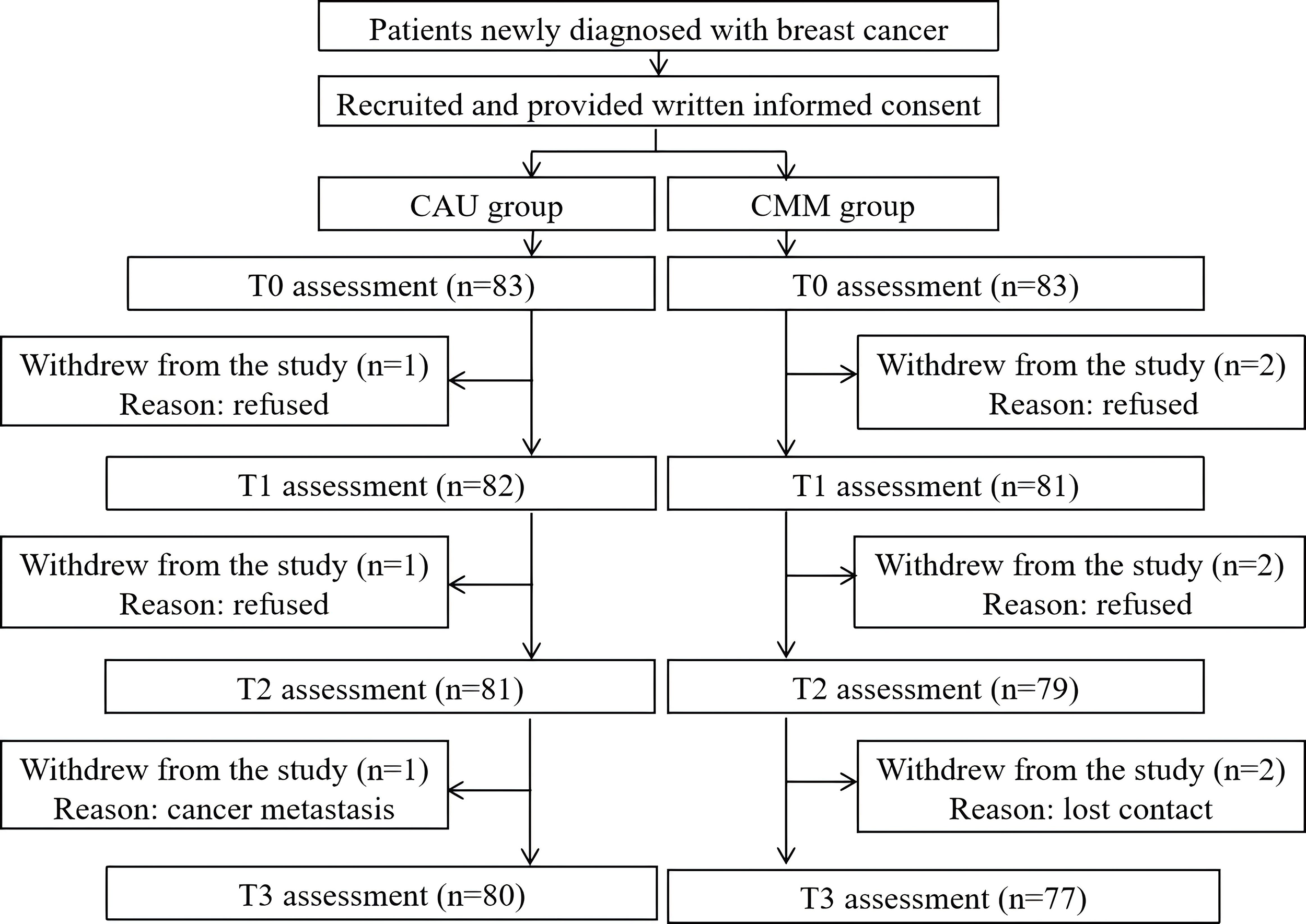
Study flowchart. CMM, case management model; CAU, care as usual; T0, baseline; T1, 3 months after surgery; T2, 6 months after surgery; T3, 12 months after surgery.
The Sociodemographic and Clinical Characteristics of the Two Groups (N = 157)
Data are expressed as
means the p value was calculated by Fisher’s exact test.
CMM, case management model; CAU, care as usual; ALND, axillary lymph node dissection; SLNB, sentinel lymph node biopsy; DCIS, ductal carcinoma in situ; IDCa, infiltrating ductal carcinoma; ILC, invasive lobular carcinoma; MC, Mucinous Carcinoma.
Effects of the intervention on shoulder ROM, muscle strength, and FESISAF scores between the CMM group and the CAU group
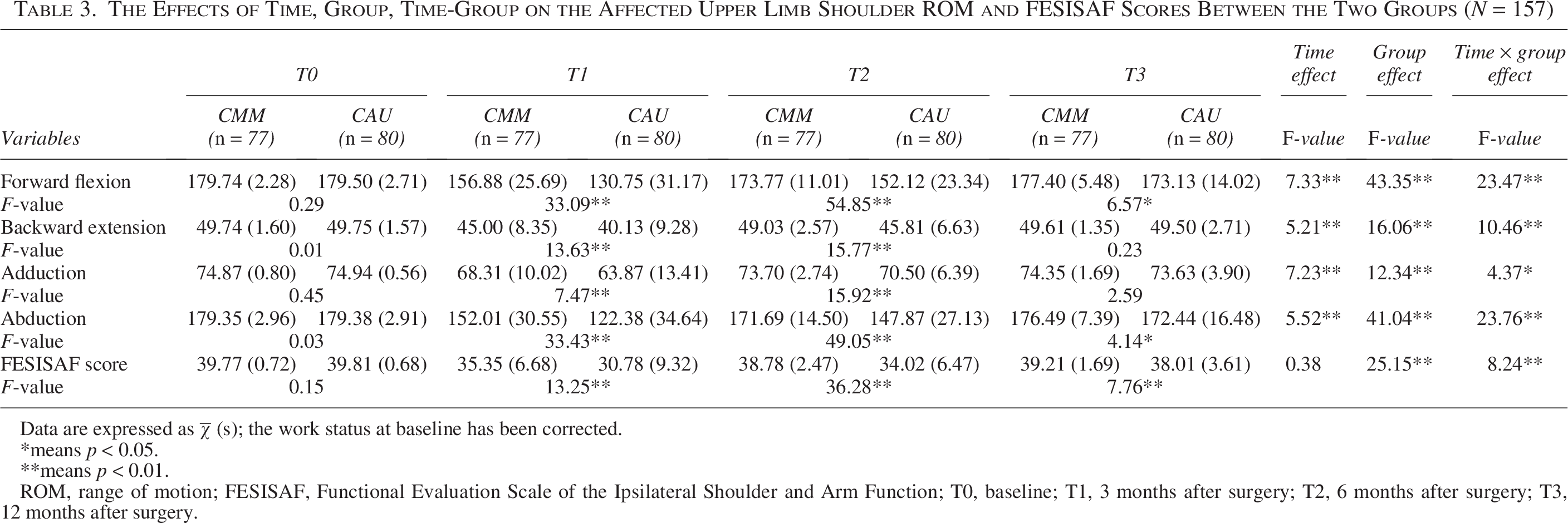
As shown in Table 3, baseline data showed no differences in affected upper limb function between the CMM group and the CAU group in regards to shoulder forward flexion (F = 0.29, p > 0.05), backward extension (F = 0.01, p > 0.05), shoulder adduction (F = 0.45, p > 0.05), shoulder abduction (F = 0.03, p > 0.05), and FESISAF scores (F = 0.15, p > 0.05). The affected shoulder ROM and FESISAF scores decreased from T0 to T1 in both groups. Then, shoulder ROM and FESISAF scores gradually increased from T1 to T3; however, the function at T3 was still worse than that at baseline. The patients in the CMM group showed significantly higher shoulder ROM and FESISAF scores than the CAU group after controlling for interactions of time and intervention (p < 0.05 or p < 0.01). Thus, we conducted separate effect analysis of the two groups at T1, T2, and T3, respectively. The results indicated that the CMM group had a significantly higher degree of shoulder forward flexion (F = 33.09, p < 0.01; F = 54.85, p < 0.01; F = 6.57, p < 0.05), as well as degree of shoulder abduction (F = 33.43, p < 0.01; F = 49.05, p < 0.01; F = 4.14, p < 0.05) and FESISAF scores (F = 13.25, p < 0.01; F = 36.28, p < 0.01; F = 7.76, p < 0.01) than the CAU group at T1, T2 and T3. In addition, backward shoulder extension (F = 13.63, p < 0.01 and F = 15.77, p < 0.01) and shoulder adduction (F = 7.47, p < 0.01 and F = 15.92, p < 0.01) in the CMM group were significantly higher than in the CAU group at T1 and T2. The change in muscle strength was the same as the ROM and FESISAF scores, and the muscle strength was better in the CMM group than in the CAU group (OR = 3.04, 95% CI: 1.43–6.46), which is shown in Table 4.
The Effects of Time, Group, Time-Group on the Affected Upper Limb Shoulder ROM and FESISAF Scores Between the Two Groups (N = 157)
Data are expressed as
means p < 0.05.
means p < 0.01.
ROM, range of motion; FESISAF, Functional Evaluation Scale of the Ipsilateral Shoulder and Arm Function; T0, baseline; T1, 3 months after surgery; T2, 6 months after surgery; T3, 12 months after surgery.
Muscle Strength and the Incidence of Affected Limb Complications over Time in the CMM and CAU Groups (N = 157)
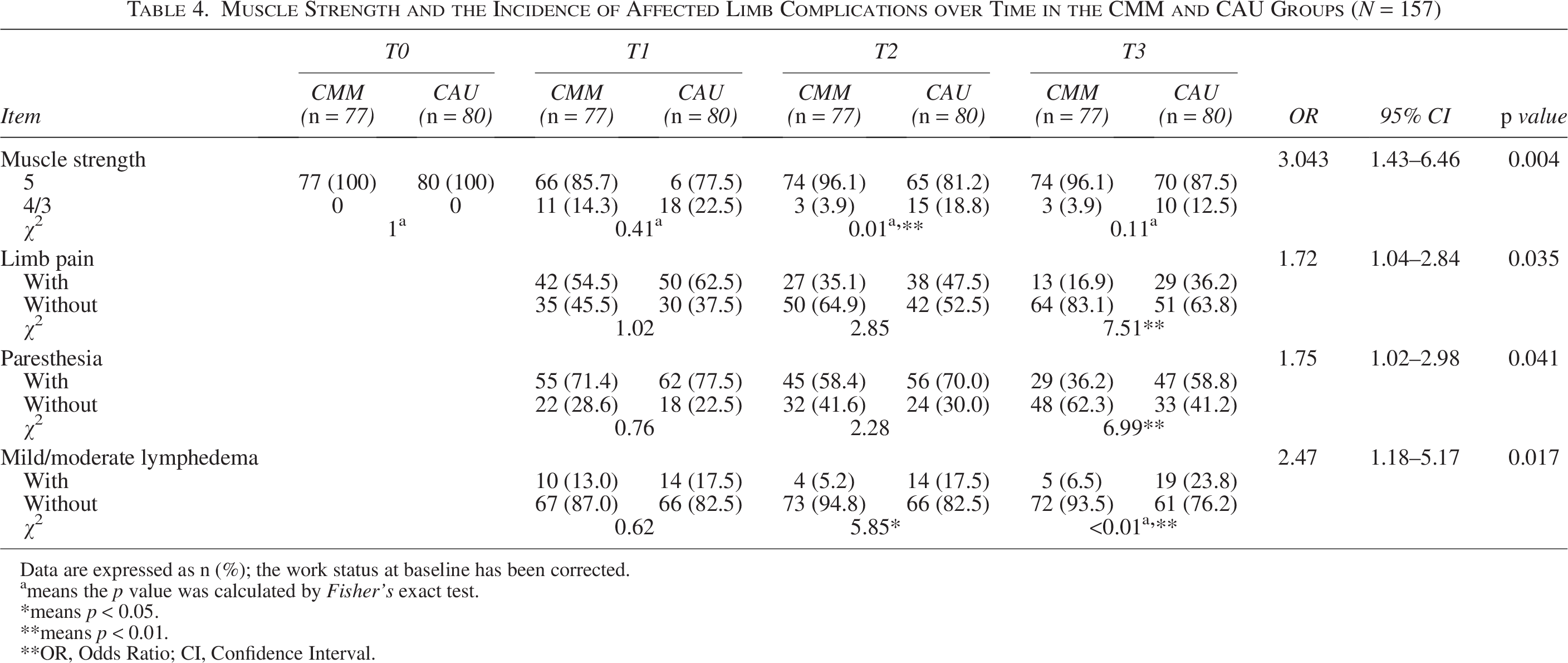
Data are expressed as n (%); the work status at baseline has been corrected.
means the p value was calculated by Fisher’s exact test.
means p < 0.05.
means p < 0.01.
OR, Odds Ratio; CI, Confidence Interval.
Effects of the intervention on the incidence of affected upper limb complications between the CMM group and the CAU group
As shown in Table 4, except for lymphedema in the CAU group, the incidence of upper limb complications in both groups declined from T1 to T3. The incidence of pain (OR = 1.72, 95% CI: 1.04–2.84), paresthesia (OR =1.75, 95% CI: 1.02–2.98), and lymphedema (OR = 2.47, 95% CI: 1.18–5.17) in the CMM group were significantly lower than those in the CAU group.
Discussion
Our study reports that upper limb dysfunction and complications may occur after breast cancer surgery and that the rehabilitation of an upper limb requires more than 1 year. To our knowledge, our study is the first to demonstrate the long-term effects of a CMM on postoperative upper limb function rehabilitation for patients with breast cancer. This study also illustrates a concrete model in China, which may help other researchers in implementing similar approaches or study designs.
Changes in upper limb function and limb complications after surgery among patients with breast cancer
Upper limb function among patients with breast cancer improved from the time of surgery for up to 1 year, yet limitations in upper limb function remained. These findings are consistent with previous studies by Assis 49 and Dylke, 13 suggesting that continued rehabilitation of upper limbs is needed for at least 1 year. Our data show that the ROM in the upper limb and patient-reported function limitations were at their worst 3 months after surgery. Upper limb function then improved rapidly from 3 months to 6 months, and slowly improved from 6 months to 1 year. Thus, functional exercises should be continued even after 3 months. Among the upper limb complications, except for the increased incidence of lymphedema of the affected upper limbs in the CAU group, the incidence of the other complications in both groups decreased from 3 months to 1 year. Previous studies showed that limitations in upper limb function and limb complications lead to reduced ability in daily activities and impact on one’s quality of life, thereby increasing the burden on caregivers. 21 Therefore, more efforts are needed to alleviate functional limitations in the upper limb of patients with breast cancer after surgery.
Patients in the CMM group showed significantly better limb function and lower incidence of limb complications than those in the CAU group
Our study shows that, compared with the CAU group, the CMM group could improve the function of the affected limb and reduce the incidence of the limb complications for patients with breast cancer. It provides evidence that the CMM effectively promotes postoperative rehabilitation of the affected upper limb among patients with breast cancer, which is consistent with the studies of Goodwin 41 and Xing. 42 The positive effects observed in the CMM group were probably due to the following. First, in the CMM group, the case manager provided whole process management including inpatient management and discharge follow-up, which is one of the biggest strengths of the CMM. During the patients’ hospitalization, the case manager provided important information on functional rehabilitation of the affected limb, assessed their mastery level, and improved patients’ knowledge and attention of limb function and complications. After discharge, the case manager provided more than 1-year follow-up as a personal consultant for patients and their caregivers, since the limitation of the affected limb may last for more than 1-year post-surgery. The case manager regularly evaluated the condition of the affected limb and encouraged the patient to perform functional exercises. Second, patients in the CMM group were provided with a multidisciplinary coordinated management by a multi-disciplinary team, which facilitated a more robust and professional care plan. The multidisciplinary team integrated the expertise of surgeons, physicians, radiologists, case managers, nurses, psychologists, physiotherapists and lymphedema therapists. The multi-disciplinary team worked to develop a treatment plan for the patients, so that they could obtain the most successful surgery and radiotherapy plan, in an attempt to reduce the occurrence of limb dysfunction and complications. During the recovery, the case manager referred the patient to a lymphedema therapist or rehabilitation therapist when serious limb dysfunction or lymphedema was found.
The adaptation of the case management model in our study
The CMM has been popularized in western countries as well as in Hong Kong and Taiwan.26,34–37,50 However, given the heterogeneity of culture, we adapted the CMM in our study. First, our study supported oncology nurses to take charge of case management over social workers or volunteers because nurses had more professional knowledge and were conducive to better collaboration with the multi-disciplinary team, which is the same as Jennings’, 40 Goodwin’s, 41 and Chen’s 32 studies. In addition, our CMM was conducted as a combination of inpatient management and discharge follow-ups, which was different from Bleich’s study. In Bleich’s study, case managers were not directly involved in the inpatient management, which may be one of the reasons why their CMM did not obtain any better outcomes than regular care. 34 The CMM combined inpatient management and discharge follow-up, which helped to foster partnership and trust with patients as well as their caregivers and was an effective way to improve cancer patients’ transition from the hospital to the home. That being said, the workload of the case manager was demanding, so the first visit was in the inpatient setting, not the clinic, which is different from other studies.32,41 Our experience suggested that our adapted CMM is a feasible and effective way to improve the short and long-term quality of care and patient outcomes among patients with breast cancer, which could be implemented into future practice and studies.
Limitations
This study has several limitations. One, the study was not a randomized controlled study, therefore, the patients in the two groups may be imbalanced. Two, the study was conducted at a single cancer center, which may limit its generalizability. Multisite randomized control trials are needed to investigate the effectiveness of the CMM. Three, this study focused on the effectiveness of the CMM, while a cost-effectiveness analysis of the CMM is lacking. Future studies are needed to provide evidence on the costs of the CMM so that stakeholders can make informed decisions.
Conclusions
Postoperative upper limb dysfunction and complications in patients with breast cancer lasted for more than 1 year. The nurse-led CMM effectively promoted the rehabilitation of affected upper limb function and reduced the incidence of limb complications among breast cancer patients. The nurse-led CMM is a feasible and effective approach for breast cancer patients in improving the short-term and long-term quality of care and, crucially, patient outcomes.
Authors’ Contributions
H.Z.: Conceptualization, writing—original draft. Y.L.: Conceptualization, writing—original draft. J.L.: Conceptualization, writing—original draft. X.Z.: Methodology, validation. Y.J.: Methodology, validation. C.G.: Formal analysis. L.Z.: Resources, project administration, writing—review and editing. H.Q.: Resources, supervision, writing—review and editing, funding acquisition. L.S.: Data curation, investigation, visualization.
Footnotes
Acknowledgments
The authors thank all the participants for their contributions to this study. The authors would also like to thank Mr. Christopher Lavender from Sun Yat-sen University Cancer Center’s Editorial Office for proofreading this article.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
This work was supported by the Science and Technology Planning Project of Guangdong Province of China (grant numbers: 2016A020215091) and the Guangdong Basic and Applied Basic Research Foundation (2025A1515011824).
Ethical Approval
Approval was obtained from the ethics committee of Sun Yat-sen University Cancer Center (No.GYXHY-2014-01-02). The procedures used in this study adhered to the tenets of the Declaration of Helsinki.