
Abstract
Background:
Lymph flow measurements can assist in attaining a better understanding of the lymphatic system’s function and its diseases. However, in vivo assessment of lymph flow has been challenging. Transit-time ultrasound technique (TTUT) provides direct quantitative lymph flow values and has been used to successfully measure lymph flow in patients with secondary lymphedema. Currently, no measurements using TTUT in healthy subjects have been reported. The aim of this study is to measure lymph flow in healthy subjects using the TTUT.
Methods and Results:
Twenty consecutive patients who had an indication for a free radial forearm flap (FRFF) reconstruction were included in the study. Patients with scars on their arms, a history of extremity lymphedema, metastatic disease, or axillary node dissection were excluded. The Transonic® Microvascular Flow Probe was used to measure lymph flow during FRFF reconstruction in accordance with the Transonic® protocol for Quantitative Patency Assessment. The subdermal superficial lymphatic collecting vessels had a mean diameter of 0.40 ± 0.10 mm (range: 0.3–0.5 mm) and a mean lymph flow velocity of 0.45 ± 0.48 mL/min (range: 0.08–1.68 mL/min). Neighboring subdermal veins measured had a mean diameter of 0.48 ± 0.11 mm (range: 0.03–0.7 mm) and a mean blood flow velocity of 0.96 ± 1.73 mL/min (range: 0.07–7.40 mL/min).
Conclusion:
The TTUT is a viable method to measure real-time lymph flow velocities in healthy subjects. Future studies with a larger sample size are required to validate the TTUT measurement accuracy and establish clinical correlations.
Introduction
The lymphatic system has an important role in fluid homeostasis, since it drains fluid and metabolic waste from tissues and plays a role in immunity by providing a route for cells to move from tissues to lymph nodes. 1 Lymph transport is a dynamic process and is dependent on an array of internal and external factors. When lymph fluid enters the initial lymphatic capillaries through an increase of hydrostatic forces, it is propelled into collecting vessels. 2 These collecting vessels differ in morphology from the lymphatic capillaries and contain smooth muscle cells (SMC) and intraluminal valves. The region between these valves are lymphangions, and these are the functional unit driving lymph flow.3,4 The rhythmical propulsion of lymph is dependent on intrinsic factors such as preload and afterload, transmural pressures, and shear stress. 5 In addition the tone of the collecting vessels can also be influenced by neurotransmitters, hormones and other metabolites.6–8 The SMC and lymphatic endothelial cells possess mechanosensors, which can detect these stimuli and are able to adjust the contraction frequency and amplitude. 2 Furthermore, the rhythmical propulsion within the lymphatic collecting vessels also responds to external stimuli such as arterial pulsation, skeletal muscle contraction, and respiratory movements. 9 Despite the critical role the lymphatic system has in many disorders, very little is known about the lymphatic system compared to the cardiovascular system. One of the reasons for this knowledge gap might be the lack of imaging or measuring techniques to obtain quantifiable information, both in health and disease. By measuring lymph flow, we may attain a better understanding of the lymphatic system and its function. 10 Up until now, quantifying lymph flow has been challenging. Multiple techniques to measure lymph flow have been proposed; however, thus far no consensus has been reached on the optimal measuring technique. Transit-time ultrasound technology (TTUT) uses the transit time differential principal to measure the difference between transit times of an ultrasonic signal traveling back and forth between two transducers. 11 TTUT has been utilized in the assessment of blood flow to measure patency and flow velocity in cardiothoracic and neurosurgery.12,13 In lymphedema surgery, TTUT has shown promising results in the direct measurement of lymph flow in patients with lymphedema. Due to its sensitivity reaching 0.01 mL/min flow velocities in microscopic vessels, it can provide quantifiable real-time measurements in lymphatic vessels. 14 Misère et al. 15 assessed patency of lymphatic vessels during lymphaticovenous anastomosis (LVA) surgery for extremity lymphedema, corroborating its feasibility in the measurement of lymph flow before and after performing the anastomosis. However, to date there are no studies evaluating the use of TTUT in physiological conditions. Thus, the aim of the current study is to describe real-time lymph flow presenting at the lymphatic collecting vessels measured on healthy patients using the TTUT.
Materials and Methods
The prospective observational pilot study was performed from November 2020 to April 2022. Twenty consecutive patients from the Plastic and Reconstructive Surgery department at the Maastricht University Medical Center, the Netherlands, who underwent free radial forearm flap reconstruction (FRFF), were included.
The inclusion criteria consisted of patients older than 18 years with an indication for free radial forearm, absence of clinical upper extremity lymphedema, no previous operations, or scars at the upper extremity. The exclusion criteria were a history of lymphedema, metastatic disease, and a history of previous operations at the upper extremity, such as axillary lymph node dissection. Written consent was received by all participating subjects. The study was performed in accordance with the Declaration of Helsinki and was approved by the medical ethical committee (NL69899.068.19; METC 19-035).
Measurement technique
All operations and measurements were performed under general anesthesia by the same qualified plastic surgeon (S.S.Q.) from the Maastricht University Medical Center. A small incision of 1.5 cm was made at the incision site of the FRFF at the wrist crease. Using a surgical microscope, the lymphatic collecting vessels and adjacent subcutaneous veins with similar diameters were harvested in the subdermal plane.
Flowprobe measurement method
The flow was measured according to the Transonic® protocol for Quantitative Patency Assessment. 16 Prior to incision, the flow probe (Microvascular Flow Probe HT363: Transonic Europe Elsoo, Netherlands) was calibrated according to the manufacturer’s instructions by submerging the probe in a saline solution to remove any air and then submerging the probe in room-temperature sterile ultrasonic gel (Parker Laboratories, Fairfield, U.S.A). A probe of 0.7 mm was used for the measurements, as it is the smallest commercially available flow probe. For accurate measurement, >70% of the diameter of the probe-sensing window had to be covered by the collecting vessel. To provide ample room for the introduction of the flow probe head and avoid interference of the acoustic transmission, approximately 1 cm of the collecting lymphatic vessel and adjacent vein were harvested. Subsequently, the flow velocity was measured in the lymphatic collecting vessels and adjacent subdermal veins. Once a repeatable and reproducible waveform was visible on the monitor, the flow was observed for an extra 15–20 seconds; afterwards, the mean flow velocity was noted. This procedure was performed once per lymphatic collecting vessel and once per subcutaneous vein. Flow values were given in mL/min. Prior to the measurement, the diameter of the lymphatic vessel and subdermal vein were measured with a sterile ruler. Measurements took approximately 10–15 minutes in total.
Outcomes
The flow velocity [mL/min] of the lymphatic collecting vessel and adjacent subdermal veins in subjects with a healthy upper extremity was measured and described.
Statistical analysis
Demographic data were presented as means with standard deviation. The flow velocities were reported as means with standard deviation and range (min–max). The differences between the lymph flow and blood flow were analyzed using a paired sample test. Results were analyzed with SPSS Statistics 25.
Data sharing statement
For original data, please contact
Results
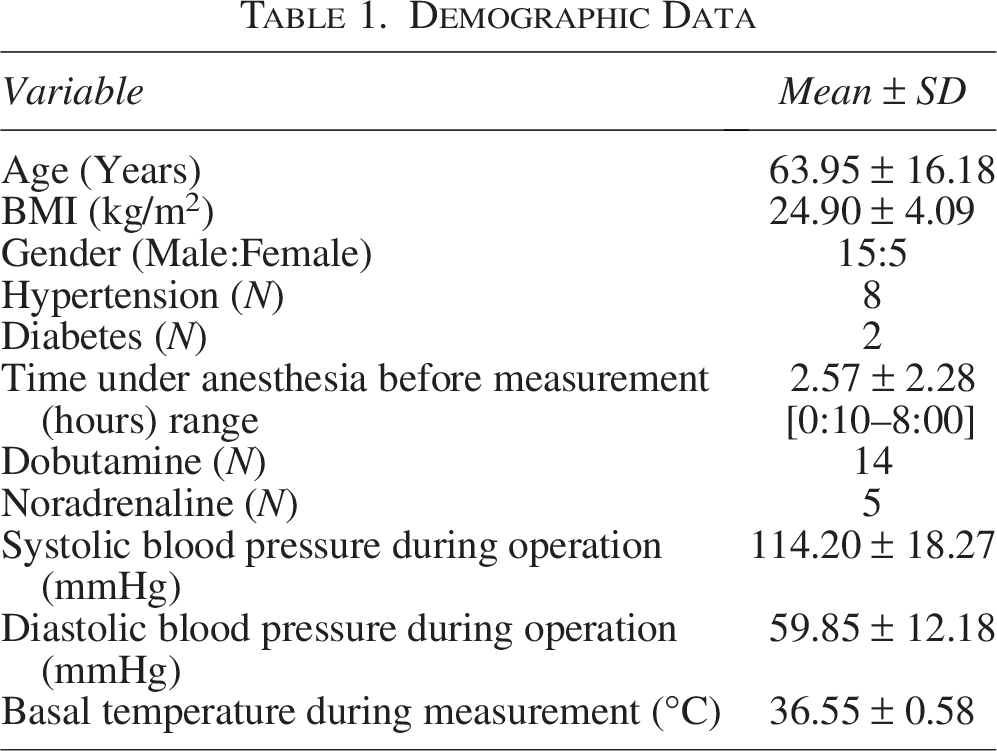
A total of 20 patients were included in the study. In one patient, the flow could not be measured due to technical reasons. The baseline characteristics are presented in (Table 1).
Demographic Data
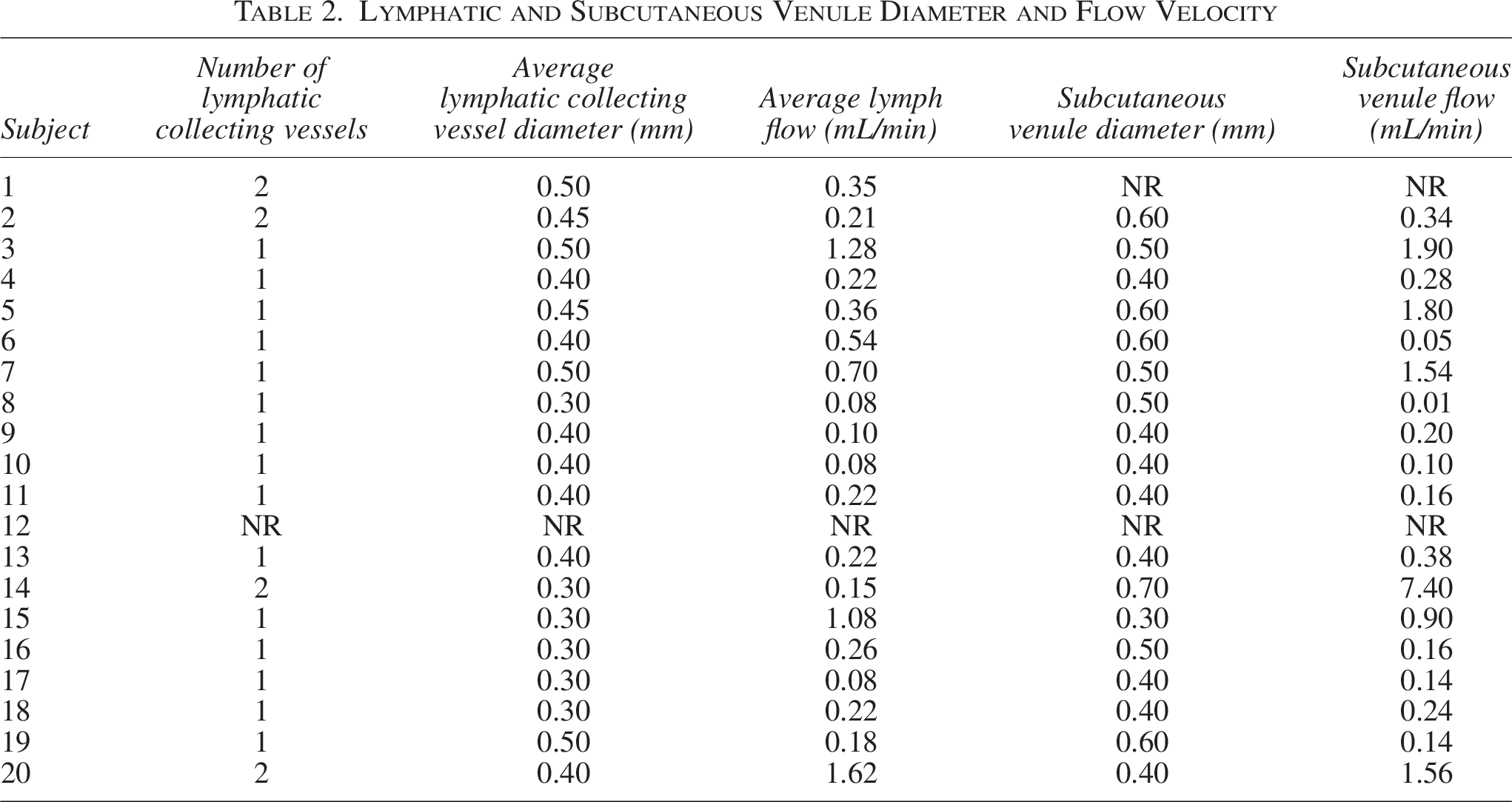
An average of one to two lymphatic collecting vessels were measured per patient with an average diameter of 0.40 ± 0.10 mm (range: 0.3–0.5 mm). The mean lymph flow velocity in these vessels was 0.45 ± 0.48 mL/min (range: 0.08–1.68 mL/min). One subcutaneous vein was measured per patient with an average diameter of 0.48 ± 0.11 mm (range: 0.03–0.7 mm) and an average blood flow velocity of 0.96 ± 1.73 mL/min (range: 0.07–7.40 mL/min). The difference between the mean values was not statistically significant (p = 0.210). In (Table 2), the mean diameter of the lymphatic vessels and veins with their corresponding mean flow velocities are shown.
Lymphatic and Subcutaneous Venule Diameter and Flow Velocity
Discussion
We have demonstrated that TTUT is able to measure lymph flow in healthy subjects without lymphedema. This method allows for direct and real-time measurement without the use of labels or tracers. The average lymph flow velocity was 0.45 ± 0.48 mL/min (range: 0.08–1.68 mL/min), while the lymphatic collecting vessels were on average 0.40 ± 0.10 mm (range: 0.3–0.5 mm) in diameter. Conversely, the subcutaneous veins had higher flow rates, registering an average blood flow velocity of 0.96 ± 1.73 mL/min (range: 0.07–7.40 mL/min), with a similar diameter vessel to that of the collecting vessels at 0.48 ± 0.11 mm (range: 0.03–0.7 mm). However, the difference in flow rates between the lymphatic collecting vessels and subcutaneous veins was not of statistical significance.
Until now, the primary application of lymphatic mapping has been the detection of lymph nodes, rather than lymphatic vessels, because the importance of lymph node tracking in metastatic disease outweighed the interest in lymphatic vessel function. 17 Consequently, data on peripheral lymph flow is sparse, and therefore reference values do not exist. 15 Nowadays, more studies have attempted to pioneer a reliable method to measure lymphatic function using multiple techniques, however not without limitations. Most of these quantification methods have to account for spatial-temporal resolution, range of depth and/or for the optical properties of the skin and tissue, which can cause distortion when visualizing and quantifying lymphatic function. Techniques such as Doppler optical coherence tomography, fluorescence recovery after photobleaching, and video microscopy cell tracking have shown potential in quantifying lymphatic function and lymphatic velocity; however, they have only been tested in a variety of animal models.18–20 Concurrently, there is a lack of standardized protocols and other experimental variables such as position, use of pharmacological substances that influence tone, contractility, and intraluminal pressures, which in turn resulted in disparate results. 21 Most importantly, these techniques cannot be applied in a clinical setting, as the data obtained from these measurements cannot be compared or extrapolated to lymph flow measurements in human subjects because of evident differences in volume and pressure gradient due to a higher mass and a higher pressure gradient imposed by gravity.
In humans, imaging modalities such as near infrared fluoroscopy (NIRF), magnetic resonance lymphography, and lymphoscintigraphy have been used to measure lymphatic function and flow. As mentioned previously, resolution, depth of imaging, and scattering influence accurate lymph flow quantification. In these cases, most importantly, regional labeling of lymphatic fluid is necessary, as lymphatic fluid is clear and in itself is difficult to label. Regional labeling is achieved by injecting radioactive or fluorescent substances into the tissue, which increases interstitial pressures and alters lymph viscosity and lymph flow. 18 Furthermore, comparing studies utilizing different investigative methods poses great difficulties due to the difference in technique and measuring units. Additionally, integrated transit time is an absolute flow measurement and is quantified in volume per minute. As a result, our data could not be compared quantitatively with other techniques.
Up until now, most studies have used NIRF to measure lymph flow in healthy and diseased lymphatic vessels, which has shown consistent results. The flow velocities of healthy lymphatic collecting vessels of the upper extremities were between 0.76 and 1.1 ± 0.3 cm/s, while lower lymph flow velocities were found in patients with lymphedema. 22 NIRF imaging is limited by light scattering and spatial resolution and has an imaging depth of ∼1–2 cm; therefore, it cannot assess lymphatic function as a whole. 22
Modi et al. assessed lymph flow using lymphoscintigraphy and established a mean flow velocity of 0.15 ± 0.1 cm/min in healthy lymphatics versus 0.05 ± 0.14 cm/min in lymphedematous extremities. 23 In patients with lymphedema, the pumping ability of collecting lymphatic vessels was found to be lower and is proportional to the amount of swelling, suggesting pump failure and resulting in impaired flow. 24 Furthermore, lymphoscintigraphy and MRI have shown lower lymph flow velocities in comparison to NIRF. This might indicate that the uptake of the labeling solutions is different per imaging modality or that deeper lymphatic vessels might work differently than the superficial lymphatic vessels. However, the data on the deeper lymphatic vessels is sparse. 22
TTUT has been applied for the measurement of lymphatic collecting vessels in patients with lymphedema. Misère et al. 15 measured lymph flow in 25 patients with secondary lymphedema. The mean lymph flow velocity after LVA was slighted increased than before the LVA (0.27 ± 0.22 mL/min and 0.25 ± 0.19 mL/min, respectively). 15 The difference in flow velocities is expected since the functioning of the lymphatic vessels is impaired in lymphedema.
What was notable in the study by Misère et al. was the high variability in lymphatic flow velocity, which was also established in our cohort. The variability could be attributed to the variation in size of the lymphatic vessels. However, due to the limited population in our cohort, no analysis could be performed to further substantiate this finding. Using the same technique, Chen et al. reported flow values between 0 and 1.2 mL/min in the lymphatic collecting vessels and higher flow values of between 0.22 and 1.4 mL/min after the LVA. 14 Currently, surgeons use their experience and judgement to assess which lymphatic vessels are suitable for anastomosis, taking factors into account, such as lymphatic vessel fibrosis and the degree of venous backflow, are visual assessment tools for the success of the LVA. Both Chen et al. and Misère et al. established that using TTUT, the surgeon can quantitatively verify flow before LVA and after LVA. The aforementioned findings implicate that TUTT has a purpose in vessel selection and patency verification during LVA surgery. Furthermore, additional studies are required to validate its reliability and accuracy in this setting.
Limitations
This is the first study describing lymph flow velocity using TTUT in healthy subjects. As mentioned before, lymph flow has been historically difficult to quantify because the lymphatic system is highly adaptable, and multiple intrinsic and extrinsic factors influence vessel tone, intraluminal pressure, and contraction, resulting in variances in the flow. The largest limiting factor was that most lymphatic collecting vessels had a small diameter, filling less than 70% of the probe. Healthy lymphatic collecting vessels have a diameter between 0.05 and 0.40 mm, which is somewhat smaller compared to lymphedematous lymphatic vessels, which are generally dilated. Furthermore, the use of vasoconstrictive agents such as noradrenaline and dobutamine in itself might have caused vasoconstriction in the lymphatic collecting vessels. 2 The mismatch in size between the lymphatic collecting vessels size and the probe might have led to a decrease in accuracy of the measurement of between 4% and 15%.25,26 The accuracy is likely dependent on the positioning of the vessel in the flow probe, as on the lateral borders of the probe the accuracy is diminished. In any case, if the probe was unable to measure lymphatic vessels, no waveform pattern would have been seen on the monitor. Furthermore, we were only able to measure one to two collecting lymphatic vessels per patient, as suitable collecting lymphatic vessels were hard to find using a conventional surgical microscope. The subjects in this study were in a supine position, under prolonged general anesthesia, and necessitating pharmaceutical support, which posed limitations for the measurements of lymphatic flow.
Russel et al. illustrated that specific drugs has shown to disrupt molecular signaling that modulates lymphatic tone, flow resistance, and thus lymphatic function. Propofol and sevoflurane have shown to inhibit spontaneous contraction of the lymphatic pacemaker cells of lymphatic vessels in murine specimens. Analogously, noradrenaline has also been shown to disrupt electrical activity within the SMC, resulting in diminished contraction of the lymphatic vessels.27,28 However, the extent of the impact of these agents on lymphatic function still poses an open question.
Therefore, further research should be conducted to better understand lymph flow and its determinants. 2 TTUT could be a useful technique to catalyze studies into the regulation of lymph flow in both healthy and diseased states. Although using TTUT is an invasive technique requiring direct access of the lymphatic vessels, this study represents the first attempt to obtain direct measurements of lymph flow in physiological condition. TTUT may have a potential clinical role in the assessment of peripheral lymphatic vessels during lymphatic surgery and could eventually improve surgical outcomes for patients with lymphedema since the quantification of lymph flow in different lymphatic collecting vessels can help to choose the most proper and functioning vessel for LVA. In the future, the development of a smaller microvascular probes may also result in more accurate measurements and be more suitable to assess lymph flow in physiological conditions.
Conclusion
TTUT using a microvascular flow probe is an adequate method to measure real-time, quantitative lymph flow in lymphatic collecting vessels in healthy subjects. However, future studies with a larger sample size are required to validate the accuracy of the measurements using TTUT, establish clinical correlations, and evaluate the determinants of lymph flow.
Authors’ Contributions
Y.M.J., R.M., S.R.v.d.H., and S.S.Q. performed the measurements; Y.M.J. and S.R.v.d.H. analyzed results and made the tables; R.M. and S.S.Q. research design. Y.M.J. wrote the article. Y.M.J., R.R.W.J.v.d.H., and S.S.Q. reviewed the article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.