
Abstract
Background:
Recent studies have consistently shown that patients with lipedema are at a higher risk for depression and anxiety. The aim of this study is to identify the psychological factors associated with lipedema syndrome (LS) and their link to the patient’s psychological symptomatology.
Methods:
A mixed-methods approach was employed, combining quantitative and qualitative components. The quantitative component involved anonymous online questionnaires, including a Health and Demographic Questionnaire, the body satisfaction and global self-perception questionnaire (BSGSPQ), the lymphedema quality of life questionnaire (LYMQOL), and the Hospital Anxiety and Depression Scale (HADS). The qualitative component consisted of oral interviews to explore the complexity of the phenomenon. Participants included those with “easy bruising,” a waist-to-hip ratio ≤0.7 (W/H), and pain levels ≥4/10 on the visual analogue scale (VAS).
Results:
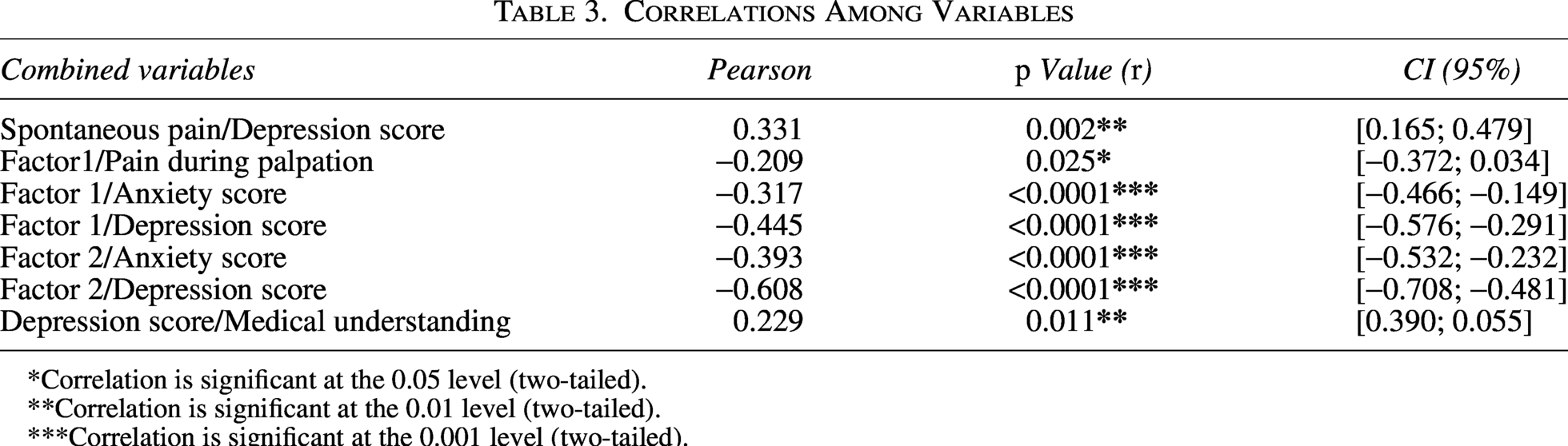
Our findings indicate that the level of depression is positively correlated with spontaneous pain (p = 0.002; r = 0.331) and the lack of medical understanding (p = 0.011; r = 0.229). Anxiety scores are inversely correlated with body satisfaction (r = −0.317) and global self-perception (r = −0.393); similarly, depression scores show similar correlations with body satisfaction (r = −0.445) and global self-perception (r = −0.608), all with p value of <0.0001.
Discussion and Conclusion:
This study highlights significant connections between the physical symptoms and mental health in patients with LS. The more affected the self-perception, the greater the depression and anxiety levels. These multiple contributing factors may explain the decline in quality of life (QOL) and deterioration of mental health. It is therefore crucial to proactively integrate mental health management into the care of LS patients. Future research should focus on identifying concrete, actionable methods to support women experiencing LS.
Introduction
Lipedema syndrome (LS) is defined as a chronic painful syndrome of the subcutaneous fatty tissue. It typically manifests during periods of major hormonal changes such as puberty, pregnancy, or menopause1–4 and affects almost exclusively women. 5 Lipedema is classified in types and stages depending on the location and severity of the adipose accumulation. It typically involves the lower limbs symmetrically at the level of the hips, thighs, or down to the ankles, while always sparing the feet.6–8 Other clinical signs often accompany this condition, such as leg heaviness, fatigue, relative joint laxity, numerous stretch marks, and capillary fragility, which is expressed by easily bruising spontaneously or as soon as they are bumped, even slightly.6,9,10
Due to still unclear physiopathology knowledge about this syndrome, many affected women are misdiagnosed: Some are mistakenly classified as obese and receive treatments such as inadequate surgeries, dieting, and exercises, which have little or no effect on the pathological distribution of tissue.11–13 Women with lipedema frequently experience a sense of misunderstanding from both their social environment and the medical community, which often remains unaware of this condition.1,14,15 In certain cultural subgroups, societal pressures may lead to the development of body image issues related to the morphological characteristics of lipedema. 1 This stigmatization of body weight, coupled with uncontrollable physical changes and a perceived lack of support from health care professionals, appears to exacerbate the risk of depression, anxiety, eating disorders, among these women ultimately affecting/reducing their quality of life (QOL). 11 While efforts to recognize and manage LS are evolving, particularly through the integration of surgical and conservative therapies, the psychological aspects of this condition are still inadequately addressed. 16
The WHO defines QOL as “an individual’s perception of his or her place in life, in the context of the culture and value system in which he or she lives, in relation to his or her goals, expectations, norms and concerns.” 17 In 2015, Dudek et al. 11 studied factors affecting QOL in women with lipedema using the WHOQOL-BREF, which is based on physical, psychological, social, and environmental assessments. They found that the more severe the symptoms and the worse the experience, the worse the QOL. Fetzer and Wise’s study 5 confirms the findings of Dudek et al. 11 and estimates that 85% of patients with lipedema are mentally affected and struggle to adapt. Their professional careers, social lives, and sexual activities are impacted, which can lead to a loss of self-confidence, depression, and suicidal thoughts. 3 Romeijn et al. 18 reported in an online survey on the psychological characteristics of women with lipedema that 42% of 163 participants suffered from depression and anxiety. Depression was correlated with the severity of the symptoms and the presence of obesity as a comorbidity. It has also been shown that the greater the symptoms and depression severity, the lower the HRQOL scores.1,19 A 2022 study 19 states that patients with lipedema have difficulties with their emotional regulation strategies. They also have significantly higher levels of anxiety in contrast to controls. All these multifactorial signs and symptoms associated with persistent, insidious pain classify LS within the chronic pain syndromes. Previous studies have established that patients with lipedema can be considered individuals living with a chronic disease.20,21 This classification inherently includes the psychological characteristics typically observed in long-term pain patients.
In addition to the somatic disorders associated with LS, patients often experience significant psychological disorders that must be taken into account when planning their treatment strategies.14,19,22 The objective of this research is to better identify the psychological factors involved in LS and their link with the patient’s psychological symptomatology.
Materials and Methods
Study design and subject
It was an observational study with a mixed-method approach including quantitative tool (questionnaires) and qualitative tool (semistructured interview). Mixed-methods research captures not only clinical effectiveness through quantitative measures but also subjective patient experiences through qualitative insights. This dual approach is essential for understanding complex clinical contexts in which outcomes measure based on more than one symptom change. By integrating both data types, mixed-method designs more accurately reflect care processes, treatment adherence, and patient perspectives.23–26
The quantitative part of the study using questionnaires started in January 2020 and ended in May 2020. The research was conducted using an online questionnaire available in seven languages (French, English, Polish, Italian, Dutch, Spanish, and German). Women with lipedema were invited to complete it by health care professionals such as doctors and physiotherapists. In addition, advertisements were posted on lipedema social networks targeting a community of women suffering from the syndrome in different countries across the five continents, including Belgium. Only fully completed questionnaires were retained and filtered using the combination of the three criteria: “easy bruising,” a ratio “waist-to-hip” ≤0.7, and pain ≥4/10 on the VAS. Questionnaires were rejected if any of these characteristics were missing. This study includes both medically diagnosed and self-monitored patients or self-reported diagnoses, provided they met the inclusion criteria. Participants in the self-diagnosed group reported meeting several commonly recognized clinical features of lipedema, including symmetrical limb enlargement, pain on palpation, and characteristic waist-to-hip ratio thresholds. These criteria were described in the recruitment information to minimize misclassification. The potential bias introduced by this approach is discussed in our analysis section.
The qualitative part began in October 2020 and ended in April 2021. Due to the COVID pandemic, the interviews were postponed by several months. This part was based on the notifications we received out of 124 women who had already answered the quantitative part. Twenty-six women sent us a message indicating their willingness to participate in the second part of the study. This approach aimed to better understand the complexity of the phenomenon being studied and to avoid bias or over-representation of a single point of view. Finally, upon recontacting the 26 participants, a total of 17 French-speaking women responded and were included. We used a diverse sampling method among these women, taking into account three criteria: BMI (>or <30), age (> or <44 years), and the presence or absence of body image disturbance (based on the BSGSPQ).
This study was approved by the Hospital Ethics Committee of Brugmann; all participants signed informed consent.
Data
Quantitative part
All data were acquired using LimeSurvey, which is an online statistical survey software. The questionnaire consists of 87 questions, which are divided into three parts:
Part I—Introduction and informed consent form.
Part II—Health and demographic questionnaire.
This part contains three types of questions:
General anthropometric questions (age, weight, height, shoe size, etc.) Questions about lipedema (clinical signs, date of diagnosis, medical history, etc.) Questions about clinical signs experienced by participants (spontaneous pain, with pressure, with touching, level of pain, loss of mobility, fatigue, etc.)
Part III—Psychological questions.
This part is divided into three subquestionnaires:
Qualitative part
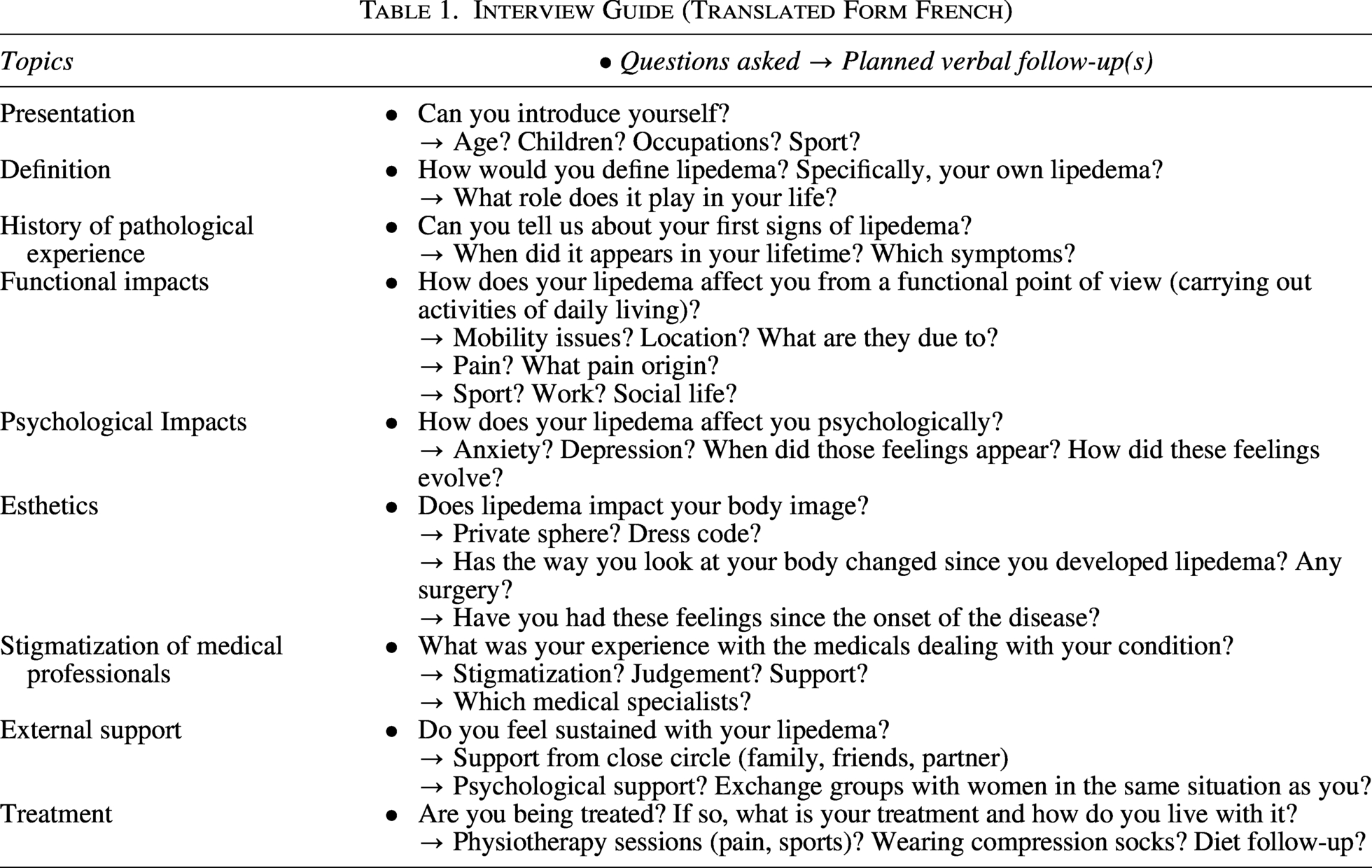
This study was conducted through semistructured interviews using a preestablished interview guide. These interviews were scheduled by appointment and conducted via video conferences on Microsoft Teams, WhatsApp, Skype, and Zoom. All interviews were recorded with the participants’ consent at the beginning of the interview. The interviews, which were unique in nature, lasted approximately 45 minutes. They were then fully transcribed and analyzed individually for consistencies and organized in six topics: the experience of diagnosis; perceived functional limitations; impact on mental health; impact on body image; the need for recognition; and experiences with the medical system (Table 1).
Interview Guide (Translated Form French)
Results
Quantitative results
There were 2214 answers to the study. Only 567 were fully completed. In the first analysis (March 23, 2020), we kept the 294 first-answered files. After applying inclusion, we had a group of 124 participants. During this study, we analyzed only the anxiety and depression scale (HADS).
Of those 124 completed files, 62% of patients had been diagnosed by a physician. The other 38% self-diagnosed have the same eligibility criteria. For these patients, five medical consultations were necessary, on average, to receive or confirm a medical diagnosis (Figs. 1 and 2; Table 2).
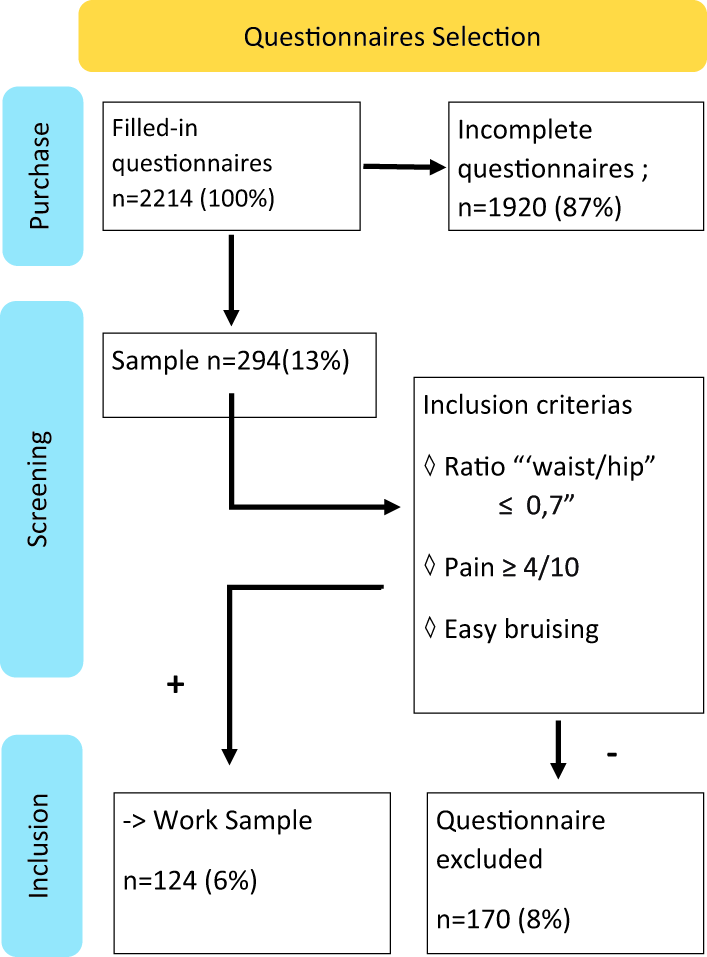
Diagram of Quantitative Selection.
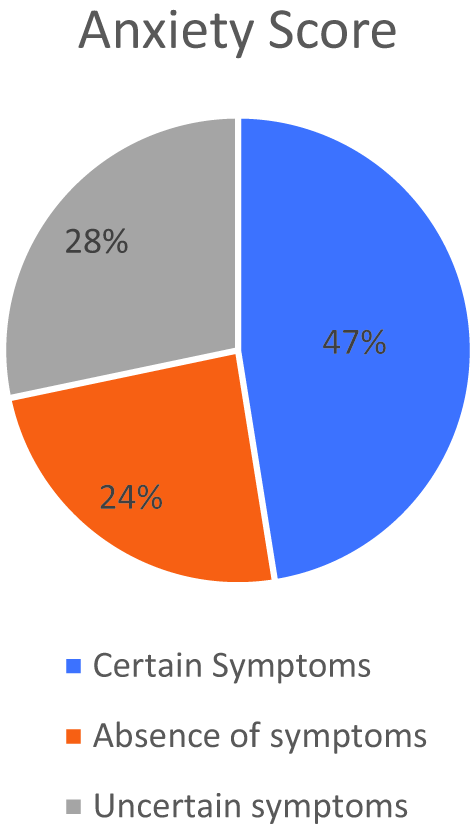
Diagram showing distribution of results about anxiety—out of the hospital anxiety and depression scale (HADS).
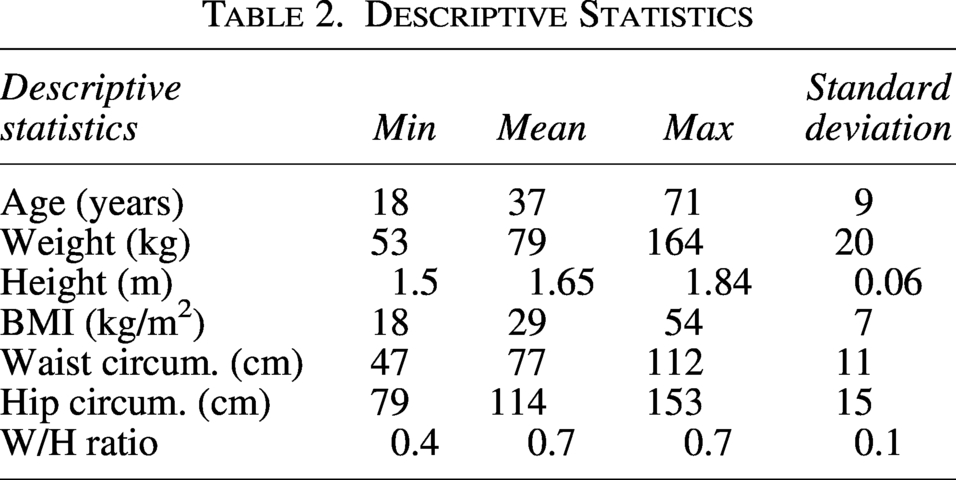
Descriptive Statistics
Interpretation: The HADS includes 14 self-rated items (7 anxiety, 7 depression), scored 0–3, with no somatic items. Subscale scores classify patients as: 0–7 = noncase, 8–10 = borderline (probable but not confirmedanxiety/depression), ≥11 = clinical case (Fig. 3).
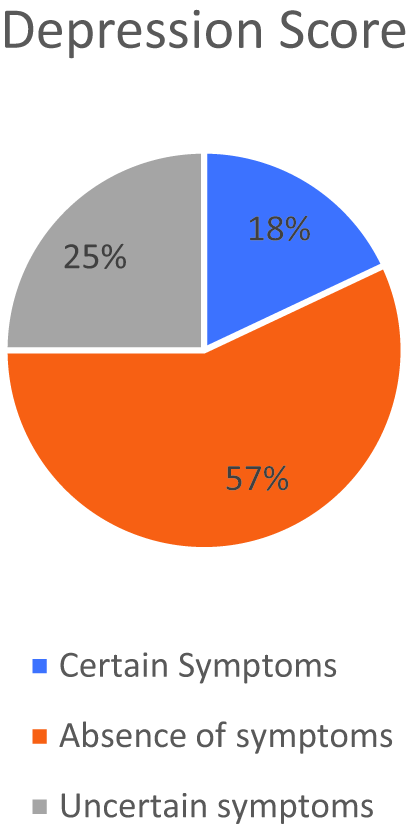
Diagram showing distribution of results about depression—out of the HADS.
Psychological follow-up
One of the questions was about the psychological therapy: “As part of my lipedema treatment, I have had psychological support.”
A patient said: “Honestly, yes, it’s necessary. If I could have had support and worked on my image regarding my body and on accepting the illness, I think I would have done less extreme things.”
Correlations among variables
Table correlation among variables
Factor 1 of BSGSPQ is corresponding to body satisfaction Factor 2 of BSGSPQ is corresponding to the global self-perception (Table 3)
Analysis of the data from this research shows that there is a highly significant correlation (0.001) for:
HADS (anxiety score) and BSGSPQ (Factor 1) HADS (depression score) and BSGSPQ (Factor 1) HADS (anxiety score) and BSGSPQ (Factor 2) HADS (depression score) and BSGSPQ (Factor 2)
Correlations Among Variables
Correlation is significant at the 0.05 level (two-tailed).
Correlation is significant at the 0.01 level (two-tailed).
Correlation is significant at the 0.001 level (two-tailed).
Qualitative results
Impact of the syndrome on mental health: Almost all participants (15 out of 17) reported reduced mental health due to LS.
Anxiety
Among the negative feelings experienced by patients, anxiety was described by a minority of women (5 out of 17), and more specifically, an anxiety focused on the evolution of their lipedema. We note the presence of frustration linked to powerlessness and injustice experienced in the face of a lack of understanding of the pathology.
Depression
LS can give rise to feelings described as depressive or, at least, tend to contribute to the emergence of such feelings (5 out of 17). Suffering from LS can even lead to the development of dark, self-destructive ideas.
Defense mechanisms
Defense strategies are then put in place to tolerate the psychological hindrances of the syndrome. One participant pointed out that LS evolves with age.
Body image
One of the difficulties mentioned by the participants stems from the way they view their own bodies. Indeed, all the women declared that their body image had been negatively affected by LS. Nevertheless, it is described that self-acceptance is becoming increasingly attainable, whether through a process of resignation or the natural passage of time.
The impact of body image issues results in several negative consequences for women with LS. For instance, many women report a disconnection from their own bodies, often experiencing the sensation of inhabiting a body that does not belong to them. A large majority (14/17) of participants report that LS has a detrimental impact on their intimate and emotional lives. The perceptions and judgments of others are identified as significant stressors for these women. Furthermore, challenges related to dressing are prevalent among patients (16/17). Consequently, these women often employ camouflage strategies to cope with their feelings of discomfort. It also appears that a negatively affected body image is associated with the development of eating disorders.
“It’s because you don’t exercise and that you don’t eat well” (a phrase said by a doctor to a patient); “I’ve always felt this misunderstanding, this rejection, if not contempt from doctors. We’re just fat people who deserve our discomfort (…) that we deserve what we have.” LS takes up a lot of space in the lives of patients. “I’ve tried psychological and psychiatric support that didn’t help at all. It works better now because I was able to explain LS, and I haven’t solved it yet…”
Discussion
The objective of this research was to gain a deeper understanding of the psychological factors associated with LS and their relationship to the patients’ psychological symptomatology. Overall, our data corroborate the well-documented symptoms of the condition. Patients with LS experience a decreased QOL, exhibit symptoms of anxiety and depression, and demonstrate altered body perceptions.
Our results show that depression level is correlated with spontaneous pain (p = 0.002; r = 0.331; r2 = 10.96%) and lack of medical understanding (p < 0.011; r = 0.229; r2 = 5.25%). Anxiety score is correlated with physical satisfaction (F1) and global self-perception (F2), respectively: r = −0.317, r2 = 10.05%; r = −0.393, and r2 = 15.45%. Depression score is correlated with F1 and F2, respectively: r = −0.445, r2 = 19.8%; r = −0.608, and r2 = 36.97%. Both for p < 0.0001. Pain on palpation is also positively correlated with the F1 (r = −0.209; r2 = 4.37%; p = 0.025). Those multiple causes can explain the loss of QOL and the deterioration of mental health.
The syndrome’s vicious circle
Dudek’s team 11 found that the more intense the symptoms of appearance-related distress and depression, the worse was the QOL. In fact, symptoms of LS decrease self-confidence and increase depression and tiredness. This leads to a decrease in physical activity, which, in turn, exacerbates pain and anxiety, contributing to the onset and maintenance of a vicious circle. 31 The interpretation of our results suggests that a similar pattern is observed for depression. In fact, depression can be up to 25.5%, 32 18% according to our study.
Patients’ explanations illustrate that the reductions or cessation of physical activity due to pain encourages a loss of self-confidence due to guilt. Simultaneously to decreasing activities, “healthy people” often tell patients that they do not eat properly or do not exercise enough in both their own private environment and in the medical setting. Thus, women find themselves caught between suffering, seeking solutions and explanations, trying to do the best they can depending on their clinical presentation, and the judgement of external observers—including health-care professionals.
Control and emotional regulation
In 2022, Al-Wardat et al. 19 taught us that LS patients had increased levels of anxiety related to difficulties with their emotional regulations and control. That adding a vulnerability factor to their overall mental health. Our results further showed that patients link their anxiety to the misunderstanding of their still unrecognized syndrome by many health care professionals (12/17 patients; 71% of interviewed patients). Furthermore, current treatment proposals seem to exacerbate emotional dysregulation by increasing the patients’ misunderstanding of their condition.
Follow-up and psychological component
Aksoy’s team 3 presented the impact of pain on QOL, depression, anxiety, mental health, and psyche-effect. They target pain as the primary symptom to address. However, the issue of which factor precedes the other remains unresolved. It may therefore be appropriate to treat pain while simultaneously providing direct support for patients’ anxiety. Physiological symptoms need to be treated in line with recommendations for psychological follow-up. In addition, psychosocial components also need to be addressed; this is highlighted by the actual low efficacy and limited availability of treatments, as well as the additional burden of psychosocial stress. 33 Therefore, therapists must have a proper understanding of the syndrome to provide appropriate support to patients, such as sociopsychological and self-confidence psychotherapy, psychological coping strategies, and multidisciplinary follow-up.11,34–36
Responsibilities of health care providers in clinical practice
It was highlighted, in 2021, that professionals play a critical role in both the diagnosis and the treatment of the illness.14,35 Nevertheless, our results show that even when depression scores are high, there is still an absence of psychological follow-up, which may be attributed to two factors: patients fail to consult psychologists and/or other therapists don’t encourage patients to seek counseling even when they present with severe depression.5,15 Results show that LS patients rarely consult psychologists: 8% in the quantitative sample and 3 out of 17 in the qualitative interviews reported doing so. Across interviews, women consistently underscored that anxiety and loss of self-confidence are closely linked to the lack of medical awareness. Indeed, participants reported requiring, on average, five medical consultations before receiving a diagnosis or even having lipedema considered. A 2018 review, by contrast, reported an estimated 2.5 consultations. 18 More recently, attention has been drawn to the large gap between symptom onset and treatment assignment. 35
Lipedema and body perception
All previous studies have shown that the LS has a psyche-effect on the patients. Our study emphasizes that the higher the depression score, the greater the decrease in global self-perception (r = −0.608; [−0.708; −0.481]; r2 = 36.97%) and body satisfaction (r = −0.445; [−0.576; −0.232]; r2 = 19.8%). We can predict with statistically significant strength (p value <0.0001) that the greater the patient’s negative global self-perception and body satisfaction, the more likely she is to experience depression. We can make a similar assertion regarding anxiety (respectively; r = −0.393; [−0.532; −0.232]; r2 = 15.45%; r = −0.317 [−0.466; −0.149]; r2 = 10.05%). Our quantitative findings were supported by qualitative reports describing altered self-perception, dissatisfaction with body image, and psychological distress.
The study also highlights that 10.96% of predicted depression can be accompanied by spontaneous pain, possibly triggered or exacerbated by tactile stimulation and pressure. 37 Findings indicate that a 4.37% of the variance in body satisfaction is explained by variation in spontaneous pain. In LS, touch directly induces pain. In contrast to other chronic pain syndromes, such as those associated with rheumatological conditions or cancers, pain in these disorders may fluctuate or remain constant. However, in the case of LS, tactile stimuli typically aggravate the pain, which contrasts with the generally beneficial effects of touch observed in other clinical contexts. This paradox is acknowledged in both clinical and private therapeutic settings, where touch is often perceived as healing. 38 Furthermore, therapeutic strategies should include social component and psychological support 39 alongside managing lifestyle and symptoms; it is necessary. Therefore, both body perception and body image should be considered simultaneously, in addition to pain in line with previous studies.
In summary, this study establishes new correlations between the known symptoms and mental health states of patients. Symptoms of LS are associated with deterioration in QOL, disturbances in body image, and heightened levels of anxiety and depression. The results reveal that the current absence of effective treatment options, therapeutic support, and delayed intervention contribute to feelings of neglect, potentially reinforcing or aggravating anxiety symptoms. Uncertainty about the potential progression of LS, the likelihood of worsening symptoms, and the severity of outcomes contribute to anxiety. These aspects have been reported by multiple patients, highlighting an indirect association between patients’ anxiety and their experience of LS.
In addition, our analyses indicate that insufficient medical understanding explains approximately 4.37% of the variance in depressive symptoms. A larger proportion may be linked to medical stigma, as suggested by Clarke et al.16,40 That aligns with participants’ narratives regarding perceived medical stigma through degrading and hurtful remarks. As previously noted, without more comprehensive patient phenotyping, clearer characterization of patient experiences, and robust diagnostic criteria, current gaps in lipedema management are likely to persist. 35
Limitations
Several study limitations have been identified. First, the inclusion of both clinically diagnosed and self-reported cases may have introduced diagnostic misclassification, as standardized clinical confirmation was not available for all participants. In addition, no subgroup analysis was performed, which limits the ability to assess whether findings differ across diagnostic categories or participant characteristics. Second, the cross-sectional correlational design prevents any causal inference. Although moderate-to-strong associations were observed, these relationships cannot be generalized to the wider population, particularly without multivariate adjustment.
The qualitative component also has limitations. Confidentiality constraints resulted in a low interview response rate (17/124), introducing potential selection bias, as respondents may differ from nonresponders in motivation, symptom severity, or psychosocial profile. The interviews were conducted in French and translated into English, which may have introduced subtle shifts in meaning and reduced transferability. As qualitative findings are context-specific, generalization remains limited.
These constraints highlight the need for longitudinal studies with standardized clinical verification to improve causal interpretation and strengthen the external validity of future research.
Conclusion
As emphasized by the link between LS symptoms and the resulting psychological distress, health care providers must prioritize the prevention of depression and anxiety within treatment protocols by addressing issues related to global perception and body image concerns. In addition, psychological support should be integrated into the overall treatment plan. The psychological factors associated with LS must be addressed alongside the underlying symptomatology to ensure comprehensive care.
Based on the results of the study, we conclude that the patients’ psychological well-being is closely interconnected with their experiences of spontaneous pain, loss of mobility, and the presence of empathetic and understanding health care professionals. These findings also indicate a need for improved clinical education regarding lipedema, as delayed diagnosis and limited provider awareness were associated with psychological burden. Future work should address not only patient support but also training and awareness among health care professionals.
Further studies should investigate which psychological support or therapy is the most efficient in LS follow-up. Approaches, such as mindfulness, sophrology, acceptance, discussion groups, psychological coping, lifestyle adjustments, and commitment therapy, could all be considered.
Authors’ Contributions
B.S.: Formal analysis, writing—original draft, and visualization. V.S.: Writing—review and editing. J.-P.B.: Conceptualization, methodology, validation, data curation, writing—review, and project administration. E.J.: Formal analysis and investigation. E.L.: Formal analysis and investigation. J.F.: Conceptualization, methodology, validation writing—review and editing, supervision, and project administration.
Ethics Statement
Ethical approval for this study was granted by the Hospital Ethics Committee of Brugmann under reference B077201941674. Written informed consent was obtained from all participants. Interview recordings were stored on a secure, encrypted server and anonymized prior to transcription.
Footnotes
Author Disclosure Statement
The authors declare to have no conflicts of interest with respect to this article.
Funding Information
No funding was received for this article.