
Abstract
Background:
Gluteal lymphedema is often developed by proximal edematous type of lower extremity lymphedema (LEL) and severe LEL. This study aimed to clarify the watershed of collecting lymph vessels in the gluteal region using indocyanine green (ICG) lymphography.
Methods:
Medical records of cancer survivors who underwent ICG lymphography for secondary lower lymphedema screening from November 2020 to September 2023 were reviewed. Non-lymphedematous limbs without a dermal backflow pattern on ICG lymphography (ICG stage 0) were included. 0.1 mL of ICG was injected intradermally at five points; the tip of the coccygeal bone, the gluteal fold, the crosspoint connecting those points and the mid-lateral thigh, and the midpoints of them in a prone position and named H1–H5 from medial to lateral. Based on ICG lymphography findings, the posteromedial and posterolateral pathway directions of collecting lymph vessels, shown as linear patterns, from each point were investigated.
Results:
A total of 20 limbs of 15 cancer survivors were included. The posterolateral pattern lymphatic pathway from H1/H2/H3/H4 was observed in 16/15/3/4 limbs. The posteromedial pattern lymphatic pathway from H2/H3/H4/H5 was observed in 13/15/18/10 limbs. Anteromedial pattern lymphatic pathway from H5 was observed in 6 limbs.
Conclusions:
Multiple ICG injections enhanced the watershed line of collecting lymphatic vessels in the gluteal region, which would be affected for gluteal lymphedema diagnosis and treatment.
Introduction
Lymphoedema is a chronic and fragile edematous disease, occasionally affected following surgical treatment for malignancy. While lymphedema of the lower extremity (LEL) and its burden on patients’ quality of life have been investigated in many published studies, there is very little literature on gluteal lymphedema.1–6 However, many lymphatic surgeons and therapists are concerned that the proximal edematous type of lower extremity lymphedema (LEL) and severe LEL can affect the hip region and lead to gluteal lymphedema. This condition thickens the dermal and subcutaneous tissues on the affected side, resulting in asymmetry of gluteal height compared to the contralateral side. Consequently, patients may experience spinal misalignment, discomfort in the sitting position, and lower back pain due to persistent pelvic inclination.5,6 Furthermore, some articles have already been written about gluteal regions’ atypical findings in image examinations.2,7
Considering the treatment of gluteal lymphedema, conservative treatments such as compression therapy and manual lymph drainage (MLD) would be applied first as the gold standard,8–10 and in progressive and refractory cases, lymphatic reconstructive surgery such as lymphaticovenular anastomosis (LVA) is considered.11,12
Although the watershed of the collecting lymphatic vessels of the thigh and their anatomical sites have been clarified,13–15 collecting lymphatic anatomy of the gluteal is not defined yet. In some kinds of literature, collecting lymphatic vessels’ watershed of the back is midline.16,17 Conversely, several reports have identified the lateral midline as the watershed region of the thigh.13,15 Therefore, the watershed line would be changed laterally from the midline of the back to the lateral midline of the thigh. Gluteal lymphedema is uncommon, yet it may become clinically significant in certain cases. Although an indocyanine green (ICG) lymphography protocol for the gluteal region based on lymphosome anatomy is required, the true watershed remains undefined, and the optimal injection site has not been determined. Since visualization of two adjacent lymphatic territories from a single injection suggests a watershed location, the aim of this study was to clarify the superficial gluteal lymphatic anatomy and to establish a clinically relevant ICG lymphography technique.18–20
Methods
Medical records of cancer survivors who underwent ICG lymphography for secondary lower lymphedema screening from November 2020 to September 2023 were reviewed. This retrospective study included patients who underwent pelvic lymphadenectomy and presented with an unaffected lower limb. The gluteal lymphatic pathways were investigated based on the non-lymphatic limb with no dermal backflow. Non-lymphedematous limbs without dermal backflow patterns on ICG lymphography (ICG stage 0) were included to evaluate the gluteal lymphatic pathways (Table 1). ICG lymphography was also performed for lymphedematous limbs as well as non-lymphedematous limbs, and the data were corrected. However, the lymphatic anatomy of lymphedematous limbs would have changed because of the interruption of the lymphatic transport system; for example, the watershed line may shift toward the side of dermal backflow due to the relative predominance of the collecting lymphatics on the contralateral side, so they were omitted.
ICG Stage Based on ICG Lymphography Findings
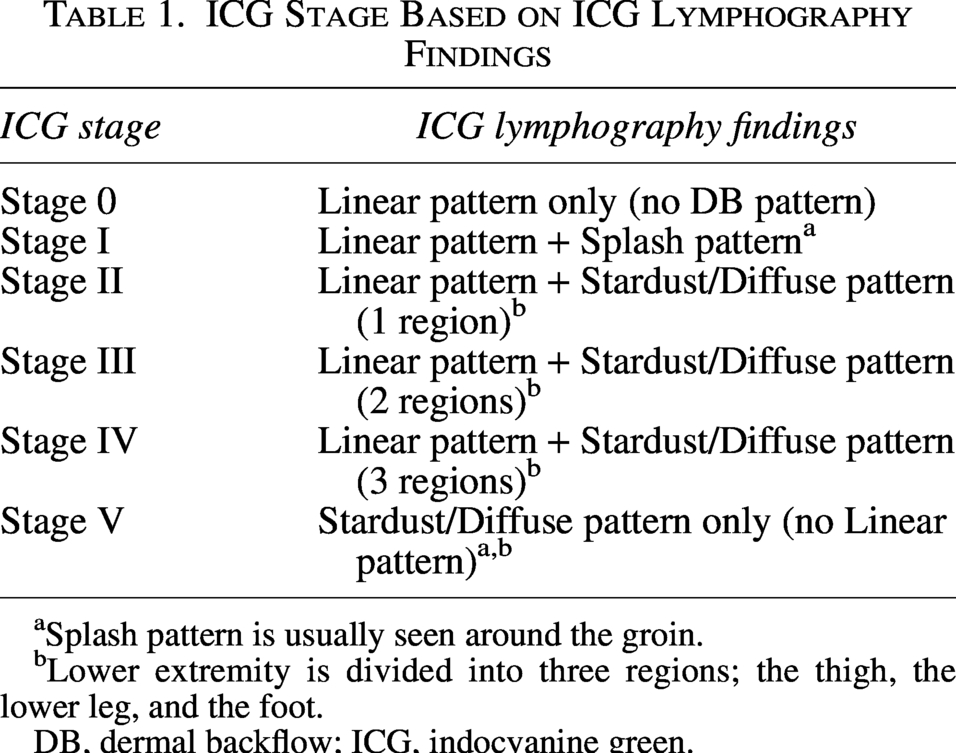
Splash pattern is usually seen around the groin.
Lower extremity is divided into three regions; the thigh, the lower leg, and the foot.
DB, dermal backflow; ICG, indocyanine green.
Gluteal ICG lymphography was performed with intradermal ICG injections. 0.1 mL of ICG (0.25% Diagnogreen; Daiicglutealharmaceutical, Tokyo, Japan) was injected intra-dermally at five points; the tip of the coccygeal bone, the gluteal fold, the crosspoint connecting those points and the mid-lateral thigh, and midpoints of them in a prone position and named H1–H5 from medial to lateral (Fig. 1). As previously described, the posterior trunk watershed is generally verified as the centerline, and the watershed of the thigh is the lateral midline.13–15 Therefore, ICG was injected into their connecting line. Immediately after ICG injection, the linear pattern was marked using a near-infrared camera (Photodynamic Eye-neo; Hamamatsu Photonics, Hamamatsu, Japan). At a plateau phase, ICG lymphography findings were evaluated, and limbs showing dermal backflow patterns were excluded from the anatomical evaluation of the gluteal lymphatic pathways. The directions of the gluteal lymphatic pathways from each point were evaluated by observing real-time lymphographic images.
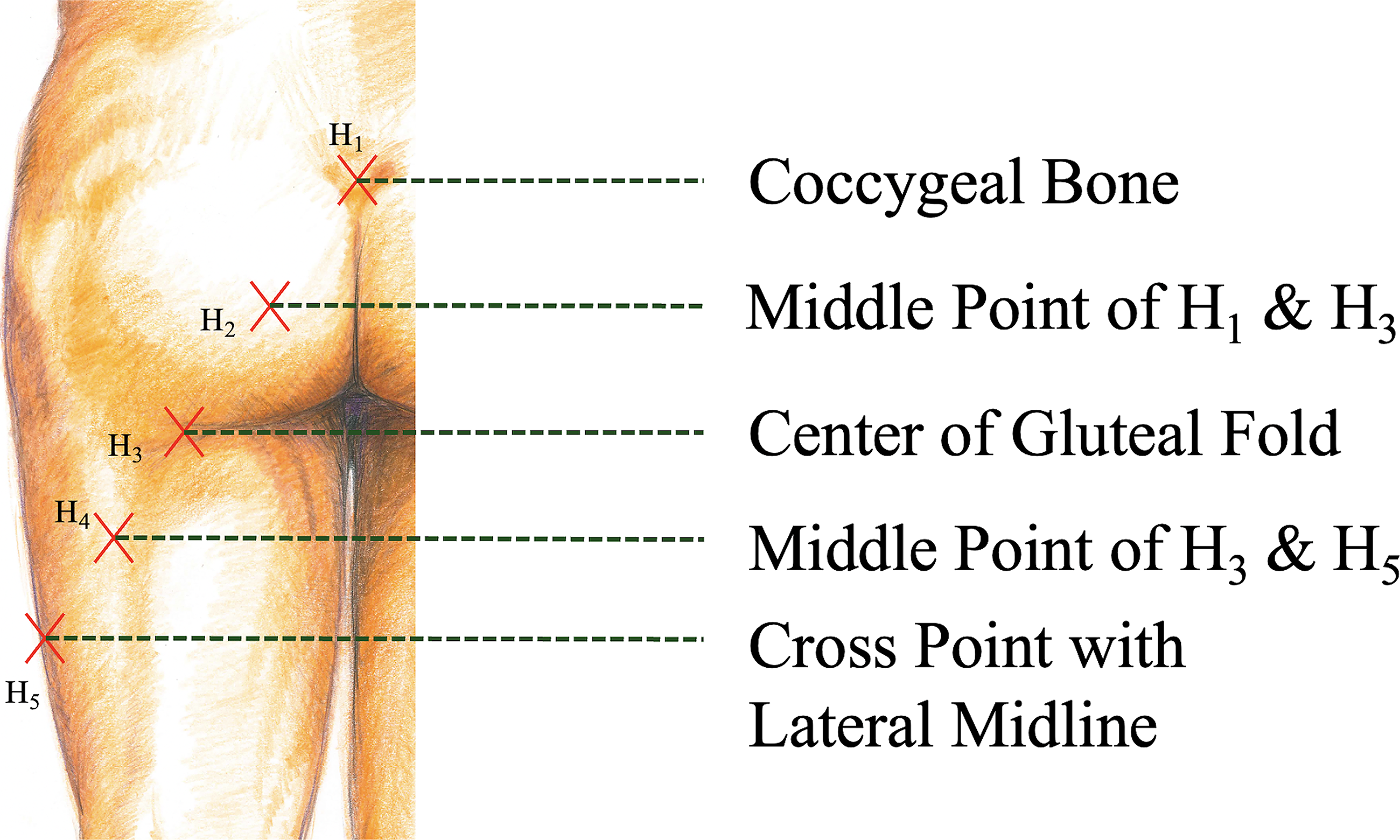
0.1 mL of ICG was injected intra-dermally at five points; the tip of the coccygeal bone, the gluteal fold, the crosspoint connecting those points and mid-lateral thigh, and midpoints of them in a prone position and named H1 to H5 from medial to lateral.
Clinical data were obtained, including sex, age, body mass index (BMI), cancer etiology, cancer treatments, and ICG lymphography findings. Based on ICG lymphography findings, the posteromedial and posterolateral pathway directions of collecting lymph vessels, shown as linear patterns, from each point at the gluteal were investigated (Fig. 2). This retrospective observational study was approved by the institution’s ethical review board (approval number NCGM-G-004179-00).
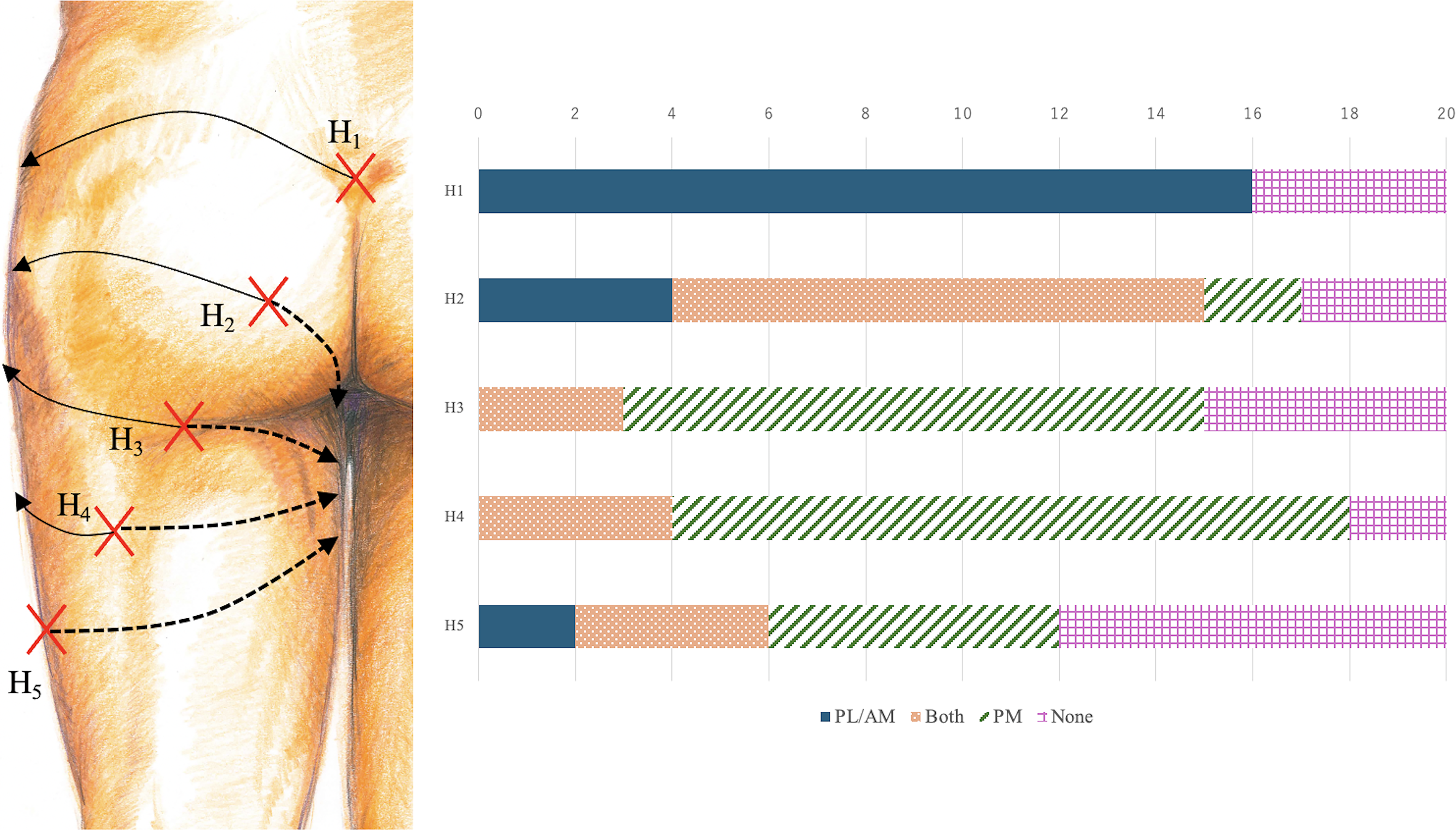
Based on ICG lymphography findings, the posteromedial and posterolateral/ anteromedial pathway directions of collecting lymph vessels, shown as linear patterns, were investigated from each gluteal point. The lymphatic pathways from each point were also visualized. PL, Posterolateral pathway. PM, posteromedial pathway. AM, anteromedial pathway.
Results
A total of 20 limbs of 15 cancer survivors (14 female and 1 male) were included; 10 patients suffered from unilateral LEL, and the contralateral limbs were unaffected, and bilateral limbs were unaffected in 5 patients. Age ranged from 38 to 79 years (average, 52.2 years), and BMI ranged from 17.1 to 34.9 kg/m2 (average, 23.8 kg/m2). Cancer etiology included uterine cervical carcinoma in eight cases, uterine corpus carcinoma in six cases, ovarian cancer and prostatic carcinoma in one case each. One case had double cancer; uterine corpus carcinoma and ovarian cancer. Cancer treatments included pelvic lymph node dissection in 14 cases, pelvic irradiation in 3 cases, and chemotherapy in 7 cases (Table 2).
Patient Characteristics
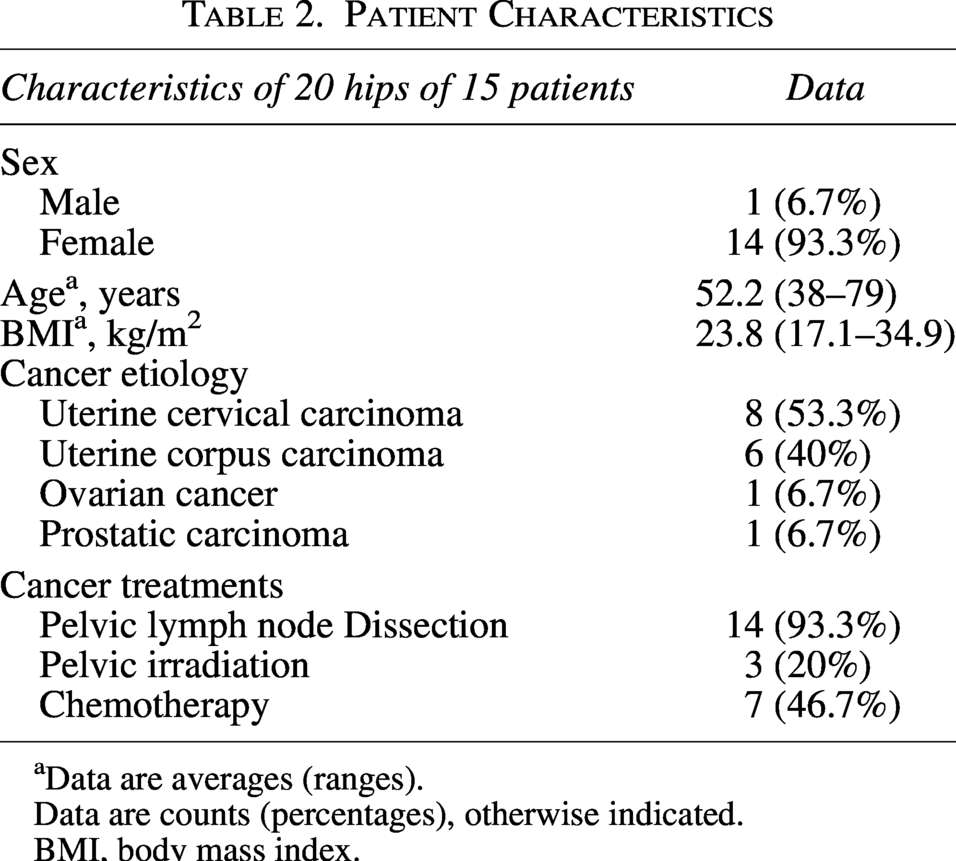
Data are averages (ranges).
Data are counts (percentages), otherwise indicated.
BMI, body mass index.
The posterolateral pattern lymphatic pathway from the H1 was observed in 16 (80%) limbs. The lymphatic pathways from the H2 were posteromedial patterns in 13 (65%) limbs and posterolateral patterns in 15 (75%) limbs; both patterns were identified in 11 (55%) limbs and no pattern in 3 (15%) limbs. The lymphatic pathways from the H3 were posteromedial patterns in 15 (75%) limbs and posterolateral patterns in 3 (15%) limbs; both patterns were identified in 3 (15%) limbs, and no pattern in 5 (25%) limbs. The lymphatic pathways from the H4 were posteromedial patterns in 18 (90%) limbs and posterolateral patterns in 4 (20%) limbs; both patterns were identified in 4 (20%) limbs, and no pattern in 2 (10%) limbs. The lymphatic pathways from the H5 were posteromedial patterns in 10 (50%) limbs and anteromedial patterns in 6 (30%) limbs; both patterns were identified in 4 (20%) limbs and no pattern in 8 (40%) limbs (Fig. 2) (Table 3).
Lymphatic Pathways from Each Point of Each Case
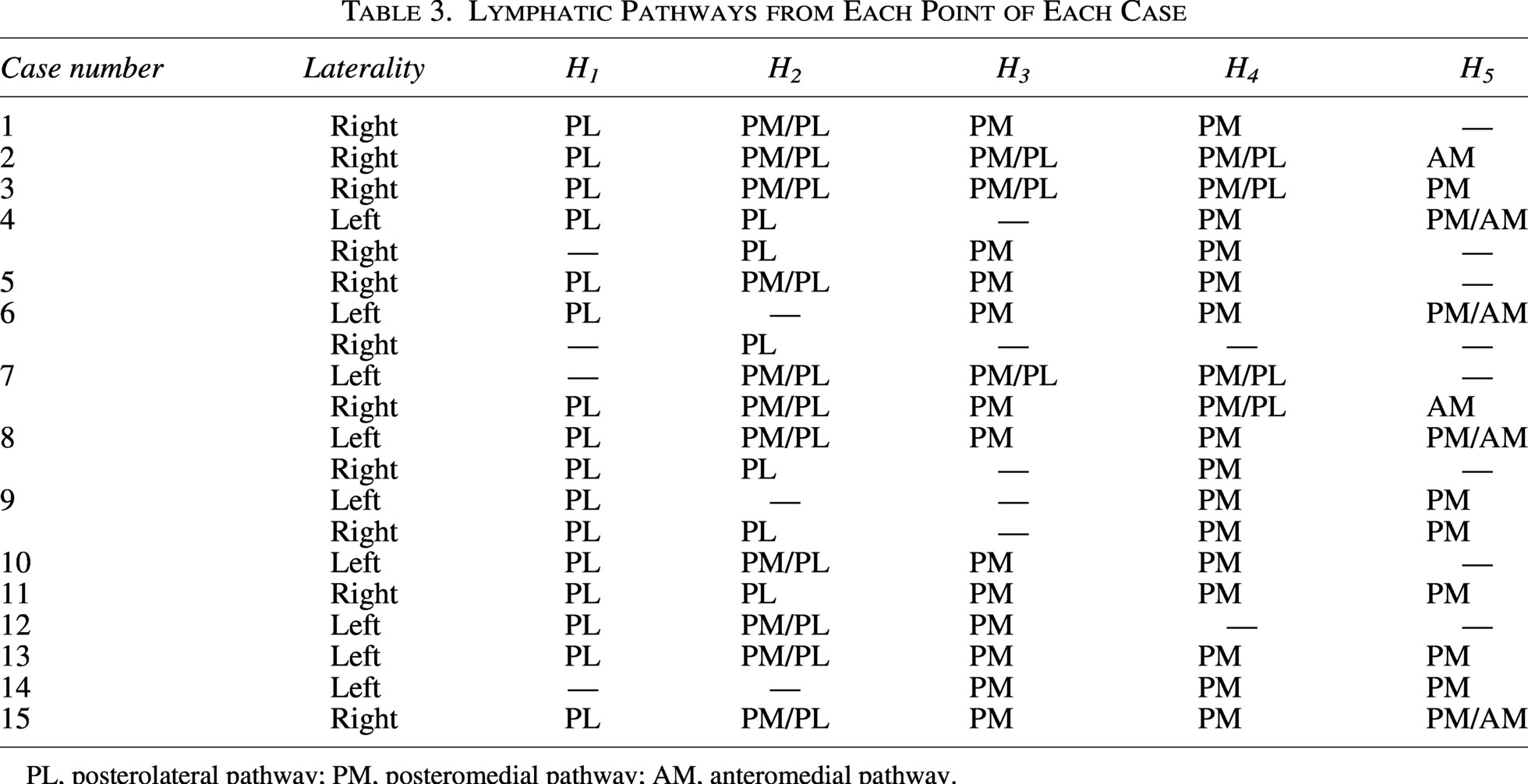
PL, posterolateral pathway; PM, posteromedial pathway; AM, anteromedial pathway.
Discussion
The watershed line of collecting lymph vessels in the back is the center line, which is well known and described in several literature.16,17 Additionally, the watershed line of collecting lymph vessels in the thigh is the mid-lateral line, which was revealed recently.13–15 Therefore, this study revealed the real watershed line of the collecting lymphatic vessels in the gluteal, back, and thigh particularly. Firstly, the back watershed line is the center line, extending until the coccygeal bone’s tip (H1). Meanwhile, the watershed line in the thigh is the mid-lateral line from the caudal side under the H5. Moreover, in the gluteal, H2 is the real watershed point because posteromedial and posterolateral patterns were well-balanced, and both patterns were identified in over half of the cases. From the same perspective, posteromedial patterns were dominant in H3 and H4. Therefore, the real watershed line of the gluteal is followed from H1 to H2, and laterally goes through in the middle of the gluteal to H5; mid-lateral thigh (Fig. 3).
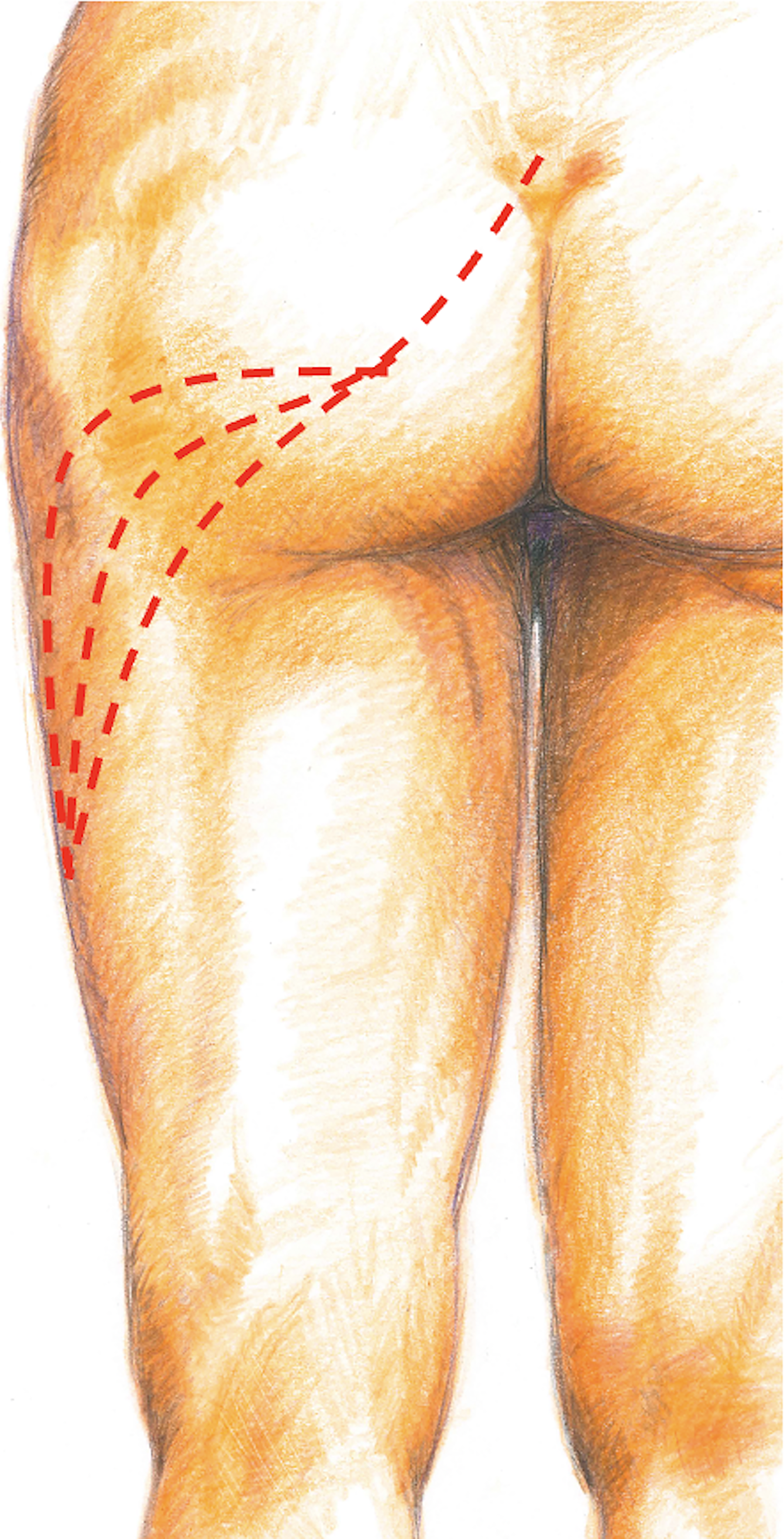
The real watershed line of the gluteal is followed from H1 to H2, and laterally goes through in the middle of the gluteal to H5. Three potential watershed lines are indicated with red dotted lines.
Considering the reason for no linear patterns in about 20% of cases at each point, there would be some connections with deep lymphatic systems via perforating lymphatic vessels because there is much fat in the hip. Suami et al. suggest that there would be some connections between superficial collecting lymphatic systems and deep lymphatic systems; perforating lymphatic vessels, in the gluteal and posterior thigh. 7 We also previously reported that there are over half of the cases which have some connections between them in the lower extremity. 21 Hence, no linear patterns from the injection point mean that there are some dominant perforating lymphatic vessels to the deep lymphatic systems rather than superficial collecting lymphatic systems.
In ICG lymphography, the selection of an appropriate injection site is critical. However, for minor lymphosomes excluding the major lymphosome located in the medial aspect of the lower limb, the optimal injection site has not yet been clearly established. Therefore, in clinical practice, ICG is often injected into a site that is considered “most appropriate” for each individual case. Ideally, the injection should be performed at the most peripheral region, such as the interdigital spaces, or at the anatomical watershed described in textbooks and previous studies, which enables visualization of the entire lymphosome. In particular, injection at the watershed is advantageous because it allows simultaneous visualization of the two lymphosomes that share the boundary, thereby reducing the number of injections required. Conversely, when two lymphosomes are not simultaneously visualized from a presumed watershed injection, likely that the site is not a true watershed. Thus, in clinical settings, injection sites are adjusted during ICG lymphography. The injection sites determined from our experience with ICG lymphography to represent the presumed gluteal watershed demonstrated visualization of two distinct lymphosomes in most cases. Accordingly, these sites were deemed valid as the “true” gluteal watershed.
The result of this study can be applied to several examinations or treatments. First, as already described previously, gluteal lymphedema affects the thickening of the dermal and subcutaneous tissue of the lymphedema-side hip, it causes the gluteal height difference to the contralateral side and discomfort in spine position and sitting position and also causes lower back pain because of the continued inclination.5,6 The gluteal lymphatic pathways can be addressed with MLD or LVA to improve these symptoms due to gluteal lymphedema. This is particularly important for MLD8–10 because the watershed and the direction of gluteal lymphatic pathways are not well-known in most previous studies and textbooks.16,17 Based on the results, procedures of MLD in the hip should be revised; massage should be done from the middle line of the hip toward the inguinal lymph nodes in oblique infero-medial and supero-lateral directions through the superior gluteal area. Meanwhile, in the inferior gluteal area, massage should be done mainly in the infero-medial direction. Additionally, in the lymphedema limbs, the watershed shifts to the dermal backflow side; the dermal backflow of the buttock is usually the lateral side in the authors’ experience, so the watershed shifts to the lateral side. Hence, in the cases of lymphedema, ICG should be injected more lateral side of the line that is suggested in this study, the unaffected limb watershed line.
Second, trauma or tumor resection in the hip may cause gluteal lymphedema, but cannot be diagnosed with conventional ICG lymphography or lymphoscintigraphy, because they show intact major lymphatic pathways.22–24 Therefore, after trauma or tumor resection, periodic ICG lymphography in the gluteal area with injections of the watershed line is for preventing and early diagnosing gluteal lymphedema.
Third, some flaps are often harvested from the gluteal region for breast and other soft tissue reconstructions; superior gluteal artery perforator (SGAP) flap and inferior gluteal artery perforator (IGAP) flap.25–28 However, Martineau et al. reported that free SGAP flap postoperative donor site seroma rate was 2–35% in their meta-analysis study 26 whereas they also described that free IGAP flap donor site seroma rate was 9% in their meta-analysis study. 28 Those rates of donor site seroma are commonly higher than deep inferior epigastric perforator flap.25–28 Although many factors should be considered, it would be possible to create a lower rate of donor site seroma with the gluteal watershed line concept because some papers already proved that collecting lymphatic vessels around the watershed line are the union of short, narrow precollectors.29,30 In this concept, the major axis of the flap should follow the watershed line both in SGAP and IGAP flaps.
Limitations of this study include the small number of cases of only Japanese cancer survivors with relatively low BMI. The results may not be applied in other ethnic groups, and the anatomical location of the gluteal watershed line of collecting lymphatic pathways may be different in obese cases. Furthermore, almost all the participants were female, so that male anatomy may differ, especially given the differences in fat distribution by sex. Moreover, although only ICG stage0 cases were included in this study, there is a possibility of including the potential lymphedema cases of keeping the clinical non-lymphedema condition, which means that although lymphatic pressure at some points would be high temporally, collateral lymphatic pathways work and keep ICG stage as intact. Therefore, an anatomical study involving healthy volunteers would be necessary to investigate more definitive conclusions.
Although further studies with volunteers are required to elucidate the comprehensive lymphatic anatomy of the hip and to confirm the clinical usefulness of the elucidated anatomy in gluteal lymphedema treatment with MLD or LVA, the results of this study would be useful for gluteal lymphedema treatment.
Conclusion
Multiple ICG injections enhanced the watershed line of collecting lymphatic vessels in the gluteal region, which has never been clarified. The results would be useful for gluteal lymphedema diagnosis and treatment.