
Abstract
Baquerizo-Sedano, Luis, José Augusto Chaquila, Juan Pablo Aparco, Carlos Torres Salinas, Orison O. Woolcott, and Pedro González-Muniesa. Extreme variability of anemia prevalence in peruvian children based on different altitude correction factors: A cross-sectional study. High Alt Med Biol. 26:374–381, 2025.
Objetives:
Higher erythrocytosis is the main hematological adaptation to altitude. Consequently, several correction factors have been proposed to diagnose anemia in children at high altitude. We compared the anemia prevalence in Peruvian children aged 6–59 months living at different altitudes according to several published correction factors to adjust hemoglobin for altitude.
Methods:
Data were collected from 578,576 children in the Nutritional Surveillance System in Peru in 2020. Anemia prevalence was estimated by altitude every 1,000 m, using four different adjustment criteria, including the recent adjustment proposal from the World Health Organization.
Results:
The total prevalence of anemia varied substantially (from 3.2% to 33.7%) depending on the adjustment criteria used. Without correction factors, the highest proportion of anemia was observed in the lowest altitude range. However, this result was no longer observed when the adjustment factors were used. For ranges above 3,000 m, moderate anemia occurred with a higher prevalence when using two different correction factors but not others or without adjustment.
Conclusions:
Our findings reveal substantial changes in anemia prevalence among Peruvian children under 5 years of age depending on the adjustment factors for hemoglobin used. More research is needed to properly diagnose anemia in children at high elevations.
Introduction
Anemia, the condition in which the body fails to produce enough red blood cells or when these cells are impaired to transport oxygen to tissues, represents a global public health problem (Gardner et al., 2023). In Latin America, infants represent a higher risk of anemia due to health disparities compared with the general population (Rosas-Jiménez et al., 2022). The prevalence of childhood (under 3 years old) anemia in Peru has continued to rise over the last 4 years, increasing by 3.7 percentage points (from 40% in 2020 to 43.7% in 2024) (Instituto Nacional de Estadística e Informática, 2024). Recently, the Peruvian government has published a new Supreme Decree for the prevention and reduction of anemia for the period 2024–2030 (Ministerio de Salud, 2024).
Studies have shown that low partial pressure of oxygen at high altitude causes a certain degree of hypoxia that triggers adaptive mechanisms to facilitate the use of oxygen in individuals born at high altitude (Hurtado et al., 2014; Webb et al., 2021). The higher production of red blood cells is the main hematological adaptation to altitude (Webb et al., 2021). For this reason, researchers have suggested the need for correction factors to better estimate hemoglobin concentrations at high altitude (Le, 2016).
The cut-off points for defining anemia vary according to sex and age (World Health Organization, 2017). The need for adjustment due to altitude has been proposed by several researchers (Aparco et al., 2023; Centers for Disease Control, 1989; Dirren et al., 1994; Sharma et al., 2019), and more recently the WHO published a report with an adjustment formula for altitude of residence, applicable from 500 m. (World Health Organization, 2024) Since 2001, WHO has adopted an altitude adjustment factor for altitudes from 1,000 m (UNICEF., University UN and Organization WH, 2001). However, the variation in the results obtained by different authors when trying to determine the prevalence of anemia in certain populations could be due to the fact that for the construction of the adjustment factors, variables such as genetic adaptation, residence time at high altitudes, and other hematological variables were not considered (Gassmann et al., 2019; Gonzales et al., 2018; Simonson et al., 2010).
Because of these discrepancies, some authors have proposed their own criteria and adjustment models. Ocas-Córdova et al. proposed a threshold of 2 standard deviations (SDs) below the mean hemoglobin of the altitude range to diagnose anemia (Ocas-Córdova et al., 2018). Sharma et al. proposed an adjustment with a more physiological approach model based on several biomarkers, such as retinol and serum ferritin (Sharma et al., 2019). The Ocas-Cordova diagnostic criterion and the adjustment proposed by Sharma suggest that the increase of hemoglobin against hypoxic environment should not be generalized and, therefore, the proposed correction factor for anemia should not be applicable to certain populations.
To date, no previous study has compared the influence on the prevalence of childhood anemia when using different published factors to adjust hemoglobin for altitude. Thus, the objective of the present study was to compare the prevalence of anemia in Peruvian children from 6 to 59 months of age living at different altitudes according to several published factors to adjust hemoglobin for altitude and diagnostic criteria for anemia.
Materials and Methods
Data sources
We used the open database of the annual Nutritional Status Information System for Children and Pregnant Women (SIEN) from the National Institute of Health of Perú (INS). SIEN is a continuous and systematic system that records, processes, reports, and analyzes information on the nutritional status of children under 5 years of age and pregnant mothers who attend public health facilities. SIEN covers the entire national territory and includes 8,032 health centers in 32 DIRESAS (Regional Health Directorate) that direct, implement, and evaluate the Integrated Health Care Policies in conditions of quality and timeliness of the Peruvian Ministry of Health. The SIEN database has been used in previous publications for spatial analyses of childhood anemia (Hernández-Vásquez et al., 2019) in Peru and can be accessed on the national open data platform: https://www.datosabiertos.gob.pe/dataset/sien-sistema-de-Znformaci%C3%B3n-del-estado-nutricional-de-ni%C3%B1os-y-gestantes-per%C3%BA-inscenan.
The data reported by the SIEN are obtained during medical appointments in all public health services according to the “Growth and Development program” and contain data from 578,576 children between 6 and 59 months in 2020 with data on sex, department (administrative division used in Peru), population, hemoglobin, weight, length, and altitude. The hemoglobin levels (g/dl) were obtained by blood test using a portable HemoCue, and the protocols followed the official technical guide of the Ministry of Health of Peru (Ministerio de Salud, 1997). To obtain information only for children aged 6–59 months, all data for those aged 60 months were excluded (N = 1,640).
Hemoglobin adjustments for altitude
The altitude above sea level corresponded to the location of the health establishment where the child was examined and is expressed in meters, and the result of the formula is subtracted from the observed hemoglobin value. The Centers for Disease Control (CDC) correction factor uses the following criteria: (Adjusted Hb)(g/dl) = −0.032*(altitude*0.0033) + 0.022*(altitude*0.0033)2 (CDC, 1989). Sharma’s proposed fit corresponds to the following formula: (0.0048108*altitude) + (0.0000004*altitude2) (Sharma et al., 2019). The recent WHO proposal presents the following linear model: (Adjustment Hb)(g/l) = (0.0056384*altitude) + (0.0000003*altitude2). In contrast to the previous WHO proposal, the hemoglobin adjustment starts from 500 meters (World Health Organization, 2024). Ocas-Córdova uses as diagnostic criteria for anemia a threshold of hemoglobin based on −2 SDs of the mean with respect to altitude range (<999; 1,000–1,999; 2,000–2,999; 3,000–3,999; ≥4,000). Because the Ocas-Cordova proposal did not originally contemplate anemia severity criteria, these subclassifications were not made.
For this new WHO proposal, the anemia threshold changes with respect to age only for the 0–23 months group: ≥10.5 g/dl. For children aged 24–59, it remains at 11 g/dl. Based on the model proposed by WHO in 2001, only a threshold of 11 g/dl was used without correction for the determination of anemia (Sharma et al., 2019). Except for Ocas-Córdova et al. and for children from 6 to 23 months, according to the new WHO proposal, the threshold of 11 g/dl will be used as the criterion for detecting anemia (Supplementary Table S1). In addition, the severity of anemia prevalence in all but the new WHO proposal was classified according to the Peruvian Ministry of Health, which adopted the WHO guidelines: mild (10.00–10.99 g/dl), moderate (7–9.99 g/dl), and severe (<7 g/dl) (Vitamin and Mineral Nutrition Information System, 2011). In the same way as the diagnostic criteria for children under 23 months according to the new WHO proposal, the classification of anemia severity was different: mild (10.4–9.5 g/dl), moderate (9.4–7 g/dl), and severe (<7 g/dl) (World Health Organization, 2024).
Statistical analysis
The prevalence of anemia was expressed according to regions, severity of anemia, and age ranges for the five altitude levels (≤999, 1,000–1,999, 2,000–2,999, 3,000–3,999, ≥4,000). To assess statistically significant differences in anemia prevalence according to hemoglobin adjustment methods and diagnostic criteria, two-sample tests of proportions were used, with a significance level set at p < 0.05. All p-values were adjusted for multiple comparisons using the Bonferroni correction. A filled map of Peru was drawn up to observe the prevalence of anemia according to the different criteria and adjustment factors. In addition, a bar chart was prepared for the severity of anemia according to age range (6–11, 12–23, 24–35, 36–47, and 48–59 months). The graphics were generated using the Microsoft Excel program. Statistical analysis was performed using the statistical package STATA version 16.0, Texas.
Ethical issues
This study did not require the approval of an ethics committee because an open database was used, and no identification of the participants was obtained.
Results
The final data included 576,936 children. The characteristics of the population are shown in Supplementary Table S2. The largest population of children was between 12 and 24 months (31.22%). Low-altitude departments, such as Callao and Tumbes, accounted for 2.45% and 1.12% of the population studied, respectively, and the departments with higher altitudes had a population level of 4.59% (Cusco), 1.41% (Huancavelica), and 3.45% (Puno). The most populated departments were Lima (23.92%), Piura (8.96%), La Libertad (6.54%), and Cajamarca (5.80%). The least populated were Moquegua (0.49%), Madre de Dios (0.61%), Pasco (0.98%), and Tacna (1.02%).
The prevalence of anemia in children between 6 and 59 months is shown in Table 1 with altitude ranges between 0 and more than 4,000 m and, according to the WHO, without hemoglobin correction and the three proposed correction criteria (Centers for Disease Control, 1989; Ocas-Córdova et al., 2018; Sharma et al., 2019). Without hemoglobin adjustment for altitude, the highest proportion of anemia was in the lower altitude range; however, this was not observed when using correction factors. The Ocas-Córdova criteria showed the lowest prevalence in all altitude ranges; regarding adjustments, Sharma had the highest prevalence in the ≤999, 1,000–1,999, and 2,000–2,999 ranges, and CDC had the highest prevalence in the 3,000–3,999 and ≥4,000 ranges. Overall, considering adjustment factors, Sharma had the highest prevalence (33.72%), and WHO, 2024 the lowest (23.12%). When comparing proportions, we did not find significant differences between the prevalences according to Sharma and WHO 2024 at altitudes above ≥4,000 meters. In addition, Ocas-Córdova shows fewer significant differences across altitude ranges.
Prevalence of Anemia in Peruvian Children Aged 6–59 Months at Different Altitudes
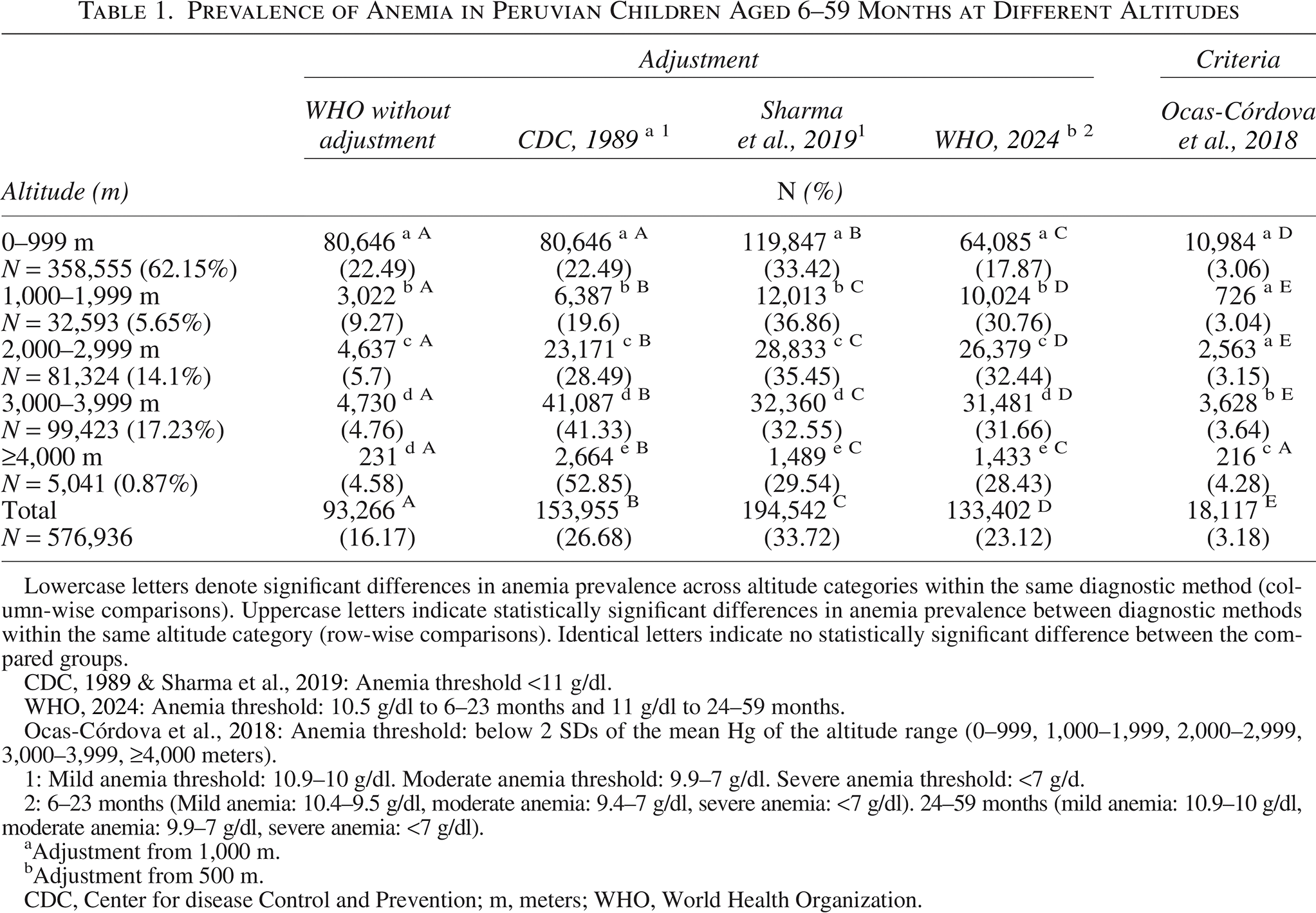
Lowercase letters denote significant differences in anemia prevalence across altitude categories within the same diagnostic method (column-wise comparisons). Uppercase letters indicate statistically significant differences in anemia prevalence between diagnostic methods within the same altitude category (row-wise comparisons). Identical letters indicate no statistically significant difference between the compared groups.
WHO, 2024: Anemia threshold: 10.5 g/dl to 6–23 months and 11 g/dl to 24–59 months.
Ocas-Córdova et al., 2018: Anemia threshold: below 2 SDs of the mean Hg of the altitude range (0–999, 1,000–1,999, 2,000–2,999, 3,000–3,999, ≥4,000 meters).
1: Mild anemia threshold: 10.9–10 g/dl. Moderate anemia threshold: 9.9–7 g/dl. Severe anemia threshold: <7 g/d.
2: 6–23 months (Mild anemia: 10.4–9.5 g/dl, moderate anemia: 9.4–7 g/dl, severe anemia: <7 g/dl). 24–59 months (mild anemia: 10.9–10 g/dl, moderate anemia: 9.9–7 g/dl, severe anemia: <7 g/dl).
Adjustment from 1,000 m.
Adjustment from 500 m.
CDC, Center for disease Control and Prevention; m, meters; WHO, World Health Organization.
When prevalence was categorized according to the severity of anemia in the lower range of altitude, mild anemia was more frequent; the same result was found in the ranges 1,000–2,000 and 2,000–3,000. For ranges above 3,000 m, a higher prevalence of moderate anemia was observed when using the CDC and Sharma et al. correction factors. In addition, the prevalence of severe anemia was similar across nearly all adjustment formulas. (Table 2).
Prevalence of Mild, Moderate, and Severe Anemia in Peruvian Children Aged 6–59 Months at Different Altitudes
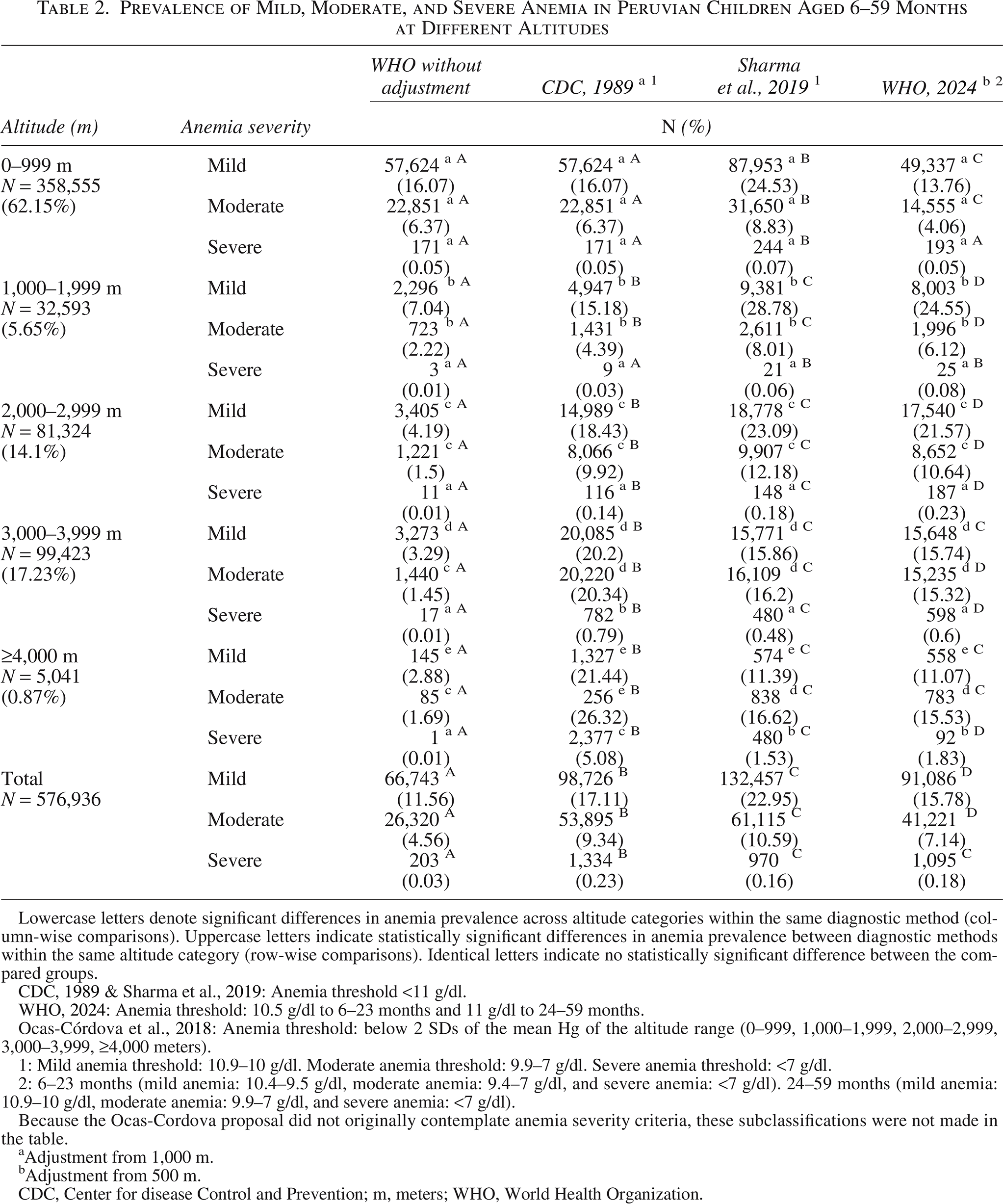
Lowercase letters denote significant differences in anemia prevalence across altitude categories within the same diagnostic method (column-wise comparisons). Uppercase letters indicate statistically significant differences in anemia prevalence between diagnostic methods within the same altitude category (row-wise comparisons). Identical letters indicate no statistically significant difference between the compared groups.
WHO, 2024: Anemia threshold: 10.5 g/dl to 6–23 months and 11 g/dl to 24–59 months.
Ocas-Córdova et al., 2018: Anemia threshold: below 2 SDs of the mean Hg of the altitude range (0–999, 1,000–1,999, 2,000–2,999, 3,000–3,999, ≥4,000 meters).
1: Mild anemia threshold: 10.9–10 g/dl. Moderate anemia threshold: 9.9–7 g/dl. Severe anemia threshold: <7 g/dl.
2: 6–23 months (mild anemia: 10.4–9.5 g/dl, moderate anemia: 9.4–7 g/dl, and severe anemia: <7 g/dl). 24–59 months (mild anemia: 10.9–10 g/dl, moderate anemia: 9.9–7 g/dl, and severe anemia: <7 g/dl).
Because the Ocas-Cordova proposal did not originally contemplate anemia severity criteria, these subclassifications were not made in the table.
Adjustment from 1,000 m.
Adjustment from 500 m.
CDC, Center for disease Control and Prevention; m, meters; WHO, World Health Organization.
Figure 1 shows the prevalence of anemia by department using the classification recommended by the WHO: mild (<20% anemia), moderate (20%–39.9%), and high (>40%). An evident change can be observed when using different correction factors.
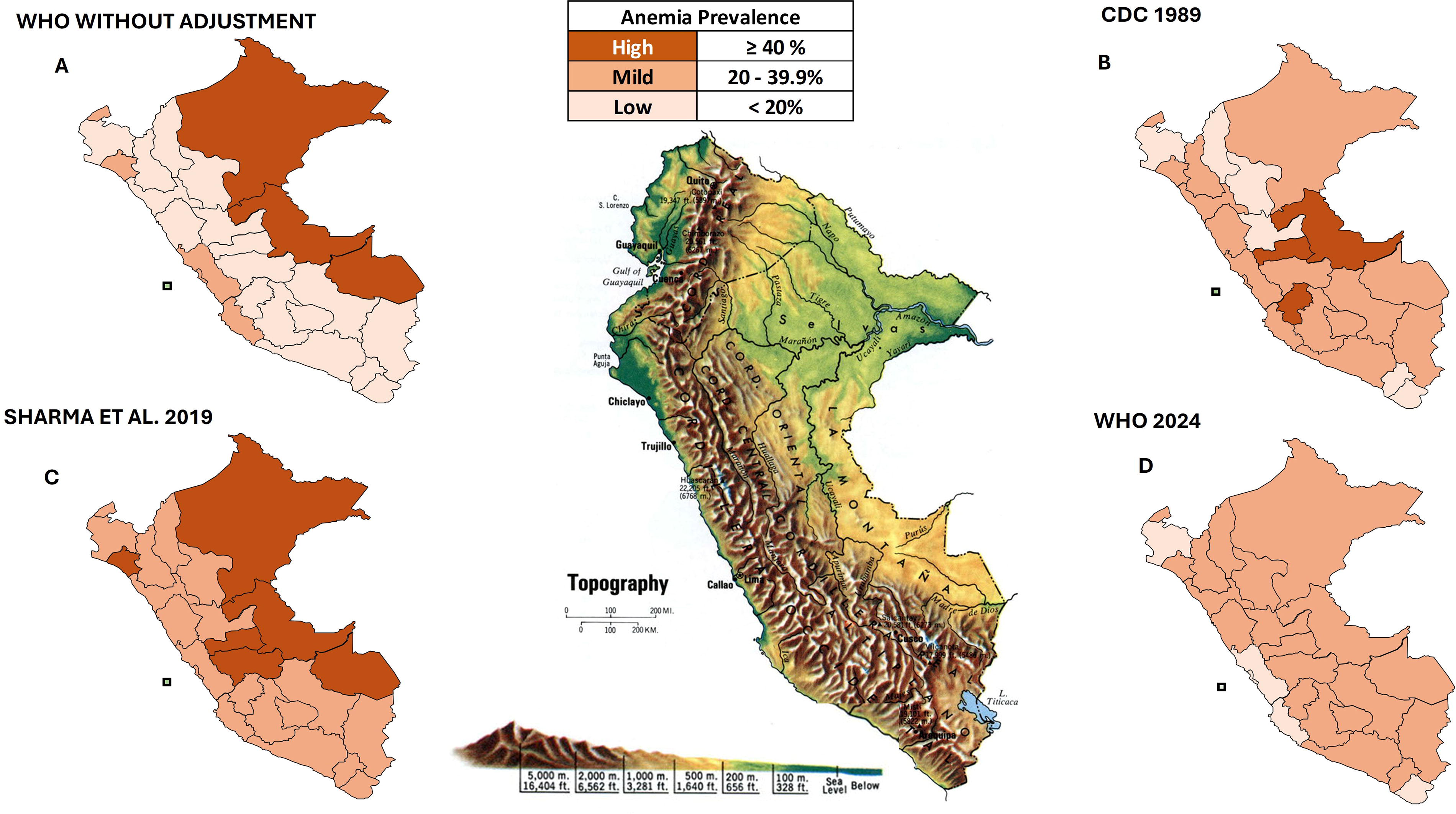
Anemia prevalence classification by department according to four criteria. Prevalence estimates included all cases, regardless of the severity of anemia. The topographic map in the center displays the altitude according to the geography of Peru.
Analysis by age ranges (Fig. 2) shows an inverse association between anemia prevalence and age when using different adjusting criteria except when the WHO, 2024 adjustment is used. This can be attributed to the lowering of the cut-off point for diagnosis in children under 2 years of age, which no longer considers children with hemoglobin between 10.5 and 11 g/dl to be anemic.
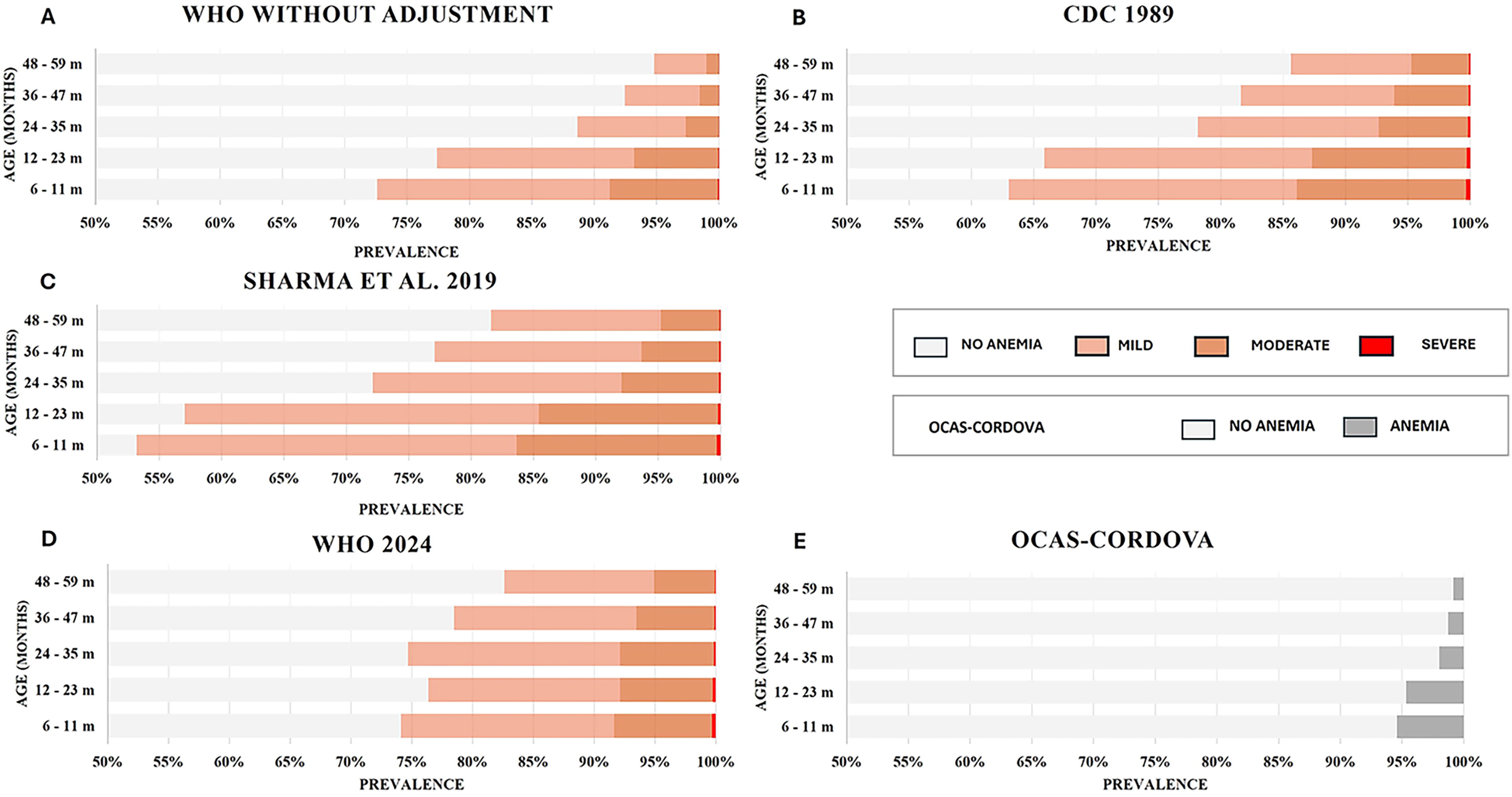
Anemia prevalence by age, with 12-month ranges. For the adjustment factors
Discussion
Our study compared the prevalence of childhood anemia using three adjustment factors and one diagnosis criteria for altitude in the children Peruvian population. Our findings in a large sample of Peruvian children aged 6–59 months clearly show that the prevalence of anemia changes substantially when using different hemoglobin adjustment criteria for altitude. Considering that 500.3 million humans live at ≥1,500 m, 81.6 million at ≥2,500 m, and 14.4 million at ≥3,500 m (Tremblay and Ainslie, 2021), an accurate diagnosis of anemia is essential to tackle this public health problem.
National public health policies have considered childhood anemia based on the high prevalence of anemia using the correction factor provided by the CDC. In 2023, the highest prevalence was found in cities at higher altitudes such as Puno (67.2%, ∼3,800 m) and Huancavelica (65%, ∼3,600 m), although also in cities located in the Amazon, including Ucayali (65.8%, ∼200 m) and Loreto (63.1%, ∼130 m (Instituto Nacional de Estadística e Informática, 2023). These variations in the prevalence of anemia may be due to multiple factors, including socioeconomic differences and access to health care in these departments, although no relationship was found between anemia with poverty levels or with the vulnerability to the food insecurity index (Ministerio de Desarrollo e Inclusión social, 2021).
Furthermore, it is speculated that the decrease in the prevalence of anemia with age could be attributed to the natural maturation of the organism, especially at the level of the immune system (Simon et al., 2015), which would lead to a lower incidence of gastrointestinal and respiratory infectious diseases.
Other researchers have suggested alternative adjustment formulas or criteria, and when these are compared with those of the CDC, they yield different prevalence rates. (Accinelli and Leon-Abarca, 2020; Bartolo-Marchena et al., 2017). Our results show differences in the prevalence of childhood anemia when comparing three adjustment factors and a diagnose criterion for anemia. We also showed the prevalence of anemia among Peruvian children when using the adjustment factor proposed by Sharma et al. In addition, we show that the prevalence of severe anemia triples when using the CDC adjustment factor compared with the hemoglobin adjustment for altitude proposed by Sharma et al.
By using the correction factor proposed by Ocas-Córdova et al., we obtained markedly lower percentages of anemia compared with the other criteria, likely due to the very conservative criteria for the diagnosis of anemia. Moreover, the authors’ proposal was only based on hemoglobin level without analyzing other biomarkers of iron status or if the population was healthy (Ocas-Córdova et al., 2018). In Puno, children aged 6–24 months presented high serum ferritin levels with a mean unadjusted hemoglobin of 11–14.5 g/dl. These ferritin levels were higher compared with those children with mean hemoglobin levels of 10–10.9 g/dl (Gonzales et al., 2018). When adjusting hemoglobin for altitude, those with high ferritin levels were categorized as having mild anemia, whereas those with normal serum ferritin were categorized as having moderate anemia (Gonzales et al., 2018). However, a more recent study in children found low iron reserves in the higher altitude regions (Cusco and Puno) (Aparco et al., 2023).
In the altitude ranges starting from 1,000 m, the prevalence of anemia as proposed by Sharma et al. presents a plateau of approximately 30%; its formula presents a mean linear adjustment of 0.095 g/dl (<1,000 m), 0.820 g/dl (>1,000 m), 1.515 g/dl (>2,000 m), 2.116 g/dl (>3,000 m), and 2.745 g/dl (>4,000 m). These results considered other factors in addition to altitude, such as vitamin A status, iron, and inflammatory markers (C-reactive protein, alpha-1 acid glycoprotein), compared to the CDC adjustment, with a mean linear adjustment of 0.412 g/dl (>1,000 m), 1.346 g/dl (>2,000 m), 2.459 g/dl (>3,000 m), and 3.831 g/dl (>4,000 m). The correction criterion proposed by the CDC is based on an equation developed for children older than 1 year who lived at altitudes below ∼3,300 m, recommending a linear adjustment for altitude (Centers for Disease Control, 1989). However, the proposed linear increase from the use of the formulas might not universally occur due to the role of adaptation time and genotype (Gassmann et al., 2019).
Taking this correction (CDC) into account, given the increase in hemoglobin with age and with a single threshold of 11 g/dl, the prevalence of anemia in children under 1 year of age will probably be higher and will decrease as the child’s age increases (Accinelli and Leon-Abarca, 2020). In addition, one study estimated the change in anemia prevalences in Peru by comparing the CDC factor with the new guidelines, finding an under- and overestimation of anemia with respect to previous guidelines (Campos-Sánchez et al., 2024). In line with this, another study showed a probable overdiagnosis of anemia in two adult populations in Ethiopia (Amhara at 3,700 m and Oromo at 4,000 m) without hemoglobinopathies and considering individuals with full iron stores. When the hemoglobin adjustment factor of the CDC was applied, these two populations passed from having no cases of anemia to having 28.3% for Amhara men and 8.5% for women, and 9.1% for Oromo men and 4.3% for women (Sarna et al., 2018).
The new WHO guidelines will generate important changes in the prevalence of anemia in two ways. The first is the initial altitude for the correction (500 m), which increases the number of people with anemia between 500 and 1,000 m; despite the reduced correction (0.2–0.4 g/dl), it will move those who are at the limit of anemia. The second, in children under 24 months, the prevalence will decrease by lowering the cut-off point to 10.5 g/dl. In countries such as Peru, with a high prevalence of anemia, both changes will result in changes in policies for the care and prevention of childhood anemia. Thus, an important aspect when using adjustment factors is the starting altitude. This number should be implemented taking into account the cascade of signaling controlled by the activity of hypoxia-inducible factors (HIFs) that culminates in the highest production of erythropoietin and iron metabolism (Haase, 2013). The mechanism of regulation of erythrocytosis is very complex (Tang and Wang, 2023), and this is still not fully understood (Villafuerte et al., 2022). In regard to this and the difficulty of human adaptation to very high altitudes, we would like to suggest that one or more mechanisms by which hypoxia stimulates erythrocytosis could have an upper limit and/or the duration of a period in which it would no longer have the initial effect, or even a decrease in its activity considering the various processes at the individual level (Azad et al., 2017) (Hattangadi et al., 2011). More comprehensive and complex studies are required to investigate this topic under chronic hypoxia.
In view of the discrepancies in the prevalence estimates of childhood anemia at the national level, our results raise concern about the need for better criteria for the accurate diagnosis of anemia in children who live at very high altitudes, also considering markers that will allow to know the iron status. Depending on the factor used, underestimations or overestimations can be obtained (Kanu et al., 2023). Our study has some strengths: the large sample of children collected by SIEN allowed us to analyze different altitude levels. In addition, our study included three adjustment factors and one criterion constructed with different methods; the adjustment proposed by Sharma et al. was developed based on biological variables, while the proposed criterion by Ocas-Córdova et al. presents a statistical method for the anemia diagnosis.
Our study has limitations. Health status, except anemia, was unknown. Thus, the inclusion of individuals with pathological conditions may have influenced our estimates. Information on ethnicity was not available; considering that genetics determines the ability to adapt to altitude, it would have been useful. In addition, key biological markers that would have been useful to improve the diagnosis of anemia, such as ferritin, serum iron, or soluble transferrin receptors, were not available for a more accurate comparison.
Conclusions
Our findings provide a current overview of the prevalence of childhood anemia in Peru and how it changes when using different hemoglobin adjustment factors for altitude compared to the conventional adjustment criteria proposed by the CDC. We recommend continuing with the progress of the reevaluation of the cut-off points and new formulas or parameters to better diagnose anemia at high altitudes. The new WHO, 2024 guideline is a good step forward to meet this objective.
Authors’ Contributions
L.B.-S.: Conceptualization, methodology, validation, writing—original draft. J.A.C.: Conceptualization, methodology, formal analysis, data curation, validation, writing—original draft. J.P.-A.: Conceptualization, methodology, validation, writing—review and editing. C.T.S.: Validation, writing—review and editing. O.O.W.: Methodology, writing—review and editing. P.G.-M.: Methodology, validation, writing—review and editing. All authors read and approved the final article.
Footnotes
Author Disclosure Statement
O.O.W.: Works as an editor for The Lancet Group. The other authors declare that they have no conflict of interest.
Funding Information
Physiopathology of Obesity and Nutrition (CIBERobn), Carlos III Health Research Institute (CB12/03/30002) supports P.G.-M.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.