
Abstract
Tu, Ke, Lei Tian, Qi Zhu, Kailian Bai, Lin Li, Mengmei Fu, Mengxia Wang, Lei Zhang, Zhuo Zhan, Haoxi Li, Xiaojun Li, Ruofan Yi, Cheng Jiang, Hua Huang, and Mingming Zhang. Intraoperative opioid-free anesthesia with dexmedetomidine and esketamine versus conventional general anesthesia in laparoscopic cholecystectomy at 3,600 m: a randomized trial on hemodynamic stability and postoperative recovery. High Alt Med Biol. 27:8–16, 2026.
Background:
Opioid-free anesthesia (OFA) is gaining attention as an alternative to opioid-based techniques. However, its hemodynamic and clinical characteristics at high altitudes, where hypoxia and resource limitations prevail, remain unclear.
Methods:
In this single-blind randomized trial, 48 patients undergoing laparoscopic cholecystectomy at 3,600 m were assigned to either a conventional general anesthesia (CGA) group (sevoflurane, sufentanil, remifentanil) or an OFA group (sevoflurane, dexmedetomidine, esketamine). The primary outcome was intraoperative mean arterial pressure (MAP); secondary outcomes included heart rate (HR), awakening time, sedation level, patient satisfaction, postoperative pain, postoperative nausea and vomiting (PONV), perioperative medication use, and adverse events.
Results:
Compared with CGA, the OFA group maintained higher intraoperative MAP, with significant differences after induction (OFA: 87.9 ± 12.3 vs. CGA: 77.2 ± 11.7 mmHg, p < 0.005) and 10 minutes after incision (OFA: 83.5 ± 14.9 vs. CGA: 72.5 ± 9.8 mmHg, p < 0.005). The CGA group exhibited a significant MAP decline at 10 minutes postincision (72.5 ± 9.8 vs. baseline: 83.0 ± 9.1 mmHg, p < 0.001), whereas the OFA group showed a transient MAP increase after intubation (96.1 ± 16.1 vs. baseline: 85.8 ± 7.8 mmHg, p < 0.01). HR trends paralleled MAP changes. Awakening time was significantly longer with OFA (OFA: 20.4 ± 7.5 min vs. CGA: 10.6 ± 8.2 min, p < 0.001), while pain scores at 6 and 12 hours were lower (p < 0.005). Sedation, satisfaction, PONV, and medication use were comparable. No severe adverse events occurred.
Conclusions:
At high altitudes, OFA with dexmedetomidine and esketamine exhibited distinct clinical characteristics compared with opioid-based anesthesia, maintaining blood pressure and postoperative analgesia but less effectively blunting intubation-induced pressor responses and prolonging awakening time. These factors should be weighed when selecting anesthesia strategies in resource-limited, high-altitude settings, particularly when managing large numbers of patients.
Keywords
Introduction
Opioids are integral to conventional general anesthesia (CGA) and play a crucial role in attenuating the stress response to surgical stimuli and maintaining circulatory stability. However, opioids have numerous adverse effects that contribute to problematic long-term use (Colvin et al., 2019), such as postoperative nausea and vomiting (PONV), respiratory depression, pain sensitization, urinary retention, skin pruritus, delirium, and other reactions. These effects are detrimental to patients’ postoperative recovery, leading to prolonged hospital stays, increased patient readmission rates, and increased medical service costs (Esparham et al., 2024; Biancuzzi et al., 2022).
Recently, opioid-free anesthesia (OFA) has emerged as a promising approach. The rationale behind OFA is to avoid the negative impact of intraoperative opioids on patients’ postoperative outcomes and the physiological pathways involved in intraoperative nociception. OFA is based on the concept of multimodal anesthesia (Beloeil, 2019).
Dexmedetomidine, a highly selective α2-adrenoceptor agonist, has sedative, analgesic, and opioid-sparing effects, making it suitable for short- and long-term sedation (Chen et al., 2023). Dexmedetomidine uniquely provides both sedation and analgesia without inducing respiratory depression and is widely used in anesthesia and intensive care (Castillo et al., 2019). Esketamine, the S (+)-isomer of ketamine, has an analgesic effect that is twice that of racemic ketamine. It offers the advantages of a lower incidence of side effects (such as hallucinations), faster recovery, and the ability to lower the minimum alveolar concentration (MAC) of sevoflurane (Lei et al., 2021). Both drugs are currently widely used in multimodal analgesia to reduce opioid consumption.
While several studies have demonstrated the feasibility of OFA in laparoscopic surgery, data on its use in high-altitude hypoxic environments are lacking. High-altitude hypoxic environments can induce physiological changes in multiple systems, including the cardiovascular system (Richalet et al., 2024; Fan et al., 2024). Because of these physiological changes, anesthetics delivered at high altitudes require an understanding of high-altitude medicine, specifically the impact of altitude on anesthesia. Previous studies have shown that the effects of anesthesia and surgery on hemodynamics are distinctly different from those of individuals who live at low altitudes (Zheng et al., 2020).
High-altitude environments induce a range of physiological adaptations, including increased basal sympathetic activity, elevated hemoglobin levels, and altered vascular reactivity (Wani and Sharma, 2017). These changes influence anesthetic drug metabolism and hemodynamic responses, as high-altitude residents often exhibit a blunted vasodilatory response to anesthetic agents and an increased risk of hypotension due to reduced intravascular volume (Siebenmann et al., 2013). In addition to these physiological differences, anesthesia practices at high altitudes face unique logistical challenges, such as shortages of medications, lack of post-anesthesia care units (PACUs), and limited specialized personnel. Under such resource-constrained conditions, maintaining hemodynamic stability and ensuring efficient postoperative recovery become particularly critical. However, there is limited evidence to guide anesthetic management in these settings. Thus, a detailed evaluation of OFA under hypoxic, resource-limited high-altitude conditions is warranted to better understand its advantages and limitations compared to conventional opioid-based anesthesia and to inform optimal anesthetic strategies for high-altitude surgery.
Therefore, the aim of this research was to investigate the hemodynamic and clinical characteristics of OFA using dexmedetomidine combined with esketamine in high-altitude regions and to compare its potential advantages over CGA. Through this research, we sought to provide evidence-based insights to inform anesthetic practice and improve perioperative care in high-altitude, resource-limited regions.
Patients and Methods
Trial design and patients
This was a single-blind parallel-group randomized controlled trial designed to assess OFA using dexmedetomidine combined with esketamine in laparoscopic cholecystectomy in a high-altitude area (at an altitude of 3,600 m). Ethics approval was obtained from the Ethics Committee of the General Hospital of Xizang Military Command (Approval No. of Ethics Committee: 2022XZZYYKY-009). This study was conducted in compliance with the Declaration of Helsinki and registered in the Chinese Clinical Trial Registry (Registration No. ChiCTR2200063948).
Eligible patients met the following criteria: (1) Tibetans who have lived on the plateau for generations, (2) aged 18–60 years, (3) admitted to the hospital with a diagnosis of acute or chronic cholecystitis or gallbladder polyps or gallstones, (4) underwent elective laparoscopic cholecystectomy at the General Hospital of Xizang Military Command between September 2022 and November 2022, (5) had an American Society of Anesthesiologists (ASA) physical status of I or II, and (6) had not left the plateau in the past year.
The exclusion criteria included (1) inability to understand and cooperate with postoperative visit questionnaires, (2) ASA status III or above, (3) pregnancy or lactation, (4) diagnosed with choledocholithiasis or gallbladder cancer, (5) receiving chemotherapy or radiation, (6) long-term use of sedatives or analgesics, (7) allergy to any drug used in the test, (8) history of hypertension or other serious chronic diseases, and (9) severe nausea and vomiting before surgery.
Patients were randomly assigned to either the OFA group or the CGA group. After the initiation of our trial, no amendments were made to the study methodology.
Anesthesia and interventions
Preoperative intramuscular atropine 0.5 mg was given to all patients to prevent an increase in glandular secretions, and intravenous access was established. After the patient entered the operating room, monitoring was initiated for electrocardiography, noninvasive blood pressure, pulse oxygen saturation, end-tidal carbon dioxide, end-tidal sevoflurane concentration, and bispectral index (BIS). Intraoperative BIS values were maintained between 45 and 55 to minimize the risk of intraoperative awareness. Neuromuscular blockade was objectively monitored by electromyography with train-of-four (TOF) stimulation. At the conclusion of surgery, neuromuscular blockade was reversed using intravenous neostigmine (0.04 mg/kg) and atropine (0.02 mg/kg), and extubation was performed only after confirming TOF ratio > 0.9.
The OFA regimen was based on previously reported methods and was appropriately modified according to the specific conditions of our hospital (Massoth et al., 2021; Sakan et al., 2023; Zhou et al., 2024). Patients in the OFA group received dexmedetomidine (0.6 μg/kg) 10 minutes prior to anesthesia induction, followed by esketamine (0.15 mg/kg), propofol (1–2 mg/kg), and cisatracurium besylate (0.15 mg/kg) for induction. Anesthesia was maintained with continuous infusions of dexmedetomidine (0.3 μg/kg/h) and esketamine (0.15 mg/kg/h), along with sevoflurane inhalation adjusted to maintain 1.0–1.2 age-adjusted MAC, as determined by real-time end-tidal concentration monitoring. Intermittent cisatracurium besylate injections ensured muscle relaxation, with additional doses of esketamine (0.15–0.2 mg/kg) and dexmedetomidine (0.3–0.6 μg/kg) before the incision.
In the CGA group, anesthesia induction consisted of sufentanil (0.4 μg/kg), propofol (1–2 mg/kg), and cisatracurium besylate (0.15 mg/kg). Anesthesia was maintained with a continuous infusion of remifentanil (6–18 μg/kg/h) and sevoflurane inhalation adjusted to maintain 1.0–1.2 age-adjusted MAC, based on end-tidal sevoflurane concentrations. Intermittent cisatracurium besylate was used for muscle relaxation. Pre-incision sufentanil (0.4 μg/kg) was administered for circulatory stabilization.
Owing to the absence of a PACU in our hospital, all patients emerged from anesthesia in the operating room and were transferred to the ward only after they fully regained consciousness. Our anesthesiology department faces a shortage of staff, so postoperative pain management was entrusted to the surgical department. As a result, we could not implement an opioid-free regimen during the entire perioperative period, and opioids, specifically tramadol, were still used for postoperative analgesia. We coordinated with the surgical department in advance for the patients involved in this study. If a patient required pain relief, an intramuscular injection of 100 mg tramadol was administered, while an intravenous injection of 10 mg metoclopramide was given, if needed, to alleviate emesis. No intraoperative or immediate postoperative analgesics (e.g., paracetamol, nonsteroidal antiinflammatory drugs, or local anesthetic infiltration) were administered beyond the specified analgesia regimens.
Outcomes
The mean arterial pressure (MAP) of the patients was recorded as the primary outcome at five time points: entry into the operating room, immediately after anesthesia induction, immediately after endotracheal intubation, 1 minute after incision, and 10 minutes after incision. These time points were marked as T0, T1, T2, T3, and T4, respectively. The heart rate (HR) at these time points was also recorded as a secondary outcome.
After surgery, one of the secondary outcomes was the awakening time. Awakening time was defined as the interval from cessation of anesthetic administration, including closure of the sevoflurane vaporizer and discontinuation of continuous infusions, to the patient’s ability to open their eyes and follow simple verbal commands such as hand squeezing or nodding. Extubation was performed once the patient demonstrated adequate spontaneous respiration and complete neuromuscular recovery (TOF ratio > 0.9). The timing of anesthetic cessation and extubation was determined by the attending anesthesiologist, and the awakening time was recorded by the anesthesia nurse.
Patients were followed up for 6 hours postsurgery and 24 hours postsurgery. The Ramsay scale for sedation, satisfaction score, visual analog scale (VAS) score for pain, and VAS score for PONV were assessed and recorded as secondary outcomes after the operation. The following are detailed descriptions of the above scales.
The Ramsay sedation scale ranges from 1 to 6: 1 indicates anxious, agitated, or restless; 2 indicates cooperative, oriented, and tranquil; 3 indicates response to commands only; 4 indicates brisk response to light stimuli; 5 indicates sluggish response to stimuli; and 6 indicates no response to stimuli.
The satisfaction score is rated on a scale of 0–4 points, where 0 indicates completely dissatisfied, 1 indicates relatively dissatisfied, 2 indicates moderately satisfied, 3 indicates satisfied, and 4 indicates extremely satisfied.
The VAS score for pain consists of a 10-cm line, where the two ends represent “no pain” and “the worst pain imaginable.” Patients mark a point on the line that corresponds to their perceived level of pain. The score ranges from 0 to 10.
The VAS score for PONV consists of a 10-cm line, where the patient marks their perceived level of nausea or vomiting on a scale from no nausea to the worst nausea/vomiting imaginable. The score ranges from 0 to 10.
Perioperative adverse events such as delirium, agitation, hyperalgesia, and chills were monitored. Perioperative drug use, including intraoperative administration of dopamine and atropine, as well as postoperative use of tramadol and metoclopramide, was recorded as an additional outcome.
There were no changes in the trial outcomes after the trial commenced.
Sample size
Based on previous research on hemodynamic fluctuations during OFA, we set α = 0.05 and β = 0.1 and employed a two-sided t-test, with the formula:
Statistical analysis
Statistical analysis was performed via GraphPad Prism 10 for macOS (version 10.2.3). Continuous variables were assessed for normality with the Shapiro–Wilk test. The data are presented as the means with standard deviations or as frequencies with percentages. For normally distributed data, intergroup comparisons were made via independent sample t-tests. Intragroup comparisons across multiple time points were performed using repeated-measures analysis of variance with Bonferroni correction for multiple comparisons. The Mann–Whitney U-test was applied to nonnormally distributed continuous variables. Notably, GraphPad Prism calculates exact p values for the Mann–Whitney U-test, which take into account tied values and small sample sizes. These may differ from approximate p values reported by other software. Categorical data were analyzed with the chi-square test or Fisher’s exact test, depending on expected frequencies. A significance level of p < 0.05 was considered statistically significant.
Randomization and blinding
Our anesthesia nurse Kailian Bai recruited participants the day before the surgery. Patients were randomly assigned to either the OFA group or the CGA group via sealed opaque envelopes, which were distributed by our resident trainee Chen Jiang, on the morning of surgery. Hua Huang, the supervisor of our department, created a random allocation sequence with Microsoft Excel 2013, ensuring 1:1 allocation and random block sizes. The participants and outcome assessors were blinded to group allocation, whereas the anesthetists could not be blinded due to intraoperative safety concerns.
Results
Patient characteristics
The Consolidated Standards of Reporting Trials (CONSORT) flow diagram of this trial is presented in Figure 1. The patients were recruited from September 22, 2022, to November 30, 2022, with the final follow-up completed on December 2, 2022. We terminated the study because we reached the time limit specified in the initial registration and collected the corresponding number of cases. A total of 63 patients were assessed for eligibility. Among them, eight patients did not meet the inclusion criteria: three patients had an ASA III physical status, and five patients had hypertension measured on the morning of surgery. Additionally, seven patients declined to participate in the study. Notably, owing to rigorous patient management during hospitalization, no patients were lost to follow-up within this period (Fig. 1).
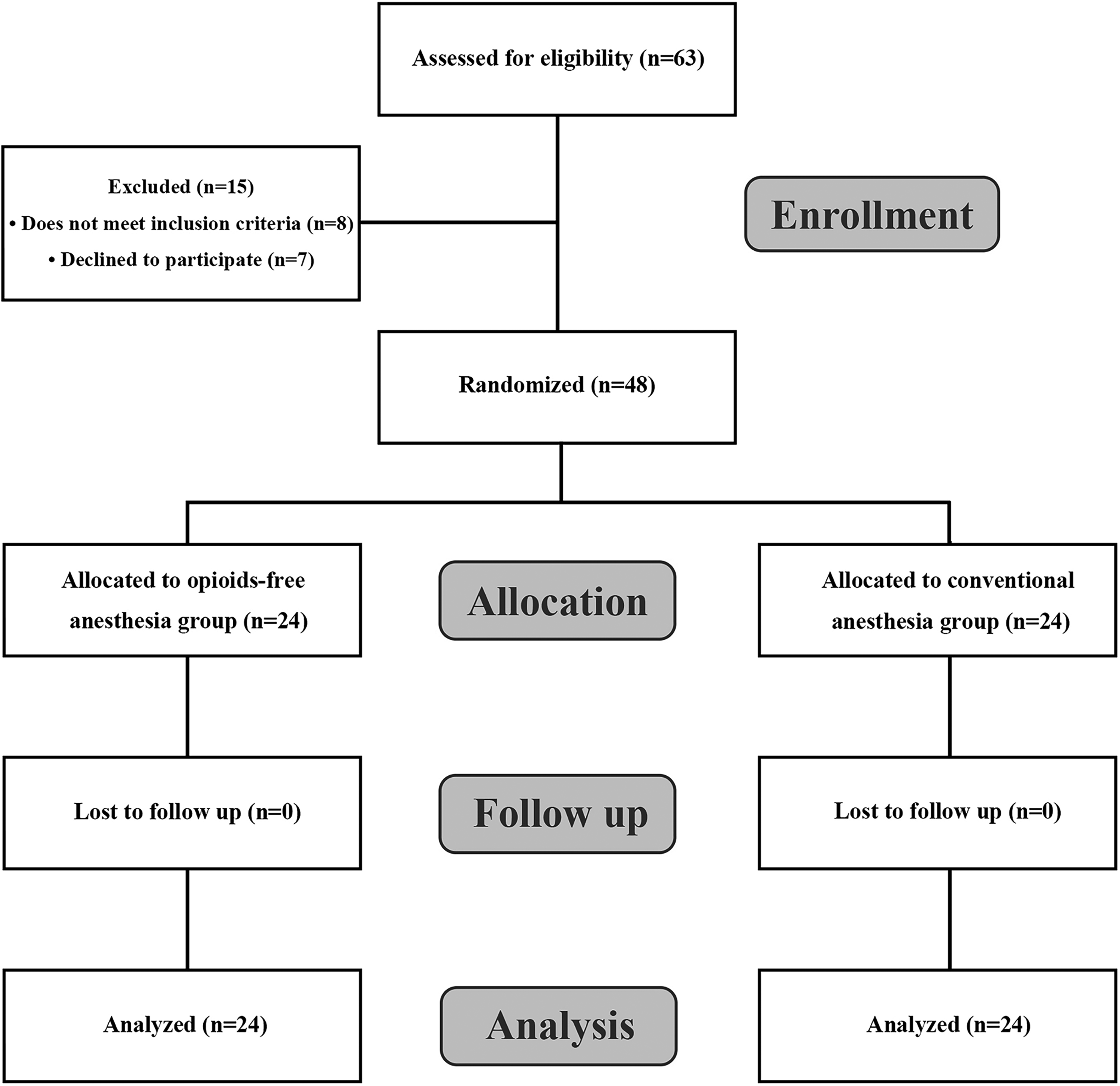
Patient flow chart illustrating the enrollment process in this study.
For each group, 24 participants were included in each analysis. All analyses were conducted according to the original assigned groups as specified in the study protocol. The participants were analyzed on the basis of their initial group allocation, ensuring that the integrity of the randomization process was maintained throughout the study. Anesthesia was induced in the operating room of the Department of Anesthesiology, and follow-up was performed in the wards of the Department of Digestive Surgery. All surgical procedures were straightforward laparoscopic cholecystectomies without complications or placement of surgical drains. Initially, we compared the general data of the two groups, including sex, height, weight, age, operation time, intraoperative blood loss, and ASA status. The clinical characteristics of the two groups were comparable, and there were no statistically significant differences (Table 1).
General Data for All Patients by Group Allocation
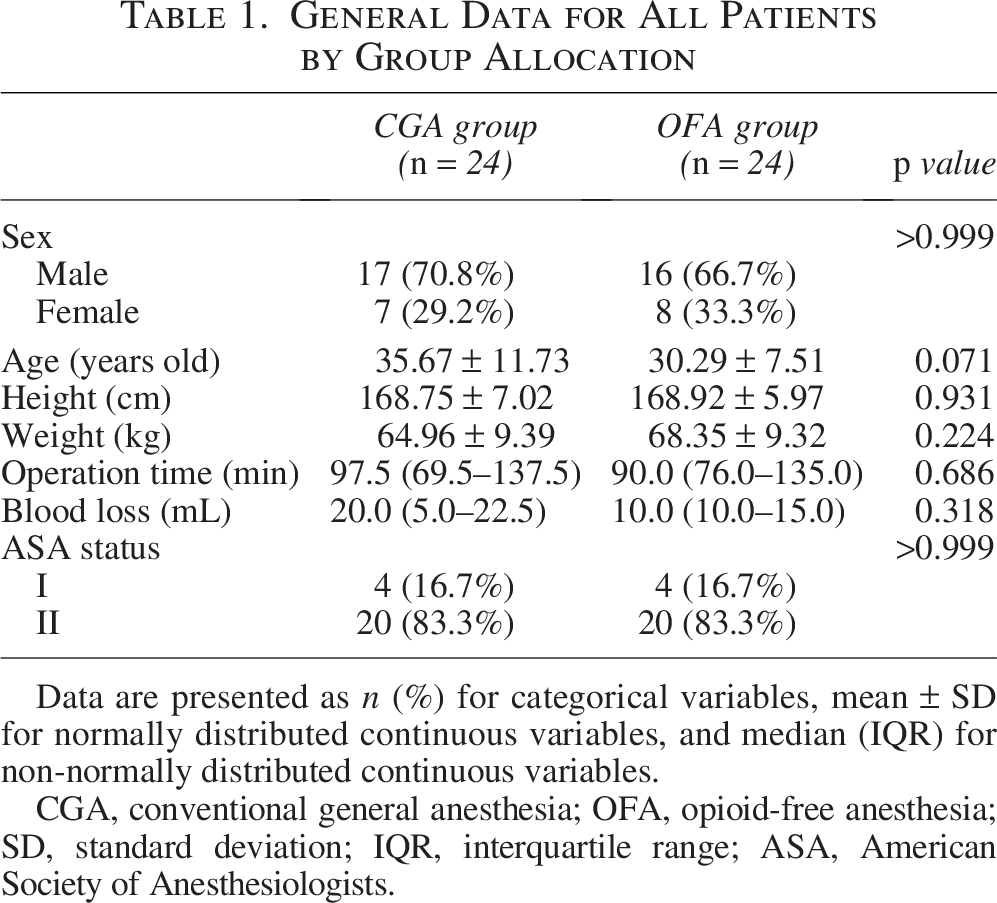
Data are presented as n (%) for categorical variables, mean ± SD for normally distributed continuous variables, and median (IQR) for non-normally distributed continuous variables.
CGA, conventional general anesthesia; OFA, opioid-free anesthesia; SD, standard deviation; IQR, interquartile range; ASA, American Society of Anesthesiologists.
Outcomes
Effects of different anesthesia methods on the MAP and HR
We recorded MAP and HR at five time points: T0 (entry into the operating room), T1 (immediately after anesthesia induction), T2 (immediately after endotracheal intubation), T3 (1 minute after skin incision), and T4 (10 minutes after skin incision), with T0 serving as the baseline. Between-group comparisons revealed significant differences in MAP at T1, T3, and T4 (p < 0.05), while HR did not differ significantly at any time point (p > 0.05).
Using T0 as the baseline for within-group comparisons, the CGA group showed significant decreases in MAP (p < 0.001) and HR (p < 0.01) at T4. In contrast, the OFA group exhibited significant increases in both MAP and HR at T2 compared with T0 (p < 0.01), with no significant differences observed at the other time points (p > 0.05). Detailed results are shown in Table 2.
MAP and HR at Different Time Points
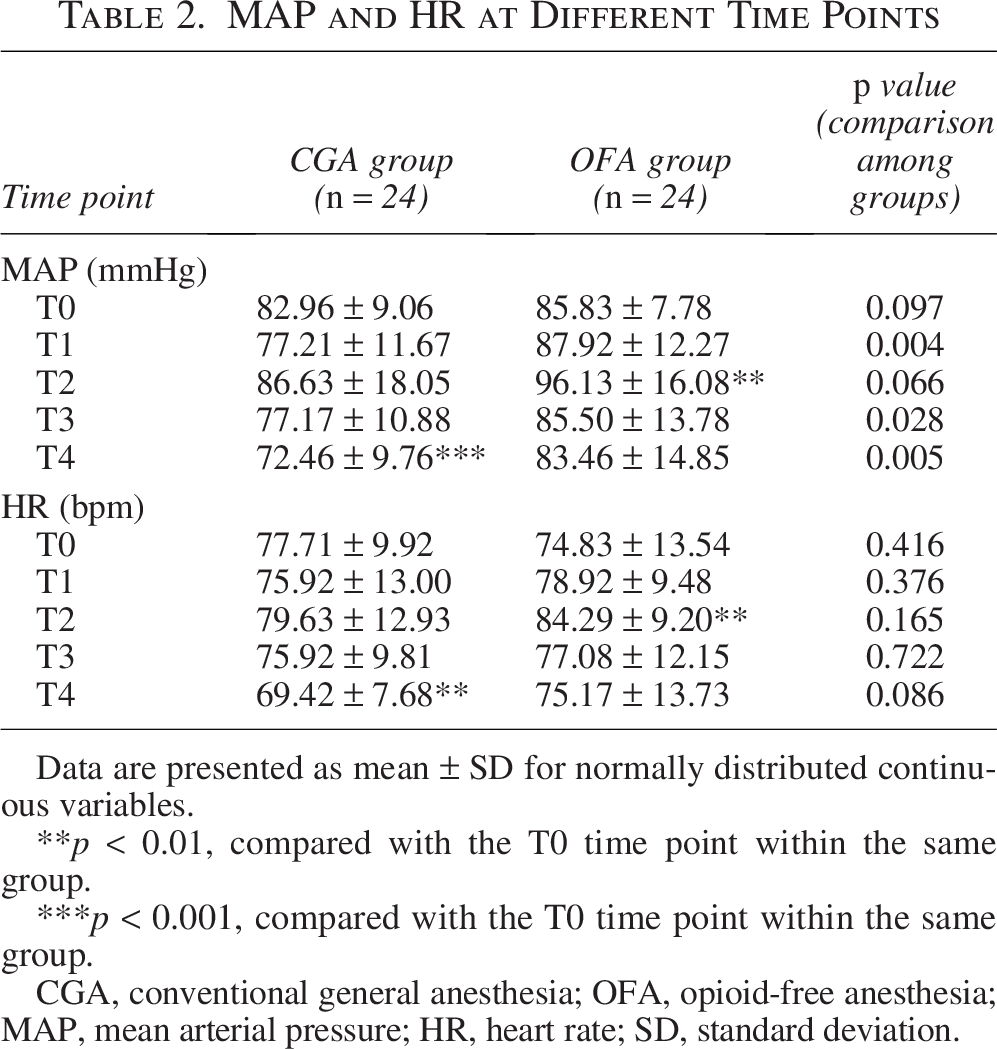
Data are presented as mean ± SD for normally distributed continuous variables.
p < 0.01, compared with the T0 time point within the same group.
p < 0.001, compared with the T0 time point within the same group.
CGA, conventional general anesthesia; OFA, opioid-free anesthesia; MAP, mean arterial pressure; HR, heart rate; SD, standard deviation.
Awakening period and postoperative follow-up outcomes
During the awakening phase, we measured the time it took for the patient to wake up from the cessation of general anesthetic drugs. Compared with that in the CGA group, the awakening time in the OFA group was significantly longer (p < 0.001). Follow-up was performed at 6 and 24 hours after surgery. There was no significant difference in the Ramsay scale score, satisfaction score, or VAS score for PONV between the two groups at 6 or 24 hours after surgery (p > 0.05). VAS scores for pain in the OFA group were significantly lower than those in the CGA group at 6 or 24 hours after surgery (p < 0.005) (Table 3).
Awakening Time and Postoperative Follow-Up Scale Scores
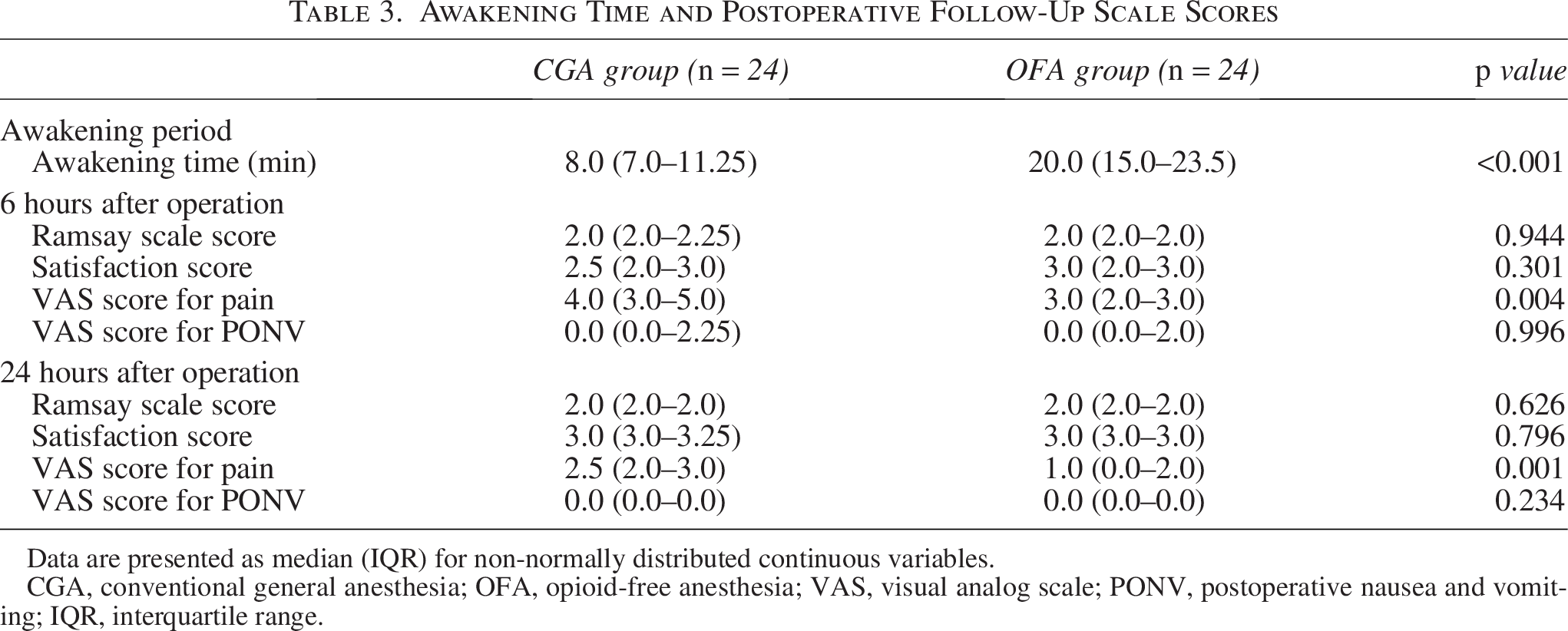
Data are presented as median (IQR) for non-normally distributed continuous variables.
CGA, conventional general anesthesia; OFA, opioid-free anesthesia; VAS, visual analog scale; PONV, postoperative nausea and vomiting; IQR, interquartile range.
Utilization of pharmacotherapy during the perioperative period
We analyzed the use of vasoactive drugs in the two groups of patients during the operation. For comparison, dopamine was uniformly used to address intraoperative hypotension, whereas atropine was used for the treatment of simple sinus bradycardia. Following the surgical procedure, we recorded whether patients received painkillers or antiemetics. We coordinated with the surgery department in advance. In the event of a patient’s need for pain relief, an intramuscular injection of 100 mg tramadol was administered, whereas an intravenous injection of 10 mg metoclopramide was given if there was a requirement to alleviate emesis. However, the statistical analysis revealed no significant difference between the two groups in terms of intraoperative drug dosage or postoperative medication usage rates (p > 0.05) (Table 4).
Perioperative Drug Use
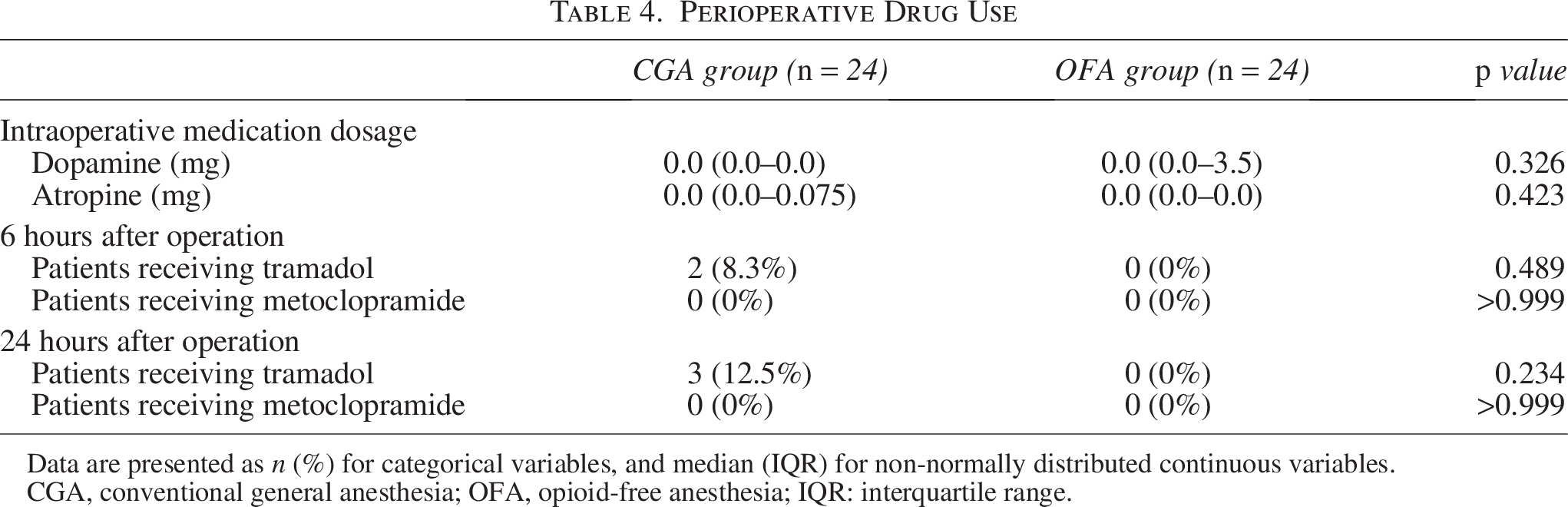
Data are presented as n (%) for categorical variables, and median (IQR) for non-normally distributed continuous variables.
CGA, conventional general anesthesia; OFA, opioid-free anesthesia; IQR: interquartile range.
Harms or unintended effects
No severe adverse events beyond the predefined postoperative pain or PONV outcomes were reported. All participants were monitored for potential adverse effects related to the intervention, but no additional negative effects were observed. Consequently, no further analysis of adverse events was necessary.
Discussion
Opioids are administered perioperatively for postoperative analgesia and intraoperatively to control the sympathetic response to surgical stimuli, frequently as a surrogate for presumed pain (Frauenknecht et al., 2019). OFA is an opioid-sparing technique that focuses on multimodal or balanced analgesia and relies on nonopioid adjuncts and regional anesthesia. Enhanced recovery after surgery protocols, often under the auspices of perioperative pain services, can help guide and promote opioid reduction and OFA without negatively impacting perioperative pain management or recovery (Chia et al., 2020).
Although the application of nonopioid anesthesia in laparoscopy has been confirmed, it still needs to be carefully applied in high-altitude areas (Zheng et al., 2020; Massoth et al., 2021; Toleska and Dimitrovski, 2019). Habitation in a high-altitude environment (chronic hypoxemia) can cause hyperhemoglobinemia, polycythemia, hypercoagulable blood, pulmonary hypertension, cor pulmonale, and congestive heart failure (Richalet et al., 2024; Zheng et al., 2020). Such changes can lead to an increased incidence of anesthesia-related complications (Singh and Singh, 2022). Although our study population consisted exclusively of Tibetans who have lived at high altitude for generations, we did not specifically compare their anesthetic responses with those of other ethnic groups. However, previous studies suggest that Tibetans may possess unique physiological adaptations to chronic hypoxia (Beall, 2007; Simonson et al., 2010), which could potentially influence their response to anesthesia. Whether the administration of OFA in high-altitude areas leads to serious adverse reactions or complications or whether OFA can benefit residents in high-altitude areas has not been confirmed. Therefore, studying the application of OFA in high-altitude areas is highly clinically valuable.
We selected intraoperative hemodynamic stability—specifically MAP—as our primary outcome due to its crucial role in minimizing perioperative risks, particularly hypoperfusion-related complications, which are heightened in chronic hypoxic, high-altitude environments. Maintaining stable MAP is paramount for patient safety in these settings.
Although the MAP values in both groups remained within clinically acceptable limits throughout the perioperative period, distinct hemodynamic response patterns were observed. The CGA group showed a progressive decline in MAP during the maintenance phase, with a significant reduction at T4. In contrast, the OFA group exhibited a transient increase in MAP at T2, corresponding to the response to endotracheal intubation. These findings suggest that, while both regimens are clinically safe in healthy individuals, they produce different cardiovascular trajectories during anesthesia.
Such differences are consistent with previous studies, which have reported that OFA may alter traditional physiological responses to noxious stimuli due to the absence of opioid-induced sympathetic suppression (Chia et al., 2020). In our study, the CGA regimen—containing remifentanil and sufentanil—likely produced cumulative vasodilatory and sympatholytic effects, leading to a gradual MAP decline. Conversely, the OFA regimen included esketamine, a known sympathomimetic, and dexmedetomidine, an α2-agonist with variable effects on blood pressure depending on dose and context. The combination of these agents may have preserved overall cardiovascular tone while permitting transient sympathetic surges, particularly during airway manipulation.
Although these hemodynamic differences may have limited clinical implications in healthy patients, they could become more relevant in individuals with reduced cardiac reserve, autonomic dysfunction, or altitude-related comorbidities. Moreover, such differences have important implications for anesthetic decision-making in high-altitude and remote hospitals, where monitoring capabilities are limited, anesthesia-trained personnel are scarce, and opioid availability is often restricted due to cost and supply constraints. In such settings, anesthetic plans must account not only for the patient’s condition but also for drug accessibility and the feasibility of monitoring and management. Our findings highlight the hemodynamic characteristics of different anesthesia strategies under high-altitude conditions, offering frontline anesthesiologists practical insight into OFA and supporting safe and feasible choices in resource-limited environments.
Owing to the low operating room turnover rate in this area, patients under general anesthesia in our hospital were not transferred to the PACU for recovery after surgery but were instead resuscitated in the operating room. We observed patients’ awakening times and reported that patients in the OFA group had significantly longer awakening times, possibly because of the prolonged half-life of dexmedetomidine. However, no other adverse events were observed during the awakening period. Although OFA may result in a longer time to wake up, it still does not meet the criteria for delayed awakening (more than 30 minutes).
Nonetheless, the extended awakening time observed in the OFA group remains a meaningful limitation in practical terms. This is particularly relevant in high-altitude regions where PACUs are rarely available, and delayed awakening may affect operating room turnover and overall workflow efficiency. Anesthetic strategies in such environments must strike a balance between hemodynamic management and recovery efficiency—whether stabilizing a small number of patients at risk of hypotension or managing large numbers of trauma patients requiring urgent surgical intervention. Future studies should focus on optimizing OFA regimens to minimize recovery time while maintaining hemodynamic stability, especially in resource-constrained, high-altitude environments.
We conducted postoperative follow-up on the two groups of patients, and there was no difference in postoperative satisfaction scores or Ramsay scale scores between the two groups, both of which remained at an ideal level. This favorable outcome may be attributed to the minimal trauma associated with laparoscopic surgery. PONV and pain are crucial factors influencing the perioperative experience of patients. During follow-up visits at 6 hours and 24 hours after surgery, we observed that patients in the OFA group experienced less severe pain than those in the CGA group. Intraoperative opioid use may contribute to postoperative pain sensitization (Colvin et al., 2019; Jin et al., 2022). Therefore, we conclude that the observed result may be attributed to the decrease in the postoperative pain threshold over time due to drug metabolism following the intraoperative use of opioids, a phenomenon not present in the absence of opioids. Notably, esketamine can also prevent hyperalgesia (Ren et al., 2023). Although the data we collected revealed that the mean VAS score for PONV in the OFA group was lower than that in the CGA group at 6 hours after surgery, there was no significant difference between the two groups.
All patients were allowed access to tramadol for postoperative pain relief on an as-needed basis. This approach was based on ethical considerations to ensure that patients experiencing more intense pain could receive timely intervention, rather than be left untreated. It also reflected the standard clinical practice in our institution, where postoperative pain management is handled by surgical wards. The availability of rescue analgesia may have attenuated differences in reported pain scores between groups. Nevertheless, a statistically significant difference in VAS scores persisted, suggesting a potential baseline analgesic advantage of the OFA regimen. While the use of tramadol did not differ significantly between the groups, it is worth noting that three patients in the opioid group required tramadol at 24 hours postoperatively, whereas none in the OFA group did. Although this difference was not statistically significant (Fisher’s exact test, p = 0.234), it may suggest a trend toward reduced postoperative analgesic needs with OFA and warrants further investigation in larger studies. Notably, no severe adverse events or complications were observed in either group during the study period, which may also reflect the effective postoperative care provided by the surgical team.
Limitations
High-altitude areas present unique logistical challenges that significantly impact the design and execution of this study. These challenges include limited accessibility to medical supplies, a shortage of essential medications, low population densities, and harsh environmental conditions, all of which hinder the smooth progression of the study. The geographic isolation of the study site meant that resources had to be transported over long distances, which often led to delays and contributed to the shortage of specific drugs required for the experiment. This constrained the range of medications available for intraoperative use, which required us to adopt simplified or standardized anesthetic protocols based on available agents. While these constraints reflect the real-world context of anesthesia practice in resource-limited high-altitude settings, they may have also limited the flexibility of anesthetic regimen selection.
For example, because esketamine is known to increase salivary and respiratory secretions, preoperative administration of an anticholinergic agent was deemed necessary to minimize the risk of airway obstruction and anesthesia-related complications. However, due to drug availability constraints at our institution, more selective agents such as penehyclidine were not accessible. As a result, intramuscular atropine was routinely administered according to institutional practice. Although necessary under these conditions, we acknowledge that preoperative atropine administration may have influenced intraoperative HR and hemodynamic responses, representing a potential limitation of the study.
Furthermore, due to similar resource constraints, intraoperative depth of anesthesia was monitored using the BIS, which was the only real-time monitoring modality available in our institution. While BIS provided a practical means to reduce the risk of intraoperative awareness, we acknowledge its limitations in the context of OFA. BIS was originally validated for propofol-based regimens and may be influenced by agents such as sevoflurane and especially esketamine, which can transiently elevate BIS values without indicating lighter anesthesia. These fluctuations were anticipated by our anesthesiologists and were not used to adjust anesthetic drug dosing. Despite these limitations, BIS monitoring offered additional guidance to clinical signs or hemodynamic changes, especially in a resource-constrained setting.
Another significant challenge was the difficulty in recruiting qualified anesthesiologists in such high-altitude regions. The physical demands and unique skill set required for anesthesiology in such a setting make it difficult to maintain an adequate number of trained professionals. Consequently, we face a shortage of staff, which impacts the quality and consistency of patient care, particularly in managing sedation and anesthesia. This shortage also restricted the duration of follow-up, limiting us to only a 24-hour postoperative follow-up period. Longer follow-up, which could have provided more comprehensive data on recovery and complications, was not feasible under the given circumstances.
In the OFA group, we were only able to ensure that opioid-free regimens were used during surgery. After surgery, patient-controlled analgesia was not used in any patient, and pain management was delegated to the surgical department. Owing to logistical constraints, including the absence of dedicated pain management teams and the need for rapid decision-making in a resource-limited environment, opioid analgesics are sometimes used postoperatively, making it impossible to completely avoid opioids. This limitation could have influenced the study’s ability to evaluate the effectiveness of opioid-free pain management during the postoperative period.
Additionally, dexmedetomidine, one of the key drugs used in this study, experienced intermittent stock shortages throughout the research period. Given its central role in sedation protocols, this shortage required us to modify our drug administration plan. To mitigate the impact of these shortages, we adopted a low-dose regimen for dexmedetomidine, which may have altered the intended sedative effects and influenced the study outcomes. Despite this, we were able to complete the experiment as planned.
This study focused on relatively healthy high-altitude residents to minimize perioperative risks and control for confounding factors. While this approach allowed us to isolate the impact of chronic high-altitude adaptation on anesthetic responses, it limits the applicability of our hemodynamic findings to patients with altitude-related pathologies. Future studies should include patients with altitude-related diseases to provide a more comprehensive understanding.
Conclusions
In this study, the combination of dexmedetomidine and esketamine for OFA demonstrated safety and effectiveness in high-altitude hypoxic environments, with no adverse outcomes observed. It provided stable intraoperative hemodynamics and effective postoperative pain relief, although it was associated with a more pronounced intubation reaction and notably prolonged awakening time, which may impact clinical efficiency, especially in high-turnover or resource-limited conditions. The study faced challenges typical of high-altitude, resource-limited settings, including medication shortages and staffing constraints, which may have influenced the outcomes. Despite these obstacles, the study was completed successfully, and the findings offer valuable insights that should be interpreted within the context of these limitations. When formulating anesthetic strategies in these environments, it is essential to balance hemodynamic control with recovery efficiency, considering both the need to maintain blood pressure in critically ill patients and the urgency of managing large numbers of emergency patients requiring rapid intervention. Future research should aim to refine OFA regimens to mitigate the issues of intubation reactions and delayed recovery, thereby avoiding clinical trade-offs, and improving care for patients in high-altitude environments.
Authors’ Contributions
K.T., Q.Z., L.T., and K.B. contributed equally to this study. K.T. performed the data analysis and drafted the initial article. Q.Z. and L.T. collected the majority of the intraoperative data. K.B. managed the case screening, enrollment, and coordination. Postoperative follow-ups were conducted by M.F., M.W., L.L., L.Z., Z.Z., H.L., X.L., and R.Y. contributed to the collection of additional intraoperative data. C.J. assigned participants to interventions. H.H. contributed to research supervision and generated the random allocation sequence. M.Z. contributed to the experimental design and article revisions. All the authors have read and approved the final version of the article.
Footnotes
Acknowledgments
The authors thank all the study participants for their involvement in the study. The authors also acknowledge the other staff members within the anesthesiology department who excellently fulfilled their respective roles during this period. Additionally, the authors are thankful for the support and cooperation provided by the surgical departments throughout this endeavor.
Author Disclosure Statement
The authors certify that there are no conflicts of interest with any financial organization regarding the material discussed in the article.
Funding Information
This study was supported by the Natural Science Foundation of Tibet Autonomous Region (No. XZ202301ZR0004G), and the National Natural Science Foundation of China (No. 82371246).