
Abstract
Wu, Tianzhun, Ruofan Li, Qingfeng Song, Li Xu, Chaofan Shi, Juanjuan Liu, Xing Gao, Shilin Huang, Shizhou Li, Dandan Zeng, Wenfeng Luo, Yan Lin, Jiazhou Ye, Minggen Hu, and Rong Liang. Using Mendelian randomization to dissect the relationship between high-altitude adaptation and liver diseases/traits. High Alt Med Biol. 27:42–48, 2026.
Background:
It has been reported that high-altitude adaptation (HAA) and susceptibility to multiple liver diseases/traits differ between individuals at higher altitudes compared to those at lower altitudes. To investigate this association, we conducted a Mendelian randomization study.
Methods:
To investigate the association between HAA and liver diseases/traits, we utilized genome-wide association studies focusing on East Asian ancestry. Our study included six liver disease-related phenotypes: autoimmune hepatitis, chronic hepatitis B, chronic hepatitis C, acute hepatitis by hepatitis A virus, hepatic cancer, and hepatic bile duct cancer, as well as five liver traits: alkaline phosphatase, alanine aminotransferase, aspartate aminotransferase, γ-glutamyl transpeptidase (GGT), and total bilirubin. A Bonferroni-corrected significance was set at p < 4.55 × 10−3.
Results:
Our study identified a significant genetically predicted causal impact of HAA on GGT (odds ratio [OR] = 1.601; 95% confidence interval [CI] = 1.204–2.129; p = 0.0012). Interestingly, the association remained statistically significant even when the causal direction was reversed, with GGT predicting HAA (OR = 1.01; 95% CI = 1.003–1.011; p = 0.0013). Both findings surpassed the Bonferroni-corrected threshold.
Conclusion:
In conclusion, our study provides suggestive evidence for a potentially causal bidirectional association between HAA and GGT. These novel insights may inform the development of targeted preventive measures and therapeutic interventions for liver diseases and high-altitude adaptation.
Introduction
The atmospheric conditions at high altitudes play a crucial role in shaping health outcomes (Beall, 2007). Many studies have reported that the high-altitude adaptation (HAA) observed in populations living at high altitude is a result of nature selection (Beall, 2007; Simonson et al., 2010). People such as the Tibetan community have developed unique physiological traits to cope with the environmental stress of hypoxia (Beall, 2007). Evidence suggests that in humans living at high altitudes, liver function undergoes significant changes to adapt to the hypoxic environment (Ge et al., 2015). Specifically, during chronic hypoxia, the liver increases fatty acid uptake and oxidation (Midha et al., 2023). Moreover, circulating levels of liver enzymes such as alkaline phosphatase (ALP), Alanine aminotransferase (ALT), and γ-glutamyl transpeptidase (GGT) are notably altered in the hypoxic environment of high altitude (He et al., 2023; Luo et al., 2013; Rawal et al., 1999). These findings underscore the importance of understanding liver changes associated with HAA and the necessity of developing effective strategies for the targeted prevention and treatment of liver diseases.
Chronic hypoxia caused by high altitude can affect liver functions, leading to abnormal amino acid levels in liver tissues (Liang and Song, 2023). Hypoxia also disrupts the liver’s roles in fuel storage and lipid metabolism (O’Brien et al., 2021). For individuals with liver diseases, it is crucial to assess whether the physiological response to hypoxia increases the risk of altitude sickness or worsens the underlying liver condition in high-altitude environment (Luks and Swenson, 2015). However, there is still a lack of comprehensive studies exploring the genetic associations between HAA and liver diseases.
Mendelian randomization (MR) analysis is increasingly used to investigate causal association between exposure and outcomes (Lawlor et al., 2008). This approach uses genetic variants strongly associated with a specific risk factor as instrumental variables (IVs) (Woolf et al., 2022). Since genetic variations are randomly assigned before birth according to the principles of Mendelian inheritance, MR analysis is considered to be capable of minimizing confounding effects (Sanderson et al., 2022). Currently, the precise causal relationship between exposure to high-altitude environments and the development or exacerbation of multiple liver conditions remains an area of active research and is not yet fully understood.
Determining the functional mechanisms of genome-wide association studies (GWASs) identified loci is challenging, as many statistically significant variants lack a direct causal biological relationship, complicating their translation into clinical applications (Long et al., 2023). Therefore, we conducted an MR design in this study, leveraging summary data from previously published GWASs to explore the causal correlation between HAA and hepatic pathophysiology (Fig. 1). Our findings reveal a causally relevant effect of HAA on GGT levels; intriguingly, reverse MR analysis also demonstrated a causal effect of GGT on HAA. This study provides valuable insights that may guide the development of targeted interventions and preventive strategies for both high altitude-related health challenges and liver diseases.
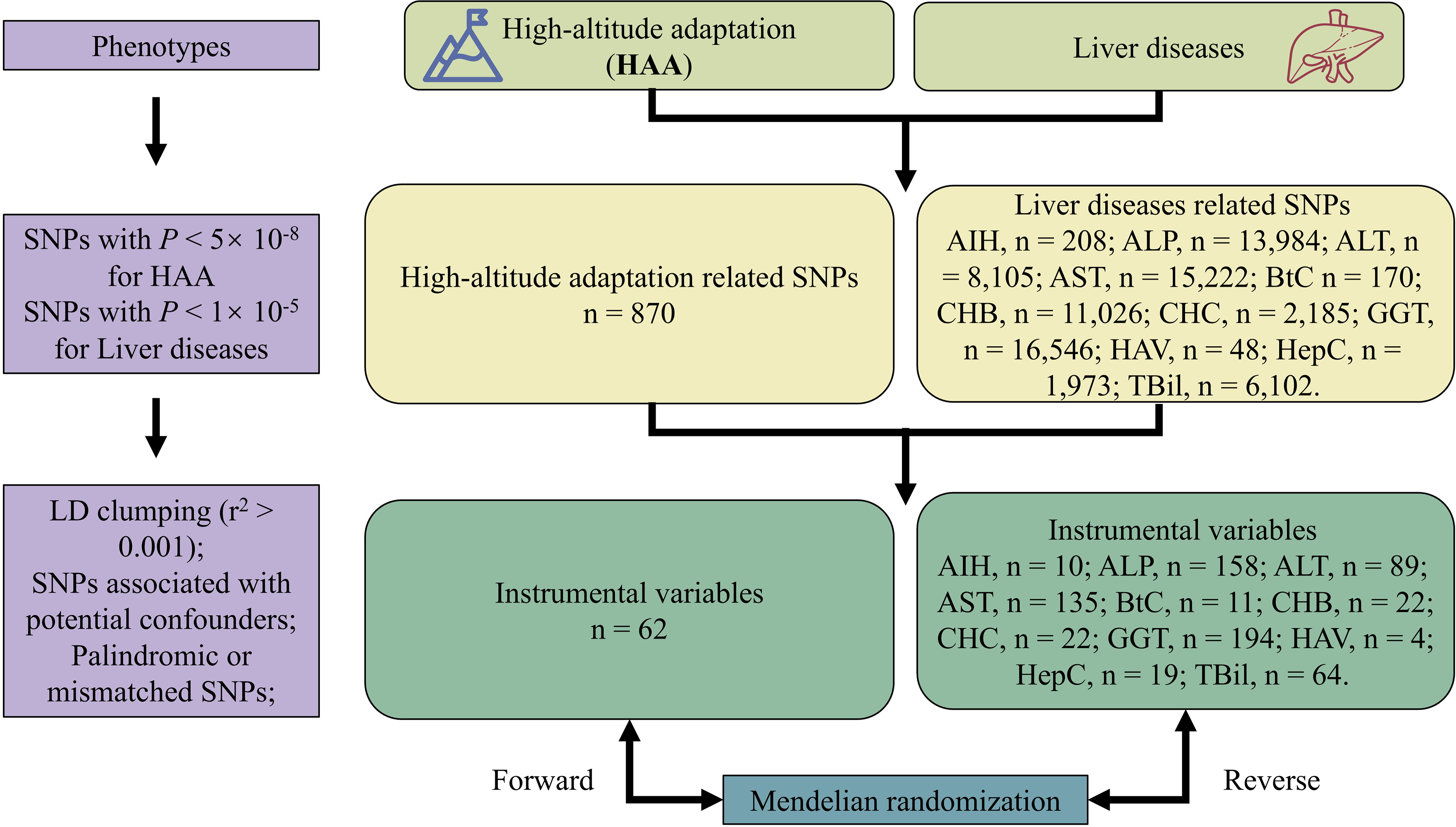
Flowchart of Mendelian randomization analysis.
Methods
Study design
A two-sample bidirectional MR analysis was performed to estimate the causal relationship between HAA and liver diseases/traits, and vice versa. To minimize bias of multi-ancestry studies, we restricted the study population to East Asians to ensure that the results are more specific to this population (Zhao et al., 2022). The GWASs summary data utilized in this study were obtained from two publicly available databases (Yang’s study:cnsgenomics.com/data/yang_et_al_2017_pnas.html;BBJ:https://humandbs.biosciencedbc.jp/en/), with the workflow illustrated in Figure 1.
Cohorts used in high-altitude adaptation
The GWAS data for HAA used in this study were derived from the study conducted by Yang et al., (2017). The subjects resided in the southwestern region of China, at an approximate elevation of 4,000 m, and none had known medical records or illnesses related to high-altitude exposure. This study included 3,008 Tibetan individuals and 7,287 participants from low-altitude regions in China. The GWAS summary details of HAA are provided in Supplementary Table S1.
Cohorts used in liver diseases
The GWAS data of liver diseases/traits were obtained from the Biobank Japan Project (BBJ) (https://humandbs.biosciencedbc.jp/en/) (Sakaue et al., 2021). In this MR analysis, we utilized GWAS summary-level data for 11 liver-related phenotypes, comprising 6 liver diseases—autoimmune hepatitis (AIH), cancer of hepatic bile ducts (BtC), chronic hepatitis B (CHB), chronic hepatitis C (CHC), acute hepatitis by hepatitis A virus (HAV), and hepatic cancer (HepC)—and 5 liver function traits: ALP, ALT, aspartate transaminase (AST), (GGT, and total Bilirubin (TBil). Detailed information on GWASs for liver diseases is provided in Supplementary Table S1.
Instrumental variable selection of high-altitude adaptation
We used IVs to explore the causal relationship between HAA and liver diseases/traits. To select IVs for HAA in East Asian population, we performed a series of measures to ensure quality. First, the single-nucleotide polymorphisms (SNPs) for HAA (p < 5 × 10−8, n = 870) were extracted. Second, if SNPs is with strong linkage disequilibrium (LD) (r2 < 0.01, clumping distance = 1,000 kb), we only retained one SNP. Third, to ensure that the selected SNPs are not associated with the outcomes, we excluded those SNPs that showed significant associations with either of the chosen liver diseases (p < 1 × 10−5). Fourth, SNPs were excluded if they were palindromic or ambiguous. Fifth, if there were no corresponding SNPs for an IV in the outcome, then we selected another SNP substitution that was in strong LD (r2 > 0.8, East Asian populations, 1,000 Genomes Project). Therefore, we obtained 62 SNPs as IVs. The list of these selected IVs is provided in Supplementary Table S2.
Instrumental variable selection of liver diseases
To further explore the potential causal effect of liver diseases/traits on HAA. Given that some liver disease-related SNPs have relatively small numbers at the P threshold of 5 × 10−8, to obain more robust results, we used a nominal significance level (p = 1 × 10−5) as the selection threshold of IVs (Long et al., 2023; Xie e al., 2023; Yang et al., 2023). The SNPs were extracted for AIH (n = 208), ALP (n = 13,984), ALT (n = 8,105), AST (n = 15,222), BtC (n = 170), CHB (n = 11,026), CHC (n = 2,185), HAV (n = 48), HepC (n = 1,973), GGT (n = 16,546), and TBil (n = 6,102). To select IVs for liver diseases/traits, we applied the same procedure as described above. Finally, we obtained 10 SNPs for AIH, 158 SNPs for ALP, 89 SNPs for ALT, 135 SNPs for AST, 11 SNPs for BtC, 22 SNPs for CHB, 22 SNPs for CHC, 4 SNPs for HAV, 19 SNPs for HepC, 194 SNPs for GGT, and 64 SNPs for TBil as IVs. The list of these selected IVs is provided in Supplementary Table S3.
Statistical analysis
To evaluate the causal association between HAA and each liver disease/trait, we performed inverse variance weighted MR analysis (Burgess et al., 2019).
To ensure the validity of MR results, we first listed the following key assumptions: (I) The genetic variant is related to the exposure; (II) the instrument used for the exposure does not involve unknown confounders; (III) the genetic variant does not directly affect the outcome outside its effect on the exposure (Emdin et al., 2017). In order to verify the basic assumptions described above (I–III), we performed sensitivity analyses to assess the robustness of the MR results, including horizontal pleiotropy and heterogeneity analyses. We employed MR-Egger regression to detect potential pleiotropy assessments. A p value greater than 0.05 indicates the absence of directional pleiotropy (Verbanck et al., 2018). Cochran’s Q test (MR-IVW) and Q statistic (MR-Egger) were employed to assess the heterogeneity, where p > 0.05 suggests no significant heterogeneity (Hemani et al., 2018). To examine whether any individual SNP significantly impacted the observed association, we conducted leave-one-out analysis, systematically removing one SNP at a time and reanalyzing the data (Gage et al., 2017).
The strength of the IVs was assessed using the F-statistic. An F-statistic greater than 10 indicates a robust instrument (Palmer et al., 2012). The F-statistic was quantified by the following equation: F = β2/SE2 (Xie et al., 2023).
We applied the Bonferroni-corrected p value threshold to account for multiple testing (1 exposure on 11 outcomes, 0.05/11 = 4.55 × 10−3). MR analysis was performed using R (v4.3.1) and R package “TwoSampleMR” (v0.5.7).
Results
Information of instrument selection
To investigate the causal effect between HAA and liver diseases/traits, we obtained the GWAS data of HAA from the Yang et al. study and data from the BBJ Project for 11 types of liver diseases/traits (including AIH, ALP, ALT, AST, BtC, CHB, CHC, HAV, HepC, GGT, and TBil) (Supplementary Table S1). The SNP selection is described in the Methods section. A total of 62 SNPs were retained as IVs for HAA (Supplementary Table S2). For liver diseases, the following SNPs were retained as IVs: 10 SNPs for AIH, 158 SNPs for ALP, 89 SNPs for ALT, 135 SNPs for AST, 11 SNPs for BtC, 22 SNPs for CHB, 22 SNPs for CHC, 4 SNPs for HAV, 19 SNPs for HepC, 194 SNPs for GGT, and 64 SNPs for TBil(Supplementary Table S3). The F-statistics for these genetic variants ranged greater than 10 (20–127) among the HAA and liver diseases/traits, respectively (Supplementary Table S4), indicating that the instruments are strong and minimizing potential weak instrument bias (Burgess et al., 2011).
The causal effects of HAA on liver diseases/traits
We performed MR analysis using five different methods to assess the causality of HAA on liver diseases/traits in East Asian population. According to the inverse variance weighted method, our MR results demonstrated that HAA is positively associated with GGT levels, with an odds ratio (OR) of 1.601 (95% confidence interval [CI] = 1.204–2.129, p = 0.0012; Supplementary Table S5), which was significant after Bonferroni-corrected (p = 0.05/11 = 4.55 × 10−3). This outcome aligned with the findings from the weighted median analysis, which demonstrated an OR of 1.558 (95% CI 1.025–2.368 p = 0.038). However, there was no evidence of causality between HAA and the risk of AIH (OR = 3.080, 95% CI = 2.503 × 10−6-3.789 × 106, p = 0.875), ALP (OR = 1.072, 95% CI = 0.774–1.484, p = 0.675), ALT (OR = 1.225, 95% CI = 0.925–1.622, p = 0.157), AST (OR = 1.157, 95% CI = 0.873–1.535), BtC (OR = 1.768, 95% CI = 0.003–908.000, p = 0.858), CHB (OR = 16.673, 95% CI = 0.893–311.257, p = 0.060), CHC (OR = 1.148, 95% CI = 0.282–4.670, p = 0.847), HAV (OR = 585.871, 95% CI = 0.468–7.327 × 105, p = 0.080), HepC (OR = 3.667, 95% CI = 0.273–49.225, p = 0.327), and TBil (OR = 1.047, 95% CI = 0.697–1.572, p = 0.826). These results indicated that HAA is causally correlated with GGT levels.
The forest plots are shown in Figure 2. Leave-one-out plots and scatter plots of these results are displayed in Supplementary Figures S1 and S2.
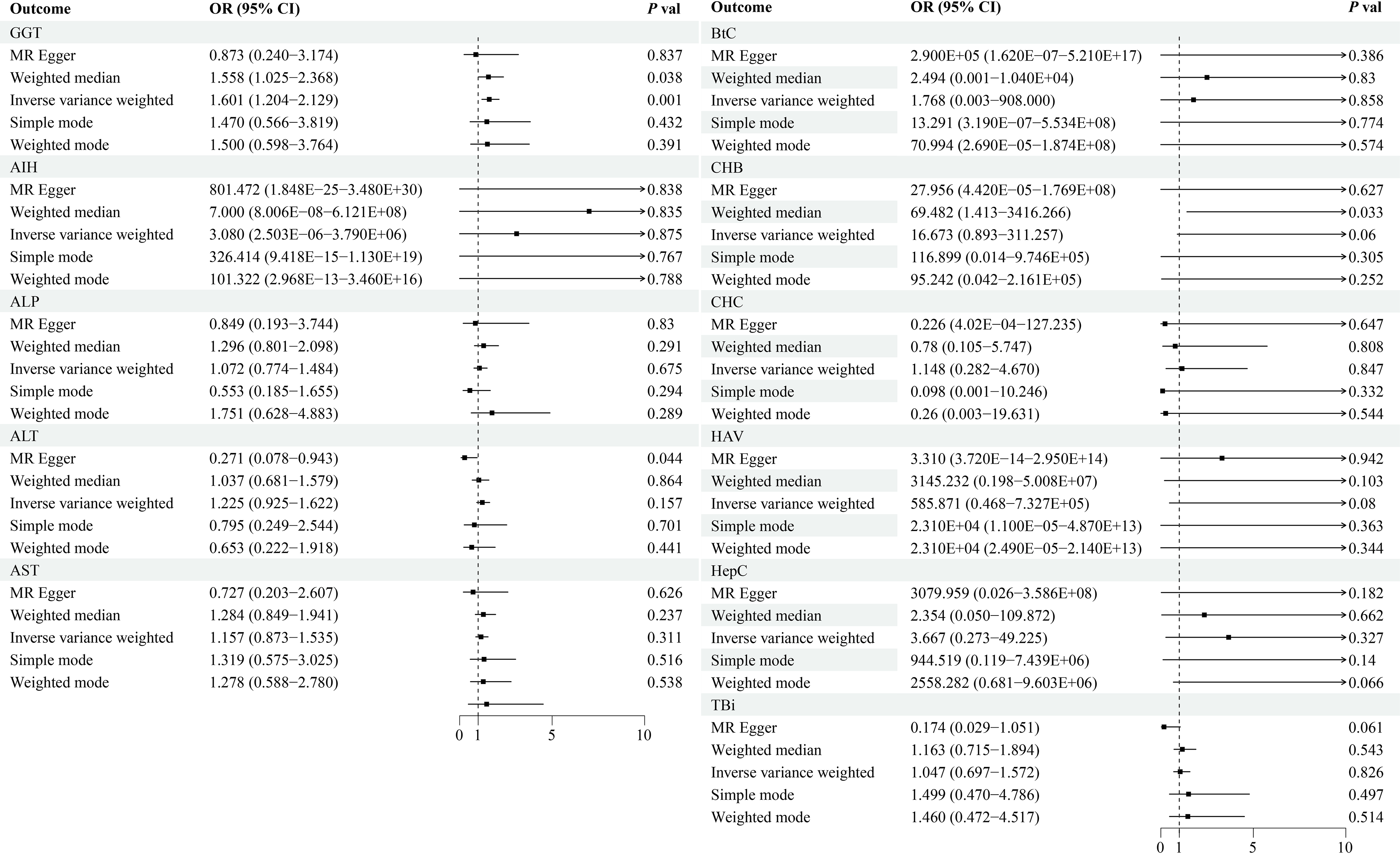
The forest plot shows the MR effect results of HAA on liver diseases. Forest plots showing the MR analysis results between HAA and liver diseases. The ORs, 95% CIs, and p values are shown. AIH, autoimmune hepatitis; ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate transaminase; BtC, hepatic bile duct cancer; CI, confidence interval; CHB, chronic hepatitis-B; CHC, chronic hepatitis-C; GGT, γ-glutamyl transpeptidase; HAA, high-altitude adaptation; HepC, hepatic cancer; HAV, acute hepatitis by hepatitis-A virus; OR, odds ratio; SNP, single-nucleotide polymorphism; TBil, total bilirubin.
The causal effects of liver diseases/traits on HAA
We then delved into the potentially causal association of liver diseases/traits on HAA. Our analysis revealed that GGT exhibited a statistically significant level of association with HAA when employing the inverse variance weighted analysis (OR = 1.007, 95% CI = 1.003 −1.011, p = 0.0013; Supplementary Table S6). Conversely, the outcomes did not meet the significant threshold for any of the other ten types of liver diseases (p > 0.05/11 = 4.55 × 10−3).
The forest plots are shown in Figure 3. Leave-one-out plots and scatter plots of these results are displayed in Supplementary Figures S3 and S4.
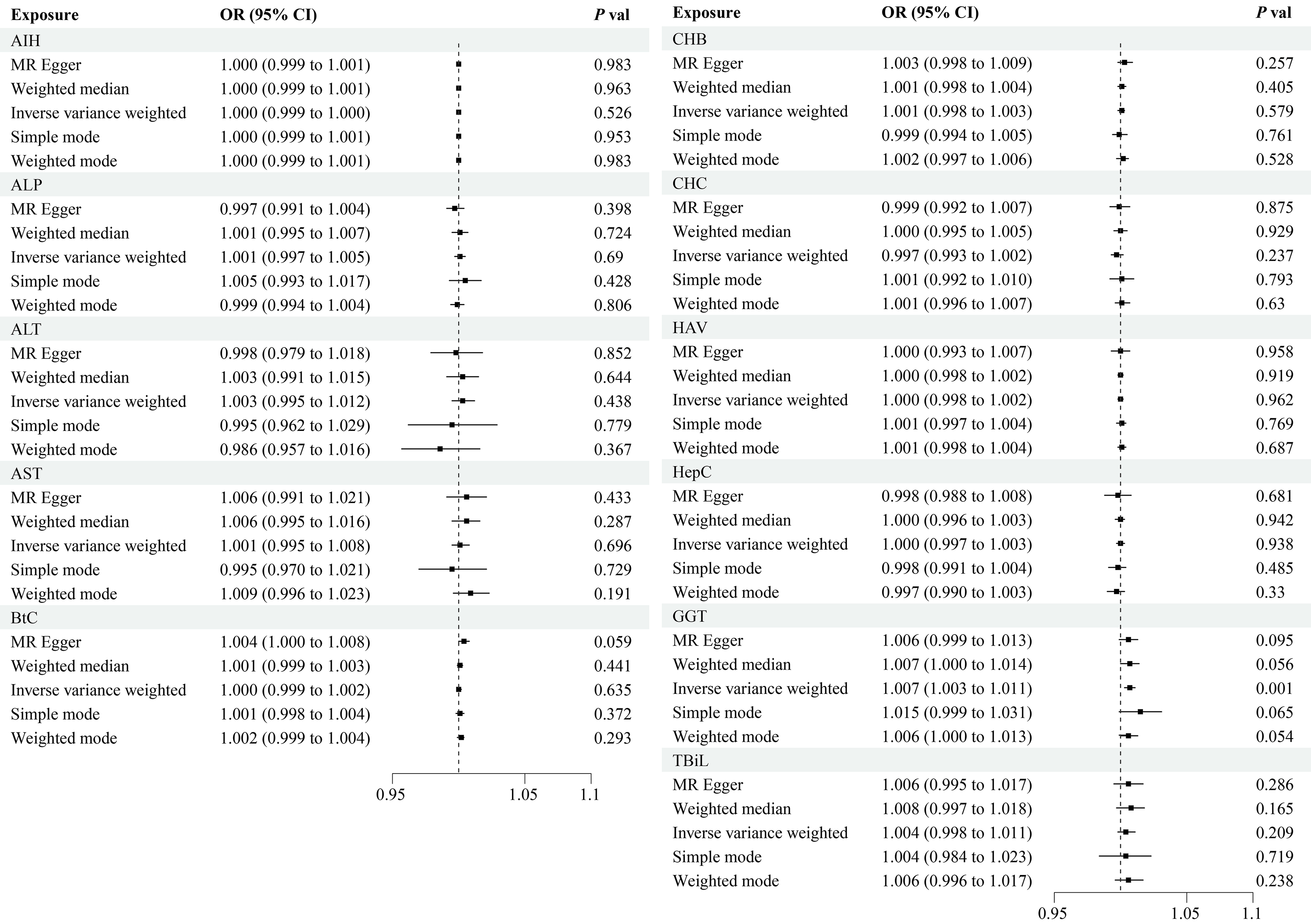
The forest plot shows the MR effect results of liver disease on HAA. Forest plots showing the MR analysis results between liver diseases and HAA. The ORs, 95% CIs, and P values are shown.
Sensitivity analysis
To verify the reliability and stability of the estimated causal effects between HAA and liver diseases/traits, we employed various analytical methods. The MR-Egger analysis yielded p values exceeding 0.05, indicating the absence of directional pleiotropy (Supplementary Tables S5 and S6). Furthermore, several heterogeneity test p values were also above the 0.05 threshold, leading us to adopt the random-effects model for effect estimation (Supplementary Tables S5 and S6). The leave-one-out analysis results showed no significant anomalies, demonstrating that the observed associations remained consistent regardless of the exclusion of any single genetic variant. These findings indicate that the associations are robust and not significantly influenced by any individual genetic variation in the dataset.
Discussion
In this study, the phenotype GGT indicates that the serum GGT concentration exceeds the normal range. By leveraging large-scale GWASs summary statistics, our bidirectional MR study investigated a causal relationship of HAA on liver diseases/traits, as well as the reverse direction. We identified a positive correlation between HAA and circulating GGT levels. Moreover, we found that GGT also has a significant causal relationship with HAA. Notably, this study is the first to explore and establish a causal relationship between HAAs and GGT. These findings provide valuable insights into the phenomenon of elevated GGT level in high-altitude population.
GWASs have been instrumental in uncovering genetic variants associated with disease susceptibility (Li et al., 2021; Wang et al., 2024). In our study, we used data from the largest known GWASs to investigate the causal effect between high-altitude adaptation and liver diseases/traits. Clinically, serum GGT is a widely recognized biomarker of hepatobiliary diseases, with elevated GGT levels often associated with increased free radicals and imbalances in glutathione (Lee and Seo, 2023). GGT located on the cell surface, hydrolyzes γ-glutamyl bonds in extracellular glutathione, playing a key role in the redox cycle (Hanigan, 2014). In addition, GGT is crucial for antioxidant defense, detoxification, and inflammation (Zhang and Forman, 2009). Recent studies have revealed causal relationships between GGT and conditions such as type 2 diabetes (Bi et al., 2022), stroke (Lee and Seo, 2023), calculus of kidney (Li et al., 2023). However, there is limited research exploring the connection between HAA and GGT. The physiological role of GGT in high-altitude populations remains largely unexplored, making our findings a significant contribution to understanding this relationship.
Several epidemiological evidence have indicated that GGT in high-altitude populations (Tibetans) exceeds compared with those observed in low-altitude emigrants (Han) (He et al., 2023; Yuan et al., 2023). He et al. defined high levels of GGT as one of the characteristic phenotypes of HAA in Tibetan (He et al., 2023). Hypoxia is known to cause hepatocyte dysfunction, contributing to conditions such as hypoxic hepatitis and liver fibrosis (Foglia et al., 2021; Solanki and Shah, 2024; Waseem and Chen, 2016). Thus, increased GGT levels may represent a physiological cost of adapting to hypoxia. Furthermore, GGT has been established as an independent predictor of hepatitis (Zhan et al., 2023), potentially contributing to the elevated incidence of hepatitis observed in Tibetan populations (Shen et al., 2014).
Individuals with elevated GGT levels appear to have an enhanced ability to adapt to the high-altitude environment. Mechanistically, GGT plays a pivotal role in regulating oxidative stress balance by facilitating the biosynthesis of glutathione, a potent intracellular antioxidant. GGT maintains redox homeostasis by hydrolyzing extracellular glutathione, enabling the recovery of cysteine—a critical precursor for intracellular glutathione synthesis (Mitric and Castellano, 2023). This upregulation of GGT increases cellular resilience to oxidative stress. High-altitude environments are characterized by extreme hypobaric hypoxia, a condition that exacerbates oxidative stress. The elevated GGT levels observed in certain individuals may act as a compensatory mechanism, enhancing their capacity to counteract oxidative damage. This adaptive response could explain why individuals with higher GGT levels are better suited to thrive in high-altitude settings (Sinha et al., 2009).
The results of our MR analysis stem from a rigorous process of instrument selection and validation. By leveraging GWAS data with a large sample size, our study enhances statistical power, providing reliable insights while mitigating concerns related to personal privacy. Additionally, the use of genetic variations as instrumental variables reduces the influence of environmental confounding, offering a distinct advantage over conventional clinical trials in establishing causal relationships.
As for limitations, first, we were unable to validate our results due to the lack of GWAS summary data for HAA in other high-altitude-adapted people. Further validation analyses are necessary to confirm the causal relationship between HAA and GGT. Our study focused exclusively on East Asian population. Previous studies have shown that various populations adapt to high-altitude environments in distinct ways because of genetic diversity (Ge et al., 2023).
Overall, GGT may serve as a valuable marker of HAA. In the future, it could be utilized as one of the biological indicators to develop predictive models for identifying HAA in populations. Additionally, GGT levels may aid in risk assessment for individuals with chronic liver diseases planning high-altitude travel, helping to mitigate potential health risks associated with such environments (Luks and Swenson, 2015).
In general, these MR results showed that increased HAA capacity will lead to a corresponding increase in GGT, and vice versa. These findings could provide a foundation for developing screening and prevention strategies for diseases associated with GGT abnormalities in high-altitude populations, offering valuable insights into health management in high-altitude environments.
Strengths and Limitations
Strengths
This is the first systematic MR analysis on the causal relationships between HAA and liver diseases/traits.
We used the currently the largest GWAS summary statistics to perform the MR Analysis.
Limitations
The study was limited to an East Asian population.
Authors’ Contributions
T.W., R.L., X.L., and Q.S. contributed to acquisition, analysis, and interpretation of data. C.S., J.L., X.G., and S.H. helped with the figures and tables. S.L., D.Z., and W.L. helped revise the article. Y.L. and R.L. reviewed and edited the article. R.L., M.H., and J.Y. approved the final version of the article. All the authors read and approved the final article.
Footnotes
Acknowledgment
The authors would like to thank the Yang et al. and BioBank Japan Project for contributing data.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This work was supported by grants from the special project of the key research and development tasks of Xinjiang Uygur autonomous region (No. 2022B03005-2); National Natural Science Foundation of China: NO.82060427, 82103297; Guangxi Key Research and Development Program: No. AB19245002; Advanced Innovation Teams and Xinghu Scholars Program of Guangxi Medical University; Guangxi Medical University Outstanding Young Talents Training Program; Guangxi Scholarship Fund of Guangxi Education Department; Guangxi Medical and health key discipline construction project; and Guangxi Medical and health key cultivation discipline construction project.
Availability of Data and Materials
Ethics Approval and Consent to Participate
Ethical approval was obtained from the original studies.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.