
Abstract
Álvarez-Herms, Jesús, Kilian Jornet, Martin Burtscher, Adriana González, and Adrián Odriozola. Gut microbiota dynamics during extreme altitude climbing: a longitudinal case report. High Alt Med Biol. 27:123–127, 2026.—The present case study would explore the acute changes of gut microbiota (GM) and some physiological responses of a world-class mountaineer during a 4-week stay at altitudes between 3,600 and 4,200 m, with four rapid ascents to different extreme altitudes, that is, 6,700, 7,000, 8,000, and 8,400 m. Severe hypoxemia, hyperglycemia, ketoacidosis, and sympathetic dominance were found to be proportionally higher with increasing altitude. Thus, the GM changed during the acclimatization period, decreasing bacterial diversity (Shannon index from 5.88 to 4.56). Remarkably, during the third week, a transient increase of the pathogenic bacteria Ruminococcus gnavus (+2,800%) was found. Thus, this significant elevation coincided with the impaired systemic health and gastrointestinal and respiratory complications. In conclusion, the present exploratory study found that a favorable and healthy GM profile, characterized by elevated mucolytic and short-chain fatty acids-producing bacteria, may improve hypoxic tolerance, reduce the risk of developing gut leakage syndrome and systemic endotoxemia, and protect against acute mountain sickness.
Introduction
In recent years, there has been increasing interest in understanding the effects of hypoxia on the intestinal system and the gut microbiota (GM). Hypoxia can impair the integrity of the intestinal epithelial barrier and promote an imbalance of the GM (Geng et al, 2023; Han et al, 2021; Hao et al, 2024). A major limitation experienced by mountaineers during expeditions is related to their inability to eat and drink enough due to intestinal complications and/or loss of appetite. The relationship between gastrointestinal (GI) complications and GM remains inconclusive. The main aim of this case study was to reduce exposure time at extreme altitudes to improve physical fitness and gut health. The premise was that reduced time at extreme altitudes may have benefits for GI health and prevent biological wear and tear and acute mountain sickness (AMS) conditions.
Materials and Methods
Ethics statement
The present study was approved by the Human Research Ethics Committee of the School of Science and Technology (M10 2021 191). The participant gave written informed consent.
Participant
The participant was a world-class professional ultra-endurance athlete and high-altitude climber (age 36 years; 171 cm; and 56 kg). His maximal oxygen uptake values measured during the last decade showed an exceptional aerobic endurance capacity (85–92 ml/(kg·min). Previously, he climbed Mount Everest in two consecutive trials during the 2017 spring season without the use of supplementary oxygen. The expedition protocol is shown in Figure 1. The present protocol was mainly designed to achieve two main goals: (1) to reduce the health and perceptive problems provoked by prolonged high-altitude acclimatization, including the relative sedentarism and fitness decrement over time and (2) to stimulate the perceptive sensations and physiological changes produced by progressive higher altitude only by rather short-term rapid ascents and prioritizing resting at not extreme altitudes.
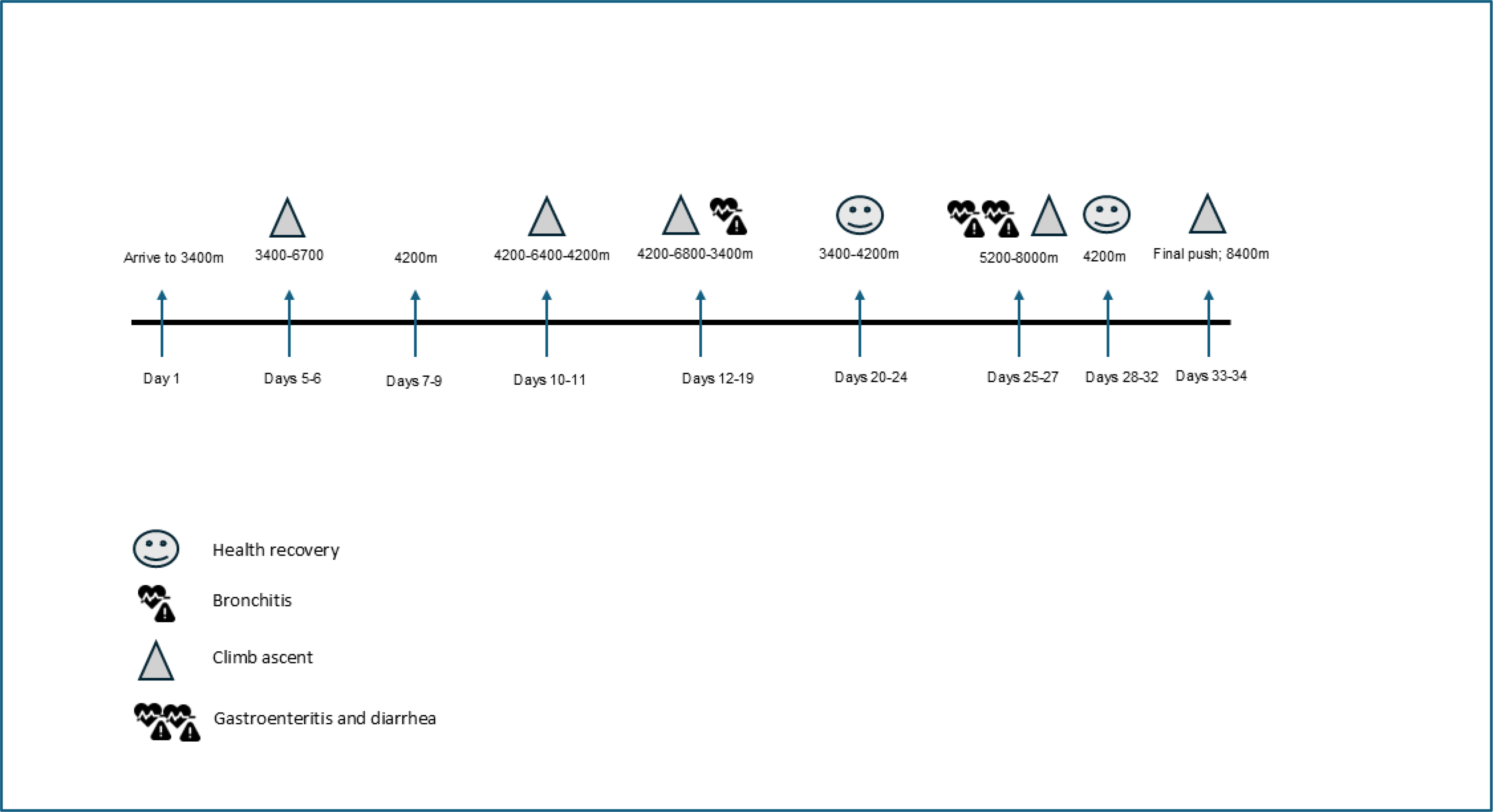
Chronological time of high-altitude expedition Description of acclimatization process during high-altitude expedition and days. On day 1, arrive at base camp at 3400 meters to Day 5, climb to 6700m, and return to base camp 2 at 4200m. From 7 to 9 days living at 4200m with a fast ascent to 6400m on days 10 and 11. Return to base camp at 4200m from day 12 to 19 when climb to 7000m with bronchitis signs. Days from 20 to 24 stay at base camp between 3400 to 4200m recovering. On days 25 and 27, it rose to 8000m with gastroenteritis and diarrhea signs that improved during 28 to 32 days at 4200m. During days 33 and 34, the final push to Mount Everest arrived at 8400m.
Physiological and GM samples
During each rapid ascent, physiological data were measured by the athlete (see Table 1). The GM samples were taken (1) before the expedition and (2) after each rapid ascent (weeks 2, 3, and 4). Muscular and arterial oxygen saturation was measured using a Moxy® monitor and pulse oximetry (such as Omron® P300 Intelli IT), capillary blood samples were analyzed for glucose and ketone levels using a Keto-Mojo® GKI, and blood lactate concentration was measured using Lactate Pro®. Heart rate was monitored using a chest strap model (Polar® H10). The GM analysis protocol is included as Supplementary Material. Future portable sequencing technologies for expeditions in future would strengthen the translational outlook of results and conclusions regarding acute changes of the GM.
Physiological Data Obtained During Fast Ascents to Different High Altitudes
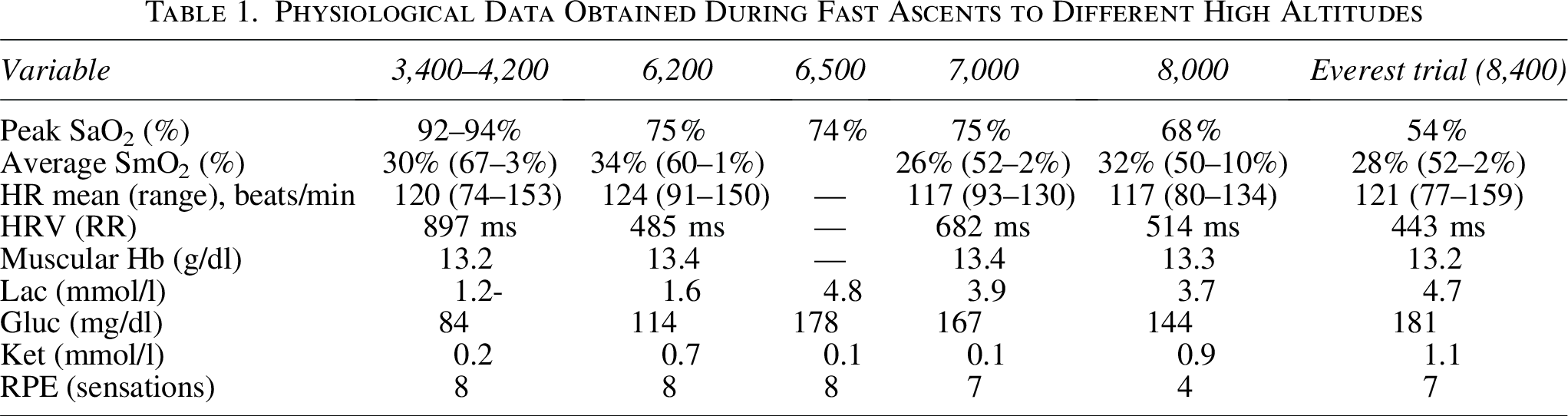
Peak SaO2 (%), HRV (RR intervals), muscular Hb (hemoglobin), Lactate (Lac), Glucose (Gluc), Ketones (Ket) showed the level achieved during the ascent at each peak altitudes. Average of SmO2 (muscular oxygen saturation) and heart rate (HR) indicates mean values of the complete ascents. Gluc, Glucose; HR, heart rate; HRV, heart rate variability; Hb, hemoglobin; Ket, Ketones; Lac, Lactate; SaO2, arterial oxygen saturation; SmO2, muscular oxygen saturation.
Results
Gut microbiota
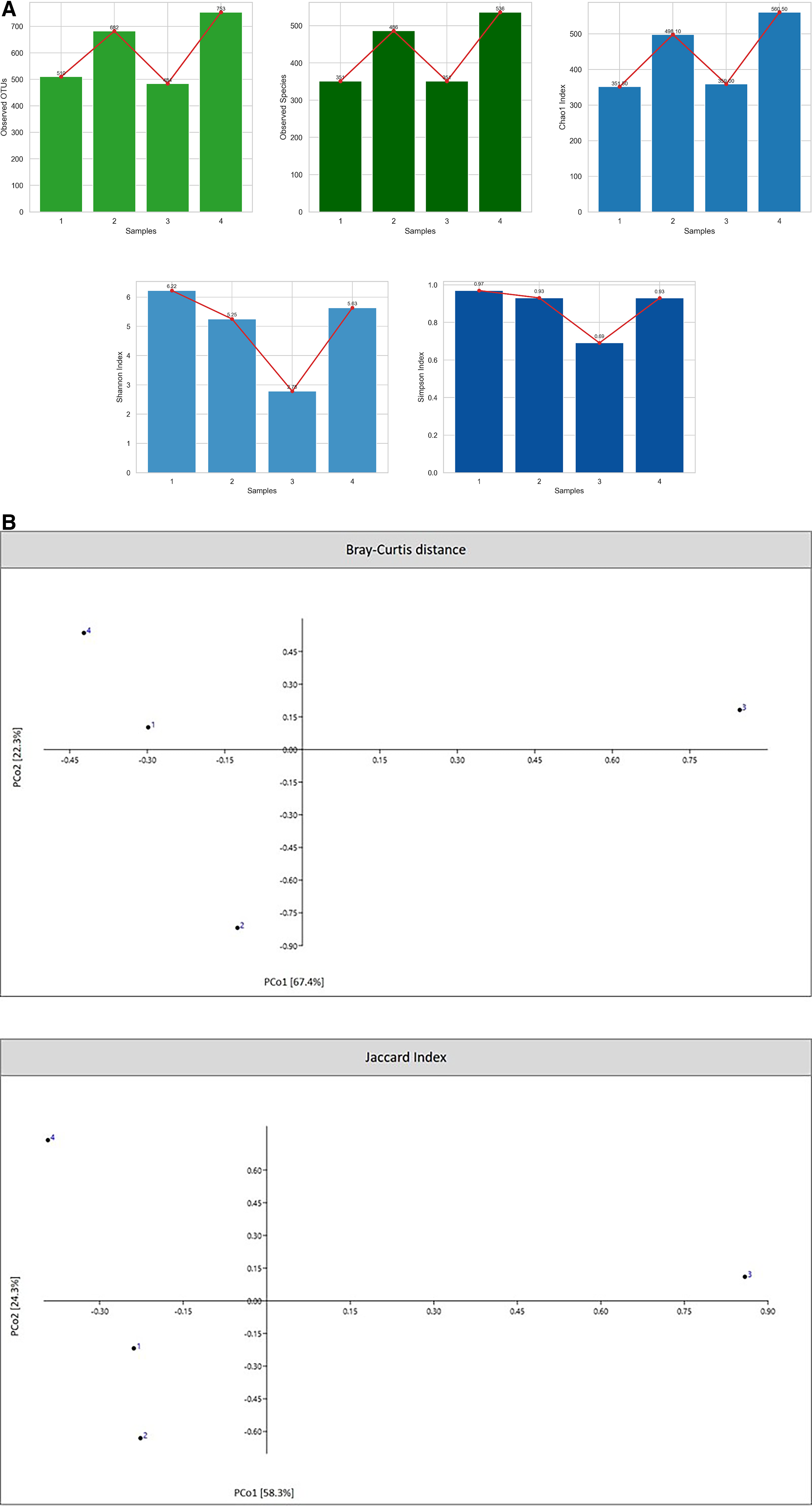
Alpha diversity (Shannon index) decreased progressively from baseline values (6.22) during the first 3 weeks of the expedition (5.25 and 2.78), but increased during the last week, coinciding with the Everest ascent attempt (5.63) (Fig. 2A). Other diversity index such as Simpson showed a similar trend for Shannon, while Chao1 increased on weeks 1 and 4 (Fig. 2A). The calculation of Bray-Curtis distance and Jaccard index showed that sample 3 was longer different on species distribution than other samples (Fig. 2B). The proportions of bacterial species changed over the 4-week period (Fig. 3).
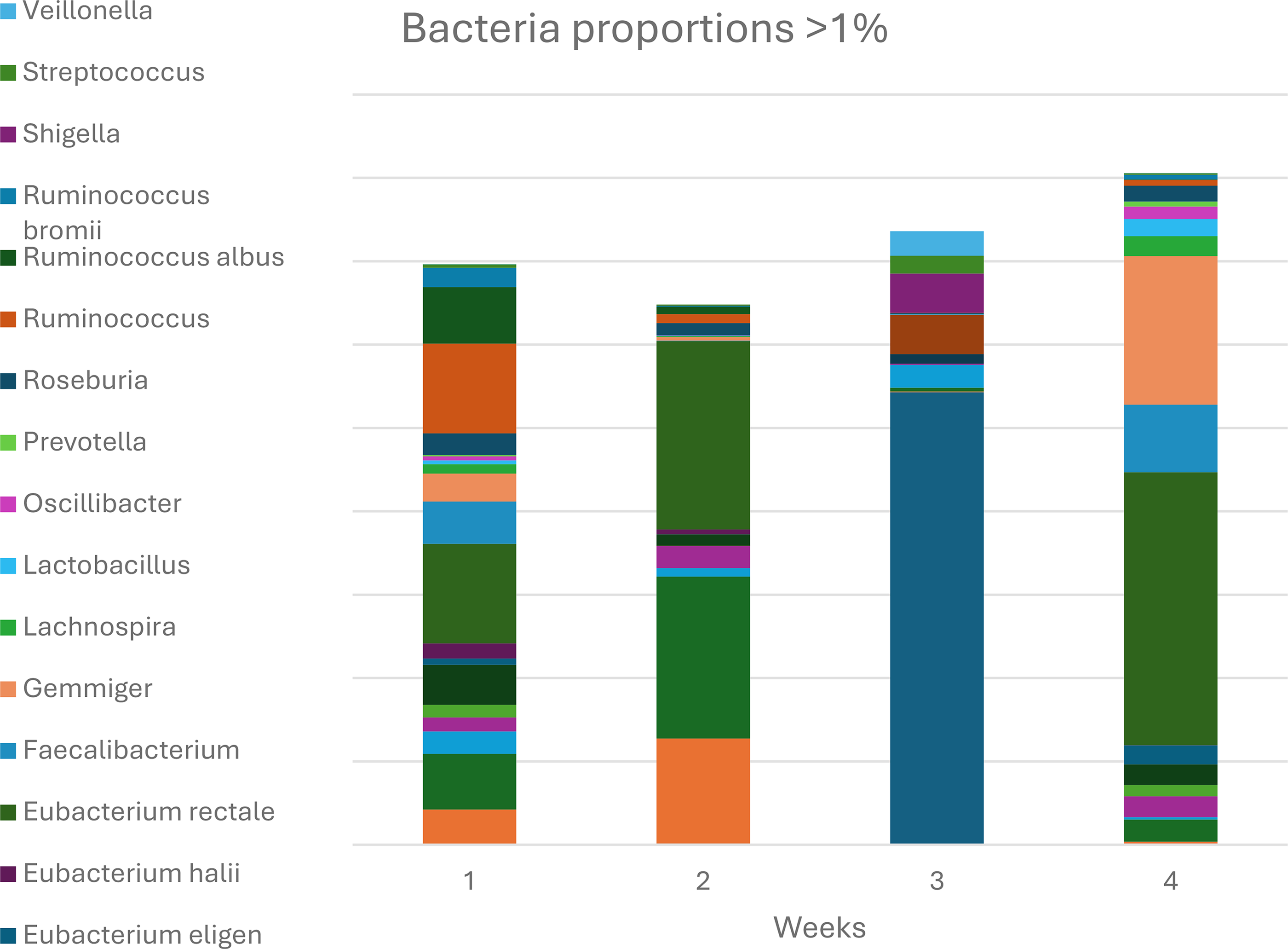
Bacteria proportions with more than 1% of the total gut microbiota sample.
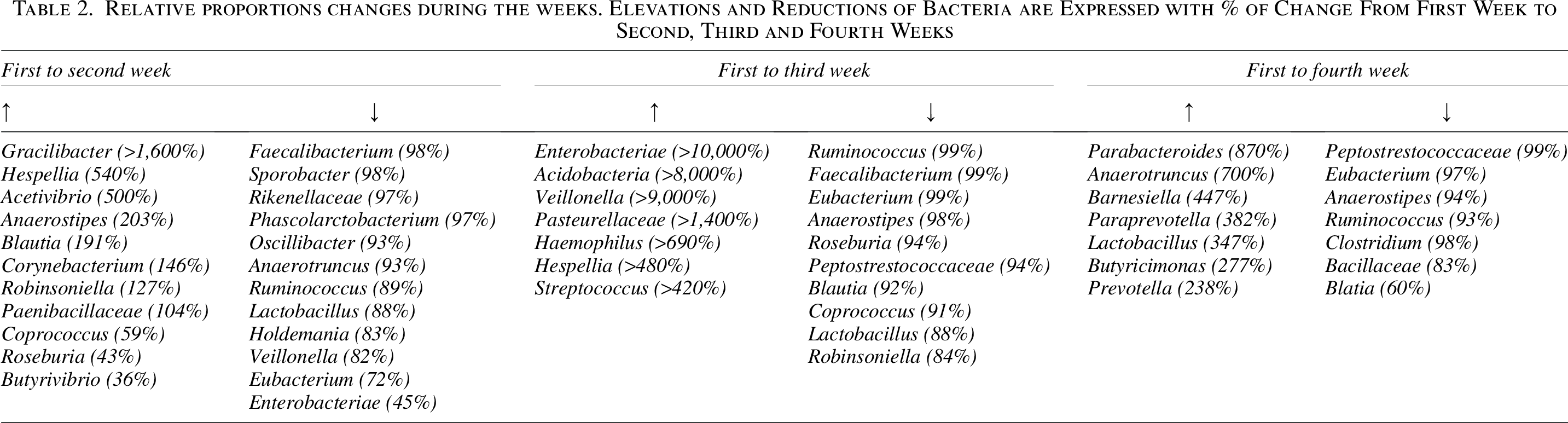
Coinciding with GI distress and respiratory viral symptoms during the third week both for GM diversity and specific bacterial species changed remarkably. The sickness symptoms were directly related to characteristic changes in the GM ecosystem and to a significant 2,800% increase of Ruminococcus gnavus from the previous week (Fig. 3). Notably, other pathogenic bacteria were also found to increase, such as Clostridium difficile, R. gnavus, Shigella spp., Salmonella enterica, Streptococcus, and/or Klebsiella pneumoniae. More beneficial bacteria were reduced or even eliminated (Table 2). During the last week, the health status improved, and the GC analysis showed an increase in alpha diversity and protective beneficial bacteria, for example, Faecalibacterium prausnitzii, Eubacterium rectale, Gemmiger spp., Blautia spp., or Coprococcus. More remarkably increases and decreases from sample 1 are presented in Table 2.
Relative proportions changes during the weeks. Elevations and Reductions of Bacteria are Expressed with % of Change From First Week to Second, Third and Fourth Weeks
Physiological performance
During the expedition, the athlete measured physiological parameters up to an altitude of 8,400 m (see Table 1).
Discussion
The results of the present exploratory study showed that exposure to extreme altitude and mountaineering for 4 weeks rapidly altered the GM profile. Thus, the progressive decrease in alpha diversity during the first 3 weeks of acclimatization may have contributed to elevating pathogenic bacteria and GM dysbiosis. During the third week, the greater decrease in GM diversity coincided with significant elevations of bacteria with potential pathogenicity such as strain of R. gnavus. Precisely this week, the athlete reported GI complications, diarrhea, fever, and discomfort reported by the athlete. Previous evidence suggests that exposure to high altitude may promote GI complaints in humans, including diarrhea, nausea, vomiting, anorexia, or even peptic ulcers without a clearly defined etiology (McKenna et al., 2022). One hypothesis described here relates to such complaints, involving GI complications associated with systemic hypoxia and changes in the GI ecosystem and gut leaky syndrome. The significant degree of intestinal ischemia produced at extreme altitudes affects intestinal barrier homeostasis with the growth of mucin degraders such as R. gnavus, exacerbating the leaky gut syndrome (Clark and Mach, 2023). To date, comprehensive studies have described the role of R. gnavus in various inflammatory diseases and particularly in athletes, which increases mucosal degradation (Clark and Mach). The epithelial barrier and mucosal layer act as a protective mechanism against the invasion of pathogens or toxins into the body (systemic endotoxemia), promoting low-grade inflammation and immune hyperactivation. Karl et al. (2018) showed an increase in intestinal permeability in a healthy group, physically active but unacclimatized men (n = 17), after a 22-day rapid exposure (air and car transport) at 4,300 m. The authors found increased permeability on days 1 and 18 of their exposure compared to sea level. In this context, Kleessen et al. (2005), during a 47-day expedition at 6,677 m, showed an increase in pathogenic bacteria at different periods of stay (day 12 to 5,200 m, day 15 to 5,500 m, and day 29 to 6,677 m) with a progressive decrease in Bifidobacteria species. Bifidobacteria adhere to the intestinal mucosa and prevent the proliferation of opportunistic bacteria (mainly Escherichia coli, Klebsiella spp., and Enterococcus spp.) that can break down the damaged biofilm and mucosal barrier, a phenomenon known as bacterial translocation (Liu et al., 2024). As GI complications disappeared and fitness recovered during the last week, GM diversity increased again, along with increases in commensal-positive bacteria (see Fig. 3). The change in short-chain fatty acid-producing bacteria may have enhanced obligatory anaerobic genera and increased their abundance in the gut, altering the GM and pH conditions. Changes of relative proportion comparing sample 1 (pre-) with the other 3 weeks confirmed the acute and rapid changes that severe hypoxia produced in GM diversity and specific bacteria (Table 2). Future validation in cohorts stratified by demographics (age, sex) and climbing experience would be necessary to assess the present exploratory results and probably compare with other climbers and native residents. However, the exceptional category of the athlete here analyzed makes the present results unique.
Conclusions
In conclusion, a healthy GM profile, characterized by elevated mucolytic bacteria and butyrate products, may improve hypoxic tolerance, reduce the risk of developing gut leakage syndrome and systemic endotoxemia, and protect against AMS. However, it would be of interest to include metabolomics analysis to quantify with precision metabolites from the GM. Therefore, taking into consideration the importance of maintaining a healthy GM before and during high altitude, acclimatization may improve successful performance on high-altitude expeditions.
Authors’ Contributions
J.A.-H.: Conceived the study, participated in its design and coordination, and drafted the article. A.O. and A.G.: Conducted genetic studies and participated in their analysis and draft. M.B.: Revised the article and helped draft the article. K.J.: Conceived the study, obtained biological samples and physiological data during the expedition, and helped draft the article. All authors have read and approved the final version of the article and agree with the authors’ presentation order.
Footnotes
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
The authors declare that they have no funding contribution.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.