
Abstract
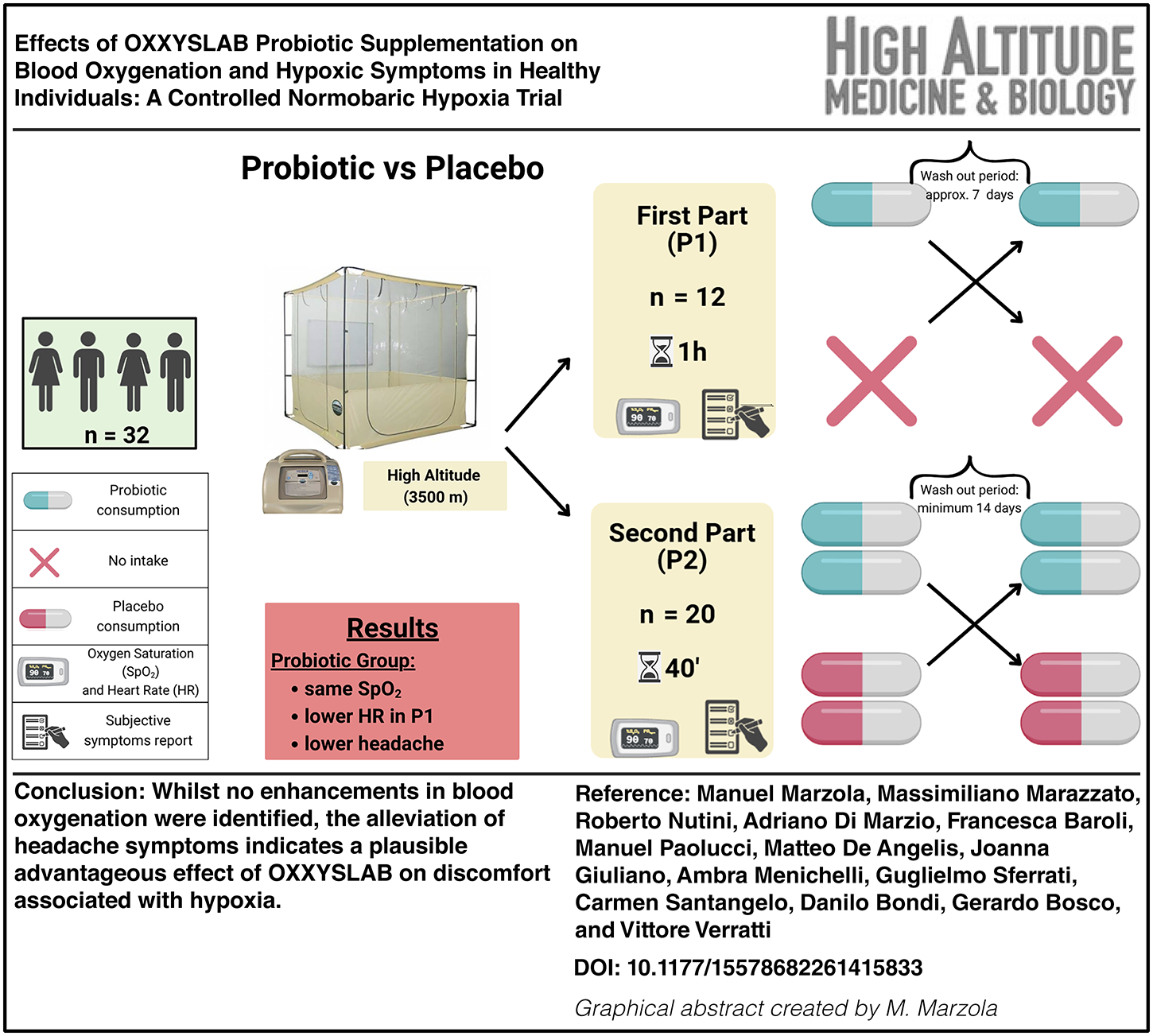
Marzola, Manuel, Massimiliano Marazzato, Roberto Nutini, Adriano Di Marzio, Francesca Baroli, Manuel Paolucci, Matteo De Angelis, Joanna Giuliano, Ambra Menichelli, Guglielmo Sferrati, Carmen Santangelo, Danilo Bondi, Gerardo Bosco, and Vittore Verratti. Effects of OXXYSLAB probiotic supplementation on blood oxygenation and hypoxic symptoms in healthy individuals: A controlled normobaric hypoxia trial. High Alt Med Biol. 00:00–00, 2026.
Background:
OXXYSLAB, a high-dose, multi-strain probiotic, has shown promise in pathological hypoxemia but remains untested under acute normobaric hypoxia (NH) in healthy volunteers. We evaluated whether OXXYSLAB alters peripheral oxygen saturation (SpO2) and alleviates hypoxia-related symptoms in healthy adults exposed to NH.
Methods:
In two randomized, double-blind, crossover phases, young adults were exposed to ∼13.5% inspired O2 for 1 hour (Phase 1: n = 12, 21.6 ± 1.3 years, body mass index [BMI] = 23.2 ± 2.8 kg/m2) or 40 minutes (Phase 2: n = 20, 21.7 ± 1.5 years, BMI = 22.9 ± 3.2 kg/m2). Participants received either a single (8 × 1011 colony-forming unit [CFU]) or double (1.6 × 1012 CFU) dose of OXXYSLAB or matched placebo in randomized order.
Results:
NH induced the expected SpO2 decrease (Phase 1: 90.0 ± 2.1%; Phase 2: 86.7 ± 2.9%), with no significant effect of probiotic supplementation on SpO2. In Phase 1, a trend toward lower heart rate (Δ = –3.2 bpm) under OXXYSLAB approached significance (p = 0.053); no effect was seen in Phase 2. Notably, headache incidence under probiotic conditions was reduced by 50% (Phase 1) and 62.5% (Phase 2) compared to placebo (p = 0.046 and p = 0.059, respectively).
Conclusion:
While OXXYSLAB did not enhance systemic oxygenation during acute NH, it significantly attenuated headache, a common symptom of hypoxia. Further research should assess its efficacy under prolonged or clinical hypoxemic conditions.
Graphical Abstract
Keywords
Introduction
At high altitudes, reduced barometric pressure lowers the partial pressure of inspired oxygen (O2), thereby decreasing its availability in the bloodstream and at the tissue level, a condition known as hypoxia (Palmer, 2010). Hypoxia can occur in two distinct ways: through reduced atmospheric pressure (hypobaric hypoxia [HH]) or by lowering the fraction of inspired oxygen (normobaric hypoxia [NH]) (Millet et al., 2012).
Exposure to hypoxia triggers complex physiological adaptations that involve endocrine, metabolic, and cardiovascular responses. These mechanisms help maintain oxygen supply to vital organs by increasing hormone activity (Verratti et al., 2017), optimizing metabolic efficiency (Tam et al., 2016), and adjusting body composition to enhance oxidative capacity (Bosco et al., 2019).
However, acute hypoxia, such as that experienced during sudden exposure to high-altitudes or simulated conditions, challenges the body’s ability to adapt effectively. Peripheral chemoreceptors detect decreased blood oxygenation within minutes, triggering compensatory mechanisms such as hyperventilation (Smith et al., 1986), sympathetic activation that increases heart rate (HR) (Hainsworth et al., 2007), and hypoxic pulmonary vasoconstriction, which elevates pulmonary artery pressure (Richalet et al., 2024). If oxygen delivery remains insufficient, symptoms of hypoxia-related stress emerge, with headache being one of the most frequent indicators (Schommer and Bärtsch, 2011).
Acute mountain sickness (AMS) is the most common disorder associated with acute exposure to moderate and high altitudes. It is primarily characterized by headache, which represents a key diagnostic criterion systematically included in standardized AMS assessment scales such as the Lake Louise. Other associated symptoms assessed in these scales include dizziness, nausea, and fatigue (Roach et al., 2018; Schommer and Bärtsch, 2011). The growing popularity of mountain tourism, high-altitudes sports, and hypoxia-based training has led to an increase in AMS cases. Despite extensive research, effective supplementation strategies to prevent AMS and mitigate hypoxia’s effects remain largely inconclusive (Karpęcka-Gałka and Frączek, 2024).
In pathological conditions associated with chronic hypoxia, such as COVID-19, the multi-strain probiotic OXXYSLAB (formerly SLAB51) has been shown to increase oxygenation markers, including partial pressure of oxygen, arterial (PaO2), O2Hb, and oxygen saturation, arterial (SaO2), when administered alongside standard treatment (Ceccarelli et al., 2021, 2020; d’Ettorre et al., 2020; Trinchieri et al., 2022). These findings suggest that OXXYSLAB may influence oxygen homeostasis via mechanisms additional to those classically involved in hypoxia adaptation.
The proposed mechanism of action relies on the probiotic’s ability to decrease intestinal oxygen consumption, thereby preserving more O2 for vital organs such as the brain, heart, and kidneys. This effect is achieved through two principal pathways: (1) reduced nitric oxide (NO) production, which induces vasoconstriction of intestinal microvessels and diminishes splanchnic blood flow, and (2) downregulation of enterocyte mitochondrial respiration, shifting cellular metabolism toward anaerobic glycolysis and further lowering local O2 demand (Ceccarelli et al., 2021). By modulating the hypoxia-inducible factor 1-alpha (HIF-1α) pathway, this promotes intestinal cell adaptation to low-oxygen conditions, shifting metabolism toward anaerobic energy pathways and sparing oxygen for systemic use (Lombardi et al., 2023). Recently, Yu et al. (2025) demonstrated in a double-blind, placebo-controlled trial at 3,800 m that supplementation with the same multi-strain OXXYSLAB formula enhanced systemic oxygen saturation (mean ΔSpO2 +3.6% daytime, +5.1% nocturnal) and significantly lowered AMS scores by 2.5 points; the authors associated these findings with HIF-1α stabilization and decreased intestinal O2 uptake.
Although these effects have been observed in disease states, it remains unclear whether OXXYSLAB can enhance oxygenation and mitigate hypoxia-related symptoms in healthy individuals under acute hypoxic conditions.
Study aims
This study aims to evaluate whether OXXYSLAB supplementation improves blood oxygenation and alleviates hypoxia-related symptoms in healthy individuals exposed to acute NH at sea level. Specifically, it investigates:
Can this specific probiotic improve systemic oxygen availability in the absence of disease? Does it reduce acute symptoms of hypoxia as headaches?
This study represents the first controlled investigation of OXXYSLAB’s efficacy under non‐pathological, acute normobaric hypoxic conditions, with possible implications for high‐altitudes adaptation, hypoxic training strategies, and performance optimization in low‐oxygen environments.
Methods
All participants signed an informed consent form. The study received approval from the local Ethics Committee (Comitato Etico delle Province di Chieti e Pescara, document no. 18, 29/07/2021). This single-center, crossover study included groups of 12 (gender-balanced, 21.6 ± 1.3 years, body mass index [BMI] = 23.2 ± 2.8 kg/m2) and 20 young adults (gender-balanced, 21.8 ± 1.5 years, BMI: 23.4 ± 3.0 kg/m2) who were, respectively, enrolled in the first part (P1) and second part (P2). To minimize potential bias, inclusion criteria required participants to be in good general health and to be permanent residents at sea level. Exclusion criteria included smoking, any history of cardiac or respiratory disease, exposure to altitudes within the previous year, and a prior diagnosis or symptoms of AMS. They were examined inside a tent associated with a hypoxic generator (Everest Summit II; Hypoxico, USA), with an oxygen air concentration of ≈13.5%, simulating an altitudes equivalent to 3,500 m, for 1 hour in P1 and 40 minutes in P2. Experiments were performed at an altitudes of ≈50 m. The hypoxic generator (Everest Summit II; Hypoxico) brings a continuous airflow (≈70–120 l/min) into the tent, ensuring constant air exchange and limiting CO2 accumulation. The tent is equipped with passive venting outlets, allowing exhaled air to exit continuously. The 13.5% oxygen level was adjusted manually to maintain a stable percentage within a 0.2% range. Throughout the experiment, the fraction of inspired oxygen (FIO2) was monitored through the oximeter associated with the system. Ambient temperature and relative humidity within the tent were recorded at 5-minute intervals by using a MeteoTracker portable station (IoTopon s.r.l., Italy).
Treatment consisted of consuming a blend of probiotic bacteria: a single dose (800 billion colony-forming unit [CFU]) for P1, a double dose (1600 billion CFU) for P2; control consisted of no intake in P1, or a placebo in P2 composed only of maltose. In P1, the treatment dose was taken 3–6 hours before the test. In P2 to standardize the intake timing, the two sachets of the probiotics or the placebo were administered on an empty stomach the first time 4 hours before the beginning of the experiment, 1 hour later the subjects were allowed to have breakfast, 3 hours before the experiment, while after an additional hour, they have taken a second dose of probiotics or placebo, 2 hours before the experiment (see Fig. 1 for a schematic representation of the study design in P2).
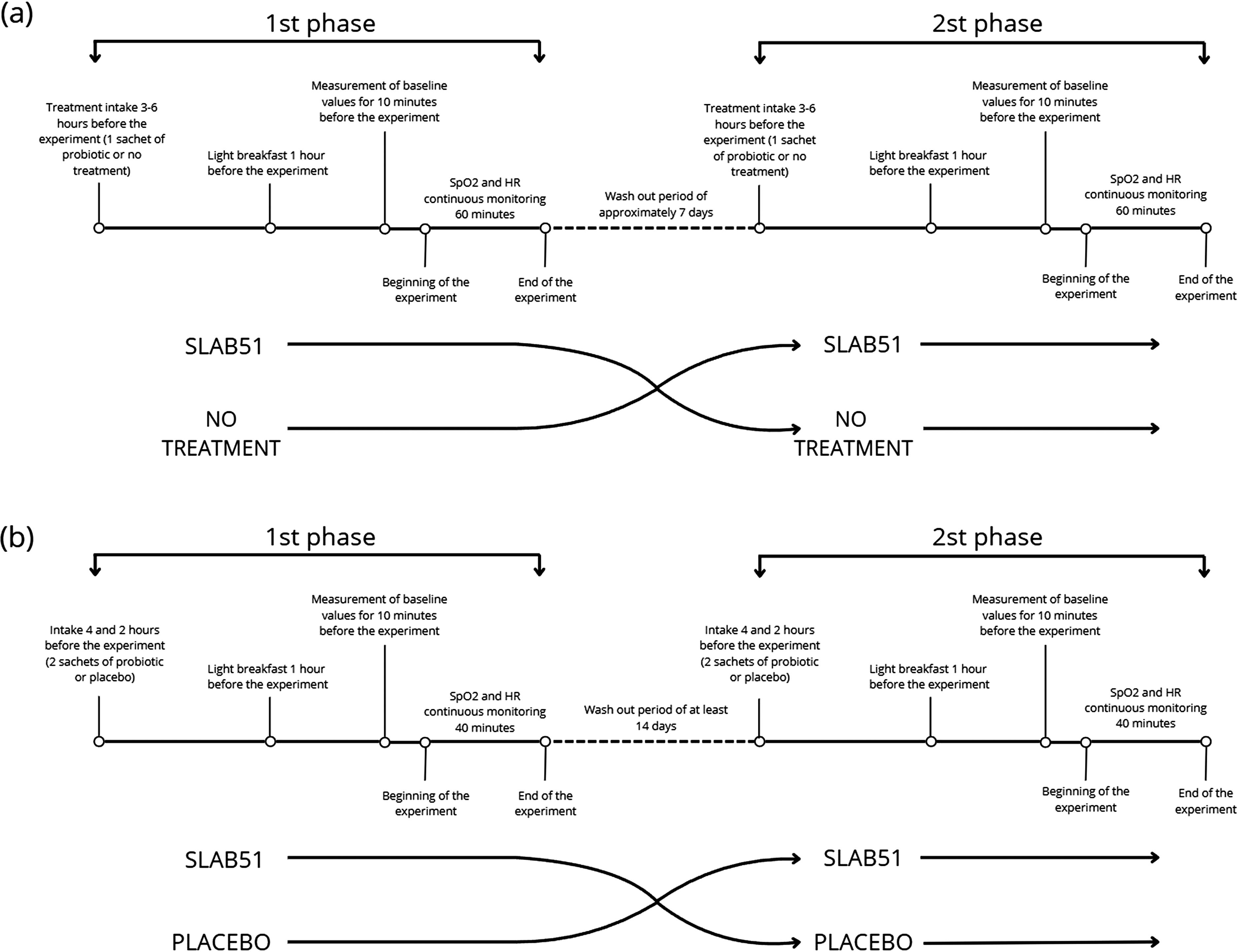
Schematic representation of the P1 and P2 study design. HR, heart rate; SpO2, oxygen saturation as measured by pulse oximetry;
The washout period between the two arms of the study was initially set to ∼7 days in P1; to reduce the possible persistence of strains in the gut, 14 days were put in P2 (Morelli and Pellegrino, 2021). For the same reasons, before the commencement of the study, all participants ceased personal probiotics intake and food-enriched strains.
The probiotic formula OXXYSLAB contains about 8 × 1011 live bacteria, comprising Streptococcus thermophilus CNCM I-5570, Lactobacillus acidophilus CNCM I-5567, Lactobacillus plantarum CNCM I-5569, Lactobacillus paracasei CNCM I-5568, Lactobacillus helveticus CNCM I-5573, Lactobacillus brevis CNCM I-5566, Bifidobacterium animalis subsp. lactis CNCM I-5571, and Bifidobacterium animalis subsp. lactis CNCM I-5572.
The participants were continuously monitored for blood oxygen saturation (SpO2) and HR by using finger pulse oximeters FS20F (Viatom Technology Co. Ltd, China). Baseline values were recorded 10 minutes before the test, and additional measurements were taken 5 minutes post-test to confirm the return to baseline levels. Subjective symptoms focused on headaches and related issues were documented during the test and in the following hours. Participants were asked to report the localization and perceived intensity of headache (classified as slight, moderate, or severe).
Statistical Evaluation
The minimum sample size in P1 and P2 was set to 12 and 20 subjects, respectively, by setting the alpha value of 0.05 and statistical power of 80%. The median values of SpO2 and HR for each recording were calculated. To determine any differences regarding SpO2 and HR in both groups, a paired-sample t-test was conducted. To determine differences in the presence of headache between the two groups, McNemar test was conducted. The p < 0.05 was considered statistically significant, and Edges’ g was used as effect size. The Shapiro–Wilk test and observation of the Q–Q plot were used as an assumption check.
For P1, median values of SpO2 and HR were calculated over the entire testing period, excluding the baseline values at the start and end of the tests. In P2, median values were derived from a 10-minute test segment in which the oxygen concentration was maintained at 13.5% to exclude periods where oxygen levels deviated from the intended hypoxia intensity.
Statistical analysis was performed using the R-based software Jamovi Version 2.3.21.0 (https://www.jamovi.org) and Prism Version 9 (GraphPad Software, San Diego, USA) to create graphs.
Results
In both P1 and P2, SpO2 decreased (90 ± 2.1 in P1 and 86.7 ± 2.9 in P2) in all participants exposed to hypoxia. According to several authors (Costello et al., 2020; Dünnwald et al., 2021), different values were recorded for SpO2 due to high inter-variability among subjects.
In P1, the treatment group showed similar SpO2 than the control group (control 90.1 ± 1.85% vs. treatment 90.3 ± 2.54%; p = 0.542, g = 0.070; refer to Graph 1 for detailed data), while HR resulted slightly reduced in the treatment group (79.6 ± 11.75 bpm vs. 74.9 ± 10.9 bpm; p = 0.053, g = 0.382). Similar results were obtained in P2 for SpO2 (control 86.8 ± 2.38% vs. treatment 86.7 ± 3.42%; p = 0.935, g = 0.018), while for HR no differences were found (control 85.2 ± 11.2 bpm vs. 84.8 ± 10.6 bpm; p = 0.862, g = 0.039; Fig. 2).
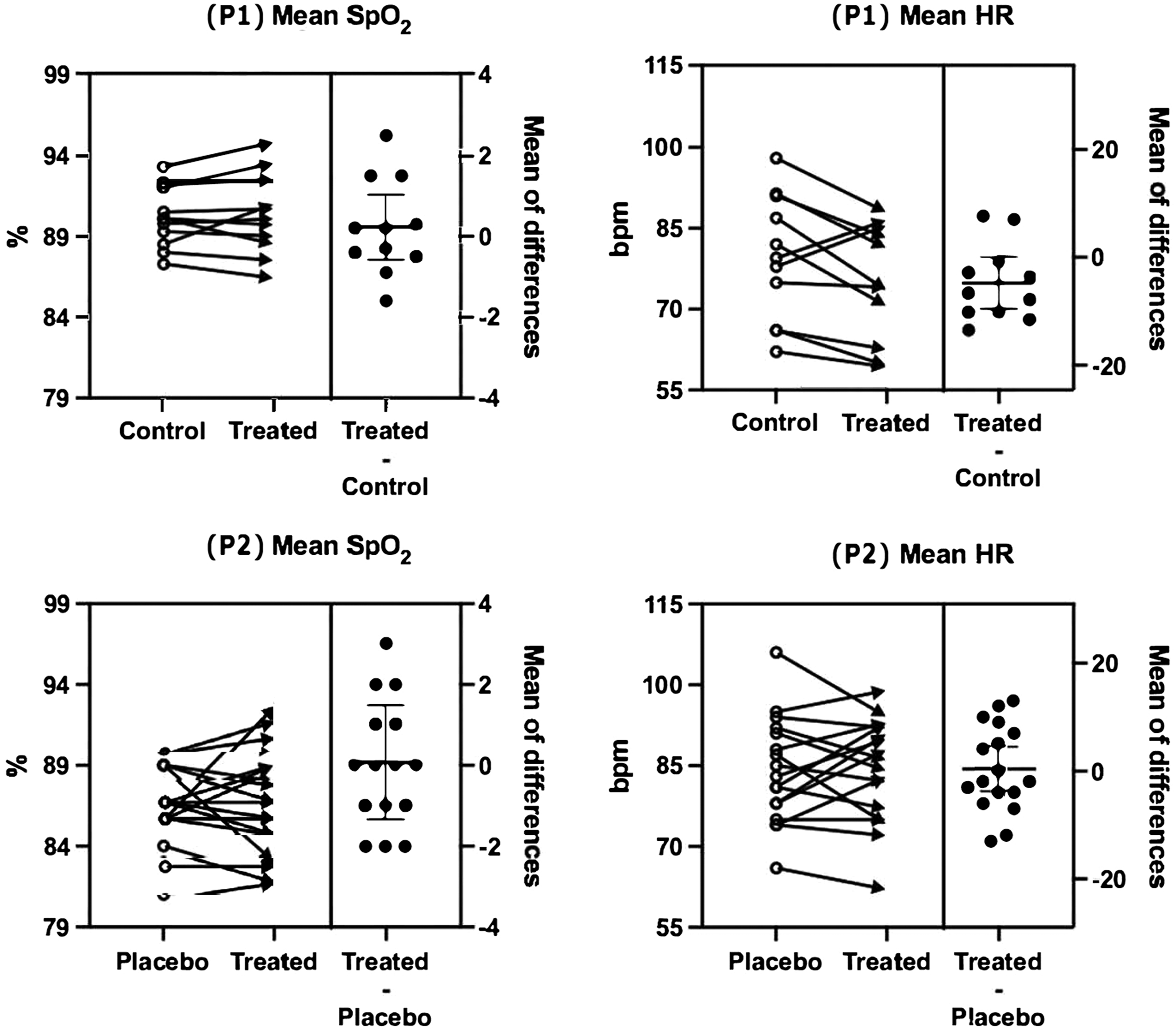
Mean SpO2 and HR during P1 and P2. P1, first part; P2, second part.
Participants in both conditions reported mild discomfort during the tests ascribable to hypoxia. The primary symptoms described were various forms of headache, with no reports of gastrointestinal issues or dizziness (see Table 1 for detailed data).
Symptoms Reported during first part and second part
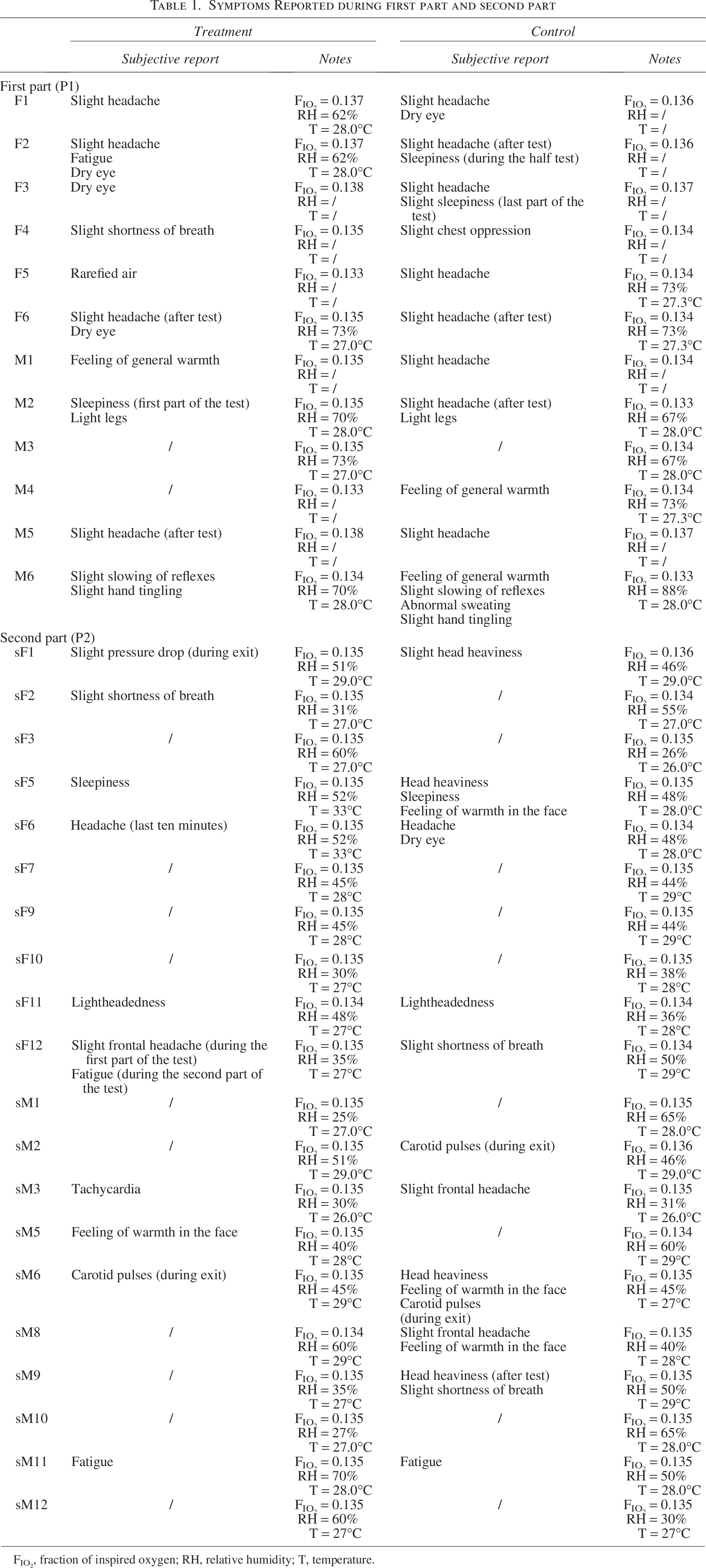
FIO2, fraction of inspired oxygen; RH, relative humidity; T, temperature.
The treatment was associated with a lower prevalence of headache and related symptoms. By considering headache as an umbrella term that included head heaviness and lightheadedness, in P1, the prevalence of headache decreased from 8 to 4 out of 12 participants, representing a 50% relative risk reduction (p = 0.046). In P2, the prevalence dropped from 8 to 3 out of 20 participants, corresponding to a 62.5% relative risk reduction (p = 0.059). Analyses stratified by sex showed a reduction in headache prevalence in both females and males in P1 and P2. In P1, headache prevalence decreased from 5 females and 3 males at the control to 3 females and 1 male after treatment. In P2, at the control, headache prevalence was distributed equally between sexes too (4 females and 4 males) and decreased after treatment to 3 females and no males (Fig. 3).
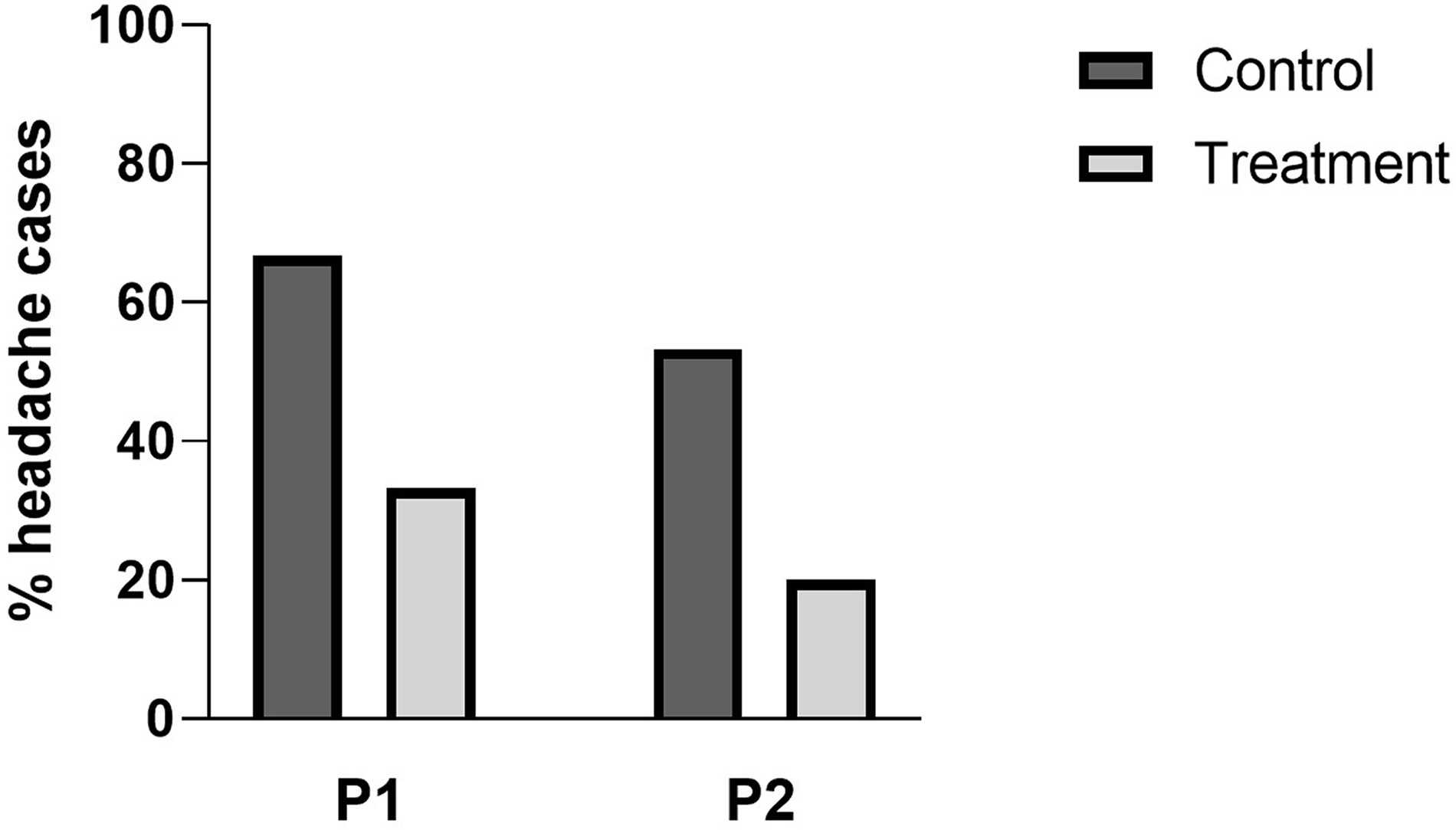
Percentages of headache cases in participants during Treatment and Control conditions in P1 and P2.
Discussion
OXXYSLAB is a multi-strain probiotic blend with high arginine deiminase activity (ADI), which plays a role in modulating Nitric Oxide Synthase 2 (NOS2), an enzyme responsible for producing NO from
Several clinical studies have provided evidence supporting the efficacy of OXXYSLAB in pathological conditions characterized by systemic hypoxia, particularly in COVID-19 patients. The addition of this probiotic to standard COVID-19 treatments has been correlated with significant increases in arterial oxygen levels (PaO2, O2Hb, and SaO2) and improved overall clinical outcomes (Ceccarelli et al., 2021, 2020; Trinchieri et al., 2022). These findings suggest a potential protective effect against physiological desaturation in individuals exposed to hypoxic environments, such as high altitudes.
The present study was designed to assess the effects of OXXYSLAB on oxygen saturation in healthy individuals under acute hypoxic conditions. To ensure consistency and control over external variables, an NH model was employed using a hypoxic tent to simulate an oxygen concentration of ≈13.5%. This approach was intended to standardize participants’ physical effort and exposure conditions.
This study represents the first controlled trial testing OXXYSLAB in healthy adults under a simulated hypoxic environment. A two-phase crossover design was implemented to confirm findings and strengthen methodological reliability. The absence of a placebo in the control group during P1 could have introduced a psychological bias (Margo, 1999), possibly leading to a more relaxed physiological state in the probiotic-treated group, thereby reducing sympathetic activation and HR.
The most notable effect observed was a reduction in headache prevalence during hypoxia exposure: 50% in P1 and 62.5% in P2 among participants treated with OXXYSLAB. However, there was no significant increase in SpO2 in the treatment group compared to controls. These findings suggest that while probiotics may not directly enhance systemic oxygenation in healthy individuals, they could provide symptom relief during hypoxic stress.
Headache is a common symptom of AMS and high-altitudes exposure. Although AMS could not be fully evaluated in this study due to the short duration of hypoxia exposure (Debevec and Millet, 2014; Roach et al., 2018), headache incidence was assessed as a relevant surrogate marker. Hypoxia-induced headaches are primarily mediated by perivascular nociceptor sensitization (RAY and WOLFF, 1940), which is exacerbated by mechanisms such as increased NO levels, neurogenic inflammation, and the release of pro-inflammatory mediators (Britze et al., 2017). While previous studies have reported the onset of headache after 2–6 hours of NH (Broessner et al., 2016), symptoms can also occur within the first hour owing to several physiological responses. In particular, global cerebral blood flow has been shown to increase rapidly during early hypoxia exposure, accompanied by elevations in oxidative stress markers that are consistent with cephalalgia pain (Morris et al., 2017; Roach et al., 2011).
Although the role of headache in defining AMS positivity is still debated (Roach et al., 2011; West, 2011), it is still considered the key symptom for determining the presence or absence of the condition.
The observed decline in headache symptoms within the OXXYSLAB-treated cohort indicates a plausible impact on the oxidative stress response. This aligns with previous findings indicating that OXXYSLAB can enhance antioxidant enzyme activity via the SIRT1 pathway, a regulatory mechanism involved in oxidative stress and inflammation (Bonfili et al., 2018). If OXXYSLAB mitigates hypoxia-related symptoms without significantly altering SpO2, its mode of action may be independent of direct oxygen redistribution, instead functioning through secondary metabolic or neuroprotective pathways. However, without direct biomarkers for inflammation and oxidative stress, this hypothesis remains speculative. It was also demonstrated that moderate physical activity at low altitudes enhances immune defenses and reduces cellular stress, whereas at high altitudes, the immune response appears weaker. This suggests a potential protective effect of exercise against hypoxia, further highlighting the importance of complementary strategies, such as probiotics, to support adaptation (Morabito et al., 2016). Future studies should include systemic markers (e.g., cytokine levels, oxidative stress markers) to validate this mechanism.
Although the differences between NH and HH diminish over time, short-term NH studies may underestimate the true physiological adaptations that occur at high altitudes. Previous research has demonstrated that NH elicits different metabolic and subjective responses compared to HH (Coppel et al., 2015; Millet et al., 2012; Richalet, 2020; Richard and Koehle, 2012). Specifically, NH leads to higher SpO2 and arterial oxygen levels than HH during acute exposure and triggers smaller respiratory and cardiovascular adaptations over prolonged exposure. Although the differences between NH and HH diminish over time, short-term NH studies may underestimate the true physiological adaptations observed at high altitudes.
Given that SLAB51/OXXYSLAB demonstrated significant effects in patients with hypoxia-related conditions (Baldassarre et al., 2023; Ceccarelli et al., 2021, 2020; d’Ettorre et al., 2020; Trinchieri et al., 2022), it is plausible that the hypoxic dose and exposure duration in this study were insufficient to activate the oxygen-sparing mechanism and that the effects of OXXYSLAB become more evident in individuals with chronic or severe oxygen deprivation.
Limitations
Several limitations must be acknowledged. Short hypoxia exposure (1 hour or 40 minutes): This time frame may not have been sufficient to induce the metabolic shifts required for oxygen redistribution. Likewise, a single acute administration of the probiotic might not have allowed enough time for microbial or metabolic modulation to occur. CO2 levels were not monitored; therefore, we cannot exclude that slight hypercapnia occurred during the experiments. Using NH instead of HH may have affected the results; future studies should investigate whether OXXYSLAB produces more pronounced effects in real high-altitudes conditions or under prolonged hypoxia. Lack of inflammatory and oxidative stress biomarkers prevents a definitive conclusion on whether the headache reduction is due to neuroinflammatory modulation rather than direct oxygen sparing. Another limit relies on placebo inconsistency: In P1, the control group did not receive a placebo, and in P2, the placebo formulation differed in shape, form, and taste from the probiotic, which could have biased participant responses.
Conclusions
This study provides the first controlled evaluation of OXXYSLAB in healthy individuals exposed to acute hypoxia. While no direct improvements in blood oxygenation were observed, the statistically significant reduction in P1 and the borderline statistically significant reduction in P2 regarding headache symptoms suggest a potential beneficial effect on hypoxia-induced discomfort.
The absence of measurable changes in SpO2 indicates that the probiotic’s oxygen-sparing effect may require prolonged exposure or be more pronounced in individuals with preexisting hypoxic stress. Furthermore, the absence of a net SpO2 benefit in our normobaric model may reflect fundamental differences between hypobaric and reduced-FIO2 hypoxia, as dissected by Yu et al. (2025); future work should directly compare HH versus NH paradigms to unravel these mechanistic nuances. Given that previous studies have reported positive outcomes in patients with chronic hypoxia (Ceccarelli et al., 2021), future research should incorporate extended-duration hypoxia models (exceeding 24 hours) to evaluate long-term metabolic adaptations, as well as high-altitudes hypobaric conditions to more accurately replicate real-world environmental exposures, biomarkers of oxidative stress and inflammation to confirm secondary mechanisms of action, and larger sample sizes to improve statistical power and confirm the observed trends.
Although OXXYSLAB did not improve systemic oxygenation in this setting, its potential role in alleviating hypoxia-related symptoms remains promising, particularly for individuals at risk of AMS or hypoxia-induced inflammatory responses. Future studies should refine the experimental design to better capture the full spectrum of the probiotic’s physiological effects.
Authors’ Contributions
M.Marzola.: Formal analysis; investigation, resources, data curation, writing—original draft, visualization, and project administration. M.Marazzato.: Conceptualization, methodology, and resources. R.N., A.D.M., F.B., M.P., M.D.A., J.G., A.M., G.S., and C.S.: Investigation. D.B.: Methodology, formal analysis, and project administration. G.B.: Conceptualization. V.V.: Conceptualization, methodology, supervision, and project administration. All authors have read and approved the final version of the article and agree to be accountable for all aspects of the work.
Footnotes
Author Disclosure Statement
The study was carried out without any financial or commercial ties that might be interpreted as a conflict of interest, according to the authors.
Funding Information
No specific grant from a public, private, or nonprofit funding organization was received for this study.
Data Availability
The data that support the findings of this study are available from the corresponding author, Manuel Marzola, upon reasonable request.