
Abstract
Chen, Biao, Shuai Li, Kun He, Dunzhu Basang, Yuzhen Suolang, Fang Li, Jiangcun Silang, Hongyuan Yi, Langjie Jinmei, La Dan, Deqing Ciren, Haifeng Xu, and Dong Wu. Mitigating Intraoperative Fatigue in Surgeons at High Altitude: A Stepped-Wedge Cluster Randomized Trial. High Alt Med Biol. 00:00–00, 2026.
Background:
Both genetically adapted Tibetan surgeons and less-acclimatized Han surgeons deployed through the Aid-Tibet medical aid program face significant challenges from hypobaric hypoxia in the Qinghai-Xizang Plateau. Hypoxia is known to impair cognitive functions and induce fatigue, threatening surgical performance and patient safety. Traditionally, surgeons in Tibet consume Coca-Cola to combat fatigue, a potentially harmful practice lacking in scientific basis. Supplemental oxygen, recommended for better cerebral oxygen delivery, is underutilized. This study compares supplemental oxygen versus Coca-Cola in mitigating intraoperative fatigue among surgeons in Tibet, considering the influence of long-term high-altitude adaptations.
Methods:
We conducted a stepped-wedge cluster randomized controlled trial at the People’s Hospital of Xizang Autonomous Region in Lhasa (3,650 m altitude). Twenty-two surgeons (11 Han, 11 Tibetan) performed 24 surgeries each, receiving either 100 ml of Coca-Cola every 30 minutes or continuous 2 l/min supplemental oxygen via nasal cannula. Cognitive fatigue was assessed using the d2 Test of Attention, and physical fatigue was measured using a dynamometer, before and after surgeries. The primary outcome was change in concentration performance (ΔCP). The secondary outcome was the change in maximum voluntary contraction force (ΔMVC). Data were analyzed using a linear generalized estimating equations model.
Results:
All 22 surgeons completed 528 surgeries. Generally, supplemental oxygen significantly reduced cognitive fatigue compared to Coca-Cola (ΔCP: 6.08, 95% confidence interval [CI]: 1.37–10.80, p = 0.012). In subgroup analysis, oxygen significantly lowered cognitive fatigue in Han surgeons (ΔCP: 7.06, 95% CI: 0.72–13.40, p = 0.029), while the effect in Tibetan surgeons did not reach statistical significance (ΔCP: 4.82, 95% CI: −0.51–10.16, p = 0.076). No significant difference was observed in physical fatigue (ΔMVC: −0.18, 95% CI: −1.77–1.40, p = 0.822).
Conclusions:
Supplemental oxygen outperforms Coca-Cola in reducing cognitive fatigue during high-altitude surgery, especially for less-acclimatized Han surgeons, supporting its adoption to enhance surgeons’ performance and well-being.
Introduction
The Chinese government has prioritized Tibet’s healthcare capacity and accessibility through various policies, including the Aid-Tibet medical aid program, which deploys medical talents from across the nation to work along with local Tibetan staff for 1∼3 years. A primary occupational challenge for the Tibet surgical workforce, including both Tibetan surgeons and Han surgeons, is the high-altitude environment, where hypobaric hypoxia profoundly impacts cognitive and physical function, inducing fatigue (Chen et al., 2023). Surgeon fatigue is a well-documented issue in medical practice, threatening patient safety and surgeon well-being (Whelehan et al., 2021; Reijmerink et al., 2024). Despite global interest in Tibet, limited research has focused on the physical challenges faced by surgeons in this environment (Systermans and Stokes, 2019).
To combat intraoperative fatigue, surgeons in Tibet traditionally consume Coca-Cola, a sugar-sweetened beverage (SSB) containing caffeine, a practice that began after Coca-Cola’s return to China in the 1980s. This practice, reflecting high SSB consumption patterns in the region, is believed to provide a temporary energy boost, potentially via caffeine’s antagonism of adenosine receptors (Ishak et al., 2012; Smirmaul et al., 2017). Thus, some travel guidelines also suggest Coca-Cola to alleviate altitude sickness symptoms. However, the scientific basis for this practice is lacking, and frequent high-sugar beverage consumption may cause other detrimental impacts (Qiu et al., 2024; Reed et al., 2022; Zhang et al., 2022).
Alternatively, studies have demonstrated supplemental oxygen therapy, via room oxygen enrichment systems or nasal cannulas, can mitigate fatigue by improving cerebral oxygen supply. This approach is increasingly accessible in Tibet due to improved medical resources and recommended by experts (Crowley et al., 1992; Falla et al., 2024; Heinrich et al., 2019).
Nevertheless, most surgeons in Tibet have not adopted supplemental oxygen as an alternative to Coca-Cola due to limited direct evidence supporting its efficacy in alleviating surgical fatigue. This study compares the efficacy of supplemental oxygen versus Coca-Cola in reducing intraoperative fatigue among surgeons in Tibet. We hypothesize that supplemental oxygen will be more effective. Additionally, we explore how high-altitude adaptations influence intervention effectiveness, using ethnicity as a proxy to distinguish genetically adapted natives from less-acclimatized residents.
Methods
Study design and participants
This study is a stepped-wedge cluster randomized controlled trial (SW-CRT) conducted at the People’s Hospital of Xizang Autonomous Region (PHXAR; altitude ∼3,650 m). Eligible participants were surgeons capable of performing surgeries lasting over 2 hours as primary surgeons and who had worked continuously in Lhasa for at least 3 months. Surgeons with medical conditions precluding participation were excluded. Participants were identified through work schedules and surgical timetables. The cohort included both Tibetan and Han Chinese surgeons to investigate potential ethnic differences in intervention efficacy. An in-hospital recruitment meeting was held to emphasize voluntary participation and the right to withdraw. The study is approved by the Medical Ethics Committee of the PHXAR (ME-TBHP-24-019) and registered with ClinicalTrials.gov (NCT06557746). All participants provided written informed consent.
Randomization and masking
Randomization of the intervention switch points in this SW-CRT was conducted by an independent methodologist using a computer-generated sequence in R software (R Foundation for Statistical Computing, Vienna, Austria). Due to the distinct delivery methods of the interventions (oral Coca-Cola consumption vs. oxygen inhalation via nasal cannula), blinding of participants and surgical staff was not possible. To minimize bias, outcome assessors and data analysts were blinded to intervention allocation.
Procedures
Clinical research staff recruited participants, collecting demographic information (including ethnicity), prior oxygen use, Coca-Cola and coffee consumption frequency, and work schedule details at enrollment. In this trial, 22 participants each performed 2 surgeries across 12 time periods, switching from Coca-Cola (control) to supplemental oxygen (intervention) at randomized intervals. As this study employs a Stepped-Wedge Cluster Randomized Trial (SW-CRT) design, the intervention progresses unidirectionally over time. Specifically, all clusters begin in the control phase (Coca-Cola) and transition to the intervention phase (oxygen) at randomly assigned, staggered time points. In the control condition, participants consumed 100 ml of Coca-Cola every 30 minutes during surgery, delivered in a sterile cup by a trained nurse. In the intervention condition, participants received continuous oxygen at 2 l/min via nasal cannula using a portable oxygen concentrator. Interventions are administered during each surgeon’s first afternoon surgery to control circadian effects. Data were collected over 24 weeks by trained research assistants in a standardized hospital setting.
Outcomes
The primary outcome was the change in concentration performance (ΔCP) score on the d2 Test of Attention, a validated measure of sustained attention and processing speed, assessed pre- and post-surgery (Amirian et al., 2014; Bates and Lemay, 2004; Brickenkamp and Zillmer, 1998; Dorion and Darveau, 2013). Participants completed the paper-based test immediately before and after each surgery. The secondary outcome was the change in maximum voluntary contraction force (ΔMVC), measured using a hand dynamometer (Vøllestad, 1997). Grip strength was assessed in triplicate pre- and post-surgery, with the highest value recorded.
Sample size calculation
The sample size was calculated to detect a 20-point difference in ΔCP (standard deviation [SD] = 52.55) between interventions, with 90% power and a 5% significance level (Bates and Lemay, 2004; Amirian et al., 2014). A design effect of 1.79 was applied to account for the SW-CRT design (intracluster correlation coefficient = 0.01), following methods by Hemming et al. (Hemming et al., 2016). With 22 surgeons (k = 22), each performing 2 surgeries (m = 2) across 12 stepped time periods (t = 12), a total of 528 surgeries (k × t × m) were required.
Statistical analysis
This study followed the intention-to-treat principle, including all randomized participants in the outcome analysis. Baseline characteristics of surgical procedures in the supplemental oxygen and Coca-Cola groups were summarized as means ± SD or median (25th percentile, 75th percentile). Clinically relevant differences, if identified, were adjusted in outcome analyses.
The primary outcome, ΔCP from the d2 Test of Attention, was analyzed using a linear generalized estimating equations (GEE) model, with ΔCP as the dependent variable and intervention group (supplemental oxygen vs. Coca-Cola) as the key independent variable. The model included a categorical time period variable, the intervention-time interaction, and accounted for clustering by surgeon. The correlation structure was selected based on the lowest Quasi-likelihood Information Criterion (QIC). If the time–intervention interaction was not significant (p > 0.05), it was removed, retaining only main effects. Statistical significance was set at p < 0.05. To quantify the magnitude of the intervention’s impact, the effect size was estimated using Cohen’s d, calculated as the mean difference in ΔCP scores divided by the pooled standard deviation. The secondary outcome (ΔMVC) was analyzed using a similar GEE model.
A prespecified key subgroup analysis explored heterogeneity in intervention effects based on high-altitude acclimatization status. For this purpose, ethnicity was utilized as a physiological proxy for acclimatization. Specifically, native Tibetan surgeons represented a genetically adapted population with evolutionary hypoxia tolerance, whereas Han surgeons—who relocated to Tibet for 1–3 years under the medical aid program—represented a less-acclimatized population relying on physiological compensation. We hypothesized that supplemental oxygen would yield more pronounced benefits for the less-acclimatized Han surgeons. This analysis included the main effect of ethnicity (as a proxy for acclimatization) and its interaction with the intervention in the GEE model. Separate GEE models were fitted for each ethnic group, reporting effect sizes and 95% confidence intervals. Additional exploratory subgroup analyses examined baseline oxygen use and Coca-Cola or coffee consumption frequency. No Type I error control was applied to subgroup analyses or secondary outcomes, and results were interpreted as exploratory. All analyses were performed in R (version 4.5.0).
Results
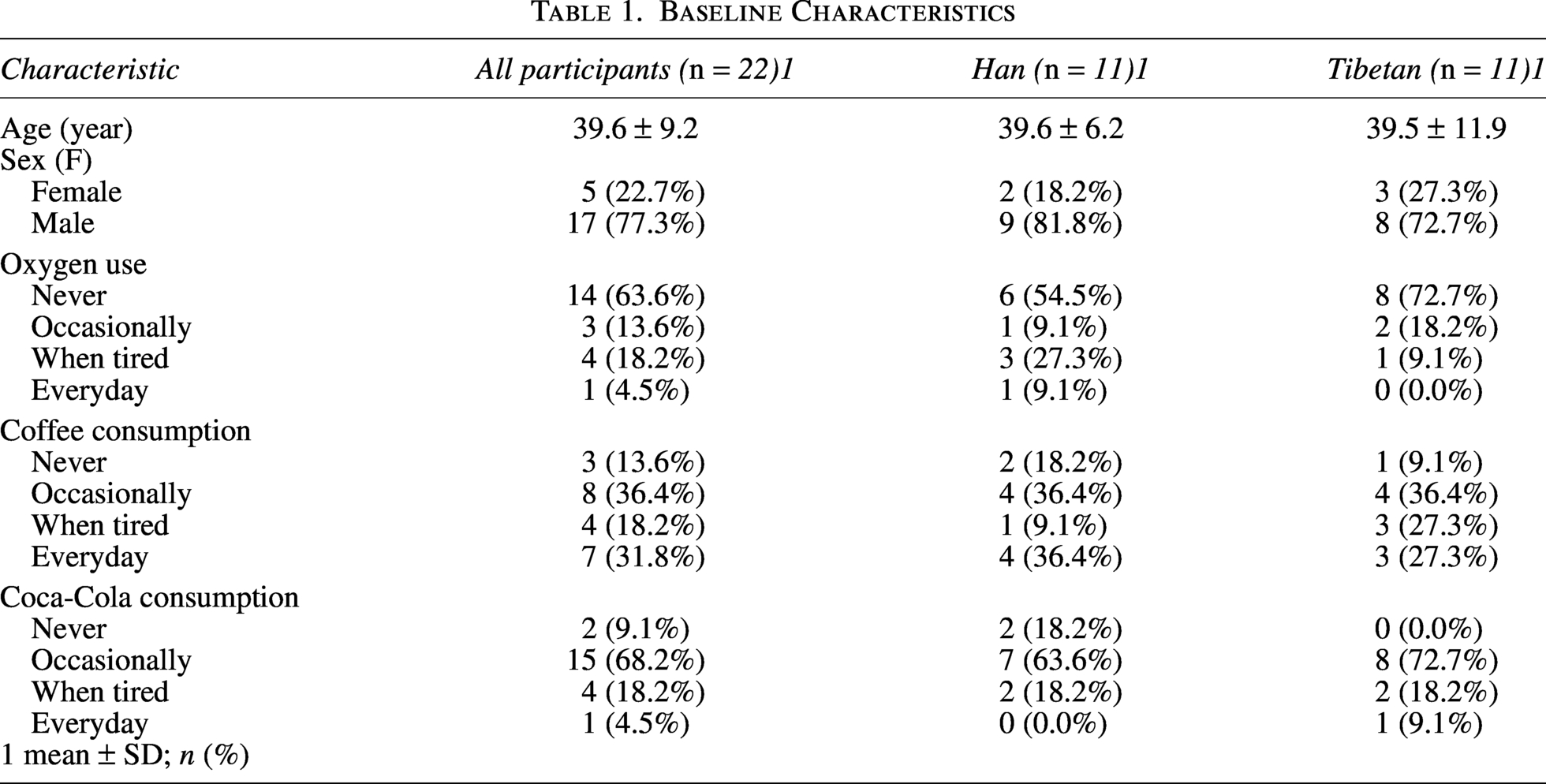
From December 2024 to March 2025, 22 surgeons (11 Han, 11 Tibetan) were recruited from the PHXAR. The cohort had a mean age of 39.6 ± 9.2 years, with 77.3% (17/22) male. Baseline characteristics, including prior oxygen use, coffee consumption, and Coca-Cola consumption, were balanced between ethnic groups (Wilcoxon rank-sum test; Table 1).
Baseline Characteristics
Each surgeon was assigned to a cluster in the SW-CRT design and transitioned from Coca-Cola to supplemental oxygen at randomized intervals across 12 time periods (Fig. 1). All 22 surgeons completed 24 surgeries each, yielding data for 528 operations with no dropouts or missing data.
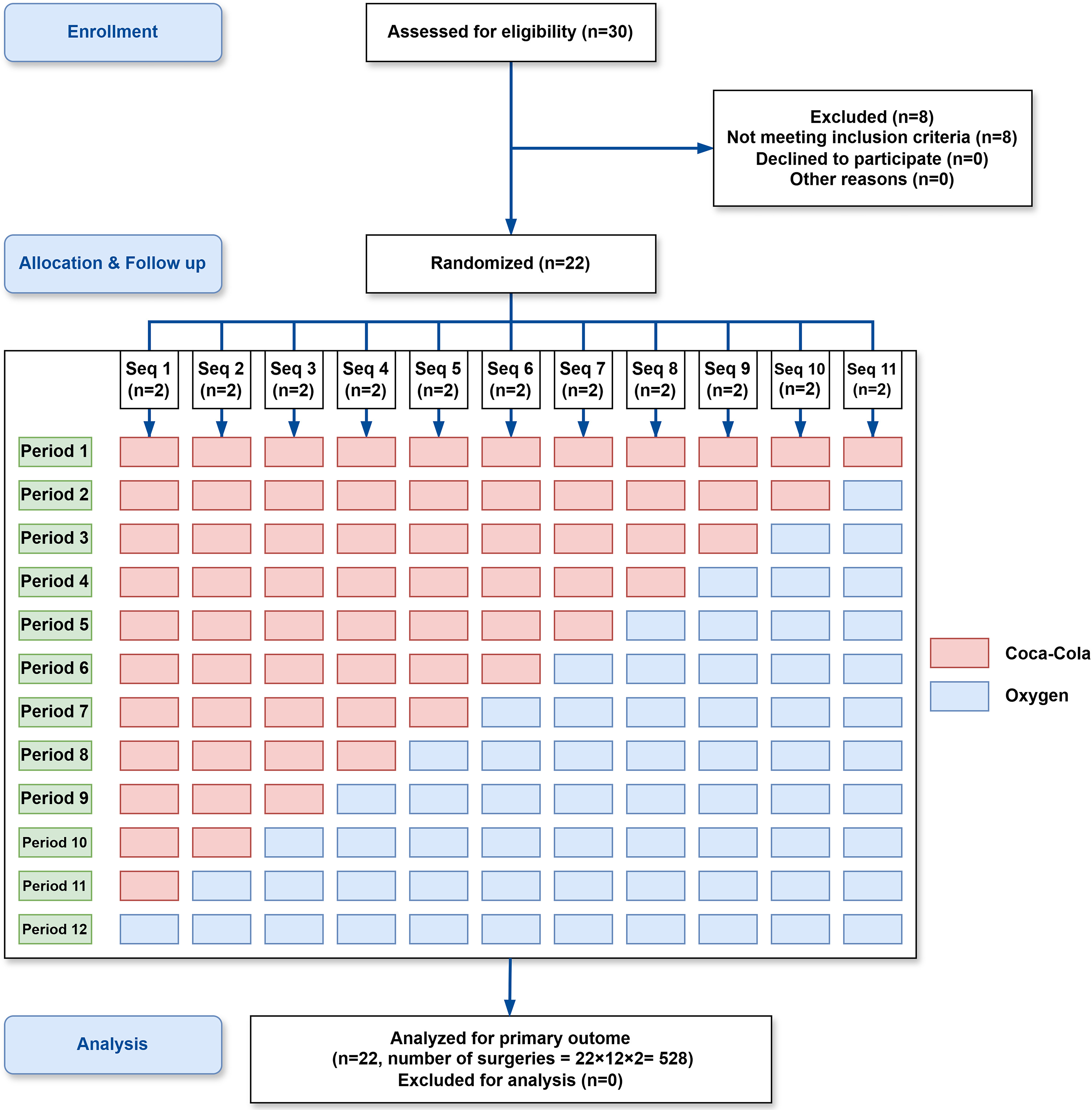
Consolidated Standards of Reporting Trials Diagram of the Stepped-Wedge Cluster Randomized Clinical Trial A total of 30 surgeons were assessed for eligibility, with 22 successfully randomized into 11 sequences (n = 2 surgeons per sequence). The trial was conducted across 12 time periods. Red cells represent the control condition (Coca-Cola), and blue cells represent the intervention condition (supplemental oxygen). Each sequence switched unidirectionally from the control to the intervention phase at randomized, staggered intervals. All 22 surgeons completed the full sequence, contributing a total of 528 surgeries (n = 22 surgeons × 12 periods × 2 surgeries per period) for the intention-to-treat analysis.
Primary outcome: ΔCP
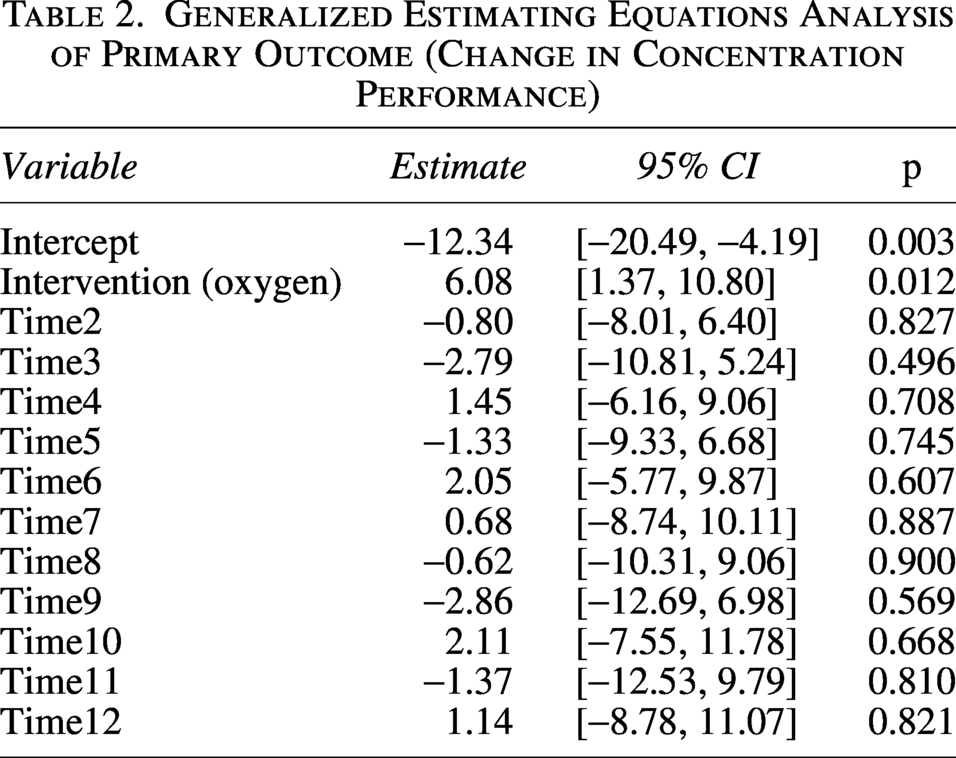
The primary outcome, ΔCP, was analyzed using a GEE model, adjusting for intervention (supplemental oxygen vs. Coca-Cola), time periods, and clustering by surgeon. An independent correlation structure was selected based on the lowest QIC. The time–intervention interaction was excluded due to model convergence issues, ensuring analytical stability.
Supplemental oxygen significantly reduced cognitive fatigue compared to Coca-Cola (ΔCP estimate: 6.08, 95% confidence interval [CI]: 1.37–10.80, p = 0.012; Table 2), indicating less concentration decline post-surgery. This 6.08-point absolute improvement in the CP score corresponds to a standardized effect size of Cohen’s d ≈ 0.116. No significant time effects were observed, suggesting consistent intervention effects across the study (Table 2).
Generalized Estimating Equations Analysis of Primary Outcome (Change in Concentration Performance)
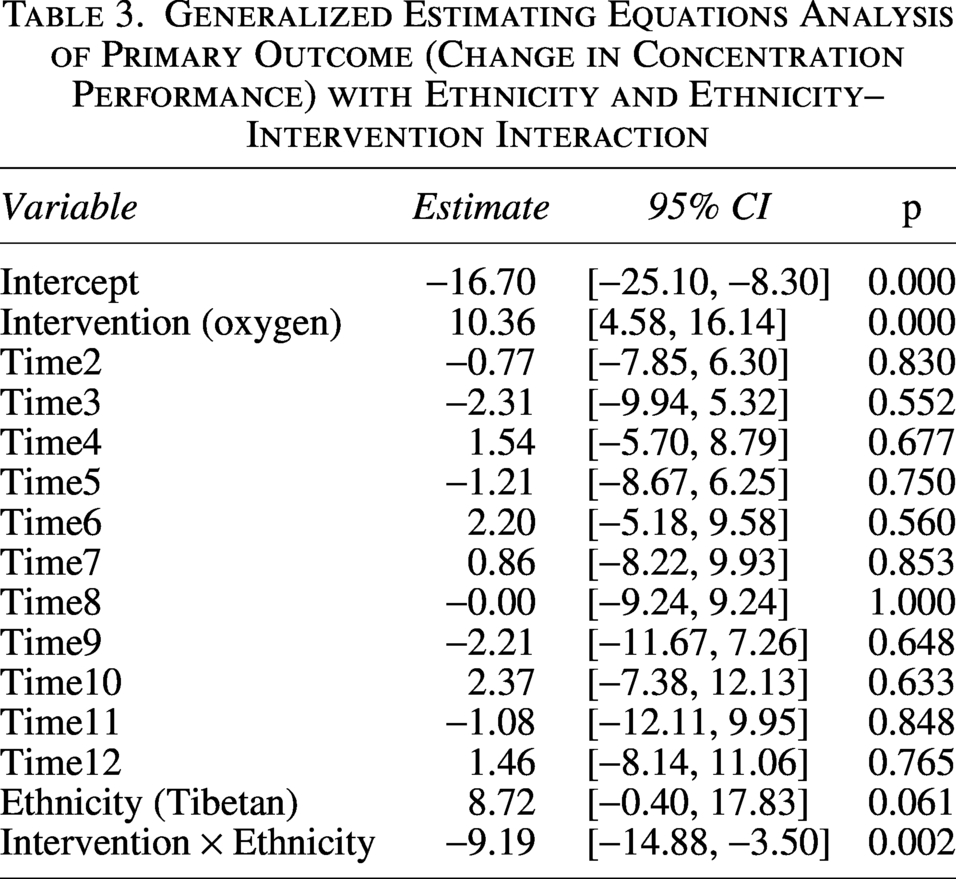
An exploratory analysis revealed a significant ethnicity–intervention interaction (estimate: −9.19, 95% CI: −14.88 to −3.50, p = 0.002; Table 3), with supplemental oxygen showing greater benefit in Han surgeons.
Generalized Estimating Equations Analysis of Primary Outcome (Change in Concentration Performance) with Ethnicity and Ethnicity–Intervention Interaction
Secondary outcome: Change in ΔMVC
The secondary outcome, change in ΔMVC, showed no significant difference between interventions (estimated: −0.18, 95% CI: −1.77 to 1.40, p = 0.822; Supplementary Table S1), indicating no effect on physical fatigue. Some time periods (e.g., Time2: p = 0.019; Time8: p = 0.035) showed significant associations, but these did not alter the overall null result.
Subgroup analysis
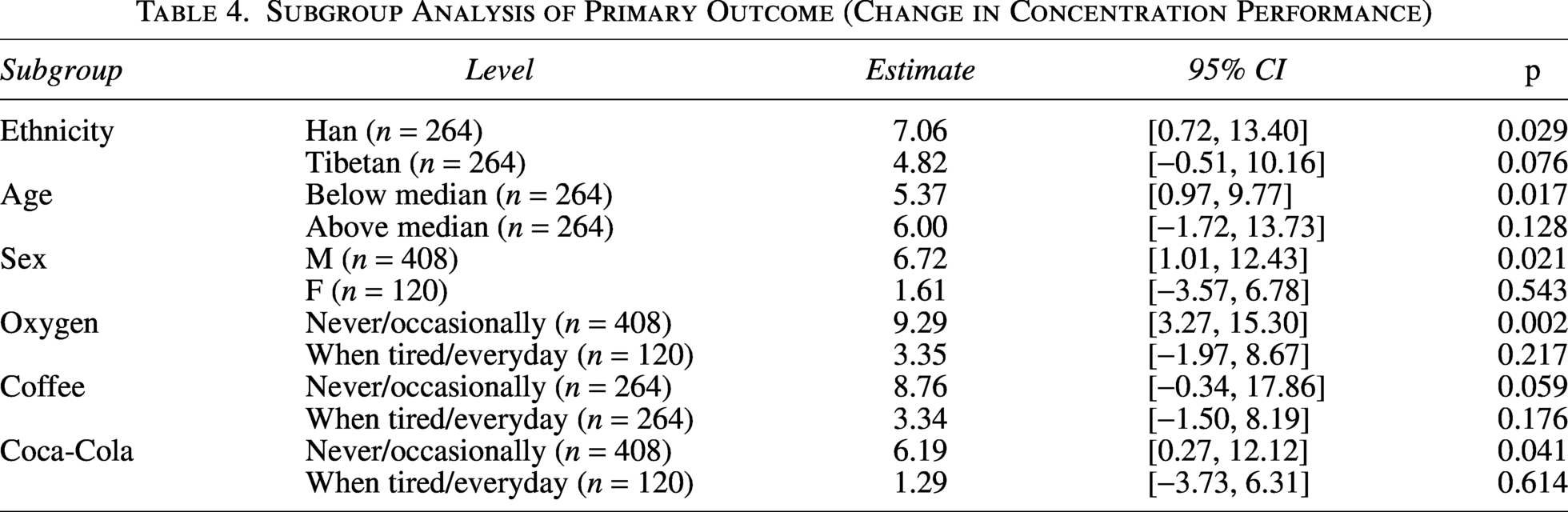
Exploratory subgroup analyses for ΔCP showed a significant effect of supplemental oxygen in less-acclimatized Han surgeons (estimate: 7.06, 95% CI: 0.72 to 13.40, p = 0.029) but not in Tibetan surgeons (estimate: 4.82, 95% CI: −0.51 to 10.16, p = 0.076). Surgeons with no or occasional baseline oxygen use benefited significantly from oxygen (n = 17, estimate: 9.29, 95% CI: 3.27 to 15.30, p = 0.002), unlike those using oxygen when tired or daily (n = 5, estimate: 3.35, 95% CI: −1.97 to 8.67, p = 0.217). Other subgroup results (e.g., by age, sex, coffee, or Coca-Cola consumption) are detailed in Table 4 but should be interpreted cautiously due to small sample sizes.
Subgroup Analysis of Primary Outcome (Change in Concentration Performance)
For ΔMVC, no significant differences were observed across most subgroups, consistent with the overall null finding (Supplementary Table S2). An exception was a negative effect in surgeons using oxygen when tired or daily (estimate: −1.66, 95% CI: −2.50 to −0.81, p < 0.001), requiring further investigation.
Discussion
This SW-CRT evaluated supplemental oxygen versus Coca-Cola for mitigating surgical fatigue among 22 surgeons at high altitude. Our findings demonstrate that supplemental oxygen is more effective than Coca-Cola in alleviating cognitive fatigue during high-altitude surgery, particularly for nonacclimatized Han surgeons. While it is a small effect, such a modest preservation of cognitive function holds practical significance within the high-stakes, hypoxic environment of high-altitude surgery.
Tibet’s surgical workforce includes native Tibetan surgeons, who are genetically adapted to high-altitude conditions, and Han surgeons, who often serve 1–3 years as part of the Aid-Tibet medical aid program (Xu et al., 2024). Tibetan surgeons benefit from physiological adaptations such as higher resting ventilation, greater lung capacity, enhanced lung function, and increased blood flow (Moore, 2017). These adaptations synergistically mitigate chronic hypoxia, reducing fatigue during physical exertion. In contrast, less-acclimatized Han surgeons may experience heightened fatigue due to inadequate adaptation. High-altitude hypoxia impairs cognitive functions, including attention, reaction time, memory, and executive function (Chen et al., 2023; Pun et al., 2019). While prolonged exposure may lead to partial adaptation, cognitive performance often remains below sea-level norms (Li and Wang, 2022; Furian et al., 2022). The greater efficacy of supplemental oxygen in Han surgeons likely reflects their reduced physiological adaptation compared to their Tibetan counterparts.
Furthermore, subgroup analysis revealed that surgeons who use oxygen “everyday” or “when tired” did not significantly benefit from intraoperative supplementation. This is likely to reflect a ceiling effect: surgeons with a habit of daily oxygen use may already maintain near-optimal baseline oxygenation. Therefore, the additional 2 l/min low-flow oxygen provides marginal gains in their concentration. Conversely, those who seldom use oxygen likely operate at a baseline of mild hypoxia. For this group, supplemental oxygen effectively reverses cerebral hypoxia, resulting in a substantial improvement. This finding corroborates the importance of on-demand oxygen therapy for individuals who are not fully acclimatized for high-altitude conditions.
Interestingly, while cognitive fatigue was significantly alleviated by supplemental oxygen, we observed no significant difference in physical fatigue between the two interventions, as measured by the change in maximum voluntary contraction (ΔMVC) force. This divergence highlights the unique cognitive demands of surgery at high altitudes. Modern surgical procedures typically involve sustained, yet moderate, physical exertion of the upper limbs. A standard 2-hour operation may not trigger a drastic decline in muscle strength. This suggests that surgical fatigue at high altitudes is predominantly a neurocognitive phenomenon rather than a musculoskeletal one, underscoring the critical need for interventions targeting cerebral oxygenation.
Coca-Cola’s traditional use in Tibet, dating to its return to China in the 1980s, lacks scientific grounding (Ishak et al., 2012; Smirmaul et al., 2017; Hackett, 2010). Beyond its limited biological mechanisms (caffeine and sugar), the “ritual” of consuming Coca-Cola may also involve a psychological placebo effect. However, our primary and secondary endpoints are validated objective measures rather than subjective self-reports. Consequently, despite the placebo effects, our core findings remain robust.
This study extends prior research on oxygen supplementation in high-altitude contexts, such as mountaineering, to surgical settings, highlighting its utility in maintaining cognitive performance during complex procedures (Falla et al., 2024; Ulrich et al., 2017). Based on these results, we recommend that high-altitude hospitals should establish supplemental oxygen as a standard intraoperative fatigue-management protocol.
To effectively translate this recommendation into clinical practice, several feasibility and safety concerns regarding nasal cannula use must be addressed. First, to prevent nasal mucosa dryness during prolonged inhalation, future protocols should utilize humidified oxygen to enhance surgeon comfort. Second, while extension tubing slightly restricts mobility, primary surgeons usually remain stationary. If long-distance movement is required, portable concentrators or temporary disconnection by circulating staff are viable solutions. Third, sterility is strictly maintained by wearing the cannula beneath the surgical mask and routing the tubing down the surgeon’s back, avoiding the surgical field entirely. Finally, fire risk is negligible. The low oxygen flow rate (2 l/min), surgical mask barrier, safe distance (>1 m) from electrosurgical units, and standard laminar flow ventilation effectively prevent oxygen accumulation, and no fire-related incidents happened during this trial.
Limitations
The sample size (22 surgeons and 528 surgeries) limited the power of subgroup analyses, and the exploratory nature of these analyses warrants cautious interpretation. The SW-CRT design mitigated this by using each surgeon as their own control across intervention phases, enhancing statistical efficiency. The single-center design may limit generalizability to other high-altitude settings. Some long-term outcomes, such as surgical error rates, were not assessed, limiting clinical impact evaluation. Surgeons’ subjective perceptions of benefit were also not formally recorded via standardized scales. Additionally, oxygen saturation was not monitored before or during operations, which precluded a dose–response analysis based on baseline hypoxia. Future research should explore these outcomes, specifically aiming to correlate cognitive fatigue scores with objective clinical outcomes or intraoperative technical errors, and validate findings in larger, multicenter studies.
Conclusion
This study provides randomized clinical trial evidence that supplemental oxygen is superior to traditional Coca-Cola consumption for mitigating cognitive fatigue in high-altitude surgery with no effect on physical fatigue. The significant benefit observed in nonacclimatized Han surgeons strongly supports its adoption as a standard of care to enhance surgeons’ performance and well-being, support physicians deployed via the Aid-Tibet medical aid program, and ultimately safeguard surgical quality in this region.
Authors’ Contributions
H.X. and D.W. conceptualized and supervised the study. S.L. and K.H. designed the study protocol. Project administration and clinical coordination were managed by B.C., S.L., and D.W. The trial implementation, participant recruitment, and measurement were executed by B.C., D.B., Y.S., F.L., J.S., H.Y., L.J., L.D., and D.C. Data analysis and manuscript drafting were performed by B.C. and S.L. All authors read and approved the final manuscript.
Footnotes
Data Availability
The datasets generated and/or analyzed during the current study are not publicly available due to ethical restrictions and the need to protect participants’ personal information but are available from the corresponding author on reasonable request.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This study is funded by the Beijing Research Ward Excellence Program (BRWEP2024W034010103), National Key Research and Development Program of China (2024YFA0918500), Science and Technology Projects of Xizang Autonomous Region (XZ202501ZY0072, XZ2024ZR-ZY001(Z) and XZ202501JD0021).
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.