
Abstract
Kolokas, Iraklis, Jenny Schlichtiger, Sara Jamali, Lina Kronschnabel, Paul Adam, Jeremias Götschke, Pontus Mertsch, Christian Goelz, Solveig Vieluf, and Stefan Brunner. Exercise-induced autonomic and cardio-respiratory stress at high altitude in leisure athletes. High Alt Med Biol. 00:00–00, 2026.
Background:
Exercise at high altitude imposes additional cardiovascular and autonomic demands on leisure athletes. We investigated how acute exposure to high altitude alters cardiovascular, respiratory, and autonomic regulation during rest, exercise start, and peak exercise.
Methods:
Briefly, 12 nonacclimatized participants (five female) performed standardized exercise tests at low and high altitude, while heart rate (HR), respiratory rate (RR), heart rate variability (HRV_RMSSD), respiratory rate variability (RRV_RMSSD), and respiratory sinus arrhythmia (RSA) were measured using wearable electrocardiogram (ECG) recordings and computer-based signal analysis.
Results:
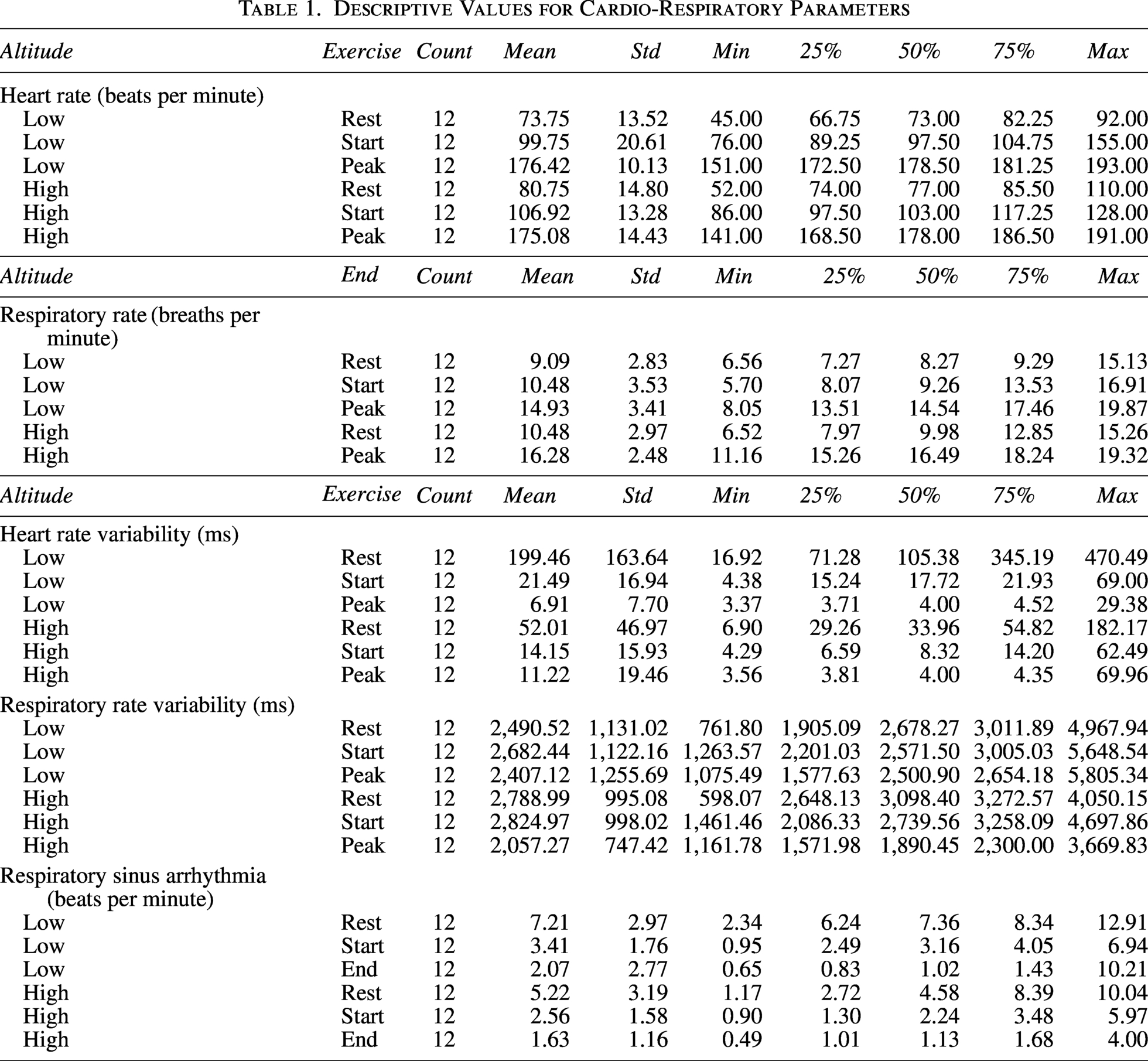
Maximal power output during the maximal incremental cycling test was lower at high altitude (235.5 ± 65.5 W) compared to low altitude (276.4 ± 77.5 W). HR and RR increased with exercise intensity and showed a nonsignificant increase at high altitude. RMSSD decreased during exercise (−116.67 ± 79.29 ms, p < 0.01) and at high altitude (−50.16 ± 91.55 ms, p = 0.015), with a significant interaction during exercise at high altitude (p < 0.01), while RRV remained relatively stable. RSA was reduced at high altitude (−1.1 ± 0.71 bpm, p = 0.028) and during exercise (−4.37 ± 0.38 bpm, p < 0.01), reflecting lower cardio-respiratory coupling.
Conclusion:
These patterns indicate that acute high-altitude exercise shifts autonomic balance, imposing heightened cardiac strain while the respiratory system maintains adaptive ventilatory flexibility, highlighting their differential roles in supporting oxygen delivery and systemic homeostasis under hypoxic stress.
Introduction
Exercise at high altitude imposes substantial cardiovascular and autonomic stress due to reduced oxygen availability, even in healthy individuals. Recreational and occasional athletes frequently engage in physical activity under these conditions without prior acclimatization, making them particularly susceptible to exaggerated heart rate and autonomic responses that can increase perceived exertion and physiological strain. The combination of hypoxia and exercise places unique demands on cardiac output, heart rate, respiratory function, and autonomic regulation, challenging the body’s ability to maintain systemic homeostasis. Given the widespread participation in alpine leisure activities, understanding cardiovascular adaptations in this population is of clear clinical and practical relevance.
In general, heart rate increases at high altitude, particularly in relation to physical activity, reflecting the cardiovascular system’s need to maintain oxygen delivery under hypoxic conditions (Singh et al., 2021). Especially, nonacclimatized individuals experience pronounced cardiovascular strain, with greater elevations in heart rate and oxygen uptake demands, which likely drive parallel increases in respiratory rate (Williams et al., 2022). Hypoxia reduces blood oxygen saturation and triggers adjustments in autonomic regulation, including increased sympathetic activity (Fornasiero et al., 2018; Hamm et al., 2020; Hou et al., 2023). These changes manifest as reduced heart rate variability (HRV), evident during both acute exposure and exercise, which serves as an index of tolerance to altitude stress, with larger HRV drops signaling diminished autonomic flexibility (Li et al., 2025; Nik Azis et al., 2025). The magnitude of HRV reduction may serve as an index of an individual’s tolerance and adaptation to high-altitude stress, with greater decreases indicating reduced autonomic flexibility (Hou et al., 2023). Such alterations in cardiac and autonomic control suggest a shift in homeostasis, potentially affecting coupling across autonomic subsystems and the integration of cardiac and respiratory regulation. Maintaining coordination between these systems is critical for sustaining oxygen delivery and metabolic support during exercise under hypoxic stress, and disruptions in this coupling may contribute to earlier engagement of anaerobic metabolism and limitations in maximal performance. Recent developments in wearable electrocardiogram (ECG) devices combined with standardized signal processing allow rapid and practical detection of cardiovascular, respiratory, and autonomic changes during exercise under challenging environmental conditions, enabling monitoring that were previously difficult to capture.
The aim of this study was to investigate how acute exposure to high altitude alters cardiovascular, respiratory, and cardio-respiratory autonomic regulation during exercise and exercise transitions in nonacclimatized recreational athletes, using this approach with wearable ECG devices and standardized signal processing. We hypothesized that both exercise and moderate altitude would be associated with higher heart and respiratory rates, reduced HRV, reflecting sustained cardiac output and reduced parasympathetic control, and increased respiratory rate variability (RRV), reflecting adaptive ventilatory flexibility under increased metabolic and hypoxic demand. We further expected altitude by activity interactions for HRV and cardio-respiratory coupling, with the greatest reductions in coupling occurring at exercise start, when rapid physiological state regulation is required under high-altitude conditions.
Methods
Study design and setting
The study was conducted as an interventional study. A cohort of 14 patients was prospectively enrolled and investigated under two different environmental conditions. All participants underwent standardized exercise testing at two locations: Munich (low altitude; 521 m altitude) and the Environmental Research Station Schneefernerhaus at Zugspitze (high altitude; 2,650 m altitude). Each participant served as their own control. Inclusion criteria were legal adulthood (age >18 years), a good level of physical endurance allowing for an exercise stress test, the absence of contraindications to exercise testing, and previously unknown cardiovascular diseases.
Exercise protocol
Exercise testing was performed using cycle ergometry following a stepwise incremental protocol (see Fig. 1). The test started at a workload of 50 watts, with increases of 30 watts every 2 minutes. Participants were instructed to maintain a pedaling cadence between 60 and 70 per minute throughout the test. The exercise test was terminated upon reaching maximal exertion.
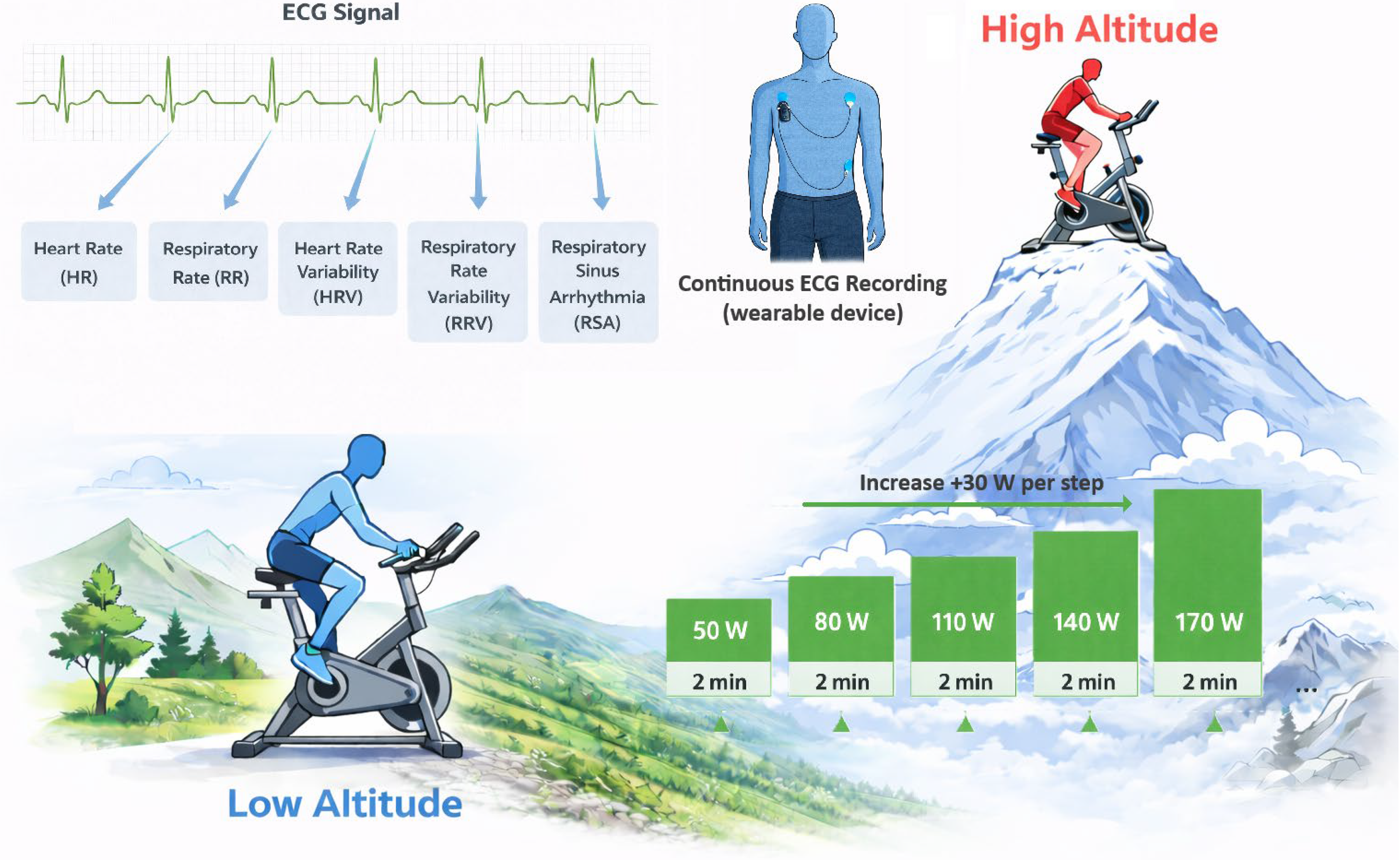
Experimental setup and protocol. Schematic representation of the study design assessing cardio-respiratory responses at low and high altitude. Participants completed a standardized incremental cycle ergometer protocol under both conditions with continuous monitoring. ECG recordings were used to extract heart rate, RR intervals, heart rate variability indices, and waveform parameters for analysis. The figure was generated with the support of ChatGPT. ECG, electrocardiogram.
Data collection
Prior to exercise testing, all participants completed a standardized questionnaire assessing sociodemographic data, medical history, and sports and physical activity history.
Vital signs and parameters of HRV were continuously monitored during exercise testing. In addition, physiological data were recorded continuously using wearable devices. At the beginning and at the end of each exercise test, a patch-based ECG recording was performed in addition to the continuous wearable monitoring.
The study was approved by the LMU ethics committee under the number 24-0742 in accordance with the Declaration of Helsinki. All participants provided written informed consent after receiving detailed information about the study aims and procedures.
Data preprocessing and signal analysis
ECG preprocessing and feature extraction were performed using NeuroKit2 (version 0.2.12)1 (Makowski et al., 2021) in Python (version 3.10.6). We filtered the ECG signals using neurokit2’s ecg_clean function with the neurokit method, which includes a 0.5 Hz high-pass filter to remove slow drifts followed up by a powerline filter at 50 Hz. Next, we segmented the signals into 1-minute windows and did automatic R-peak detection using Neurokit2’s build-in detection method (method: “neurokit”). Next, we visually verified detected R-peaks, keeping only the segments where R-peak detection worked correctly. From the accepted windows, we kept cleaned segments from rest, the start, and the peak of exercise. As “start of exercise,” we refer to the first stage of the exercise test, and as “peak of exercise,” we refer to the last stage of the exercise test. For those we calculated the following metrics: mean heart rate, respiratory rate, root mean square of successive RR-interval differences (HRV_RMSSD), RMSSD of breath-to-breath cycle (RRV_RMSSD), and respiratory sinus arrhythmia (RSA). RSA reflects the phasic modulation of heart rate by respiration, providing a quantitative index of parasympathetic control and the dynamic coupling between cardiac and respiratory systems. To further examine whether altitude affected HRV independently of heart rate, an additional HR-binned analysis (90–170 bpm, 20-bpm increments, ± 5 bpm range) was performed, comparing median HRV values between low- and high-altitude conditions within matched HR ranges.
Statistics
We used statsmodels (version: 0.14.6)2 (Seabold and Perktold, 2010). A repeated-measures ANOVA with the within-subject factors altitude (low altitude and high altitude) and exercise (rest, start, and peak of exercise) was performed for all cardiovascular outcomes. Effect sizes are reported as partial eta-squared (ηp2). When significant interactions occurred, post hoc comparisons were conducted using Bonferroni-adjusted paired contrasts. All analyses were performed using a significance level of 0.05.
Results
In total, 14 healthy participants volunteered, and the final sample comprised 12 participants (mean age: 31.1 ± 10.2 years, body mass index: 24.0 ± 2.4 kg/m2, 5 females), as 2 were excluded due to missing data in either the ground-level or high-altitude recordings. Among the final cohort, there was one active smoker. Four participants (30.8%) reported regular alcohol consumption. The mean weekly sports activity was 4.7 ± 2.1 hours. Ergometer power output was reduced at high altitude compared with low altitude. The absolute maximum power dropped from 276.4 ± 77.5 W at low altitude to 235.5 ± 65.5 W at high altitude, representing a performance decline of 14.8%. The relative power decreased from 3.86 ± 1.04 W/kg to 3.28 ± 0.85 W/kg at high altitude, marking a reduction of 15.0%. Across all participants, exercise in high altitude induced measurable changes in cardiovascular activity (see Fig. 2 and Tables 1 and 2).
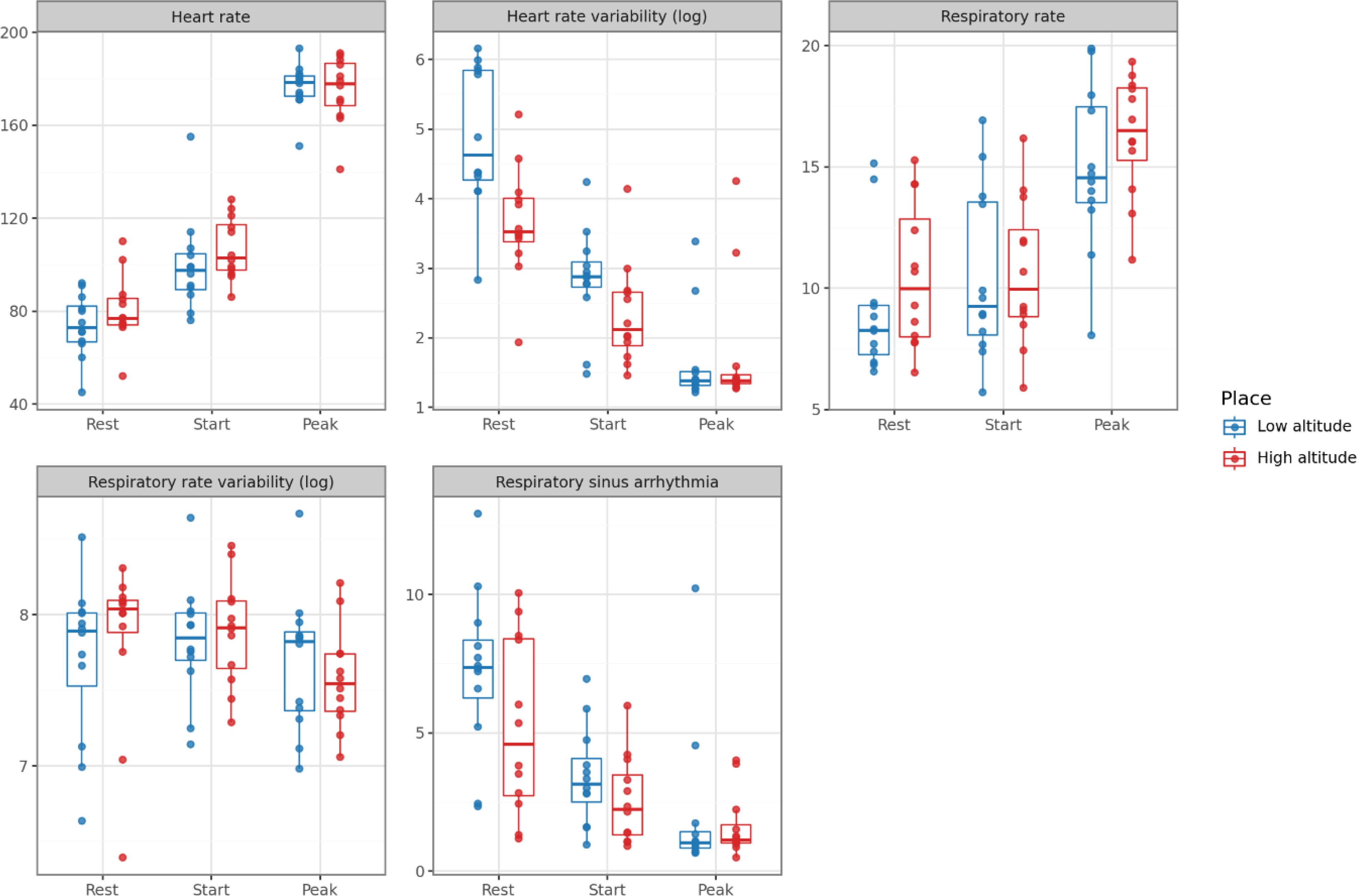
Box-plots of mean heart rate, heart rate variability (HRV), respiratory rate, respiratory rate variability, and respiratory sinus arrhythmia (RSA) measured at low and high altitudes at rest, at the start of exercise, and at peak exercise.
Descriptive Values for Cardio-Respiratory Parameters
ANOVA Results for Cardiovascular Baseline, Variability, and Coupling Parameters
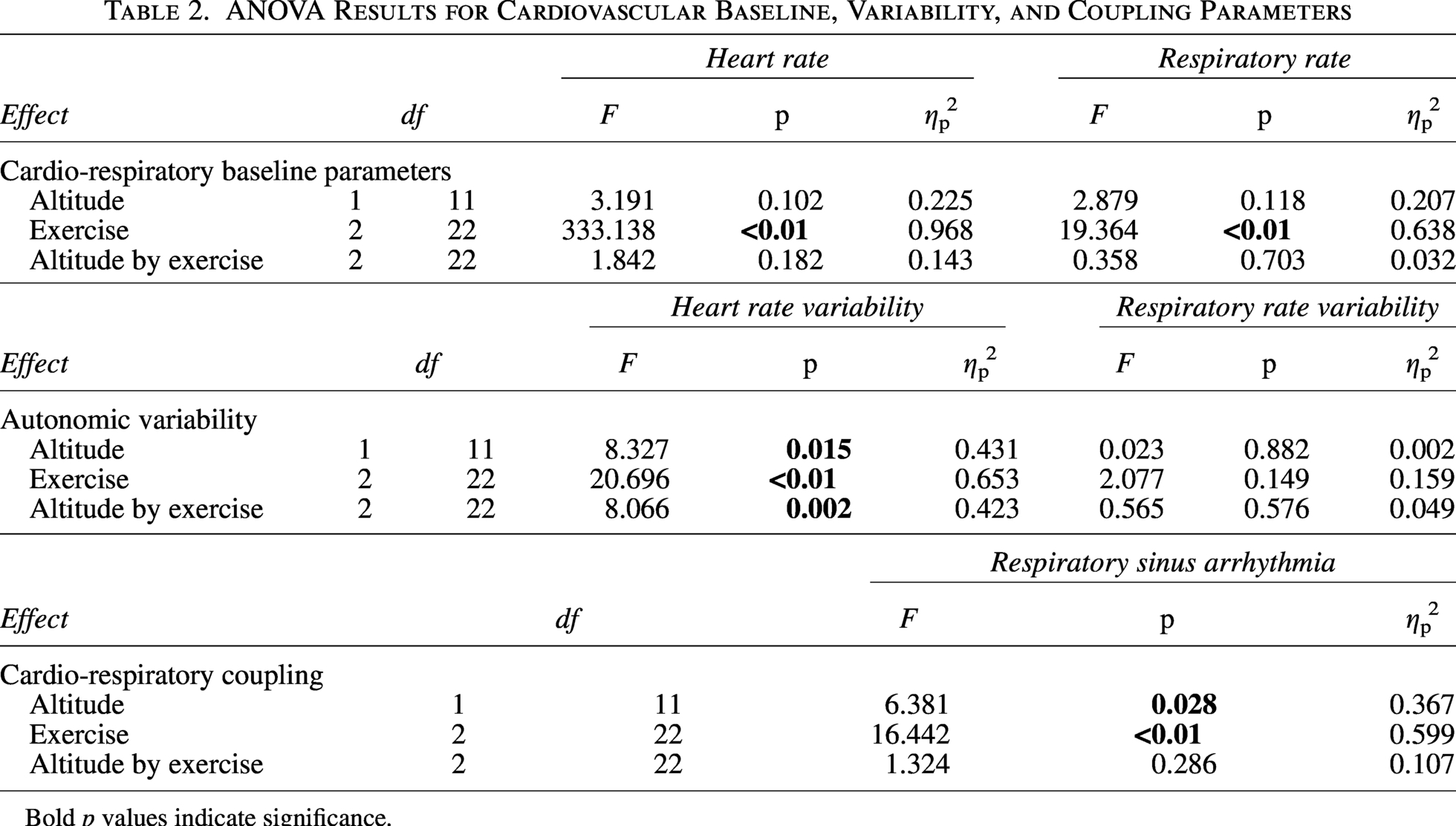
Bold p values indicate significance.
Heart rate (HR) showed a significant main effect of exercise phase. Post hoc comparisons indicated that HR at rest was lower than at exercise start (p < 0.01), and HR at the peak of exercise was higher than both rest (p < 0.01) and exercise start (p < 0.01). A similar exercise-related pattern was observed for respiratory rate, with higher values at the peak of exercise compared with both rest (p < 0.01) and exercise start (p < 0.01; see Fig. 2).
Heart rate variability (HRV; RMSSD) demonstrated significant main effects of altitude and exercise, as well as a significant altitude-by-exercise interaction. Post hoc analysis following up on the significant interaction revealed higher values at exercise start compared with the peak of exercise at low altitude (p = 0.02) and higher values at rest compared with both start (p < 0.01) and peak of exercise (p < 0.01) at low altitude. It also revealed marginally significant higher values at rest compared to the start (p = 0.06) and peak of exercise (p = 0.06) at high altitude and higher values at rest at low altitude compared to rest at high altitude (p = 0.01). Respiratory rate variability (RR_RMSSD) did not show any significant main or interaction effects (see Fig. 2).
RSA exhibited significant main effects of altitude and exercise phase. Post hoc comparisons for the exercise phase indicated higher RSA at rest compared with the start (p < 0.01) and peak of exercise (p < 0.01). RSA was higher at low altitude compared to high altitude (p = 0.03).
Across heart rate bins, HRV (RMSSD) decreased with increasing heart rate in both conditions, with lower values at high altitude at lower HR bins and a convergence between conditions at higher HR ranges (Fig. 3).
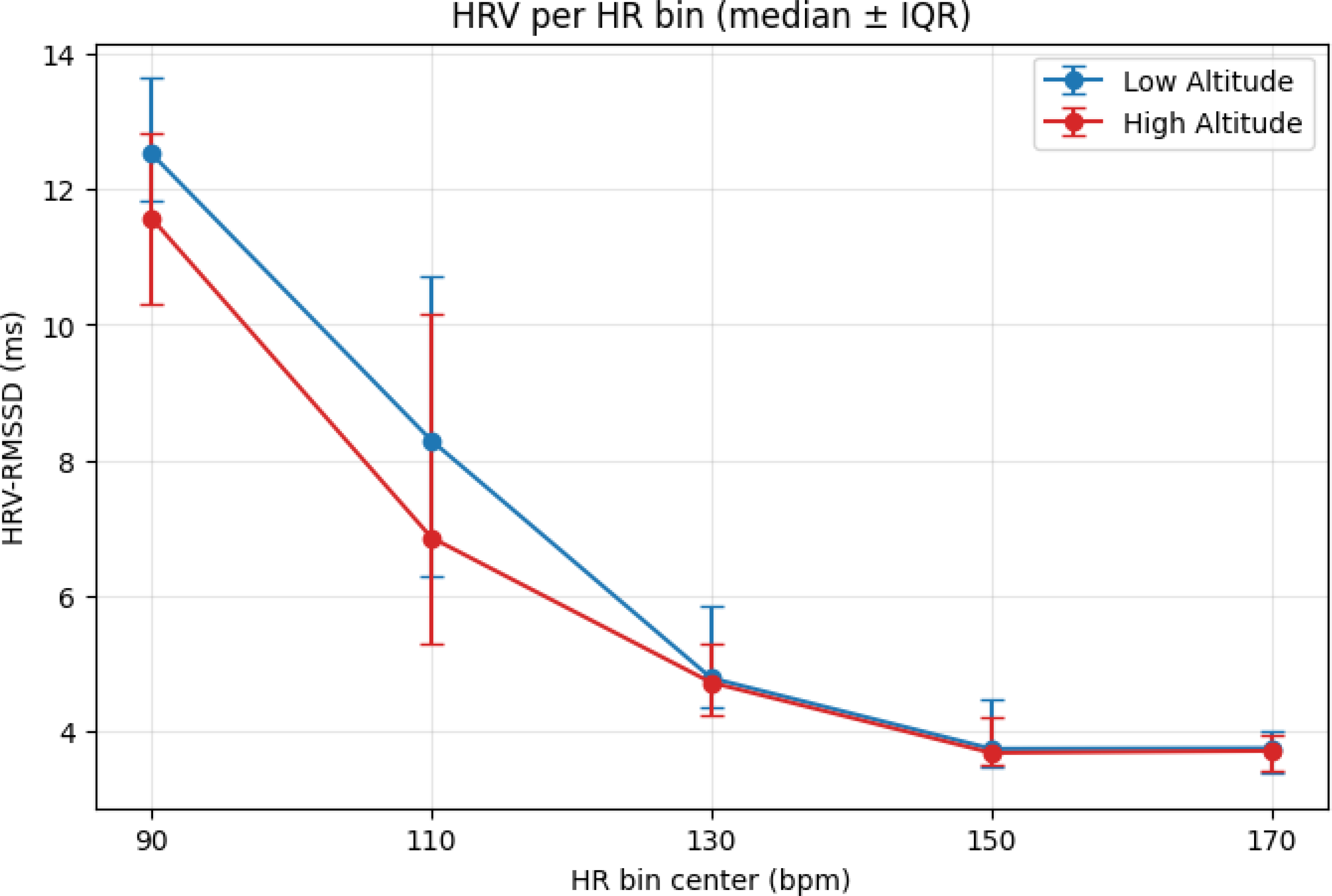
Displays the median values per HR bin over the respective participants. HR, heart rate.
Discussion
Exercise at high altitude leads to lower performance and imposes distinct strains on the cardiac and respiratory systems in recreational athletes. The cardiac system primarily maintains oxygen delivery, reflected in HR and HRV adjustments, while the respiratory system assumes a modulatory role, with RRV remaining stable despite altitude and exercise stress. This functional dissociation contributes to reduced cardio-respiratory coupling, likely reflecting an earlier shift toward anaerobic metabolism, consistent with lower peak power and faster attainment of maximal exertion at altitude. Overall, these findings highlight how cardiac maintenance and respiratory adaptability interact to govern systemic homeostasis under hypoxic exercise.
Beyond this cardiorespiratory interaction, altitude exposure is known to induce marked shifts in autonomic regulation, characterized by increased sympathetic activation and altered vagal modulation. In particular, previous work has demonstrated that acute hypoxic exposure affects cardiac autonomic control as reflected by parameters such as heart rate deceleration capacity (DC) and periodic repolarization dynamics (PRD). Hamm et al. showed that normobaric hypoxia is associated with measurable alterations in DC and PRD, indicating early changes in vagal withdrawal and sympathetic activation even under controlled hypoxic conditions (Hamm et al., 2020). Furthermore, acute exposure to altitude has been linked to a reduction in DC, reflecting impaired parasympathetic cardiac control after ascent (Hamm et al., 2018). Of note, interindividual differences in these autonomic markers have also been associated with susceptibility to acute mountain sickness, suggesting that autonomic regulation is not only a physiological response but may also have prognostic value in altitude medicine (Hamm et al., 2020). In this context, our findings of increased sympathetic activity and altered HR–HRV behavior are consistent with a shift toward sympathetic predominance under hypoxic exercise conditions.
Importantly, the detailed assessment of these cardiovascular, respiratory, and autonomic responses was enabled by wearable ECG devices combined with standardized computer-based signal processing. This innovative approach allowed noninvasive monitoring of HR, HRV parameters, respiratory rate, RRV, and RSA during rest and across varying levels of exertion, capturing subtle physiological and pathophysiological changes that would be difficult to detect in extreme and adverse conditions using traditional laboratory assessments (Nik Azis et al., 2025; Riley and Gavin, 2017). Beyond controlled research settings and standard everyday practice, this technology holds particular promise in high-altitude medicine and other extreme environments, where rapid detection of cardio-respiratory or autonomic strain is critical (Wang et al., 2024). Wearable monitoring allows real-time tracking of physiological responses, supports individualized feedback, and can guide acclimatization strategies, training load management, and safety measures, providing a practical tool for clinicians, coaches, and field practitioners to monitor and protect athletes and individuals who are exposed to challenging conditions.
The observed cardiovascular and autonomic adaptations at high altitude may have clinical implications. (Fornasiero et al., 2018) Monitoring heart rate, HRV, and RRV can help track cardiovascular strain (Li et al., 2025) and detect early signs of maladaptive responses (Tsai et al., 2025). Identifying individuals who are at higher risk, such as those with pre-existing cardiovascular or respiratory conditions, lower fitness, or limited altitude experience, allows for targeted precautions to ensure safety. Finally, these findings can inform structured acclimatization strategies, guiding the gradual adjustment of exercise intensity and duration to improve performance while minimizing hypoxia-related risks.
Our study presents several methodological and interpretive limitations that should be considered when interpreting these findings. The study focused on recreational athletes, limiting generalizability, for example, to elite athletes, sedentary individuals, or those with pre-existing cardiovascular or respiratory conditions. Short-term exposure to hypoxia reflects acute responses rather than long-term acclimatization, and controlled exercise testing may not fully replicate real-world high-altitude environments. While HR, HRV, and RRV were measured, other markers such as stroke volume, oxygen saturation, pH, pCO2, pO2, or lactate kinetics could have provided a more complete view of systemic adaptation. In addition, further statistical analysis of the interaction between HR and HRV across conditions could have provided deeper insights into how altitude modulates autonomic responses but was constrained by data availability. Individual differences in baseline fitness and prior altitude experience may have influenced responses. Further, the study did not evaluate mitigation strategies such as pre-acclimatization or pacing adjustments, limiting direct recommendations for safe exercise at altitude. Finally, we did not integrate pharmacological blockade into our study protocol, which would have allowed a more precise characterization of sympathetic and parasympathetic contributions. Future work should, therefore, consider the use of atropine and/or β-blockade to further elucidate autonomic control mechanisms.
In conclusion, exercise at altitude substantially affects cardiovascular and autonomic responses in recreational athletes, with altitude further modulating heart rate, blood pressure, and sympathetic activity. These findings demonstrate that even moderate physical activity in unacclimatized leisure athletes can impose significant cardiovascular strain, highlighting the importance of monitoring heart rate, blood pressure, and autonomic function to ensure safe participation in high-altitude activities.
Footnotes
Acknowledgments
The authors gratefully acknowledge the Environmental Research Station Schneefernerhaus and its team, operated by the Bavarian State Ministry for the Environment, for providing access to its unique research infrastructure. S.V. was supported by the Hightech Agenda Bavaria. They thank all the participants and the volunteer assistants who supported the data collection in Munich and on the Zugspitze.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.