
Abstract
Lower urinary tract symptoms (LUTS) are common in older men and are frequently associated with benign prostatic hyperplasia (BPH). The relationship between BPH and endogenous total testosterone (TT) levels has been widely studied. The aim of this post hoc analysis was to determine the association between LUTS and endogenous TT levels in a subset of men participating in the 2013 Prostate Cancer Awareness Week, a U.S. community-based prostate cancer screening program. Men completed the International Prostate Symptom Score (I-PSS) questionnaire, prostate size was estimated by a digital rectal examination, and serum TT and prostate-specific antigen levels were measured. Mean TT levels (ng/dl) did not significantly correlate with prostate size category (r = +.03, p = .69): normal, 419.2 (n = 106); enlarged, 394.7 (n = 71); abnormal, 416.4 (n = 7); and abnormal/suspicious, 515.2 (n = 19). Mean TT levels (ng/dl) did not significantly correlate with I-PSS category (r = −.06, p = .40): none, 468.5 (n = 15); mild, 414.0 (n = 138); moderate, 397.4 (n = 66); and severe, 437.9 (n = 7). Mean TT levels (ng/dl) did not significantly correlate with I-PSS quality of life rating (r = −.13, p = .055): delighted, 474.5 (n = 43); pleased, 424.6 (n = 65); mostly satisfied, 361.2 (n = 63); mixed, 448.2 (n = 29); mostly dissatisfied, 337.2 (n = 17); and unhappy, 435.8 (n = 6). Adjustment for prostate size or prostate-specific antigen levels yielded similar findings. In conclusion, endogenous TT levels did not correlate with LUTS or prostate size, and these findings support the saturation theory in which TT is not able to induce further androgen-stimulated prostate tissue growth due to receptor saturation. Any worsening of LUTS following testosterone replacement therapy in hypogonadal men may be related to stimulation of prostatic cells previously deprived of testosterone.
Keywords
Introduction
Lower urinary tract symptoms (LUTS) are common in older men, with the prevalence of moderate-to-severe LUTS ranging from 22% in men aged 50 to 59 years to 45% in men aged 70 to 80 years (Rosen et al., 2003). LUTS comprise storage (irritative) symptoms (i.e., urinary frequency, nocturia, urgency, urinary incontinence) and voiding (obstructive) symptoms (i.e., slow-stream, intermittency, hesitancy, straining, postmicturition dribble, and sensations of incomplete emptying). LUTS may result from a complex interplay of pathophysiological influences, including prostatic pathology and bladder dysfunction (Chapple & Roehrborn, 2006).
Benign prostatic hyperplasia (BPH), a nonmalignant proliferation of the epithelial and stromal cells, leads to prostate enlargement, primarily in older men. Prostatic cell proliferation and the development of histological features of BPH are generally considered to be dependent on the bioavailability of testosterone and its metabolite, 5α-dihydrotestosterone. An association between these androgens levels and BPH measures has not been consistently reported. Because of the known effects of androgens on prostate growth, testosterone prescribing information warns that the therapy may worsen BPH symptoms, and clinicians are advised to monitor patients with BPH who are receiving testosterone replacement therapy (TRT) for worsening of signs and symptoms of BPH (Bhasin et al., 2010).
While the association between BPH and endogenous total testosterone (TT) levels has been widely studied, there is less clarity on the effects of endogenous TT levels on LUTS. (Pearl et al., 2013, Yassin, El-Sakka, Saad, & Gooren, 2008). The aim of this post hoc analysis was to study the relationship, if any, between TT level and both prostate size, estimated by digital rectal examination (DRE), and LUTS, as assessed by the International Prostate Symptom Score (I-PSS).
Method
The study sample comprised men who elected to be screened during the 2013 Prostate Cancer Awareness Week (PCAW). PCAW is a U.S. community-based prostate cancer screening program, sponsored by the Prostate Conditions Educational Council, with approval provided by Colorado Multiple Institutional Review Board. Men are offered the opportunity to attend PCAW during the third week of September, with recruitment through media announcements and information posted on the Prostate Conditions Educational Council website. Methodology of PCAW has been previously published in detail (Stone, Miner, Poage, Patel, & Crawford, 2014). Men undergoing screening (N = 3,277) provided written informed consent, completed a series of health questionnaires (including the I-PSS) and received a medical evaluation. A subset of men (N = 1,367) had blood drawn for laboratory assays, including measurement of TT and prostate-specific antigen (PSA) levels. Serum TT levels were measured using the ADVIA Centaur XP immunoassay system (Siemens, Malvern, PA; total TT normal range 300-700 ng/dl, sensitivity 10-1,500 ng/dl); PSA levels were measured using the Hybritech PSA immunoassay and the Beckman Access (Beckman Coulter Inc., Fullerton, CA). Prostate size was estimated by DRE and categorized (see Table 1) based on the opinion of the examiner. Analyses were performed using data from men with TT levels measured from an 8- to 11-a.m. blood draw (n = 229). The self-administered I-PSS questionnaire was used to assess the severity of BPH symptoms over the prior month (Barry et al., 1992). The I-PSS includes seven symptom severity questions (each scored 0-5, higher scores indicate more severe symptoms on a scale of 0-35), which are collectively referred to as the I-PSS total score, and one quality of life (QoL) question that is scored independent of the symptom severity questions. The seven I-PSS symptom severity questions can further be categorized into an irritative symptom subscore (questions on urinary frequency, urgency, and straining) and an obstructive symptom subscore (questions on urinary incomplete emptying, intermittency, weak-stream, nocturia). Spearman correlation coefficients were calculated between TT levels and prostate size categories/PSA values and I-PSS categories and QoL ratings as well as between TT levels and I-PSS total, irritative symptoms, and obstructive symptom subscores. Analysis of covariance was used to adjust the I-PSS variables for prostate size. In all analyses, adjustments were made for age and BMI.
Baseline Characteristics (Men With a Blood Draw Time From 8 to 11 a.m., N = 229).
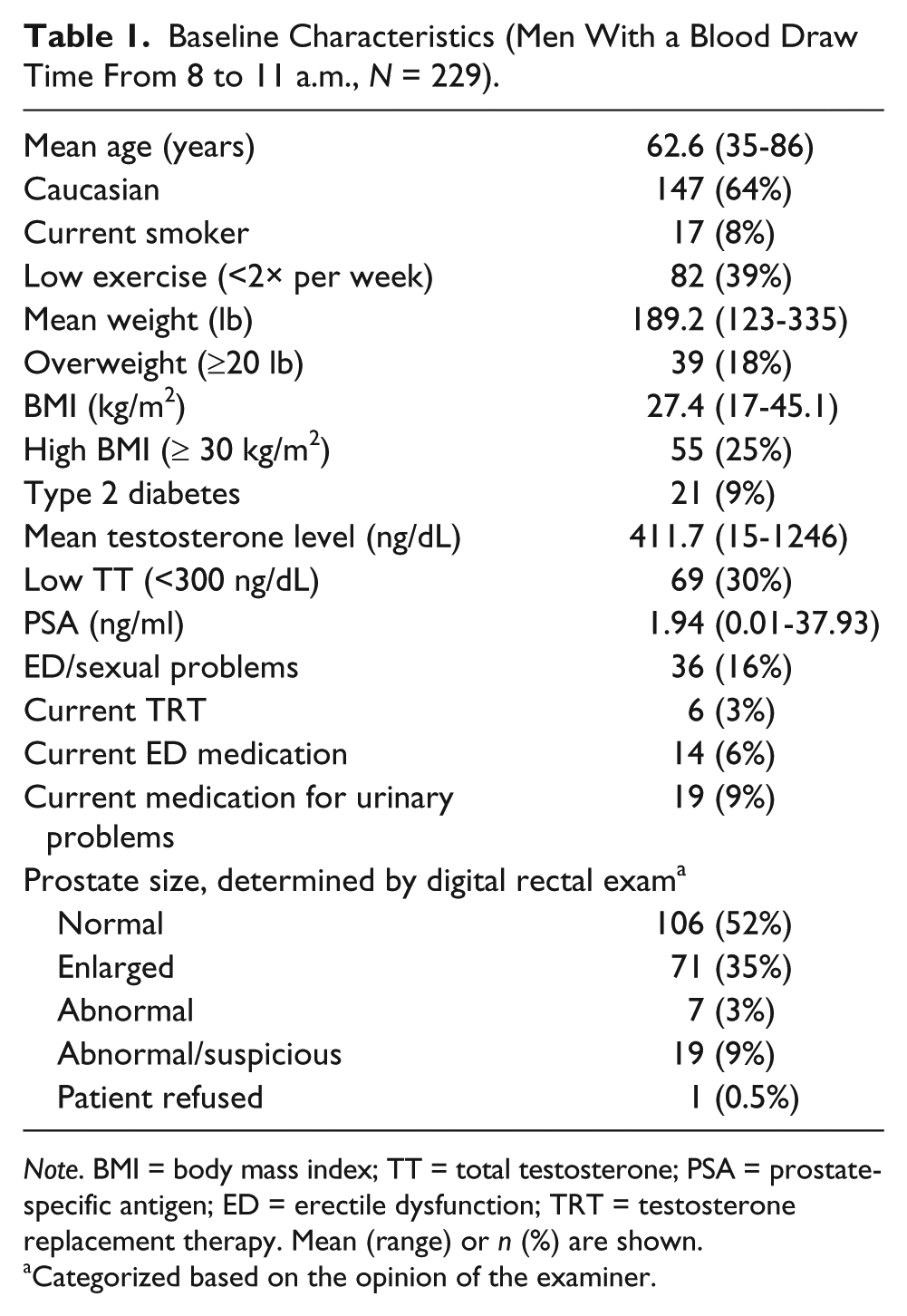
Note. BMI = body mass index; TT = total testosterone; PSA = prostate-specific antigen; ED = erectile dysfunction; TRT = testosterone replacement therapy. Mean (range) or n (%) are shown.
Categorized based on the opinion of the examiner.
Results
There were no significant correlations between mean TT level and prostate size (r = +.03, p = .69), I-PSS category (r = −.06, p = .40) or PSA level (r = +.03, p = .69) (see Table 2). Although mean TT levels did not significantly correlate with I-PSS QoL rating (r = −.13, p = .055), there was some evidence that patients with a higher QoL had slightly higher testosterone levels. There were no significant correlations between TT level and I-PSS total (r = −.073), irritative symptom subscore (r = −.10) or obstructive symptom subscore (r = −.04; p > .1, in all cases). Adjustment for prostate size yielded similar findings.
Total Testosterone Level by Prostate Size and Measures of Lower Urinary Tract Symptoms.
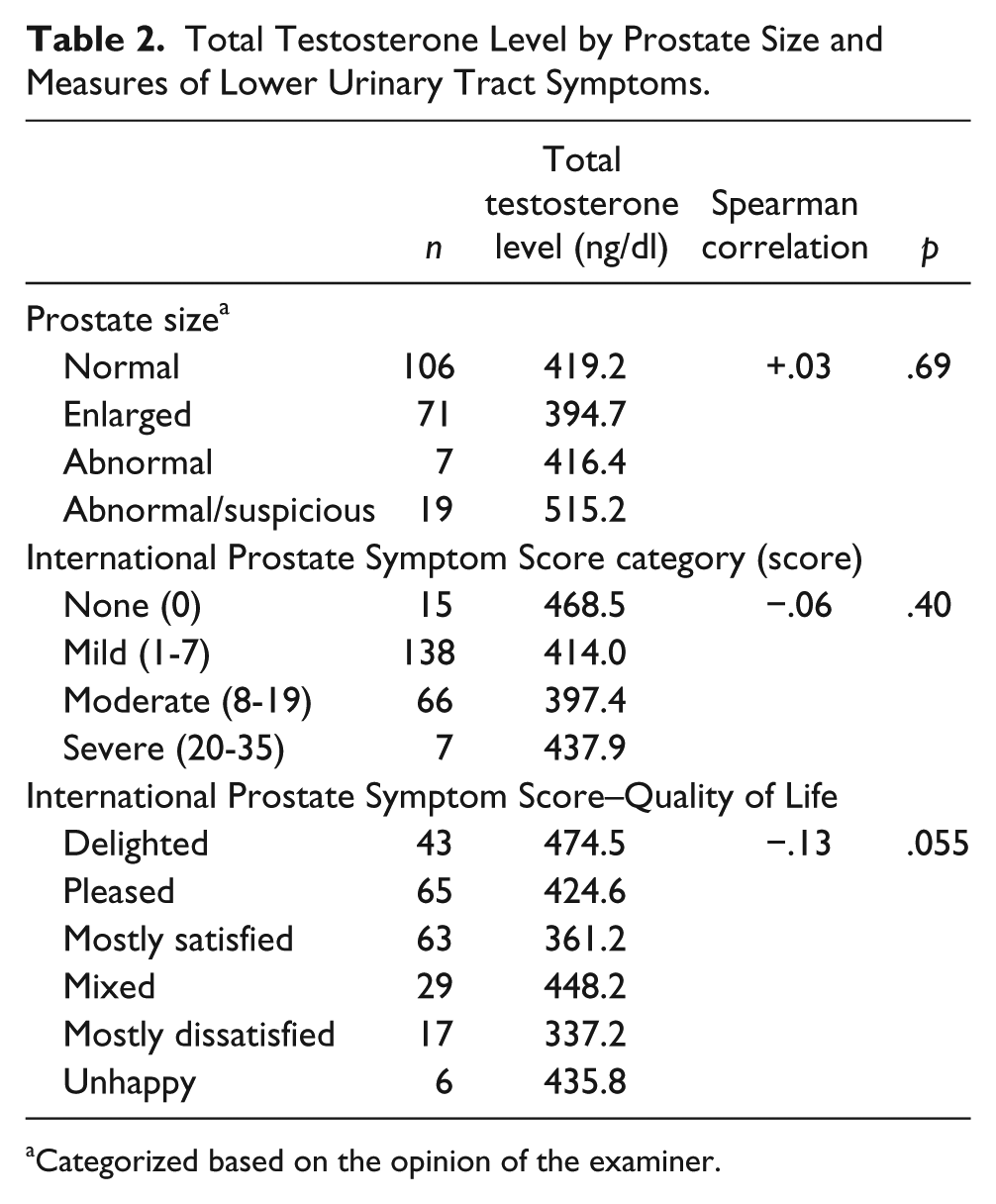
Categorized based on the opinion of the examiner.
Discussion
In this analysis, endogenous TT levels did not correlate with prostate size, PSA level, or LUTS. The findings are consistent with an earlier study, using a similar group of men, which concluded that testosterone levels had no impact on LUTS status, PSA level, or prostate volume (Schatzl et al., 2000).
These findings may add support to the saturation theory, which postulates that increased levels of testosterone do not further induce androgen-stimulated prostate tissue proliferation due to receptor saturation (Khera, Crawford, Morales, Salonia, & Morgentaler, 2014). While this study assessed only endogenous TT levels, these data suggest that worsening of LUTS following TRT in hypogonadal men may be related to stimulation of prostatic cells previously deprived of testosterone.
Study limitations include the following: the use of a community-based study of relatively small sample size (n = 229), which was not prospectively designed or powered to determine the relationship between TT levels and prostate size or LUTS; the population was not restricted to hypogonadal men or men with LUTS; prostate size was determined by DRE; free/bioavailable testosterone levels were not determined; and only a single TT measurement was made, without consideration for day-to-day variability.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AN, DAP, SAD, and DM are salaried employees at Eli Lilly and Company; EDC is a consultant for Bayer, Inc MDx, Genomic Health Jansen Pharmaceuticals, Dendreon, and Ferring Pharmaceuticals; WP is a collaborator/contractor with MDx Health, Strand Diagnostics, Genomic Dx, Abbott Laboratories, and Bayer, Inc.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The analyses were performed by Eli Lilly and Company