
Abstract
Colorectal cancer (CRC) is the second leading cause of cancer death among Latino men in the United States, yet they have low screening rates. This study explored barriers and facilitators of colonoscopy screening among Latino participants in a CRC screening promotion program. Six focus groups were conducted, in Spanish, with 45 Latino men, of which 28 had received and 17 had not received a colonoscopy. Analysis of the discussion transcripts identified barriers to CRC screening, facilitators to CRC screening, and recommendations for health information dissemination. There was consensus among all participants that they had not received adequate information on colonoscopy screening from their health care providers. Unscreened participants wanted more details about the colonoscopy procedure and bowel preparation. Screened men were more knowledgeable than unscreened men about CRC, the colonoscopy procedure, and the benefits of early detection. Participants also expressed their fears, concerns, and perceptions of stigma in relation to colonoscopy screening. They described family and personal testimonials as facilitators to engaging in colorectal cancer screening. Findings underscore the need for ongoing research and educational efforts to address personal and cultural stigma surrounding colonoscopy and CRC, particularly in underserved communities. Study findings also highlight the danger of missing out on opportunities to increase CRC screening when colonoscopy is the primary screening option offered. Additional research is needed to ensure trust in the health care system and to examine the effectiveness of testimonials on CRC screening among Latino men.
Keywords
Introduction
Colorectal cancer (CRC) is the second leading cause of cancer death among Latino men in the United States (American Cancer Society, 2021). Screening for CRC can prevent such deaths through early detection and because precancerous growths can be removed in the course of a colonoscopy (American Cancer Society, 2021). The most widely used CRC screening tests include the Fecal Immunochemical Test (FIT), Fecal Occult Blood Test (FOBT), and colonoscopy (Steinwachs et al., 2010). Colonoscopy is generally considered the gold standard given its high sensitivity and specificity, and since 2000 its use has increased (Issa & Noureddine, 2017; Steinwachs et al., 2010), reflecting factors at the provider (Bandi et al., 2012; Hawley et al., 2014; Hoffman et al., 2011; Klabunde et al., 2009), and policy levels (Klabunde et al., 2007; Steinwachs et al., 2010). FITs also have increased while FOBTs have declined. All screening modalities reduce CRC mortality when compared to no screening (Bandi et al., 2012; Issa & Noureddine, 2017; U.S. Preventive Services Task Force, 2016), and data show that Latinos and non-Hispanic Blacks prefer FOBT over colonoscopy (Inadomi et al., 2012). Likewise, individuals without health insurance or employment, and non-English speakers, are more likely to complete FIT/FOBT than colonoscopy (Petrik et al., 2018). Nationally, CRC screening rates among Hispanic men are low: 60% of Hispanic versus 69% of non-Hispanic white men ages 50+ years are up to date (American Cancer Society, 2021). Less use of colonoscopy among Hispanics largely explains these differences, as rates of stool tests are higher among Hispanic than non-Hispanic White adults (American Cancer Society, 2021).
Reasons for low CRC screening range from socioeconomic to cultural to health system barriers (American Cancer Society, 2021). They include low health literacy and CRC knowledge as well as language and other access barriers (i.e., transportation, lack of time, health insurance). Additional barriers may include concerns about required bowel preparation prior to the procedure (Jones et al., 2010; O’Malley et al., 2002; Quick et al., 2013) and fear of negative test results (Nagelhout et al., 2017). Such barriers are not unique to the Latino population, but research shows language is a greater barrier for Latino men compared to Latina women (Diaz et al., 2013) and that concerns related to masculinity and embarrassment are more common among Latino men (Getrich et al., 2012). Furthermore, Latino men are less likely than men of other ethnicities and races to take care of their health and they use less health care services than non-Hispanic White men (Peak et al., 2010).
This qualitative research was conducted to address the challenges the research team was encountering in enrolling men for a CRC promotion program that offered no-cost colonoscopy screening. The goal was to gather information that would help in developing an intervention targeting Latino men for colonoscopy screening within a federally qualified health center. The research literature on CRC screening interventions among Latino men is scarce. A systematic review of CRC screening interventions among Latino men reported only seven published intervention studies promoting CRC screening, with only two studies exclusively targeting Latino men (Mojica et al., 2018). Although other qualitative studies have evaluated facilitators and barriers to colonoscopy screening (Honein-AbouHaidar et al., 2016), we were concerned about the generalizability of results and wanted to understand contextual influences in this specific community. Thus, we conducted focus group discussions to explore knowledge, attitudes, and beliefs about CRC and CRC screening and discuss how to best disseminate health information. This article is designed to inform targeted interventions that address CRC screening among medically underserved populations.
Methods
This study was conducted in June 2015 as part of an evidence-based cancer education-plus-navigation program that offered education, navigation, and no-cost cancer screening tests to a Latino population in South Texas who was not up to date with breast, cervical or colorectal cancer screening guidelines. The program was designed and implemented in collaboration with a federally qualified health center (FQHC) and three community organizations. Participants for the education-plus-navigation program were recruited via community outreach and clinic in-reach by community health workers (Mojica et al., 2021). At the time of the current study, 4,000 women and 293 men had enrolled in the education-plus-navigation program. Concerned about our challenges enrolling and screening men, we designed the current study to focus on CRC screening among Latino men ages 50 to 75 years.
Participants
Although program staff had not been in recent contact with all 293 men and anticipated challenges in reaching them, we decided to contact all of them to ensure an acceptable number participated in the focus groups. The program database that included contact information and screening status was used to identify the men. Telephone outreach by two community health workers located only 108 men who were reachable. Among these, 35 declined to participle in the study. Of the 73 who expressed initial willingness to participate, 45 attended the focus groups. The Institutional Review Boards at the Health Science Center and State University (Study Number 8320) approved the study.
Data Collection
Research staff assigned participants to focus groups based on whether they had received a colonoscopy: 3 groups with screened men (28 total men) and 3 groups with unscreened men (17 total men). In each focus group, there was one man who did not speak English; participants opted to conduct the focus groups in Spanish to not exclude these participants. Participants signed an informed consent form and completed a demographic survey. A trained Spanish-speaking moderator led each focus group, and two project members took notes. The moderator and notetakers created an open and welcoming environment to encourage participants to express their individual experiences and feelings. The groups were conducted in a meeting room at a local FQHC. The research team developed the discussion questions from sample discussion guides and reported barriers and facilitators identified in other qualitative research studies of barriers and facilitators to colorectal cancer screening, many of which were included in a systematic review and meta-study synthesis (Honein-AbouHaidar et al., 2016). The interview guide began with open-ended questions on cancer and CRC to get big-picture insights. The remaining questions were specific to beliefs and attitudes about CRC screening and elicited opinions on screening barriers and facilitators. Questions also covered general health practices and health information seeking behavior. (See the Supplemental Appendix for a copy of the discussion guide.) The audio-recorded sessions were conducted in Spanish and each lasted 90 min. Participants received a $25 Visa gift card for their participation and were served either breakfast or dinner in conjunction with the focus group session.
Data Analysis
Demographic survey data were exported into an Excel file and analyzed to obtain frequencies, means, and standard deviation. T-tests and chi-square independence tests were used to determine any statistically significant differences between unscreened and screened men. All focus group audio files were transcribed verbatim by a professional transcription service in the source language. Data were analyzed using a content analysis approach: “classify[ing] large amounts of texts into efficient number of categories that represent similar meanings” (Hsieh & Shannon, 2005). Two bilingual researchers independently read each transcript to get an overall sense of the whole text and then reread the transcripts by interview question to capture key concepts and thoughts. An iterative process of team discussions was used to resolve discrepancies in coding and to develop the final codebook. In developing the codebook, we knew we had reached data saturation when no new codes or themes occurred in the data (Saunders et al., 2018). Final codes had to appear in two or more focus groups and were sorted into categories based on how they were related: barriers to CRC screening, facilitators to CRC screening, and recommendations for health dissemination. Once categories were identified, researchers selected illustrative quotes for each category to summarize findings (Eldh et al., 2020). The study team used Atlas.ti version 1.6.0 for Mac for data management.
Results
Study Sample
Focus group participants (N = 45) included 28 screened and 17 unscreened men. Table 1 presents a summary of the sample socio-demographic characteristics. Men were a mean age of 58 years (SD = 6) and 14 (31%) were born in the United States. The 31 who were foreign born had lived in the United States, on average, for 28 years (SD = 15). Thirty-two (71%) were married, 20 (44%) were employed full- or part-time, 19 (42%) reported an annual income of less than $10,000, and 34 (76%) had less than a high school education. Twenty-two (49%) men had health insurance and 39 (87%) reported having a usual source of care. There were no statistically significant differences between the screened and unscreened men in socio-demographic characteristics other than doctors’ visits. Twenty-four (86%) screened men but only 10 (59%) unscreened men reported having a doctor’s visit in the past year (p < .042). Also, 37 out of 45 (82%) participants reported their health as “excellent/very good/good” and 5 (11%) had a family history of CRC.
Characteristics of Latino Men Participating in Focus Group Discussions (N = 45)
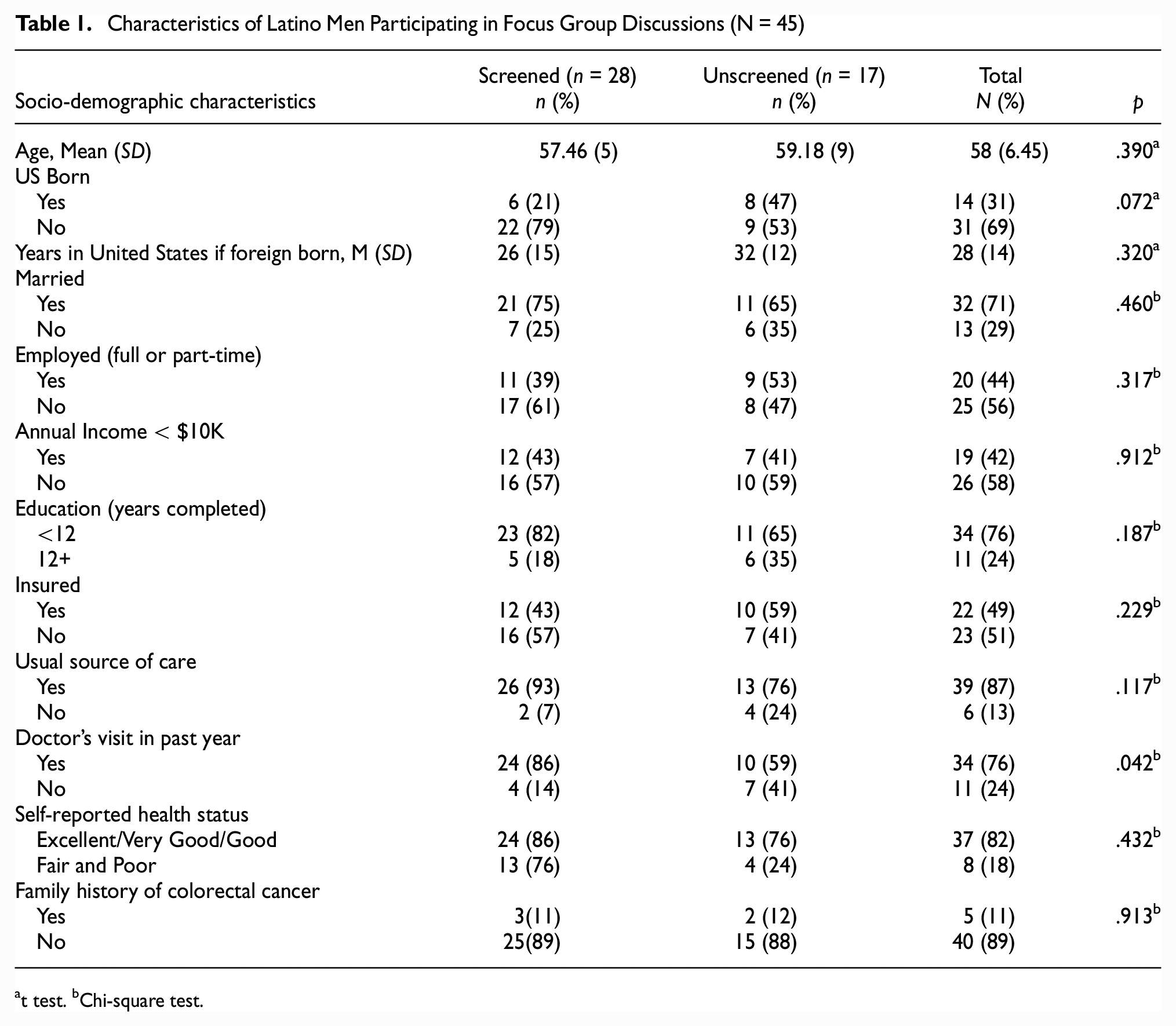
t test. bChi-square test.
Content Analysis
Barriers to CRC Screening
Participants identified barriers to CRC screening that included a range of knowledge deficits, potential costs of CRC screening and other financial concerns, lack of health insurance, stigma, perceived potential threats to masculinity, and fears of a cancer diagnosis and possible death. They also mentioned lack of knowledge about CRC and CRC screening modalities. Such lack was common among unscreened participants, who were unsure how colonoscopies are performed, what type of preparation was required, whether they would be sedated during the colonoscopy, the type of instruments utilized in the procedure, potential side effects, and whether they would expect pain. Few unscreened participants were knowledgeable about CRC risk factors and screening guidelines. A common response from unscreened participants to the question, “What do you think causes colon cancer?” was “I don’t have any idea.” Unscreened men also associated CRC with invasive or serious medical procedures they had heard about that only occur in late-stage CRC. For example, one unscreened man said, “They put you in [colostomy] bags . . .,” and another man said “ . . . they remove your intestines . . . I think of the worst of it.” Some unscreened participants mentioned that they avoided learning about cancer and screening while others said they were eager to learn about it. Men in the latter group asked questions such as, “How do you detect the symptoms?” and indicated that they had come to the focus group because of a desire to learn more, saying things like, “we are here to learn . . . this is why we came.” Previously screened men were more knowledgeable about CRC, the colonoscopy procedure, and the benefits of screening and early detection. Yet, some mentioned that they only realized after completing the procedure that what they had previously thought about the procedure were myths. One screened man said, “I was naïve . . . they say colon and I was thinking the actual rectum . . . I didn’t know that it’s a long cord [the colonoscope] . . . and when they show you the images you’re left like, Wow!”
Participants identified concrete access barriers to CRC screening, including cost and lack of health insurance coverage. All men were concerned about the cost of screening tests and the loss of income resulting from missing work. Several unscreened men reported that they sometimes forego general exams due to lack of financial resources. Screened men also shared that they were in the United States to work and provide for their wives and children, and even family in their home countries, and thus they cannot afford to pay for preventive care. One screened man noted that “cost . . . is one of the reasons why [Latino men] are not ready [to participate in screening] because of the economic situation they have.” Several participants pointed to out-of-pocket expenses they would face for screenings even with health insurance. Other barriers both screened and unscreened men noted included difficulty accessing the health care system in terms of scheduling appointments and getting to the clinic, especially for a colonoscopy screening since they need someone to drive them home afterwards. One screened man highlighted the difficult trajectory between exposure to CRC information and completing a CRC screening test: “The problem at that point is not so much the [health] information . . . the problem is how to get to the point of diagnosing it.”
Perceived stigma associated with a colonoscopy was another common theme among participants. Men described colonoscopy as an invasive procedure. They felt it would undermine their masculinity and that others in the community would feel it did, too. One participant explained, there is a “strong culture, rooted in the Hispanic culture, is that if they insert something in you, you stop being the man you are.” Another screened man reported on the reaction of men in his inner circle to hearing he had a colonoscopy: “No, friends and brothers, when they hear about colonoscopy they say, ‘Well, if you get a colonoscopy it means that you are no longer a virgin.’” This statement speaks to the fear men have about the invasiveness and consequences of the test. One man said, “I’m a man, how are they going to do that to me!” The men agreed that they wouldn’t “let anybody know [them] in the butt. There ain’t anybody gonna touch my ass.” Even just talking about it caused one man to say, “Look, I even crossed my legs talking about this.” Participants were also concerned about being exposed and vulnerable while sedated during a colonoscopy: “Who knows how the doctor is? No, man, you don’t know [if] he is going to grab you while asleep.” Unscreened men also acknowledged a general reluctance among family members to talk about CRC: “They never talk about . . . No talking about it.” There was consensus among participants that this type of mistrust and fear of vulnerability was a barrier to CRC screening.
Generalized fear and anxiety was another barrier. Men identified fears of dying, of finding out something is wrong, and that the colonoscopy would be painful. Every participant reported fear of dying as a barrier to CRC screening, and they all equated cancer with dying: “You know that if you get it [cancer] you are going to die . . . you have cancer and you’re going to die. Not that you get embarrassed . . . I think that it’s more fear.” Other responses indicated the degree to which fear affects screening decisions: “plain fear” of having a colonoscopy and “We stop ourselves because of the fear.”
Facilitators to CRC Screening
The most identified facilitators to CRC screening participation were family support, patient testimonials, and expansion of screening test options. Screened men identified family as the reason they had been screened. Most participants reported being married or living with a partner, and those who had been screened talked about the active role their spouses played in the screening process, such as keeping appointments on a calendar and discussing their medical appointments with them. Unscreened men also confirmed the important role women can play in persuading men to get screened. One unscreened participant said, “Yeah. Women are the ones who [give] the encouragement to go see the doctor and things like that.” Similarly, men without spouses or children also talked about the importance of having “female friends” who would talk with and encourage them to get screened. One participant noted, “I have a very best friend and when I talk to her about something that I have, I like to see what she tells me . . . I mean a good person to share stuff with . . . I get encouragement like that.” Although one unscreened participant acknowledged that ultimately the decision was up to him, and a few unscreened men complained that “kids just call to ask for money,” or that “I am the one who has to be looking out for myself,” there was a general consensus that family could make them more likely to get screened. The unscreened men discussed ways they could be encouraged to think about their children and grandchildren, and implicitly, their desire to have more time with them when deciding to get screened.
Personal stories of CRC screening experiences were another facilitator to CRC screening, a factor screened men emphasized. Nearly all screened men reported that they would share their personal stories and screening experience so that others could learn that completing a screening was painless and had not been as bad as they imagined. One screened man shared that “the people who don’t [want to screen] could be convinced by people like us who are there to tell them [about CRC screening] . . . because we already did it.” Having the opportunity to discuss CRC screening experiences with previously screened individuals had encouraged some men to seek screening. They noted this strategy could contribute to easing concerns for unscreened men: “as long as someone who already went through it explains that it’s nothing.” Another man commented that “it’s just about convincing them that you can’t feel anything.” Another man’s strategy was to show others his pictures from the colonoscopy and to use humor in talking to others about his experiences. Participants in the unscreened groups commented that they would be interested in discussing CRC screening with men who had previously completed a screening to learn more about the procedure and hear about their overall experiences. They also embraced the opportunity to discuss “certain symptoms of the disease . . . the most serious [CRC symptoms].”
Another common facilitator was exposure to a variety of screening options. When asked, “What do you think would make it easier for Latino men to get checked for colon cancer?” nearly all participants suggested access to a “blood test” or other less invasive tests. One unscreened man wondered why health providers are not able to check the blood for cancer if they can perform other tests, such as paternity tests. Another unscreened man said, “If they could do it with blood only, I’d go. If it’s all blood . . . You don’t have to touch nowhere around there [meaning the anus].”
Recommendations for Health Information Dissemination
Recommendations provided by both screened and unscreened men focused on accessibility. In-person distribution of health materials and information from a community health worker or physician was the most preferred mode of health information dissemination. Interactive educational sessions or presentations also were preferred, primarily because of the opportunity to ask questions and clarify confusing information or instructions. Participants identified churches and workplaces (e.g., construction sites) as places where they would like to receive in-person information, including doctor’s offices and the emergency room (ER). One unscreened man observed, “If you go to an emergency [room], they see you because of an emergency but they don’t give you any pamphlets/brochures, information. Yes look, check yourself for this.” Participants noted this strategy would be especially beneficial for men who do not go to a physician’s office but access care only through the ER. Several participants reported that they themselves used the ER as their main source of care. Others suggested text messages, email, brochures, and television commercials might provide health information. Participant comments included “The majority of people, of men, sit and watch TV, to view sporting events and things like that . . . these are the moments when you could introduce a little bit of information” and “you can send information via the internet, and we can put it on Facebook for our friends.” Also, nearly everyone in the focus groups reported using the internet and smartphones, suggesting the utility of digital communication platforms for disseminating and accessing health information among Latino men.
See Table 2 for selected illustrative quotes for each category (i.e., barriers to CRC screening, facilitators to CRC screening, recommendations for health information dissemination) described in this section.
Categories With Illustrative Quotes for Barriers and Facilitators to Colorectal Cancer and/or Colonoscopy Screening Among Latino Men

Note. CRC = Colorectal cancer.
Discussion
This study was conducted with 45 Latino men in an FQHC who had participated in a CRC screening promotion program. Men expressed need for more information and highlighted their fears, concerns, and perceptions of stigma regarding colonoscopy screening.
There was consensus among all participants that they had not received adequate information on colonoscopy screening from their health care providers. Unscreened participants wanted more details about the colonoscopy procedure and bowel preparation, and they expressed annoyance about simply being told to get the exam. Screened men were more knowledgeable than unscreened men about CRC, the colonoscopy procedure, and the benefits of early detection. Their responses highlighted the importance of instrumental support by health care providers and family members to ensure actual participation in screening.
More information from health care providers, including details about the actual examination process, might go a long way in improving the patient-provider relationship and mitigating some of the mistrust men in this study reported. A recent scoping review of barriers to CRC screening similarly highlighted mistrust of the health care system among immigrant groups (Puli et al., 2023). In those studies, mistrust was characterized as “general mistrust” and defined as “low physician-patient rapport, lack of communication, and unclear screening guidelines.” In this study, on the other hand, men were explicit about their mistrust. Men feared the conduct of the provider while sedated: “Who knows how the doctor is? No, man, you don’t know [if] he is going to grab you while asleep.” Participants also wanted more information on other screening options, such as blood tests, that are widely favored by all races/ethnicities (Byrd et al., 2019; Green et al., 2017; Taber et al., 2014). Further validation of the information gap was evidenced in discussions about the lack of CRC health information tailored specifically for men, in contrast to the amount of information on breast cancer for women. Although the evidence on the effectiveness of male-tailored health information in impacting men’s screening behaviors is lacking, one study found that it can contribute strongly to intention to engage in prostate cancer screening and to some degree to CRC screening (Teo et al., 2018). In the absence of evidence, dissemination of culturally and linguistically tailored and targeted health information in general, and CRC screening specifically, may be advisable given the urgency of the issue and widespread limited knowledge.
Another important barrier was the stigma associated with colonoscopy screening. Men who perceived of colonoscopy as being stigmatized by their communities refrained from talking about it with family and friends. This stigma surrounding colonoscopy among Latinos often is associated with anxiety about homosexuality (Fernandez et al., 2008; Hennelly et al., 2015). In this study, unscreened men further described the colonoscopy as a loss of virginity, in the sense that they had never been “touched down there.” This sentiment speaks to the fear of the invasiveness of the test and no longer being “innocent” when they are “touched down there.” Men expressed not wanting fingers or cameras “back there” and that someone touching them “back there” was unthinkable. Unscreened men clearly had greater mistrust of providers than screened men. However, in this research, unscreened participants expressed optimism that testimonials from screened men could increase acceptance and screening of colonoscopy. Given that unscreened men (compared to screened men) primarily reported negative experiences with cancer (e.g., advanced cancer and cancer-related deaths), access to personal testimonials from screened men could contribute to reducing fear and stigma by introducing positive experiences with screening and survivorship. As has been reported in other studies of CRC screening (Getrich et al., 2012) and preventive services (Hunter et al., 2007), participants also noted the importance of family as a facilitator to engaging in CRC screening. Both screened and unscreened men suggested that emphasizing family responsibility and presenting screening as potentially contributing to men’s ability to be around for their children and grandchildren in the future might increase uptake. However, unscreened men might require more persuasion.
A counterintuitive finding is the lack of significant differences in socio-demographic characteristics between screened and unscreened men. This finding may indicate that, in this sample, beliefs, attitudes, and stigma surrounding colonoscopy might be more important determinants of colonoscopy screening compared to sociodemographic characteristics, such as income and education that generally affect access to health care. The screened and unscreened men only differed on whether they had a doctor’s visit in the past year. Screened men were far more likely to report a doctor’s visit in the past year than unscreened. Although we do not know whether the screened men completed the colonoscopy within the past year, this finding may indicate that they place a greater value on their health or (if they received the colonoscopy in the past year) perhaps they heard from other men who had a colonoscopy given that they were strong advocates for testimonials.
This research had several limitations. First, the sample who participated in the focus group was small and purposive and thus is not representative of other Latino men. The small sample size also may account for the lack of significant differences in socio-demographic characteristics between the screened and unscreened men. However, this approach allowed for in-depth exploration of factors influencing CRC screening and men’s thoughts about what might promote screening in their community. Second, we may have omitted collection/measurement of variables that may have meaningfully distinguished between the screened and unscreened men. Third, the sample was drawn from patients at a single FQHC and thus cannot be generalized to other contexts and settings. In addition, men had previously enrolled in the education-plus-navigation program, which potentially introduces selection bias, as the education they received may have influenced their attitudes and beliefs about colonoscopy screening and their participation in the focus groups might indicate a desire to improve their health. Further selection bias may arise from the fact that the men who participated in this study represented 15% of the overall men enrolled in the education-plus-navigation program. However, these men represented 68% of the men who were reachable by phone.
Despite these limitations, the study gave participants the opportunity to express their fears, concerns, and their perceptions of stigma in relation to colonoscopy screening. At the end of the focus groups, men expressed their appreciation for having the opportunity to engage in discussions with other men. In addition, the project engaged bilingual community health workers to recruit participants and bilingual researchers to read and analyze all transcripts in Spanish. Also, study findings can be used to inform interventions to increase CRC screening among Latino men.
Conclusions
Discussions revealed important barriers and facilitators to colonoscopy screening among Latino men attending an FQHC. The need for educational information targeting men, and ideal settings to reach men, were also points of discussion. Study findings also highlight the danger of missing out on opportunities to increase CRC screening rates by offering colonoscopy as the primary screening option. Findings underscore the need for ongoing research and educational efforts to address personal and cultural stigma surrounding colonoscopy and CRC screening, particularly in underserved communities. There is also a need to examine the effectiveness of personal testimonials on colorectal cancer screening among Latino men. Furthermore, we need additional research to ensure trust in the health care system, especially among men who often avoid preventive health care.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883231179325 – Supplemental material for Barriers and Facilitators of Colonoscopy Screening Among Latino Men in a Colorectal Cancer Screening Promotion Program
Supplemental material, sj-docx-1-jmh-10.1177_15579883231179325 for Barriers and Facilitators of Colonoscopy Screening Among Latino Men in a Colorectal Cancer Screening Promotion Program by Cynthia M. Mojica, Nancy Vargas, Savannah Bradley and Deborah Parra-Medina in American Journal of Men's Health
Supplemental Material
sj-docx-2-jmh-10.1177_15579883231179325 – Supplemental material for Barriers and Facilitators of Colonoscopy Screening Among Latino Men in a Colorectal Cancer Screening Promotion Program
Supplemental material, sj-docx-2-jmh-10.1177_15579883231179325 for Barriers and Facilitators of Colonoscopy Screening Among Latino Men in a Colorectal Cancer Screening Promotion Program by Cynthia M. Mojica, Nancy Vargas, Savannah Bradley and Deborah Parra-Medina in American Journal of Men's Health
Footnotes
Acknowledgements
Special thanks to the men who participated in the focus group discussions. The authors also thank the community health workers who helped with recruitment and the federally qualified health center who provided access to their meeting rooms.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Center for Advancing Translational Sciences [KL2 TR001118] and the National Cancer Institute [R01CA218923] of the National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.