
Abstract
Semen quality is a key factor in male reproductive health. The multifactorial etiology of male infertility involves complex interactions between environmental exposures and psychological states. The “mind-body” interaction, specifically the synergistic impact of lifestyle, social support, and fertility stress on semen quality, remains underexplored. This cross-sectional study recruited 485 men from our hospital between May 2021 and April 2023. Participants were categorized into normal (n = 256) and low semen quality (n = 229) groups based on WHO Laboratory Manual for the Examination and Processing of Human Semen (6th Edition). Participants completed the Social Support Rating Scale (SSRS), Fertility-related Quality of Life (FertiQoL), and Fertility Problem Inventory (FPI). Backward stepwise logistic regression was employed to identify independent predictors. Occupational heat exposure was the strongest risk factor (adjusted odds ratio [OR] = 4.188, 95% confidence interval [CI]: [1.527, 11.484], p = .005). Higher fertility-related stress showed a trend toward an independent association with low semen quality (adjusted OR = 1.005 per point, 95% CI: [1.000, 1.011], p = .068). Higher education level was a protective factor of semen quality (adjusted OR = .624, 95% CI: [0.415, 0.937], p = .023). Clinical management of male infertility should integrate psychological screening with occupational health guidance to optimize reproductive outcomes.
Introduction
Infertility has become a growing global health concern, affecting approximately 15% couples of reproductive age (Huang et al., 2023). Male-related factors account for nearly half of these cases (Organization, 2021). Semen quality, a key factor of male reproductive health, plays a pivotal role in fertility outcomes. A growing body of epidemiological evidence has highlighted a progressive decline in global sperm concentration and quality (Levine et al., 2023; Luo et al., 2023). Consequently, elucidating the multifactorial determinants of semen quality is crucial for clinical intervention and public health stategies.
Despite substantial advances in andrology, the precise impact of modifiable lifestyle and environmental determinants on spermatogenesis remains controversial. Although prevailing evidence generally implicates cigarette smoking (Henriques et al., 2023; Osadchuk et al., 2023) and heat exposure (Verón et al., 2024; X. Zhang et al., 2024) as potent risk factors of semen integrity, recent high-quality cohorts have yielded conflicting data, suggesting that these effects may be modulated by individual susceptibility or exposure thresholds (Harlev et al., 2015; L. Wang et al., 2024; X. Wang et al., 2020). While urban pollution is a well-established contributor to declining sperm quality (Rubes et al., 2021), recent analyses have identified distinct clusters of reduced semen quality in agricultural regions, implicating agrochemical exposure (Giulioni et al., 2021; Rahban et al., 2025). Similarly, evidence regarding educational attainment remains conflicting, with observed associations likely stemming from unequal health care access (Badreddine et al., 2024).
A predominantly biological or environmental focus often overlooks the critical “mind-body” interaction in male reproductive health. Psychological stress is not merely a consequence of low semen quality, but potentially a contributing etiological factor. Recent evidence indicates that poorer fertility-related quality of life may coexist with impaired conventional semen parameters (Abulizi et al., 2023), whereas other studies report null associations with spermatogenesis markers despite clear links to sexual dysfunction (Coward et al., 2019). Infertility-related stress, commonly measured by the Fertility Problem Inventory (FPI), encompasses social, sexual, and relational strains that may plausibly affect male reproductive potential. High fertility stress was associated with lower sperm concentration and total sperm count, which suggests that stress levels may modify how psychosocial well-being relates to motility outcomes (Mireyi et al., 2025; Reddy et al., 2025). Direct FPI–semen parameter studies remain limited. Social support is increasingly viewed as a key psychosocial resource that buffers stress exposure and may translate into measurable reproductive benefits in men. Emerging clinical evidence suggests that higher perceived support is linked to more favorable motility profiles, and that support can moderate the deleterious associations between stress and semen quality (Abulizi et al., 2023; Ansah et al., 2025). The strength and direction of these associations appear context-dependent, underscoring the need for rigorous studies integrating standardized support assessments into semen quality evaluation.
This study aimed to elucidate the complex synergistic factors influencing semen quality by analyzing the associations between lifestyle and standardized measures of Social Support Rating Scale (SSRS), Fertility-related Quality of Life (FertiQoL), and FPI. This multidimensional approach offers novel insights for clinical management and intervention.
Materials and Methods
Participants
The objective of this study was to evaluate the impact of social support, fertility stress, and fertility quality of life on male semen quality. A total of 485 male participants were recruited from our hospital between May 2021 and April 2023. All participants underwent semen analysis and completed the structured questionnaires.
Inclusion criteria: (a) men of reproductive age engaging in regular unprotected sexual intercourse and whose wives have failed to conceive spontaneously within 12 months due to male factors, and whose women have regular menstruation and no significant abnormalities in gynecological fertility-related examinations; (b) voluntary participation with informed consent obtained prior to assessment.
Exclusion criteria: (a) patients with a major medical condition (e.g., malignancies, severe psychiatric disorders, severe chronic diseases); (b) a history of diagnosed psychological disorders, drug or substance abuse, alcohol addiction, experience of mind-body therapies or psychological interventions, or use of antipsychotic medications in the past 6 months; (c) inability to comprehend or independently complete the questionnaires.
Ethics Statement
All procedures performed in studies involving human participants were in accordance with the Declaration of Helsinki (as revised in 2013). The studies involving human participants were reviewed and approved by Ethics Review Committee of The First Affiliated Hospital of Xinjiang Medical University (Approval no.: 20210226-168). The patients/participants provided their written informed consent to participate in this study.
Grouping
All participants were classified into two groups, including low semen quality group and normal group, based on the semen analysis results. Classification criteria were established in accordance with the WHO Laboratory Manual for the Examination and Processing of Human Semen (6th Edition) (Organization, 2021). Referring to the lower reference limits (fifth percentile) derived from fertile men, participants were classified into the low semen quality group if they exhibited a sperm concentration of <16 × 10⁶/mL or a progressive motility of <30%. Conversely, those meeting or exceeding these thresholds were classified into the normal group (Supplemental Table S1).
Data Collection
For each participant, baseline characteristics were systematically collected, including age, height, weight, place of residence, educational level, income, smoking status, marital status, related disease, and occupational environmental exposures.
Social Support Rating Scale
Social support was evaluated using the SSRS, a 10-item instrument for extensive validation of mental health in China (Xiao, 1994). Items 1–4 and 8–10 are single-choice questions scored on a 4-point scale (1–4). Item 5 consists of four sub-items (A–D), each scored from 1 (“no support”) to 4 (“full support”). For Items 6 and 7, a score of 0 is assigned for “no source,” while other responses are scored based on the count of identified support sources. The total score is the summation of all items, comprising three subscales: objective support (sum of Items 2, 6, and 7), subjective support (sum of Items 1, 3, 4, and 5), and utilization of support (sum of Items 8, 9, and 10). Consistent with established criteria, total scores were categorized into three levels: low (<22), moderate (22–44), and high (>44) (M. Hu et al., 2025).
FertiQoL
FertiQoL is a self-administered instrument jointly developed by experts from the European Society of Human Reproduction and Embryology (ESHRE) and the American Society for Reproductive Medicine (ASRM) (Boivin et al., 2011). It was designed to provide a precise assessment of quality of life specifically in patients with infertility. The 36-item scale comprises two primary modules: the Core FertiQoL (e.g., Emotional, Mind-Body, Relational, and Social subscales) and the Treatment FertiQoL (e.g., Treatment Environment and Treatment Tolerability). Raw scores for each subscale and the total scale are transformed into a standardized range of 0–100, where higher scores indicate superior fertility-related quality of life.
Fertility Problem Inventory
Fertility stress was evaluated using the FPI (Newton et al., 1999). This 46-item instrument comprises five subscales: social concern (10 items), sexual concern (8 items), relationship concern (10 items), need for parenthood (8 items), and rejection of childfree lifestyle (10 items). Responses are rated on a 6-point Likert-type scale ranging from 1 (strongly disagree) to 6 (strongly agree). Higher aggregate scores indicate higher levels of fertility-related stress.
Statistical Analysis
All statistical analyses were performed using R software. Continuous variables with a normal distribution were expressed as mean ± standard deviation (SD), while non-normally distributed data were presented as median (interquartile range, IQR). Categorical variables were described as frequencies (%). Comparisons between two continuous groups were conducted using the independent samples t-test or the Mann–Whitney U test, as appropriate based on data distribution. Categorical variables were compared using the χ² test. To identify independent risk factors associated with sperm quality, variables with a p < .10 in the univariate analysis were entered into a backward stepwise logistic regression model. Statistical significance was defined as a p-value less than .05.
Results
Baseline Demographic Characteristics
A total of 485 men were included in this study, including 256 (52.8%) in the normal group and 229 (47.2%) in the low semen quality group with at least one abnormal sperm parameter. The baseline demographic, lifestyle, and occupational characteristics of the two groups are presented in Table 1.
Baseline Demographic Characteristics.
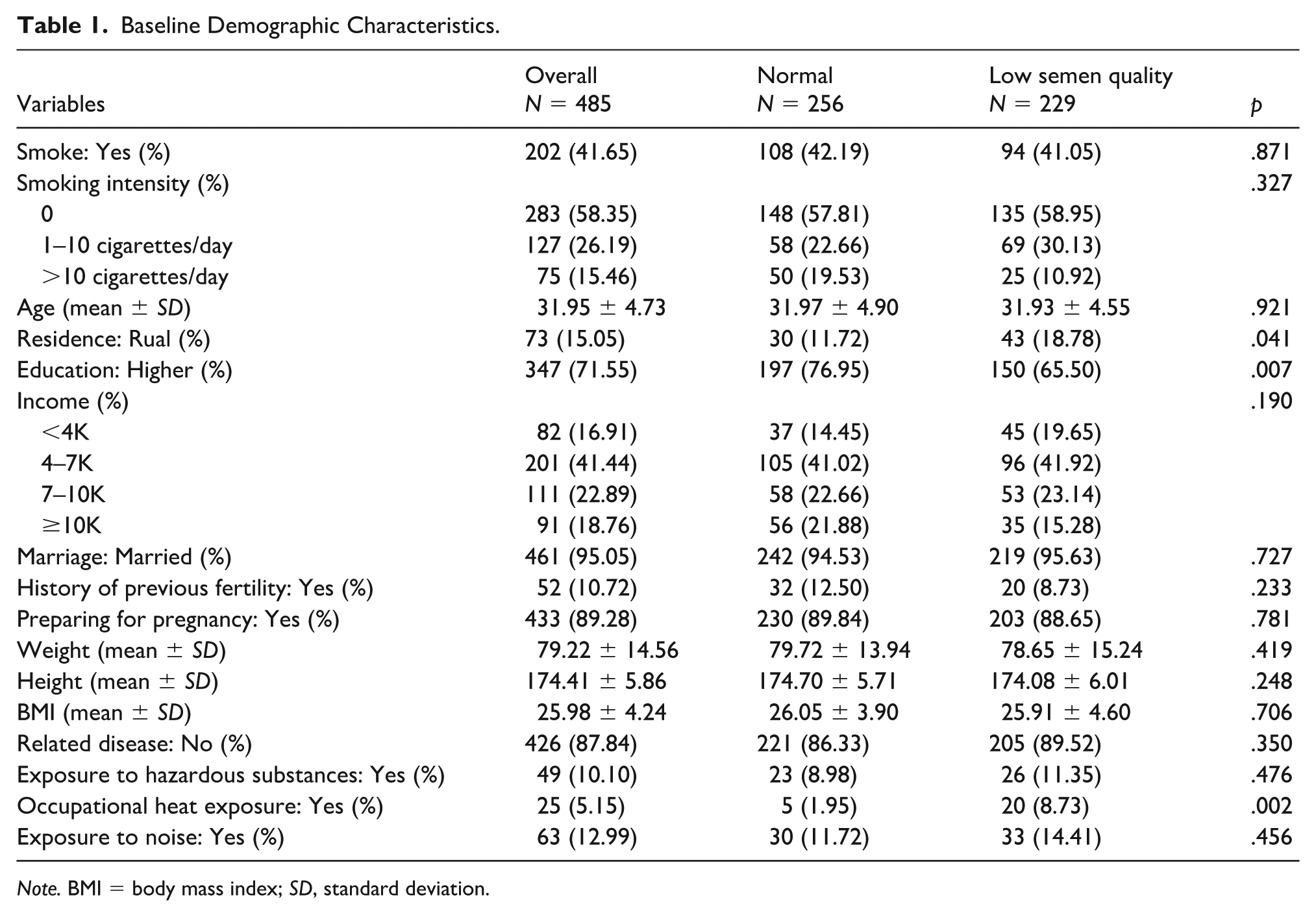
Note. BMI = body mass index; SD, standard deviation.
The two groups were comparable in terms of age, with mean ages of 31.97 ± 4.90 years in the normal group and 31.93 ± 4.55 years in the low semen quality group (p = .921). No significant differences were found in body mass index (BMI, p = .706), weight (p = .419), height (p = .248), income (p = .190), marital status (p = .727), history of previous fertility (p = .233), preparing for pregnancy (p = .781), self-reported related diseases (p = .350), exposure to hazardous substances (p = .476), or noise exposure (p = .456). The smoking status (p = .871) and smoking intensity (p = .327) were similar, but there was a higher proportion of light-to-moderate smokers (1–10 cigarettes/day) in the low semen quality group (30.13% vs. 22.66%) and a higher proportion of heavy smokers (>10 cigarettes/day) in the normal group (19.53% vs. 10.92%).
Notable differences between the two groups were observed in several variables. The low semen quality group had a significantly lower proportion of participants with higher education (65.50% vs. 76.95%; p = .007) and a higher prevalence of rural residence (18.78% vs. 11.72%; p = .041) compared to the normal group. Furthermore, occupational exposure to high temperatures was markedly more frequent in the low semen quality group than in the normal group (8.73% vs. 1.95%; p = .002).
The Relationship Between Social Support and Semen Quality
Social support assessed by SSRS is presented in Table 2. The mean total SSRS score in the overall cohort was 38.81 ± 7.27. The low semen quality group tended to have lower total SSRS scores than the normal group (38.20 ± 7.02 vs. 39.35 ± 7.46, p = .083). Then, a significant difference (p = .032) was observed in social support levels (low, moderate, and high) according to established SSRS cutoff values. Men in the low semen quality group were more likely to have moderate or low social support and less likely to have high social support. The objective support has a lower trend in the low semen quality group (p = .067), whereas subjective support and support utilization did not present a significant difference between groups (p = .231 and p = .626, respectively).
SSRS Scores in the Two Groups.
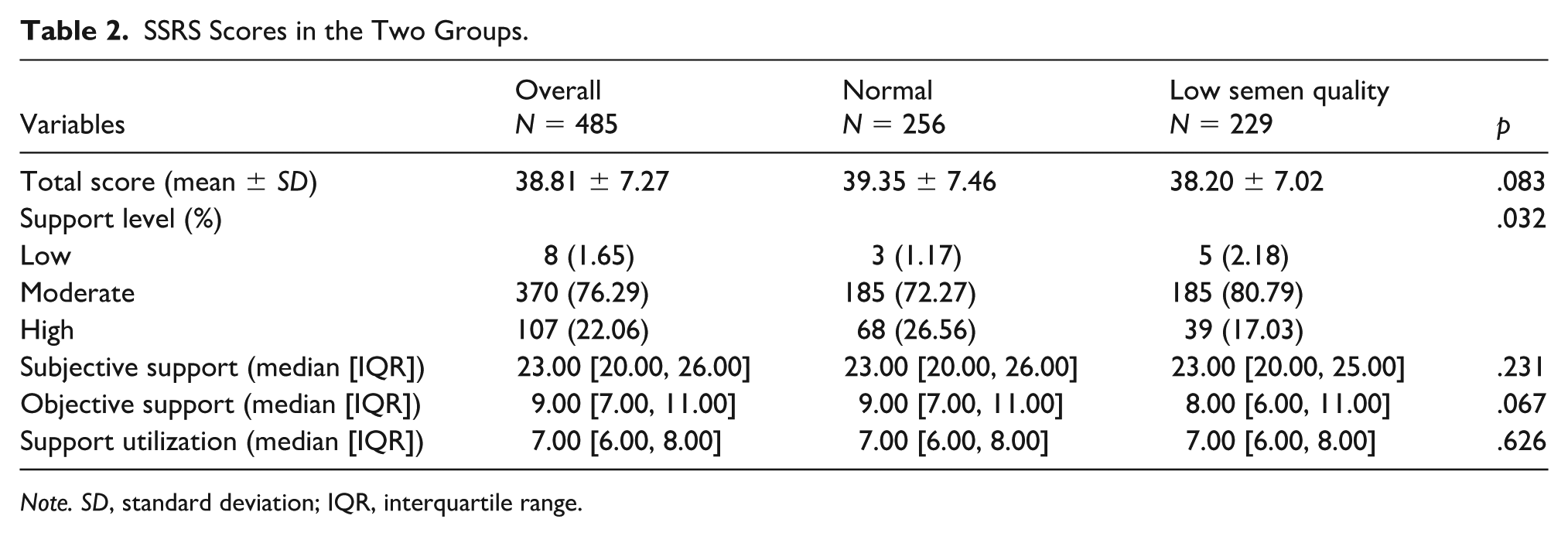
Note. SD, standard deviation; IQR, interquartile range.
The Relationship Between FertiQoL and Semen Quality
The results of FertiQoL (Table 3) presented that the total score in the low semen quality group is significantly lower than that in the normal group (median 68.38 [IQR 59.56–77.94] vs. 70.59 [61.58–81.80], p = .044). Similarly, the Core FertiQoL score, which assesses general fertility-related well-being, was significantly elevated in the normal group (p = .028). In the subscale analysis of the core scale, significant differences were observed in Emotional (p = .037), Mind-Body (p = .045), and Social (p = .033) domains. No statistically significant difference was found in the Relational domain (p = .289). Regarding the Treatment subscale, no statistically significant difference was found in Environment (p = .590) and Tolerability (p = .270) domains.
FertiQoL Scores in the Two Groups.
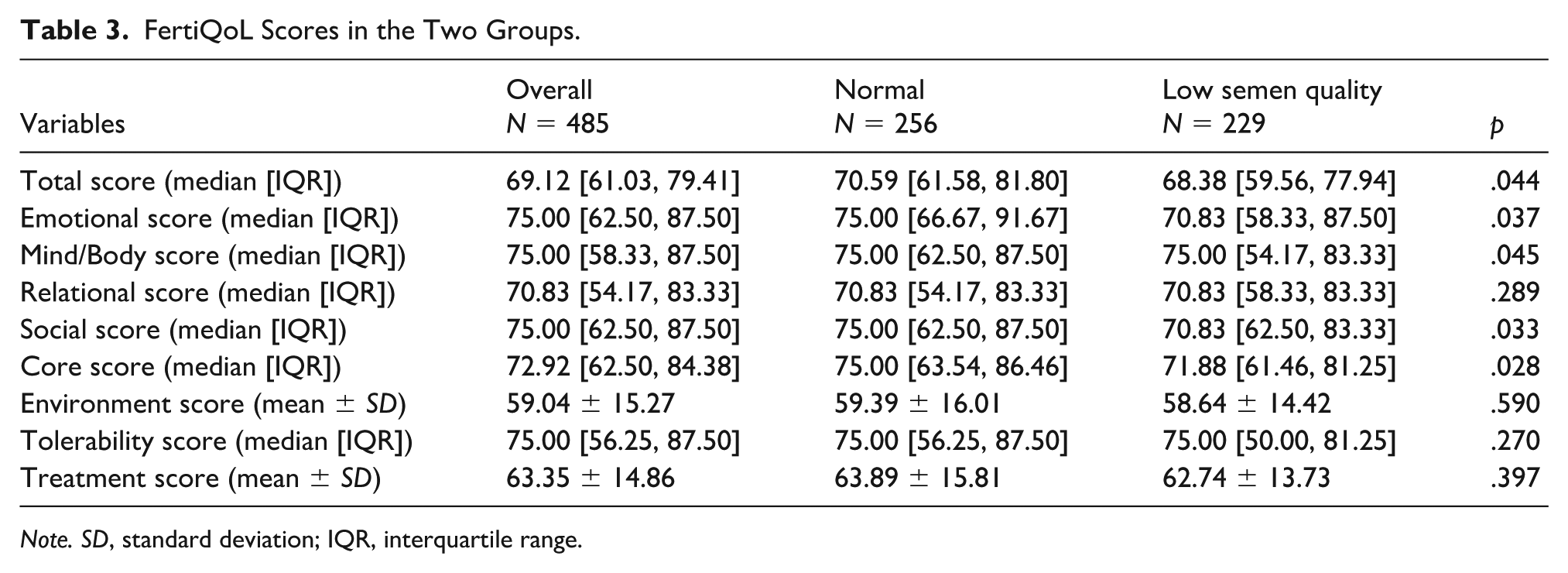
Note. SD, standard deviation; IQR, interquartile range.
The Relationship Between Fertility Stress and Semen Quality
Table 4 presents the analysis of fertility stress using the FPI. The results indicate that the low semen quality group experienced significantly higher levels of stress compared to the normal group. Specifically, the total FPI score was significantly higher in the low semen quality group (168.22 ± 33.85) compared to that in the normal group (161.30 ± 34.37; p = .026). In the analysis of specific stress domains, the low semen quality group consistently reported higher levels of concern. Significant differences were observed in social concern (p = .024), sexual concern (p = .012), and relationship concern (p = .044). However, no significant differences were found in the scores for Rejection of childfree lifestyle (p = .201) and Need for parenthood (p = .279) between the two groups.
FPI Scores in the Two Groups.
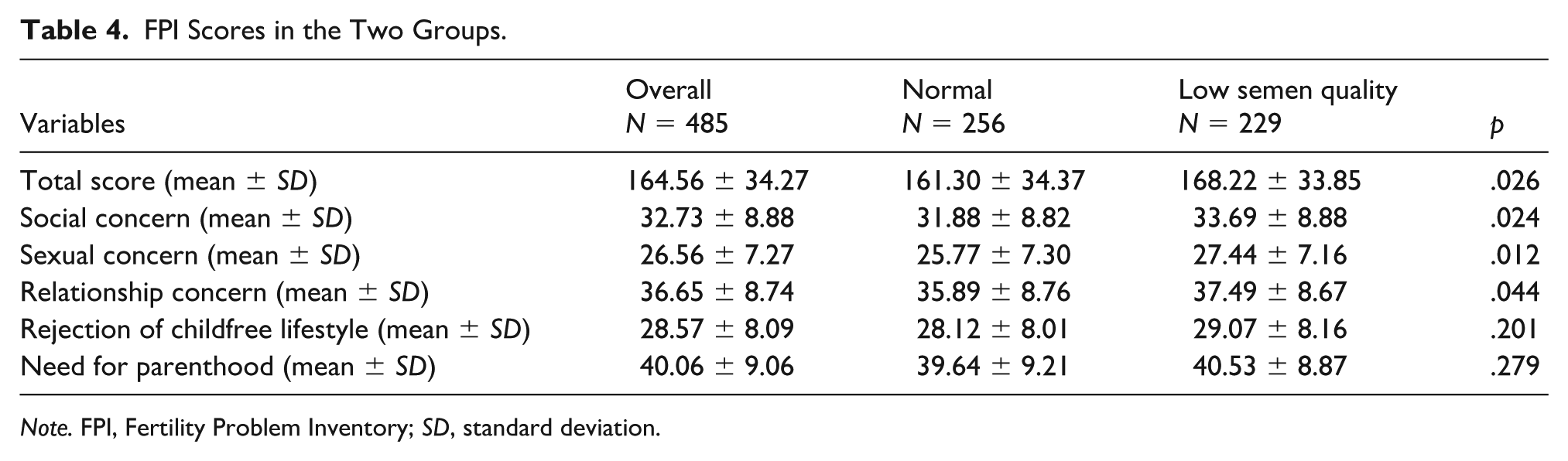
Note. FPI, Fertility Problem Inventory; SD, standard deviation.
Stepwise Analysis of the Variables Affecting Semen Quality
To identify independent factors associated with low semen quality, a multivariate logistic regression analysis was performed. Variables that with a p value of less than .1 in the univariate logistic analysis (e.g., rural residence, higher education, occupational heat exposure, total SSRS score, total FertiQoL score, and total FPI score) and smoking intensity were entered into a backward stepwise selection (Table 5). Three factors were associated with semen quality, including education level, occupational heat exposure, and fertility stress. Individuals exposed to high temperatures in their work environment had an increased risk of semen abnormalities compared to those unexposed (adjusted OR = 4.188, 95% confidence interval [CI]: [1.527, 11.484], p = .005). Higher education levels were associated with a reduced likelihood of semen abnormalities (adjusted OR = 0.624, 95% CI: [0.415, 0.937], p = .023). For every 1-point increase in the FPI score, the odds of low semen quality increased by 0.5% (adjusted OR = 1.005, 95% CI: [1.000, 1.011], p = .068), suggesting that higher stress levels are associated with low semen quality.
Multivariate Logistic Regression Analysis.
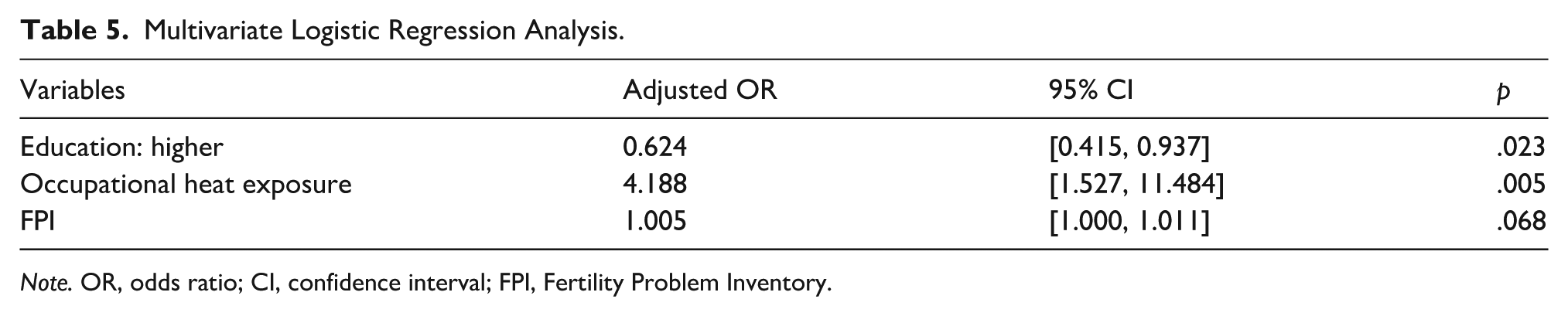
Note. OR, odds ratio; CI, confidence interval; FPI, Fertility Problem Inventory.
Discussion
This study provides a multidimensional analysis integrating demographic, environmental, and psychological variables. Our principal finding is that occupational heat exposure and fertility stress, which is assessed by FPI, are significant independent risk factors for impaired semen quality. Higher educational level acts as a protective factor. Our study underscores that semen quality is influenced not only by external environmental exposure but also by psychological determinants, specifically fertility stress.
Epidemiologic evidence suggests that heat exposure compromises male reproductive potential. Register-based data in Danish firefighters suggest that chronic full-time service is associated with higher male infertility, whereas part-time work shows no significant risk (Petersen et al., 2019), consistent with an exposure–dose relationship and a potential healthy-worker effect. A large longitudinal cohort study in south China further indicated the association between heat exposure and semen quality (Deng et al., 2023). The evidence indicated a nonlinear temperature–semen association, with declines in sperm count and morphology at higher environment temperatures and during heat waves, and window-specific susceptibility across spermatogenesis. A large Argentine retrospective study involving approximately 55,000 men demonstrated that exposure to heat waves during spermatogenesis was associated with significant reductions in sperm concentration, total sperm count, and normal sperm morphology, with the magnitude of impairment increasing with prolonged heat wave duration (Verón et al., 2024). These findings align closely with our observation of impaired semen quality linked to occupational high-temperature exposure and provide robust epidemiological corroboration of the vulnerability of human spermatogenesis to thermal stress. Mechanistically, heat exposure most likely impairs sperm quality through multiple damaging pathways targeting both germ cells and their supporting somatic microenvironment. Evidence indicated that chronic genital heat stress is associated with mitochondrial superoxide generation, loss of mitochondrial membrane potential, and increased DNA fragmentation, consistent with the activation of the intrinsic apoptotic program in ejaculated sperm (Budzinska et al., 2024; Ziaeipour et al., 2021). Heat stress may also compromise Sertoli cell function by altering lipid metabolic signaling. For instance, a recent study indicated that heat stress upregulates arachidonic acid (AA), which subsequently triggers autophagy-related alterations (Y. Hu et al., 2024). This process is mediated by the elevation of reactive oxygen species (ROS) and the perturbation of the mitochondrial electron transport chain (e.g., Complexes I, II, and V). In a controlled human study involving short-term scrotal hyperthermia, isobaric tags for relative and absolute quantitation (iTRAQ)-based proteomic analysis revealed the downregulation of critical proteins associated with sperm flagellar structure and energy metabolism (e.g., AKAP4, ODF1, and ODF2), which provide a molecular explanation for the compromised sperm motility following heat exposure (Y. Q. Wu et al., 2020).
We observed a protective effect of higher education. This association likely operates through indirect pathways rather than direct biological mechanisms. Glazer et al. conducted a large cross-sectional analysis of U.S. men undergoing semen analysis and found a clear educational gradient in semen quality and risk of oligospermia (Glazer et al., 2019). Compared with the reference group, men with high school education or lower qualification exhibited significantly higher odds of oligospermia, whereas those with a bachelor’s degree or higher showed a markedly lower risk. Similarly, large sperm-bank datasets in China report statistically significant variation in semen phenotypes by education level, supporting the plausibility that education-linked behaviors and work conditions permeate spermatogenic outcomes (Li et al., 2022). In a large-scale occupational study of Chinese sperm donors, the authors identified several associations between occupation and semen quality that remained robust across various statistical models (Tang et al., 2022). Notably, they explicitly stated that these associations were not significantly modified by confounding factors such as educational level. In a large-scale study conducted at a Chinese male infertility clinic, the authors observed that exposure to PM₁ was associated with declines in multiple semen parameters (Y. Zhang et al., 2023). However, these associations were generally homogeneous across education subgroups upon stratification. This suggests that educational attainment does not significantly alter the risk of semen impairment in the context of certain environmental exposures. In summary, we propose that educational level, unlike direct biological exposures, may exert an indirect influence on semen quality through mediating pathways such as occupational environment, access to health care, and behavioral lifestyle choices. Furthermore, the discrepancies in existing literature regarding the association between education and semen quality may be attributable to variations in study population sources, inadequate adjustment for occupational and behavioral confounders, and inherent selection bias.
A critical contribution of this study is the identification of fertility stress as an independent predictor of semen quality, even after adjusting for potential confounders. Our results suggest a dose-response relationship, where higher FPI scores are correlated with low semen parameters, consistent with some previous studies. Mireyi et al. stratified 1,024 males into normal and abnormal semen groups (Mireyi et al., 2025). In the abnormal semen group, a higher FPI score was negatively correlated with sperm concentration and total sperm count, whereas associations with motility parameters were weaker and non-significant. These findings suggest that fertility stress may predominantly impair the quantitative rather than the functional aspects of spermatogenesis. A study enrolling 718 men attending a fertility center employed the Perceived Stress Scale-4 (PSS-4; Reddy et al., 2025). When comparing the highest versus lowest stress quantiles, the authors observed significantly reduced total sperm counts and normal morphology counts. While an adverse trend was noted for certain DNA damage markers, not all DNA integrity or hormonal indices reached statistical significance. Collectively, these data support the notion that stress is associated with declines in specific dimensions of semen quality. Furthermore, a study of 1,362 young men compared three distinct stress instruments and revealed that perceived stress was inversely correlated with sperm concentration, total count, and motility in a dose-dependent manner. Conversely, stressful life events alone showed no significant association. These findings suggest that the subjective experience of stress may be a more sensitive predictor of semen quality than the mere accumulation of objective events. Mechanistic evidence further supports biological plausibility by implicating stress-related mitochondrial metabolic reprogramming (e.g., pyruvate dehydrogenase kinase-pyruvate dehydrogenase complex axis dysregulation) in impaired semen quality (W. Wang et al., 2025).
Interestingly, while univariate analyses indicated that men with low semen quality had lower SSRS and FertiQoL scores, these factors were not significant in the multivariate result. We interpretated that the impact of social support and general quality of life on semen quality may be mediated through stress levels. Social support likely mitigates the physiological impact of stress rather than directly enhancing spermatogenesis. Our perspective is consistent with a study focusing on the association between FertiQoL and semen parameters, which concurrently evaluated the moderating roles of social support and fertility stress (Mireyi et al., 2025). The results indicated a positive correlation between social support and total sperm motility specifically within the low semen quality group. The absence of a similar finding in the normal group suggests that social support does not exert a universal, reproducible effect across all populations. Interventions targeting stress reduction might be more clinically effective than general social support measures alone. We noted a paradoxical finding regarding smoking. A higher proportion of heavy smokers was observed in the normal semen group compared to the low semen quality group. It may reflect survivor bias, where men with robust innate spermatogenic potential maintain normal parameters despite heavy smoking, whereas those with lower baseline fertility are more easily affected even by light smoking (Ranganathan et al., 2019; S. Wu et al., 2025). In addition, self-reported smoking data may be subject to reporting bias. Nonetheless, the deleterious effects of tobacco on DNA integrity and semen quality are well-documented and should not be disregarded based on this finding (Åsenius et al., 2020; Cui et al., 2025).
It is crucial to acknowledge that the psychosocial constructs central to this study operate within a specific cultural and structural environment. The validity of self-reported data on stress and social support is inevitably influenced by cultural forces, such as norms of masculinity that may discourage help-seeking and the pervasive stigma of male infertility. Furthermore, structural markers like rurality and lower education are not simply control variables but indicators of systemic disadvantages that can independently heighten stress and limit resources. Acknowledging these contextual layers is essential for a nuanced interpretation of our findings and their clinical implications.
Several limitations of this study must be acknowledged. First, the cross-sectional design precludes the determination of causality. We cannot definitively state whether stress causes poor semen quality or if the diagnosis of poor semen quality elevates stress, although the biological plausibility supports the former or a bidirectional relationship. Second, semen quality was assessed based on a single sample, which may not account for the natural temporal fluctuation of sperm parameters. Third, the occupational heat exposure finding is based on a small subgroup (n = 25), resulting in a wide CI and warranting cautious interpretation until confirmed in larger studies. Finally, this study employed single-site, hospital-based recruitment, which may limit generalizability. Men attending a fertility clinic represent a help-seeking subpopulation; individuals who do not seek care due to stigma, cost, or access barriers were not captured. Therefore, findings may not fully apply to the general male population. Future studies with repeated sampling and measurements of physiological stress markers are essential to validate these findings.
Conclusion
This study highlights the critical “mind–body” interaction in male reproductive health. We identified occupational heat exposure and fertility-related stress as independent risk factors for impaired semen quality, whereas higher education served as a protective factor. These findings advocate for a multidisciplinary clinical approach, integrating psychological screening and stress management with occupational health guidance to optimize male fertility outcomes.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883261454721 – Supplemental material for Occupational Heat Exposure and Fertility Stress as Independent Factors of Low Semen Quality: A Multidimensional Analysis
Supplemental material, sj-docx-1-jmh-10.1177_15579883261454721 for Occupational Heat Exposure and Fertility Stress as Independent Factors of Low Semen Quality: A Multidimensional Analysis by Ningning Han, Zhijuan Liu, Lijuan He and Rui Han in American Journal of Men's Health
Footnotes
Ethical Considerations
All procedures performed in studies involving human participants were in accordance with the Declaration of Helsinki (as revised in 2013). The studies involving human participants were reviewed and approved by Ethics Review Committee of the First Affiliated Hospital of Xinjiang Medical University (approval no.: 20210226-168).
Consent to Participate
The patients/participants provided their written informed consent to participate in this study.
Consent for Publication
Not applicable.
Author Contributions
Conceptualization: Rui Han. Formal analysis: Ningning Han. Funding acquisition: Rui Han and Lijuan He. Investigation: Ningning Han and Zhijuan Liu. Methodology: Lijuan He. Project administration: Rui Han. Writing – original draft: Ningning Han. Writing – review and editing: Rui Han, Lijuan He, and Zhijuan Liu. All authors read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the “Tianshan Talents” Training Program for High level Talents in Medicine and Health (TSYC202401B126), State Key Laboratory of Pathogenesis, Prevention and Treatment of High Incidence Diseases in Central Asia, Xinjiang Medical University (SKL-HIDCA-2024-GX3), and Xinjiang Key Laboratory of Special Environment and Health Research Open Subjects (SKL-SEHR-2021-05).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.