
Abstract
More men live alone than ever before, and this increases their risk for mortality. In-hospital studies for men who have struggles associated with living alone have not been amply studied. We used the 2022 National Inpatient Sample to explore hospital outcomes among men with “problems living alone.” Using multivariable regression analyses, we examined in-hospital mortality, length of stay, total hospital charges, and post-discharge disposition. In 2022, 12,109,441 men were admitted to U.S. hospitals. Overall, 45,860 (0.4%) were coded for problems related to living alone, and 12,063,581 (99.6%) were not. Men with problems living alone were older (62.1 ± 17.4 vs. 67.3 ± 15.7; p < .01) and had a higher comorbidity burden, indicated by the Elixhauser mean score (4.04 ± 2.3 vs. 4.35 ± 2.1; p < .01). Men with problems living alone had lower mortality (adjusted odds [aOR] = 0.7; 95% confidence interval [CI] = [0.61, 0.83]; p < .01) and lower hospital charges (adjusted mean difference [aMD] = −$6,374; 95% CI = [−9,707, −3,040]; p < .01). However, they had longer stays (aMD = +0.7 days; 95% CI = [0.52, 0.97]; p < .01) and lower odds of being discharged home (aOR = 0.61; 95% CI = [0.57, 0.64]; p < .01). Men with problems living alone had different in-hospital findings than other men; some of these were surprisingly distinctive. Interventions during hospitalization may be supportive and help optimize reductions in health care resource utilization.
Introduction
The number of men living alone has been increasing, especially in industrialized countries. In the United States, 38 million households now consist of a single person, representing 29% of the national total. This demographic shift has significant implications for public health, particularly for men. Living alone, a common and objective proxy of social isolation, is associated with mortality in a wide variety of clinical populations and population-based cohorts (Gopinath et al., 2013; Pimouguet et al., 2016; Schmaltz et al., 2007; Steg, 2012). While such associations are population-based, the impact of living alone on outcomes during acute hospitalizations, such as in-hospital mortality, length of stay (LOS), and hospital charges, has not been adequately studied.
Approximately 25% of older adults who live alone are also socially isolated – meaning they have a lack of contact with family or friends (Teo et al., 2023). This may increase one’s risk for delayed hospital arrivals to receive rapid interventions in the setting of acute medical events, such as stroke (Reeves et al., 2014) or heart attacks (Ohama et al., 2020). As such, a significant risk of morbidity and mortality affects this patient population.
This study sought to compare in-hospital clinical and resource utilization outcomes between men who had problems living alone and those who did not. We hypothesized that mortality and resource utilization outcomes among hospitalized men with problems living alone would be worse compared to those without this hardship.
Methods
Setting/Database
We used data from the National Inpatient Sample (NIS) database for the year 2022. NIS data are accessible through the Agency for Healthcare Research and Quality’s Healthcare Cost and Utilization Project (HCUP) (National Inpatient Sample (Healthcare Costs and Utilization Project), 2025). The NIS is a publicly available all-payer inpatient health care database for hospitals in the United States. The database approximates a 20% stratified sample of hospital discharges from 47 participating states, plus the District of Columbia. There were more than 6.5 million unweighted hospital stays in 2022. It is estimated that over 32 million hospitalizations occurred in 2022 when weighted to represent all admissions. This represented 95% of hospitalizations in the U.S. Strata include hospital size/volume, academic teaching status, geographic region, and hospital ownership. The current study uses the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) coding system for all discharge diagnoses.
Study Population, Patient and Hospital Characteristics, and Outcomes
Male patients were extracted from the database; females were excluded. The ICD-10 code Z60.2 (problems related to living alone) was used to distinguish between men who struggled with living alone and those who did not. In-hospital mortality was the primary outcome. Secondary outcomes included LOS and total hospital charges and discharge disposition following hospitalization. We controlled for the following a prior hospital and patient confounders in our multivariable regression models: (a) hospital teaching status, (b) hospital volume capacity, (c) age; (d) insurance (Medicare, Medicaid, Private Insurance, Uninsured); (e) median household income (from <$38,999 to >$63,000 based on home zip code); (f) severity of illness (no class specified, minor loss of function, moderate loss of function, major loss of function, and extreme loss of function); (g) risk of mortality (no class specified, minor likelihood of dying, moderate likelihood of dying, and extreme likelihood of dying), and (h) comorbidity burden assessed using the Elixhauser comorbidity index – this variable consisted of 30 comorbidities to measure chronic conditions and was created for in-hospital administrative databases to predict in-hospital outcomes (Elixhauser et al., 1998). The top five admitting diagnoses for both study populations were also assessed.
The study was deemed exempt by our hospital’s Institutional Review Board; the institution and approval code were anonymized for review.
Statistical Analysis
The adjusted Wald tests were used for categorical and continuous variables. Adjusted odds ratios [aORs] for in-hospital mortality were attained via multivariable logistic regression. Adjusted mean differences [aMDs] from multivariable linear regression analyses were used to compare LOS and total hospital charges. The p-values were two-sided, and the significance level of type I errors was 0.05. Stata 18.0 statistical software (StataCorp, College Station, TX, USA) accounted for design complexity (stratification, weighting, and clustering) and incorporated strata, primary sampling weights, and secondary sampling weights.
Results
In 2022, 12,109,441 men were admitted to U.S. hospitals. A total of 45,860 (0.4%) were coded as having problems related to living alone, and 12,063,582 (99.6%) were not. Patients who had problems living alone were older (62.1 ± 17.4 vs. 67.3 ± 15.7; p < .01) and had a higher comorbidity burden – Elixhauser mean score (4.04 ± 2.3 vs. 4.35 ± 2.1; p < .01). Additional patient and hospital characteristics are shown in Table 1. The top five admitting diagnoses for men with problems living alone versus those who did not are also shown in Supplemental Table 1.
Patient and Hospital Demographics From the 2022 National Inpatient Sample, Comparing Men With Problems Related to Those Who Do Not.
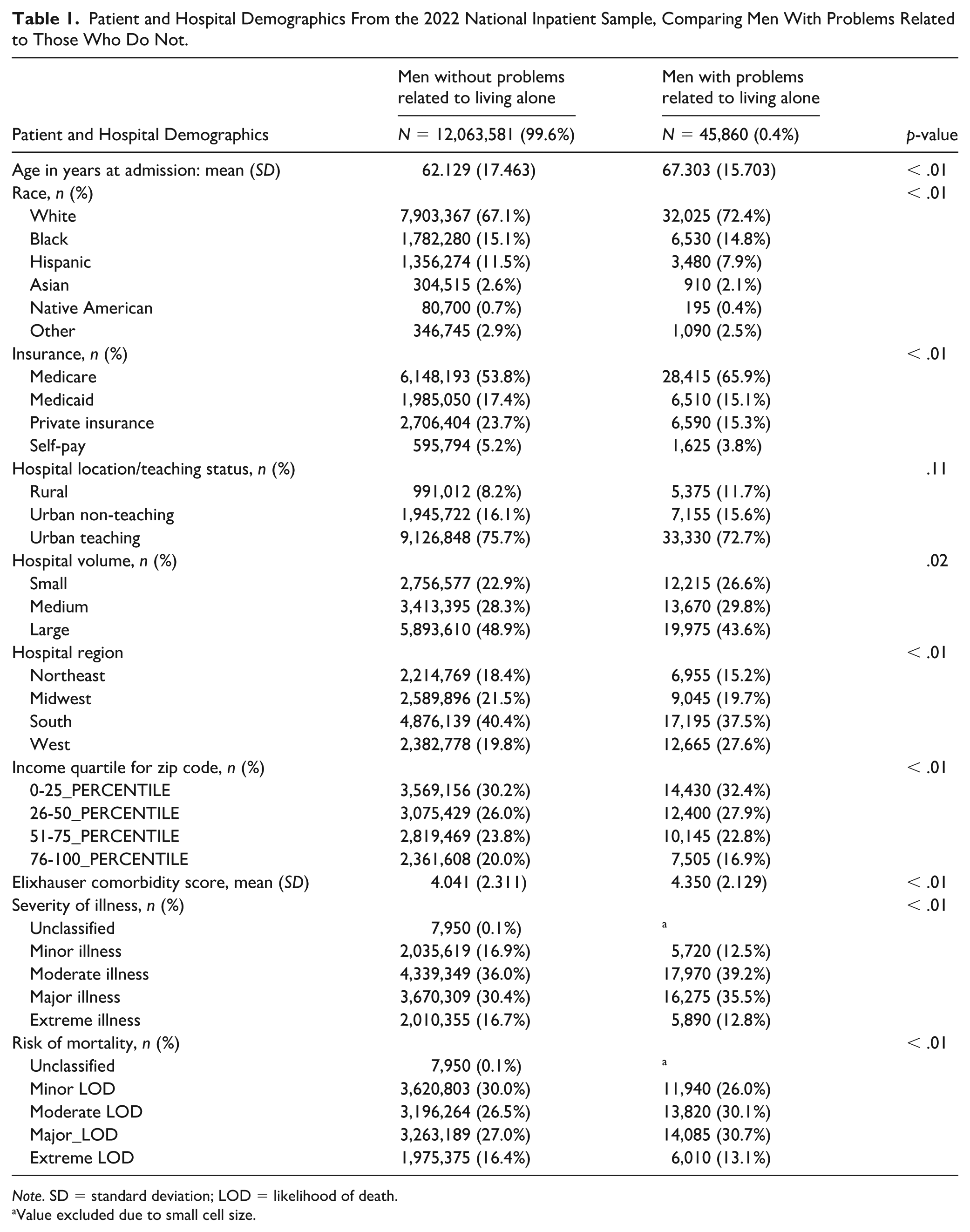
Note. SD = standard deviation; LOD = likelihood of death.
Value excluded due to small cell size.
Men with problems living alone had lower mortality (aOR = 0.70; 95% confidence interval [CI] = [0.61, 0.83]; p < .01) and less hospital charges (aMD = −$6,374; 95% CI = [−9,707, −3,040]; p < .01) compared to those who did not. Patients with problems living alone had a longer LOS (aMD = +0.7 days; 95% CI = [0.52, 0.97]; p < .01) and lower odds of being discharged home after hospitalizations (aOR = 0.61; 95% CI = [0.57, 0.64]; p < .01). All unadjusted and adjusted mean differences and odds ratios are shown in Table 2.
Mean Differences and Odds Ratios for Inpatient Outcomes of Hospitalized Men – Those With Problems Living Alone to Those Who Did Not: National Inpatient Sample Database (2022).
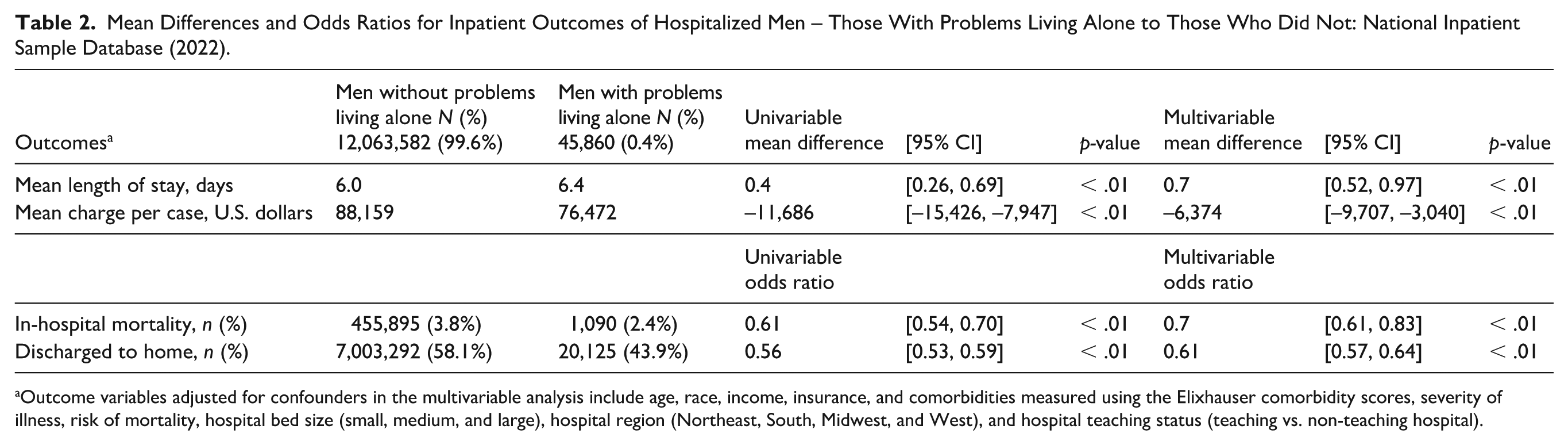
Outcome variables adjusted for confounders in the multivariable analysis include age, race, income, insurance, and comorbidities measured using the Elixhauser comorbidity scores, severity of illness, risk of mortality, hospital bed size (small, medium, and large), hospital region (Northeast, South, Midwest, and West), and hospital teaching status (teaching vs. non-teaching hospital).
Discussion
In this analysis of data from this large nationwide database, there were some odd or unexpected results for men with problems living alone; these men had longer lengths of stay but lower charges – usually these two outcomes are highly correlated and certainly tend to go in the same direction. These patients were less likely to be discharged home, perhaps suggesting hesitancy related to support or safety concerns, thereby prolonging their hospitalization without significant ongoing inpatient testing or management. Because all hospitals focus on capacity and throughput, these results might suggest the need for earlier and more comprehensive input from the entire multidisciplinary team to prevent extended hospital stays and promote efficient discharges among this subgroup of patients.
This study found that men living alone had paradoxically lower adjusted odds of in-hospital mortality. This finding stands in contrast to most studies, which correlate living alone and social isolation with a higher risk of long-term, all-cause mortality, particularly for men (Berkman & Syme, 1979; Seeman et al., 1987). By contrast, and similar to our mortality result, a study focusing on older (>65 years) home care recipients in Canada, Finland, and Aotearoa found that loneliness was independently associated with a lower likelihood of mortality (Egbujie et al., 2025). Notably, patients in that study received some form of home care, with regular check-ins. Another study based on the Chinese Longitudinal Healthy Longevity Survey found that the risk of all-cause mortality was significantly lower among older adults living alone than among those living with families or in nursing homes (Pu et al., 2023). This was attributed to differences in health status and the quality of alternative care settings (nursing homes and family care settings). Some studies show delays in hospital presentation among patients who live alone (Ohama et al., 2020; Reeves et al., 2014). It has been shown that individuals living alone and lacking support may present to hospitals earlier in the course of an illness (Hastings et al., 2008), when they might not have been as sick as others (Lowthian et al., 2012). We could not determine details of patient support prior to admission, and we also adjusted for the severity of illness and risk of mortality of our patients. Additional studies should be conducted to better identify the risk factors contributing to these patients’ outcomes.
Regarding health care utilization, Dramé and colleagues (2012) reported that older adults who live alone are significantly more likely to use emergency departments. This pattern suggests that these men with limited social support may seek medical care earlier or may not be severely ill. Consequent hospitalizations for these less severe conditions should logically translate into better outcomes and lower per-admission costs.
Multidisciplinary approaches that use hospital social workers and case managers may help address challenges in health care utilization (Fabbre et al., 2011). With many patient groups, such as men having problems associated with living alone, there can be lengthy delays with discharges – even after the patient is deemed medically ready. Studies specifically focusing on social workers’ roles show their involvement in patient care, through early assessment of complex psychosocial needs and coordination with community resources, is critical for reducing hospital LOS (Fabbre et al., 2011; Parry et al., 2008).
Several limitations of this study must be considered. First, the diagnosis of “problems related to living alone” (Z60.2) may be underutilized and does not provide granular details about the nature of the “problem.” While this coding provides a useful framework, our analysis relies on the accuracy of the ICD-10-CM coding system. Second, the database lacks information on home support structures. Hence, we were unable to determine if patients had home visits or check-ins. Third, as an observational study, our findings demonstrate association, not causation. Fourth, it is possible that some of the subtle differences in the admitting diagnoses between the two groups may have accounted for some of the observed differences in outcomes – despite the large N and adjustments for covariates in the regression. Finally, this study’s findings may be explained by survivor bias. Theoretically, men who had problems living alone with the most severe illnesses and mortality risk died before reaching the hospital. Therefore, the population in this inpatient database may have been a slightly more resilient cohort; the same bias might also have been expected in the control group. Despite those limitations, we were able to analyze a large number of patients using NIS, a vast and nationally representative all-payer database. Our study expanded the scope of research to include underrepresented populations.
Conclusion
When men with problems living alone are admitted to our nation’s hospitals, they experience longer hospital stays, and fewer can be discharged home. However, they have a lower risk of mortality and lower charges. The results of this study may help clinicians recognize that the patients are at high risk for complex discharge planning. Early engagement of case managers and social workers at admission may be crucial to mitigate discharge delays, improve system efficiency, and ensure equitable care for this vulnerable group of men.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883261454724 – Supplemental material for Outcomes for Hospitalized Men Noted to Have Problems Associated With Living Alone in the United States
Supplemental material, sj-docx-1-jmh-10.1177_15579883261454724 for Outcomes for Hospitalized Men Noted to Have Problems Associated With Living Alone in the United States by Emmanuel Tito, Sumedha Nallamothu, Thang Nguyen, Saanvi Dixit, Scott Mitchell Wright and Che Matthew Harris in American Journal of Men's Health
Footnotes
Acknowledgements
Dr. Scott M. Wright is the Anne Gaines and G. Thomas Miller Professor of Medicine supported through Hopkins’ Center for Innovative Medicine, and he is the Mary Gallo Scholar for Hopkins’ Center for Humanizing Medicine.
Ethical Considerations
This study received ethical approval from the Johns Hopkins Institutional IRB (Approval No. 00518068) on August 1, 2025. This is an IRB-approved retrospective study; all patient information was de-identified, and patient consent was not required. Patient data will not be shared with third parties.
Consent to participate
Not sought, as the National Inpatient Sample (NIS) database contains only de-identified, secondary data.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.