
Abstract
Permanent supportive housing (PSH) has been recognized by the U.S. federal government as the “clear solution” to chronic homelessness. Whether and how access to PSH affects HIV risk is unclear. This mixed methods pilot study uses a convergent parallel design in order to better understand social relationships and HIV risk during the transition from homelessness to PSH. Findings suggest that (a) Sexual activity and HIV risk behaviors increase with housing, (b) Social network size and composition appear to change as individuals transition into PSH, and (c) There is tension between moving forward and leaving behind the past once a person has housing. This study demonstrates that PSH constitutes a specific risk environment that has not been previously investigated.
Individuals who have experienced chronic homelessness, many of whom have co-occurring mental illness and substance use disorders, tend to have attenuated social networks consisting of limited social capital (Hawkins & Abrams, 2007; Trumbetta, Mueser, Quimby, Bebout, & Teague, 1999). Research involving samples of homeless individuals who use subsistence services has shown that social networks are, to a notable extent, composed of individuals who drink, use drugs, and engage in HIV risk behaviors (Tucker, Wenzel, Golinelli, Zhou, & Green, 2011; Wenzel et al., 2012), yet may also include some people who do not engage in such risk behaviors and who offer support and emotional closeness (Tucker et al., 2009). Network members can either positively or negatively influence one another’s behaviors through social comparison processes, social sanctions and rewards, information exchange, and socialization of members (Kennedy et al., 2010; Latkin, Mandell, & Vlahov, 1996). In the case of homeless individuals with a preponderance of network members engaging in risky behaviors, the syndemic that results from such concentrated disadvantage and excess disease burden, including high rates of HIV (Singer & Clair, 2003), is both a cause and consequence of long-term homelessness (Drake, Osher, & Wallach, 1991).
Offering permanent supportive housing (PSH) using a housing first approach has been recognized by the U.S. federal government as the “clear solution” to chronic homelessness (U.S. Interagency Council on Homelessness, 2010). This approach refers to providing immediate access to affordable housing that is accompanied by supportive health and social services. PSH has been credited with reducing the number of chronically homeless individuals since 2006 (U.S. Department of Housing and Urban Development, 2010). In addition to being effective at ending homelessness (Collins et al., 2012; Pearson, Montgomery, & Locke, 2009; Tsemberis, Gulcur, & Nakae, 2004) and consistent with basic human rights (Office of the High Commissioner for Human Rights, 1976), PSH has been found to be cost-effective when serving people with complex health and social needs (Culhane, 2008; Culhane, Metraux, & Hadley, 2002).
Despite the obvious benefits of PSH and the empirically established association among homelessness, housing, and HIV risk (Culhane & Gollub, 2001; Dunn & Hayes, 1999; Latkin, German, Vlahov, & Galea, 2013; Shaw, 2004; Weir, Bard, O’Brien, Casciato, & Stark, 2007), studies of HIV risk behaviors among chronically homeless individuals in PSH are still limited. Although HIV risk has been investigated among people living with HIV/AIDS (PLWHA), little data exist on HIV risk behaviors among individuals entering supportive housing not intended for PLWHA. Among PLWHA who received housing, 50% of residents reported having had unprotected sex at the time of follow-up interviews (Aidala, Cross, Stall, Harre, & Sumartojo, 2005). Another study found that housed PLWHA were more likely to be sexually active than homeless PLWHA (Kidder, Wolitski, Pals, & Campsmith, 2008). Housing does not necessarily address well-documented individual HIV risk factors among adults who have experienced homelessness, such as inconsistent use of condoms (Tucker et al., 2013), multiple or concurrent partners (Wenzel et al., 2012; Wenzel, Tucker, Elliott, & Hambarsoomians, 2007), or medically inaccurate beliefs about HIV transmission (Brown et al., 2012). Furthermore, individuals with histories of chronic homelessness living in PSH may experience limited community integration and continued marginalization even with prolonged PSH tenure (Tsai, Mares, & Rosenheck, 2012; Yanos, Stefancic, & Tsemberis, 2012). Although individuals living in PSH can develop social connections once housed, prosocial network ties that can mitigate HIV risk taking (Rice, Milburn, & Rotheram-Borus, 2007; Rice, Stein, & Milburn, 2008; Wenzel et al., 2009) may be harder to develop in densely populated and disadvantaged neighborhoods where PSH is often located (Byrne et al., 2013; Wong & Stanhope, 2009). Furthermore, having housing might facilitate sexual intimacy (Henwood et al., 2013; Padgett, Henwood, Abrams, & Drake, 2008) and therefore increase the risk of HIV transmission in the absence of condom use, for example. Research has also shown that a significant minority of individuals in PSH experience social isolation and loneliness, whether by choice or because of an inability to connect with others (Rhoades et al., 2011). Limited social integration and a contraction of social networks, which may result in a lower quality of life, could also reduce HIV risk.
To better understand social relationships and HIV risk during the transition from living on the streets to PSH, we conducted a mixed methods longitudinal pilot study that was intended to inform the design of a larger study. Since research about social networks processes is typically either quantitative or ethnographic in nature, this study may appeal to a multidisciplinary mixed methods audience concerned about complex social issues. In this case, having housing may represent an improved opportunity for intimacy and longer term relationship building (Brown et al., 2012; Yanos, Barrow, & Tsemberis, 2004); yet some homeless individuals may prefer to postpone intimate relationships unless or until they achieve more than residential stability, such as employment (Padgett et al., 2008). We suspect that, in general, intimate relationships might increase among individuals who secure housing because many view homelessness as a barrier to having intimate relationships (Bourgois, 1998; Brown et al., 2012; Brown, Kennedy, Tucker, Golinelli, & Wenzel, 2013); yet it is unclear if HIV risk behaviors also increase. Given such complexity, this study attempted to address the following research questions: (a) How do social networks change as individuals transition from homelessness to PSH? and (b) In what ways does the transition to PSH affect HIV risk behavior? Because these are independent yet related questions, we used a convergent parallel design in which quantitative and qualitative data were analyzed separately and findings merged during interpretation (Creswell & Plano Clark, 2011).
Method
This pilot study focused on homeless individuals transitioning into PSH through an organization in downtown Los Angeles from May through September 2012. This organization provides single-site PSH (yet has many buildings) that includes on-site case management and care coordination services. Participants were interviewed just before entering PSH and again approximately 3 months after transitioning into PSH using a mixed methods approach that involved conducting both quantitative surveys and qualitative semistructured interviews. Both types of data were collected at the same time with participants first completing the quantitative portion of the interview before being asked open-ended qualitative questions. The quantitative portion was not intended to inform the qualitative section, yet the focus of the former may have influenced participants’ responses to the latter.
Study Sample
Individuals were identified by street outreach workers or other agencies as eligible for housing (i.e., chronically homeless) and had secured lease agreements in preparation to move into PSH. Baseline interview appointments were made when a housing unit became available for each individual. The interviewer obtained written consent prior to the baseline interview. Participants were interviewed at the leasing office for the housing site an average of 15.4 days prior to entering housing. Two thirds of participants were housed within 15 days of being interviewed; 89% were housed within 30 days of the baseline interview. Of the 40 people who initially agreed to be interviewed, 33 individuals enrolled in the study at baseline. Twenty-five study respondents completed the follow-up interviews, which represents a 76% follow-up rate. Interviews were scheduled at a place and time convenient to each respondent, and the average time between baseline and follow-up interviews was 3.3 months (range: 2.8-4.1 months). The affiliated institutional review board approved the protocols for protecting human subjects for this study. Participants received $30 for each completed interview.
Quantitative Data
Demographic information regarding age, race and ethnicity, gender, education level, marital status, employment situation, and housing status was collected from all participants during the quantitative, interviewer-administered questionnaire. This questionnaire also contained a social network interview component, which asked respondents to name individuals they had been in contact with during the previous 3 months (at baseline) or since moving into housing (at follow-up). In social network parlance, these named individuals are referred to as alters. Questions assessed characteristics of alters and the relationship between alters and respondents. The following prompt was used to elicit alter nominations:
Now I’d like for you to name 20 people that you know and who know you. These should be people you have had contact with sometime during the past 3 months or so—either in person, by phone, mail or e-mail, or online. You can name any adults you know and who know you no matter who they are or where they live. Please name adults age 21 and older only—do not give me the names of those under age 21. These people you name should include the people you had sex with in the past 3 months, unless you feel you do not know them and they do not know you. Let’s start by naming people that are most important to you and then we’ll work outwards toward people who are less important to you.
An iPad application designed for social network interviewing was used and displayed a map of all named alters, allowing the respondent to point to or tap on relevant alters for each question. Each alter was listed in a box on the screen (represented only by initials), which would become highlighted when selected. Examples of social network questions include “Who can you count on to listen to you when you need to talk, or is someone you can confide in?” “Who have you felt emotionally close to most of the time during the past 3 months?” “Who is a service provider you met in a shelter or other housing location?” “Who have you ever had sex (anal, vaginal, or oral sex) with?” Each question was presented with a yes or no response option and alters meeting each question’s criteria were selected. Interview questions were based on those used in previous studies involving homeless adult men and women (Wenzel et al., 2012; Wong & Stanhope, 2009).
Changes in demographic, risk behavior, and social network characteristics between baseline and follow-up were examined. For risk behavior and social network characteristics, variables were created for each outcome of interest indicating whether that behavior or characteristic had increased, decreased, or remained unchanged between baseline and follow-up. For social network variables, changes were calculated by comparing proportions of the overall network to control for changes in network size between baseline and follow-up. Due to the small sample size, tests of statistical significance were not used. Rather, trends identified by comparing baseline and follow-up values are presented and explored.
Qualitative Data
Qualitative data collected at baseline focused on the importance of housing for homeless individuals in terms of conferring a sense of stability and ontological security that provide a base for relationship development and other aspects critical to promoting quality of life (Padgett, 2007). Baseline and follow-up interviews consisted of similar questions (e.g., “How will [or has] having your own place change [or changed] your relations with family, friends, other people?”) to provide insight into perceptions of social relationships with family, friends, and intimate partners and expectations of these relationships after being housed. Other questions included “What does your typical day look like?” and “How have things changed for you recently?” As noted, qualitative data collection was concurrent with the quantitative data collection but analyzed separately.
The qualitative, semistructured portion of the interviews took between 30 and 60 minutes to complete and was conducted after the survey portion of the interview was complete. Interviews were audio recorded and professionally transcribed. Classic content analysis was used to systematically code transcribed data, allowing the identification of key themes (Boyatzis, 1998). Three research assistants, a doctoral student, and two full-time faculty members performed this work. The first author and the doctoral student independently coded approximately half of the baseline transcripts before reviewing them together. Overlapping or agreed-on coded material was entered into a case summary data matrix, which then served as a template to code the remaining baseline and follow-up transcripts. Categories in the template included topics such as positive change with housing, negative change with housing, relationship with family, and housing’s impact on relationships. Longitudinal qualitative comparisons were facilitated by organizing the matrix by precoded and postcoded material, and emergent themes were consensually validated (Padgett, 2012).
Results
Quantitative Findings
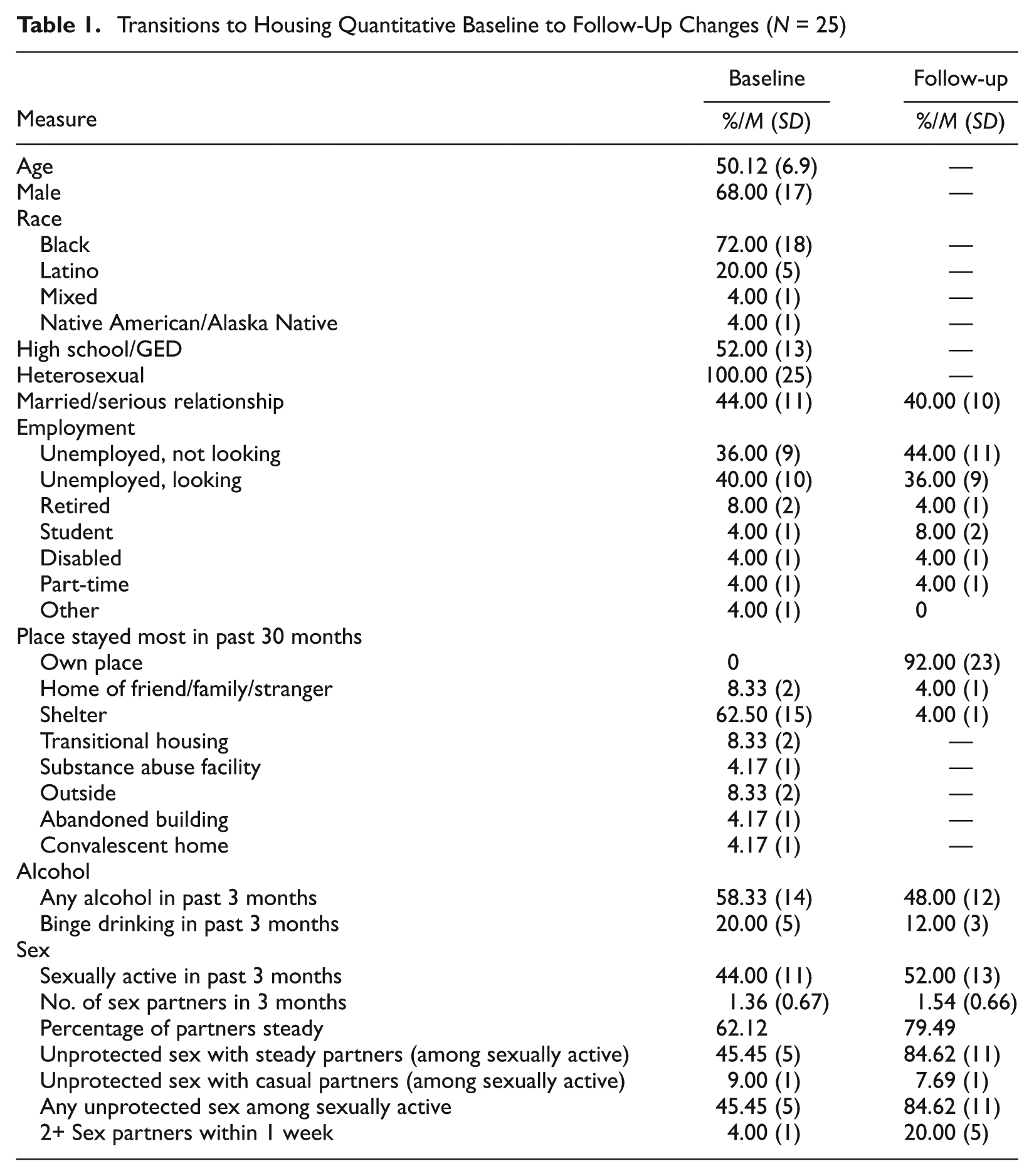
As shown in Table 1, of the 25 respondents who completed both baseline and follow-up interviews, 68.0% were men and 72.0% were African American. Their mean age was 50 years (SD = 6.9). Only 52% had completed high school or more education, and all participants reported their sexual identity as heterosexual. Employment rates and the percentage of people who reported that they were currently in a serious relationship or married were relatively stable from baseline to follow-up. All participants in this study received single-occupancy units, but a surprisingly high number of respondents reported that they were married or in a serious relationship at baseline (44.0%). Despite this high rate, the vast majority of respondents reported that their serious partner was stably housed separately from themselves (90.1%), and no respondents reported living with their serious romantic partner at either baseline or follow-up. At baseline, most respondents (62.5%) reported a shelter as their most common living arrangement during the previous 3 months, more than 12% reported sleeping outside or in an abandoned building most of the time, and 8.3% reported they had mostly stayed in a transitional living program. At follow-up, the vast majority (92.0%) reported their most common place of stay during the prior 3 months as their single-occupancy unit; one respondent reported staying mostly in a shelter and another stayed in the home of a friend or family member.
Transitions to Housing Quantitative Baseline to Follow-Up Changes (N = 25)
Network size decreased between baseline and follow-up for 50.0% of respondents, increased for 37.5%, and stayed the same for 12.5%; overall mean number of network alters decreased from 12.7 (SD = 6.7) at baseline to 11.0 (SD = 5.3) at follow-up. Respondents reported several other changes in the composition of their social networks between baseline and follow-up Table 2; these results are presented in Table 2. Slightly less than 50% of respondents reported increases in the proportion of their networks composed of family members. The majority of respondents also reported decreases in the proportion of housing (62.5%) and nonhousing (50.0%) service providers in their networks. Most respondents reported changes in the proportion of network alters with whom they communicated in person, by phone, and in writing, but these changes were mixed. For example, 50.0% of respondents reported more alters whom they saw in person at follow-up, whereas 45.8% reported a decrease in this type of alter.
Transitions to Housing Quantitative Social Network Interview Baseline to Follow-Up Changes (N = 25).
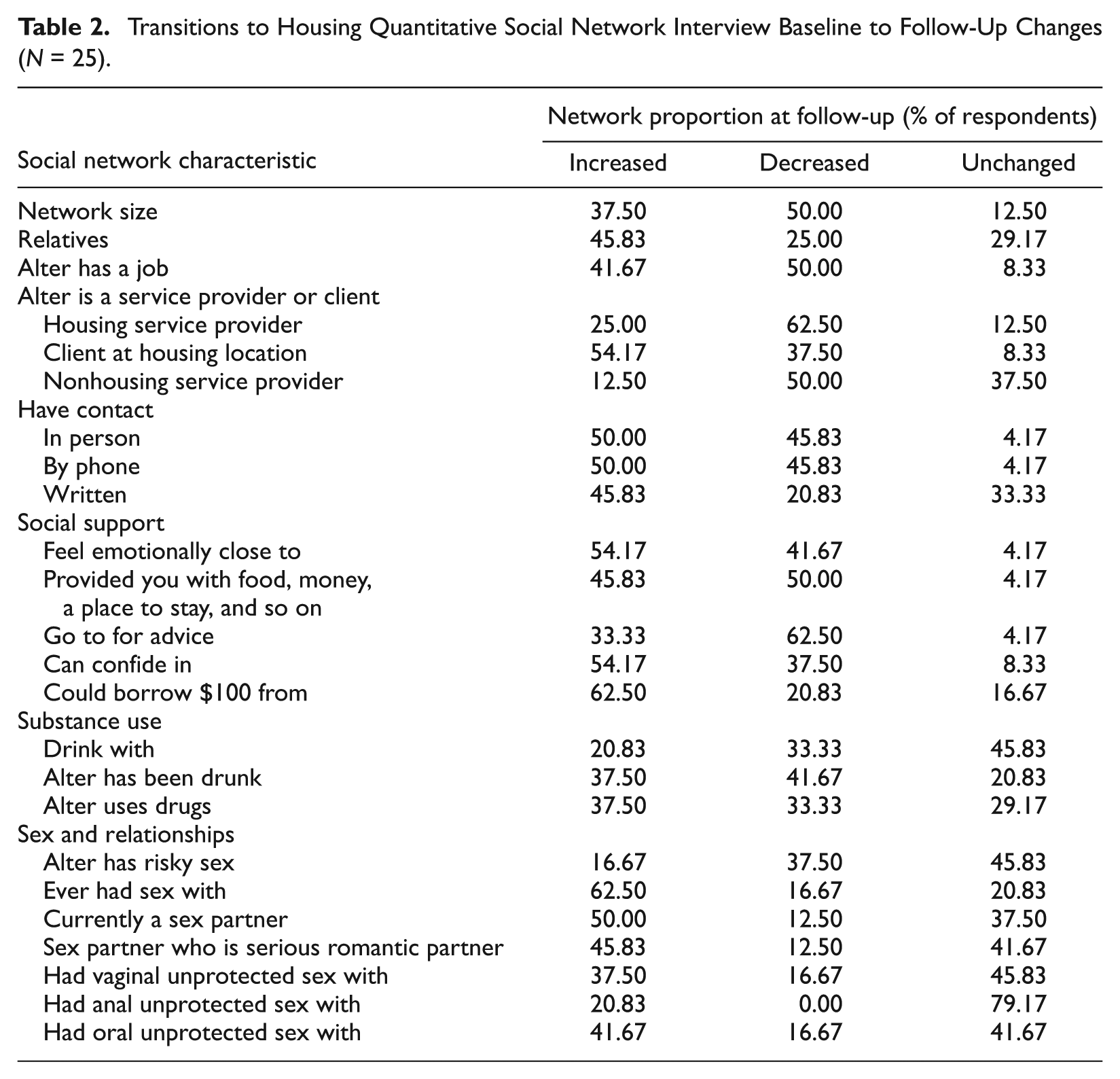
Some aspects of social support, as reflected in social network composition, also appeared to change between baseline and follow-up. Sixty-three percent of respondents reported a decrease in the proportion of alters whom they could go to for advice; yet mixed changes were reported in the proportion of alters that respondent felt emotionally close to, alters they could confide in, and those who provided tangible support (defined as food, money, clothes, or a place to stay). Although respondents varied in whether they had received tangible support from network alters, most respondents (62.5%) reported an increase in the proportion of people from whom they believed they could borrow $100 if they really needed it.
Substance use risk behavior among alters also changed after participants moved into housing, but in both directions. The proportion of network alters who used drugs increased between baseline and follow-up for 37.5% and decreased for 33.3% of participants; similarly, the proportion of alters who had been intoxicated increased for 37.5% and decreased for 41.7% of respondents.
Respondents reported more sexual activity with network alters at follow-up. Sixty-three percent of respondents reported an increase in the proportion of lifetime sex partners in their network and 50.0% reported an increase in the proportion of current sex partners. Only 16.7% and 12.5%, respectively, reported decreases in these types of alters. The proportion of alters who were both sex partners and serious romantic partners likewise increased for 45.8% of respondents. Nonsocial network quantitative data also revealed increases in overall sexual risk behavior, as shown in Table 1, with sexual activity increasing from 44.0% at baseline to 52.0% at follow-up and unprotected intercourse increasing from 45.5% to 84.6% among sexually active respondents. The average number of sex partners among participants who were sexually active increased slightly, from 1.36 to 1.54, and the percentage of those sex partners defined by participants as steady (rather than casual or one-time partners) increased from 62.1% to 79.5%. Unprotected sex with steady partners nearly doubled from 45.5% to 84.6% (mirroring the increase in overall unprotected sex). Despite the increase in unprotected sex occurring primarily with steady partners, the rate of concurrent sex (having two or more sex partners in a single week) also increased between baseline and follow-up from 4.0% to 20.0%.
Qualitative Findings
Qualitative analysis revealed two main themes related to changes in social relationships: giving to those who are less fortunate and distancing oneself from negative influences.
Giving to Those Who are Less Fortunate
Participants expressed being in a newfound position of privilege after receiving housing. Many reported using that position to help others or volunteer at agencies that assist individuals in need. Examples include a woman who visited people in a nursing home, a man who worked with ministries that feed and clothe people experiencing homelessness and visited convalescent homes, and a man who mentored individuals new to sobriety. One man who spoke of wanting to join AmeriCorps stated, “Trying to do that as well and being of service and have a helping personality. Now that’s therapy for me.” In addition to wanting to give back, participants said helping others also provided structure and filled up free time. One woman chose to maintain ties with the organization that stored her belongings when she was homeless, stating:
Thursdays I go down and do some community service where I used to keep my clothes at. I go down there and clean their building for them once a week, clean the bathroom and mostly bathroom and sweep out the place, what have you. That gives me something to do.
Having a place to call home was also something participants wanted their former peers to experience. As one woman explained:
I find it disgusting that when I walk by the front desk of our housing I can clearly see there’s 12 empty units there, consistently, the same one for I don’t know how long. I tried to get services for a lady across the street who happens to be possibly a little bit older than myself . . . and I came to find out that she’s mute. She can’t speak. If something were to happen to her she couldn’t shout for help. You know what I mean? And every day we walk by her. Every day the staff walks by her. The housing inspectors, HUD [individuals from the U.S. Department of Housing and Urban Development]. My goodness. There has to be a better pipeline of services for special needs people like that.
Two participants offered to let homeless people stay with them. One woman explained:
I think this week I brought two girls . . . so they can, you know, get off the street and take a shower and wash their clothes, relax, eat, watch TV and just get off the streets for a while, so every now and then—like, yesterday I brought [Woman 1] and the other day I brought [Woman 2], but just so they can have a little solitude, you know, just get off the street. They’re just really tired. You just get tired, so I guess I’m, like, looking at myself saying well, you know, that could be me again. Just struggling out there, but it’s not, so I just kind of like—I appreciate everything that I’ve got right now.
Participants said their desire to give back came from their newfound status of being formerly homeless while simultaneously maintaining contact with individuals who remain homeless.
Distancing Oneself From Negative Influences
Recovery from substance abuse was identified as an important goal among individuals who transitioned into PSH, which resulted in reevaluating many of their existing relationships. As one man noted:
All my drug addict friends, alcoholic friends. I see them when I see them. I don’t go on my own and I don’t hang around them no more. . . . Because all, in the past, all they know is drinking and drugging.
Another participant spoke of purposely separating himself from negative influences:
And I tried to separate myself from those relationships now instead of having major riff on me in that circle, you know? I’m deleting all phone numbers that don’t benefit or contribute to my welfare and benefit, and I’m deleting all friendships that can’t help me positively. If they’re negative, they have to go.
Eighteen of the 25 participants interviewed at follow-up spoke of participating in substance abuse services, most commonly Alcoholics Anonymous and Narcotics Anonymous, in which participants surrounded themselves with others who could assist them in their sobriety. One participant spoke about how this resulted in a clear divide with former network members:
The people I used to use with . . . I don’t deal with people that—because their lifestyle don’t coordinate around that. . . . I don’t kick it on the corners like I used to do. And I don’t talk the same language they talk.
Although the overall emphasis was on disconnecting with old relationships, most participants indicated attempts to develop new relationships.
Discussion
As depicted in Table 3, this study’s mixed methods approach yielded several confirmatory findings that can be categorized as convergent (answers are validated by each method), complementary (related questions are answered by each method), or expansive (one method answers questions raised by the other; Palinkas, Holloway, et al. 2011). The quantitative findings from this pilot study suggest that social network size and composition change as individuals transition from homelessness to single-site PSH, yet not in a consistent manner. Half of the study participants experienced a contraction in the size of their social networks, whereas slightly more than a third expanded their social networks. The qualitative findings contextualize these changes (i.e., convergence) and indicate that participants were engaged in an active process that involved attempting to put distance between network members viewed to be negative influences and engaging in new relationships (i.e., complementarity). These new relationships were described as important to sustaining recovery from substance abuse and as occurring during attempts to help peers who had similar life struggles and who were less fortunate.
Results of Convergent Parallel Design.
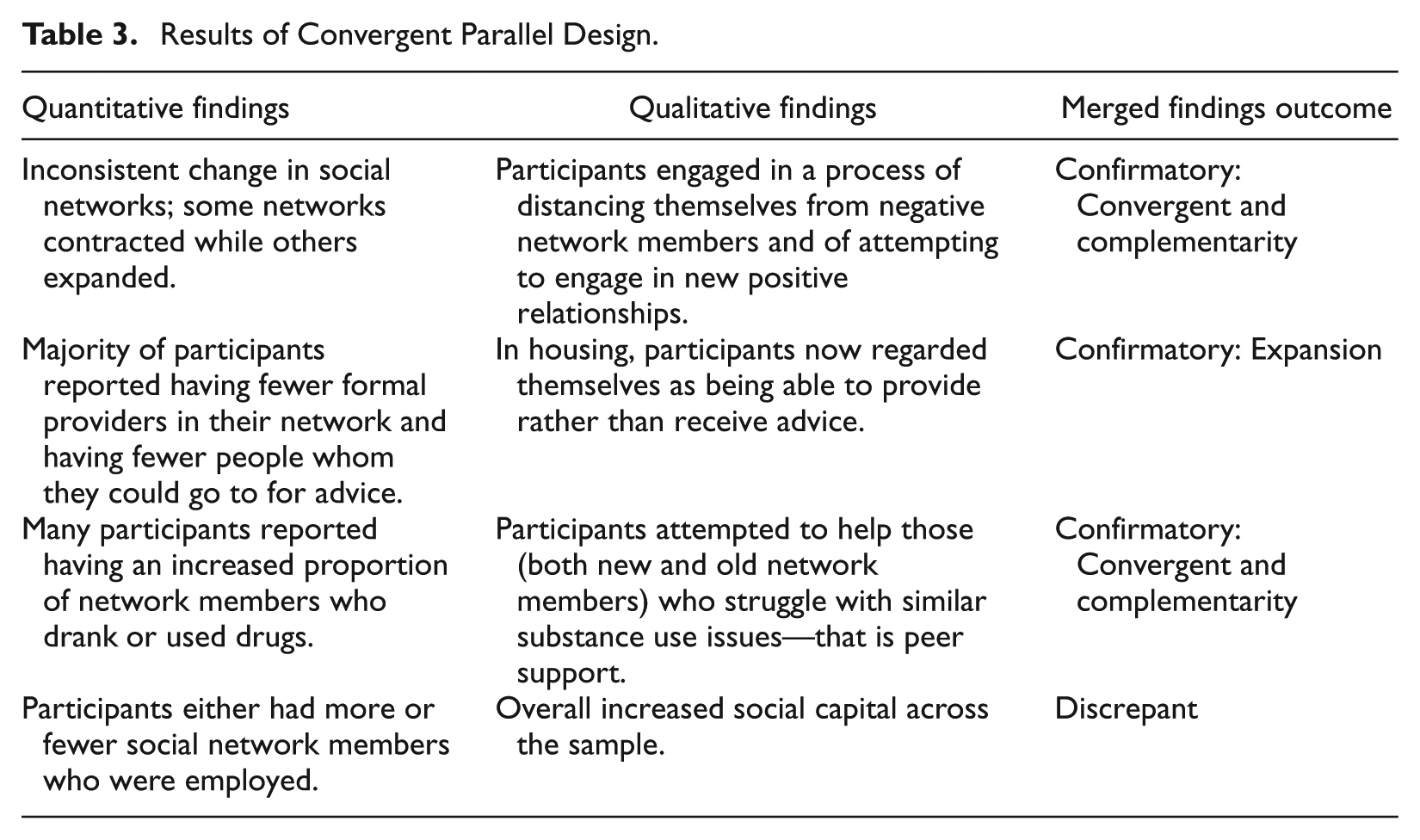
The processes responsible for changes in network size also accounted for changes in network composition. The qualitative finding that participants regarded themselves as being able to help others may also account for why the majority of participants reported having fewer people whom they could go to for advice; that is, participants now regarded themselves as being able to provide rather than receive advice (i.e., expansion). This is also reflected in the majority of participants who reported having fewer formal providers in their network. Interestingly, a possible discrepant finding was that the majority of participants also indicated that they had increased social capital, reflected both in the qualitative findings and reports at follow-up that they had more people from whom they could borrow $100 even though participants were almost evenly split between having more and fewer social network members who were employed.
Despite changes in the size and composition of social networks, there was limited change in the number of participants who used alcohol; half of the participants reported no change in the number of alters with whom they consumed alcohol. In fact, more than a third of participants reported having an increased proportion of network members who drank or used drugs. As suggested by the qualitative findings (i.e., convergent and complementarity), this may be due to maintaining relationships with existing network members in an effort to help them or establishing relationships with new network members who struggle with similar substance use issues for purposes of peer support. This mixed methods approach yielded social network findings that were both complementary and expansive (Palinkas, Horwitz, Chamberlain, Hurlburt, & Landsverk, 2011), suggesting tension between moving forward after receiving housing and leaving behind the past that involved homelessness.
The quantitative findings that sexual activity and HIV risk behaviors increase as individuals who are experiencing chronic homelessness transition into PSH are concerning and require further investigation. Although such findings are not entirely unexpected given existing high rates of HIV risk behaviors (Brown et al., 2013; Tucker et al., 2013; Wenzel et al., 2007) and that homelessness is often viewed as a barrier to having intimate relationships (Bourgois, 1998; Brown et al., 2013), how to intervene is less clear given the complicated and dynamic changes in social networks indicated by these mixed methods findings. It may be that increased provider involvement that addresses such risk factors is needed rather than what appears to be a contraction of providers in participants’ social networks. Findings may also suggest that a contraction in social networks does not necessarily indicate that tenants are isolated, but instead are choosing increased intimacy (Padgett et al., 2008; Yanos et al., 2004). Recent critiques that PSH serves as a mechanism of social control by keeping people isolated and fails to promote social recovery (Hopper, 2012) may be inadvertently underemphasizing the larger risk environment in which PSH tenants are embedded. Because this pilot study suggests HIV risk may increase once individuals are housed, greater attention needs to be paid to how PSH constitutes a risk environment (Latkin et al., 2013).
Strengths and Limitations
To our knowledge, this pilot study was the first to consider changes in social networks and HIV risk as individuals transition from homelessness to PSH, and it benefited from a mixed methods approach. Social network studies are typically either quantitative or ethnographic in nature; mixed methods are infrequently used to investigate network phenomena. Indeed, new methods for rigorously collecting mixed methods data on social network processes are a topic of recent investigation (Palinkas, Holloway, et al., 2011; Rice et al., 2014). Given the small sample of 25 people who were interviewed prior to moving into housing and 3 months after transitioning to PSH, the results of this study are not generalizable to the larger population of homeless adults accessing housing. The small sample size also limited our ability to interpret the degree to which certain percentage changes are significant and meaningful. In addition, to protect the confidentiality of our respondents and their social networks, the institutional review board asked that we not collect any identifying information about social network alters. As such, it was not possible for us to assess network stability between baseline and follow-up. We also did not ask about illicit drug use due to not having a certificate of confidentiality. This is an important risk factor for HIV that was not considered. Finally, this study focused on a sample of individuals entering single-site PSH, and it is unclear whether there would be differences between single- and scatter-site PSH.
Nevertheless, these findings are informative and the study’s use of mixed methods can be expanded to conduct a larger, more focused inquiry. In addition to improving the representativeness and size of the sample, future research could include a more strategic use of mixed methods such as a specific focus on intimacy within the qualitative inquiry or better linking the qualitative inquiry to quantitative responses. Although we observed changes in social relationships, other changes may occur over longer periods of time and thus a longer follow-up period is warranted (Pickett-Schenk, Cook, Grey, & Butler, 2007). Future research proposed by the authors will expand the size, scope, and methods of this study so that we can better understand the relationship between changes in social networks and HIV risk as people transition from homelessness to different types of PSH.
Conclusion
PSH is effective at ending homelessness even for people who have experienced long-term homelessness. Despite its obvious benefits, transitioning to PSH represents a major life event that involves significant stress and change. This study suggests that significant changes occur in an individual’s social network during the transition to PSH, a process that is complicated by a desire to move forward in personal recovery, yet remain tied to the recent past of homelessness. This study also suggests that the transition to PSH can introduce new risks or intensify existing risk profiles, including HIV risk behaviors. Future research should examine the mechanisms and extent of risk behavior that may be introduced as individuals move into PSH, consider whether there are differences between single- and scatter-site PSH, and use these findings to guide appropriate intervention efforts.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.