
Abstract
A challenge for mixed methods researchers concerns integration in the methodological dimension. Employing a fully longitudinal mixed methods case study design, we examined the physical and psychological changes in a chronically ill older person via telenursing video consultations. We collected daily measures of his physical state and conducted clinical interviews before and during the COVID-19 pandemic. Our two-step approach integrated mixed data types, first, by making meta-inferences at five time frames during his illness trajectory and, second, by developing “global meta-inferences,” or interpretations across the meta-inferences from each of the five time frames using joint display analysis. We contribute to the mixed methods literature by illustrating integration in the methodological dimension through a fully longitudinal mixed methods case study.
Keywords
An arena of developing interest for mixed methods researchers concerns advancing procedures for intersecting (Plano Clark & Ivankova, 2016) or scaffolding together (Fetters, 2020) two methodologies in a program of research for integration in the methodological dimension (Fetters & Molina-Azorin, 2017; Greene, 2015). Relevant examples include mixed methods grounded theory (Creamer, 2018; Guetterman et al., 2019; Howell Smith et al., 2020; Johnson et al., 2010; Walsh, 2015) and mixed methods case study (Guetterman & Fetters, 2018; Plano Clark & Ivankova, 2016). A gap in the literature has been the intersection of longitudinal mixed methods with a mixed methods case study. In the following, we review relevant literature pertinent to mixed methods research for each of these, provide the rationale for integrating the two methodologies, and then illustrate its relevance to nursing research in the COVID-19 era. We further delineate a process for drawing meta-inferences across multiple stages of the longitudinal mixed methods investigation.
Longitudinal and Mixed Methods Research
Although mixed methodologists have advanced understanding of longitudinal mixed methods research designs (e.g., Christ, 2007; Evans et al., 2012; Hauken et al., 2019; Holder, 2018; Neves & Baecker, 2020; Plano Clark et al., 2015; Schumacher et al., 2021; Van Ness et al., 2011; Waller et al., 2021), examples integrating in the methodological dimension with longitudinal mixed methods studies are needed. In this article, we illustrate integration in the methodological dimension in a study utilizing longitudinal research and case study design.
Plano Clark et al. (2015) defined longitudinal research as “a research approach in which the researcher repeatedly collects and analyzes data over time” (p. 299). They reviewed 32 self-identified mixed methods studies using a longitudinal mixed methods design (LMMD) to examine how this design was used and issues that may occur when conducting longitudinal mixed methods research. Based on a literature review, Plano Clark et al. (2015) also identified variations in the design procedures and several considerations when using an LMMD. Among the issues raised by the authors were “data analysis and integration issues” (p. 312). Furthermore, they argued that there was a paucity of studies explicitly reporting data integration. Instead, the reviewed articles rarely integrated the quantitative (QUAN) and qualitative (QUAL) data sets except in the final discussion. Although the number of studies using an LMMD has recently increased (e.g., Hauken et al., 2019; Holder, 2018; Neves & Baecker, 2020; Waller et al., 2021), more empirical studies using an LMMD that concretely demonstrate integration of multiple sets of QUAN and QUAL data obtained over time are needed.
When using an LMMD in biomedical research, there are three distinct types of approaches based on the timing of data collection: prospective, retrospective, and fully longitudinal (Van Ness et al., 2011). Plano Clark et al. (2015) described these approaches as follows: (a) a prospective approach involves the use of QUAL data collected once at the first time point of the QUAN longitudinal strand, to record participants’ expectations regarding the issue to be measured quantitatively; (b) a retrospective approach involves the use of QUAL data collected once at the last time point of the QUAN longitudinal strand, to record participants’ recollections of the issue that was measured quantitatively; and (c) the fully longitudinal approach involves the use of both QUAL and QUAN data collected at all time points (p. 298).
Case Study and Mixed Methods Research
Yin (2018) offers a twofold definition of a case study that incorporates its scope and features. Regarding the scope, Yin defines the methodology as, “an empirical method that investigates a contemporary phenomenon (the ‘case’) in depth and within its real-world context, especially when the boundaries between phenomenon and context may not be clearly evident” (p. 15). Regarding the features of a case study, he emphasizes its characteristics of “an all-encompassing mode of inquiry, with its own logic of design, data collection techniques, and specific approaches to data analysis” (p. 16). Guetterman and Fetters (2018) intersected/scaffolded mixed methods and a case study and identified two distinctive design types: (a) mixed methods–case study design (MM-CS) and (b) case study–mixed methods design (CS-MM). In the MM-CS design, a case study is used for the QUAL component of a mixed methods study, while in the CS-MM design, researchers conduct a case study by collecting both QUAN and QUAL data. The authors discussed the potential of combining case studies and mixed methods to “yield a complete understanding,” so long as they are “conducted systematically and thoughtfully” (p. 901).
Rationale for Integrating Longitudinal and Case Study Methodology in Nursing
In nursing research, the value of using a fully LMMD is recognized as a means to fully understand the dynamic illness trajectory of the participant (Schumacher et al., 2021). The use of a case study provides added value for clarifying day-to-day clinical issues for nurses better than the mean score of a clinical trial (Morse, 2006). A fully LMMD is a suitable methodological approach to collect and analyze complex longitudinal data, such as examining and monitoring individuals with chronic diseases over time.
Although previous evaluation studies of telenursing practice followed peoples’ chronic conditions using a mixed methods design (Dias & Fragoso, 2013; Ernesäter et al., 2016), the authors provided no discussion on how to continuously integrate QUAN and QUAL data from a longitudinal perspective. Creswell (2015) and Fetters et al. (2013) suggested that, to provide a comprehensive picture of the course of a longitudinal study, it is essential to analyze and integrate QUAN and QUAL data and create joint displays in order to draw repetitive meta-inferences.
Given the lack of literature about intersecting longitudinal mixed methods with a mixed methods case study, our purpose is to introduce a fully longitudinal mixed methods case study (FLMM-CS) design. We use our telehealth/telenursing research during the pandemic of SARS-CoV (COVID-19) to illustrate the methodological procedures. We define an FLMM-CS design as collecting and analyzing both QUAN and QUAL data repeatedly over time for a single case. Longitudinal mixed data integration is achieved by drawing meta-inferences at set time periods and by making global meta-inferences that encompass all time periods through data integration. With this design, a researcher is able to describe and interpret the dynamic nature of the case and gain in-depth understanding of the phenomenon under investigation within its real-world context.
In the present study, we used an FLMM-CS design, an intersected/scaffolded design of a fully LMMD (Plano Clark et al., 2015), and a CS-MM design (Guetterman & Fetters, 2018) to obtain a detailed and in-depth understanding of the dynamic illness trajectory of an older adult with severe chronic obstructive pulmonary disease (COPD) for more than 2 years, including during the COVID-19 pandemic. We also provide a concrete example that illustrates ways to integrate QUAN and QUAL data in an FLMM-CS design using a joint display.
The Need for Alternative Care Models for Individuals With Chronic Diseases During the COVID-19 Pandemic
COVID-19, first reported in November 2019, is a rapidly transmitted infection that spreads through direct person-to-person contact (World Health Organization [WHO], 2020b). On March 11, 2020, the WHO declared COVID-19 a global pandemic (WHO, 2020b). The governments of many countries, including Japan, imposed drastic restrictions on people’s mobility to prevent the spread of infection (Prime Minister’s Office of Japan, 2020). These restrictions severely and negatively affected the daily life of people, especially older adults with chronic conditions, and increased the demand for nondirect contact health care services—such as telehealth/telenursing—that could investigate cases longitudinally.
The pandemic (WHO, 2020b, 2021) has highlighted the need to establish a robust remote medical care system, as strict social distancing protocols have hindered people’s access to hospitals or clinics in view of the health risks. WHO’s (2020a) COVID-19 strategy necessitates the development of large-scale public health capacities, with urgency and equity acting as guiding principles, to stop transmission. Moreover, this unprecedented global pandemic has continued for longer than was initially expected. In response to this crisis, the Japanese government deregulated online health services in April 2020 to encourage more widespread telehealth services, in order to provide non-in-person health care (Cabinet Office of Japan, 2020). The Ministry of Health, Labour and Welfare (2015) of Japan recently set a target to improve the quality, value, safety, and performance of health care by 2035 by utilizing information communication technology.
Responding to the increased demand for information communication technology, the first author and her colleagues developed a home-monitoring-based telenursing system (Kamei et al., 2018). This system provides continuous nursing care for individuals with chronic conditions such as COPD, diabetes, amyotrophic lateral sclerosis, heart failure, cancer, and pneumonia. Telenursing is defined as “the use of information communication technologies to provide nursing practice at a distance” (Kumar & Snooks, 2011, p. 1). Telenursing can help monitor individuals’ daily physical and psychological states, perform triage, and provide health consultations so participants can manage their chronic diseases for long periods without disruption. Telenursing can be utilized in various situations to promote health, manage illness, or facilitate consultations (Ota & Maeda, 2020). A telenursing service combined with telemonitoring reduces dependence on physical health care resources, such as emergency department visits, significantly (Kamei et al., 2013). However, telenursing is still not widespread in the Japanese health care context, including in nursing school education (Kamei et al., 2021).
Health care services have predominantly employed a positivistic approach, monitoring individuals’ physical state using numerical data to retain objectivity in clinical judgment. However, as the WHO (1948) defines health as “a state of complete physical, mental, and social well-being and not merely the absence of diseases,” merely monitoring people’s physical state does not suffice for understanding the details of their real lives, especially in home care situations. Therefore, it is also essential to perform monitoring, which focuses on both physical and psychosocial dimensions. The integration of both dimensions facilitates provision of proper nursing care. Moreover, in terms of COVID-19, people with severe COPD are particularly vulnerable to infection. Hence, telemonitoring technology is a promising solution that allows chronically ill persons to maintain their health while avoiding additional risks from in-person visits to medical care centers.
Home-Based Telemonitoring
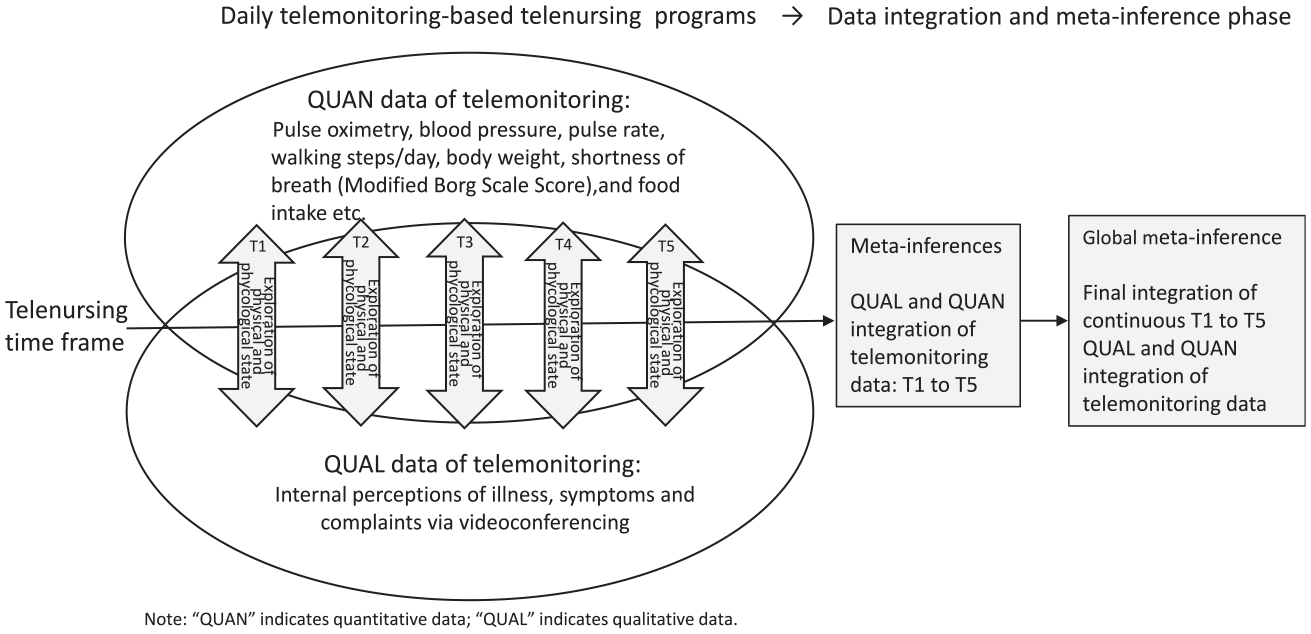
In home-based telemonitoring, a telenurse, that is, a nurse who uses telecommunications and information technology to provide nursing care, monitors the daily QUAN data of participants—such as pulse oximetry, blood pressure, walking steps, body weight, breathlessness scale, and comprehensive state scale—as well as QUAL data—such as internal illness perception, symptoms, and complaints. The telenurse integrates both types of clinical data to provide optimized telenursing. Thus, empirically investigating the dynamic course of changes in an individual’s physical and psychological health states over time through this practice can be rigorously done using a methodological approach like the FLMM-CS design to capture the complexity of the case.
Theory Informing the Study: The Illness Trajectory of Individuals With Chronic Diseases
Corbin and Strauss (1991) developed a chronic illness trajectory framework as a nursing model to improve people’s quality of life. The model provides a framework for addressing the expectations of patients and their families regarding the future course of the illness. It has eight phases: pretrajectory, trajectory onset, crisis, acute, stable, unstable, downward, and dying. A chronic disease encompasses both QUAN changes (e.g., blood pressure and test values) and QUAL changes (e.g., anxiety and perception of illness), creating a long trajectory that spans the remainder of the participant’s life span.
Study Purpose
The research aim of this study was to investigate the impact of home-based telemonitoring for supporting essentially home-bound individuals with severe chronic illness. The methodological purpose of the study was to illustrate through our example of FLMM-CS design (a) the integration of daily physical and psychological telenursing data and a participant’s perception of illness and (b) how this integration is achieved via a two-step approach for developing not only meta-inferences at each time point but also global meta-inferences encompassing all periods, through the continuous comparison of QUAN and QUAL data. This approach expands ways to conceptualize analysis of longitudinally collected mixed methods data and to develop an integrated assessment strategy in an FLMM-CS, such as long-term telenursing implementations.
Method
Design
We employed the FLMM-CS design to investigate the potential benefits of the home-based telemonitoring approach. This study continuously assessed dynamic changes in a person’s physical and psychological states by collecting daily data on various monitoring parameters, such as blood pressure, walking steps/day, and breathlessness (QUAN), and participant’s clinical interviews during video consultations with nurses (QUAL) for more than 24 months (including during the COVID-19 pandemic period).
Ethical Considerations
We explained the purpose and methods of the study to the participant. He was informed that anonymity and confidentiality would be maintained and that he could withdraw from the study at any time during data collection without penalty. A signed consent form was obtained from the participant before participation. The ethics committee of our institution approved this study.
Conceptual Framework
The conceptual framework illustrating the investigation is shown in Figure 1. The time frame indicates the participant’s trajectory of receiving daily telemonitoring and telenursing. The trajectory was divided into five time frames, ranging from Time (T) 1 to T5. T1 was when the participant was introduced to home monitoring with oxygen therapy; T2 began with the participant’s discharge from the hospital after recovering from exacerbation of heart failure; T3 refers to the 6-month period after T2, when the participant received telenursing; T4 was the pre-telerehabilitation period and coincided with the outbreak of the COVID-19 pandemic; and T5 was the telerehabilitation phase, which was concurrent with the COVID-19 pandemic.
Conceptual framework of the fully longitudinal mixed methods telenursing study.
The Case
The participant, Mr. Ando (a pseudonym), was a 65-year-old man with COPD Stage IV (very severe; Global Initiative for Chronic Obstructive Lung Disease, 2020), who was receiving round-the-clock home oxygen therapy. He has a comorbidity of heart failure Classification II (i.e., heart failure symptoms with moderate exertion, such as ambulating two blocks or two flights of stairs; American Heart Association, 2017). Mr. Ando lived in Tokyo with his daughter. He visited a physician once a month under the Japanese health insurance system. The physician suggested the implantation of a pacemaker and defibrillation to treat arrhythmia. However, Mr. Ando refused them as he neither wanted to be a burden on his daughter nor prolong his life with the help of “machines.” He believed that his daughter would never get married if he was around since no one would want to marry a person with a sick parent requiring constant medical care.
Data Collection
QUAN Data Collection
We provided a daily monitoring–based telenursing service for 730 days to Mr. Ando, a man afflicted with a severe lung disease called COPD. QUAN data collected through daily monitoring included oxygen saturation, blood pressure, pulse rate, step counts/day, body weight and body mass index (BMI), shortness of breath (modified Borg Scale score: 0, not at all; 10, extreme breathlessness; Borg, 1982), mobility, food intake, sleeping status, excretion (0, not at all; 3, as usual), other symptoms including depressed feelings (0, no; 1, yes), physical pain (Wong-Baker FACES® pain scale: 0, does not hurt; 10, hurts terribly), and a 10-point visual analog scale (0, worse; 10, best). Full details have been provided in a previous article (Kamei et al., 2018).
QUAL Data Collection
QUAL data were obtained from the nurses’ telenursing records. During these clinical interviews, telenurses asked the participant about his overall status, breathing, activity, vitality, perception of illness, management of telenursing equipment, and daily life via telephone consultation or telenursing video consultation systems (Table 1). The telenurses recorded the participant’s details from his clinical interviews in their notes. These telephone and video consultations were initiated as per the telenursing protocols (St. Luke’s International University Telenursing SlG, 2018), based on the participant’s condition. After his discharge from the hospital, the assigned telenurses instructed the participant on how to manage the telenursing equipment in his daily life. Whenever the values of any parameters exceeded the predetermined thresholds set by his physician, the nursing monitoring center invited the participant to join a telephone or video consultation. The daily telenursing activities were digitally recorded and transcribed. The original Japanese recordings were qualitatively analyzed to maintain the Japanese context. Thereafter, the themes, categories, subcategories, and quotes were translated into English and edited by a professional English editor. The editing did not alter the intent of the original message. We back-translated the text into Japanese and confirmed “meaning-for-meaning equivalence” of the translation (Schrauf, 2016, p. 100).
Qualitative Data Collection.

Data Analysis
The QUAN data were analyzed using descriptive statistics and the physical state trend, using the Japanese version of the IBM SPSS statistical software Version 24 (IBM Corp., 2016). The QUAL data (interviews and telenursing records) were read thoroughly to obtain a sense of the participant’s trajectory and answer the research question. The QUAL data were analyzed by employing QUAL thematic analysis (Braun & Clarke, 2006) using NVivo 12 (QSR International, 2020). Both analyses mainly focused on breathing; steps, an indicator of activity; and BMI as a measure of vitality.
Mixed Methods Data Integration
We examined the participant's illness and life trajectory by mainly describing the parameters of shortness of breath, daily activity, vitality, and other internal perceptions of illness. The clinical interviews were linked by matching these four significant parameters and integrating QUAL and QUAN data to draw meta-inferences over time. According to Teddlie and Tashakkori (2009), “a meta-inference is a conclusion generated through an integration of the inferences that have been obtained from the results of the QUAL and QUAN strands of an MM study” (p. 152).
During the analysis phase, each author brought cross-disciplinary insights to the discussion (Neves & Baecker, 2020). The first author, T.K., brought her expertise in telenursing and geriatric nursing. The second author, A.K., contributed her insights from engaging in dialogue with Mr. Ando as his telenurse. The third author, N.N., added biomedical viewpoints to the analysis; the fourth author, H.K., brought her expertise in cross-cultural health communication. Furthermore, H.K. framed the data in the cultural and social context to improve the validity of the analysis and interpretation.
The Two-Step Approach for Drawing Meta-Inferences in the FLMM-CS Data
The two-step approach of the present study for developing global meta-inferences in an FLMM-CS design consists of the following procedures. Step 1 involved (a) identifying meaningful data to collect in both the QUAL and QUAN strands that included the physical (i.e., shortness of breath, steps/day, and vitality) and psychological (i.e., perceptions about health, illness, and daily living; experiences with telenursing) information in this case study; (b) determining a conceptual unity in the time frame to integrate QUAL and QUAN data repeatedly over time, as illustrated through the creation of clinically significant windows of the participant’s trajectory; and (c) integrating the QUAL and QUAN data collected during each time frame and drawing meta-inferences by using joint displays, as discussed by Guetterman et al. (2015) . Step 2 involved (a) comparing and contrasting meta-inferences from each of the different time frames to comprehend the changes occurring over time, which were determined by clinically meaningful periods in the participant’s illness trajectory, and finally (b) developing global meta-inferences by integrating the inferences across all time frames (i.e., T1-T5). For integrating the two types of data, we created a joint display to “organize, recognize, and represent mixed methods findings” (Fetters, 2020, p. 199). Figure 2 illustrates the data collection and integration process.

Procedural diagram of the fully longitudinal mixed case study design of the telenursing study.
Results
Progress and Clinical Course of Daily Monitoring From the QUAN Strand
Mr. Ando began receiving home-monitoring-based telenursing daily in November 2018. During the course of this study, the intervention included data from before and during the COVID-19 pandemic. We provided Mr. Ando with monitoring and triage services for 730 days, offered a total of 83 telephone/video consultations, and conducted five interviews during his outpatient visits.
Pre-COVID-19
Figure 3 illustrates the QUAN data from daily monitoring of the key clinical parameters and illustrates Mr. Ando’s illness trajectory based on shortness of breath (modified Borg Scale score), walking steps (activity), and BMI (vitality). At T1, when he was first introduced to telenursing, Mr. Ando had severe limitations in his physical activity due to shortness of breath. One month later, Mr. Ando’s physician detected an exacerbation of heart failure, which required hospitalization. Mr. Ando was hospitalized and received treatment for 1 month. After discharge, his physical and psychological states improved, changes in home rehabilitation motivation were observed (T2), and he subsequently regained vitality (T3).
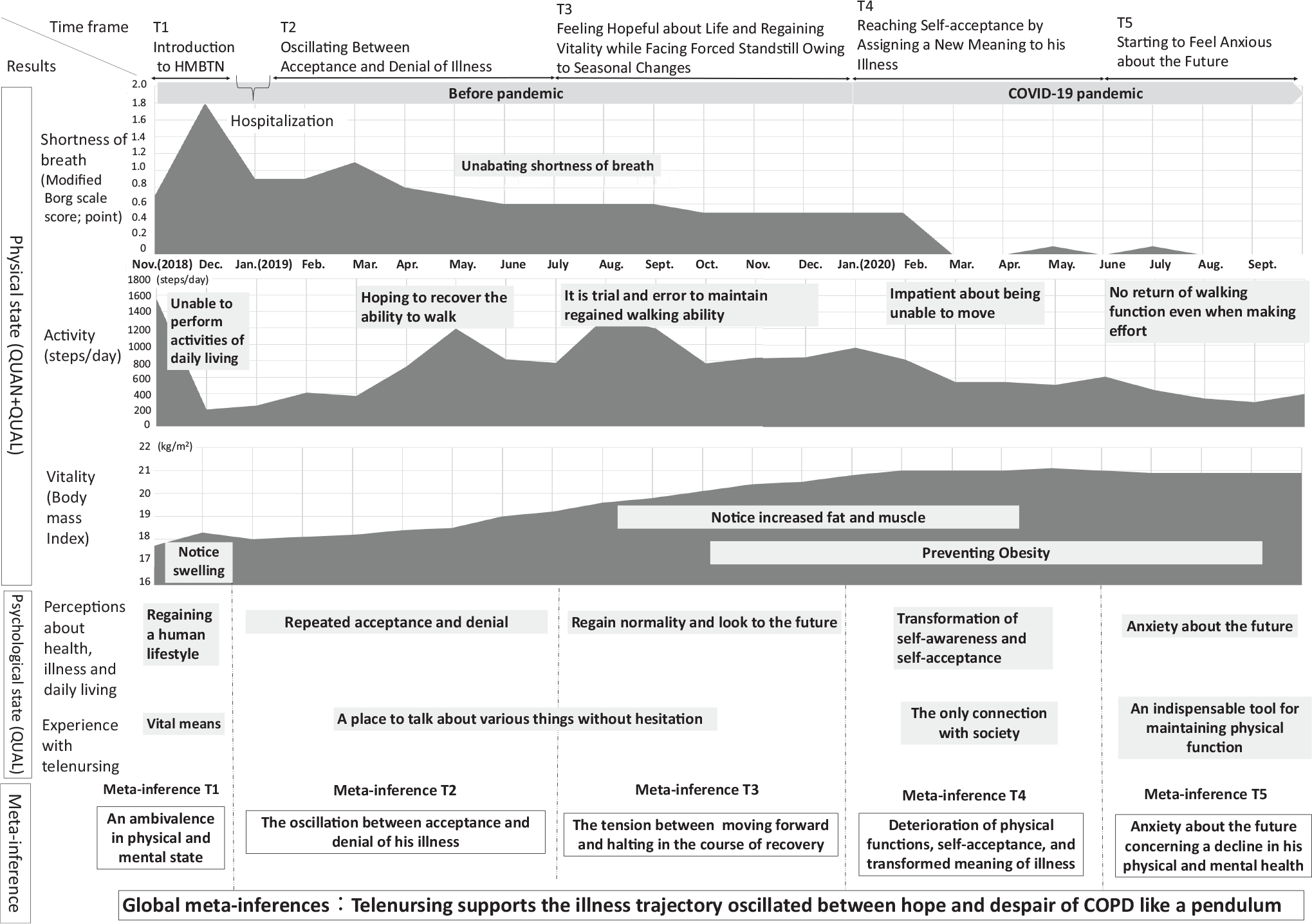
Fully longitudinal mixed methods case study results of physical and psychological changes in an older adult with chronic obstructive pulmonary disease through telenursing.
The Onset of the COVID-19 Pandemic
In the middle of January 2020, 12 months after Mr. Ando began telenursing, the first COVID-19 case was reported in Japan. On April 7, 2020, the Japanese government declared a state of emergency owing to the increased incidence of COVID-19 (Prime Minister’s Office of Japan, 2020). The Tokyo Metropolitan Governor announced a state of emergency until May 25, 2020 (Tokyo Metropolitan Government Disaster Prevention Information, 2020). The fear of contracting a COVID-19 infection hindered Mr. Ando’s external activities, reducing his number of steps to an average of 548 steps/day. Meanwhile, Mr. Ando was experiencing an improvement in his shortness of breath symptoms (T4). However, Mr. Ando’s walking function progressively deteriorated, and he started to experience gradual, albeit slight, worsening of breathing (T5). In sum, from T2 to T5, Mr. Ando’s shortness of breath showed gradual improvement.
Changes in Mr. Ando’s Perceptions Regarding His Illness From the QUAL Strand
The T1 initial meeting between the telenurse and Mr. Ando via the video conference system revealed changes in Mr. Ando’s perceptions regarding his illness. Before being introduced to telenursing, Mr. Ando could not walk at all because of extreme shortness of breath. He was receiving home oxygen therapy; however, he felt disappointed with the therapy because his breathing did not improve. He said, “The home oxygen therapy was different from what I had imagined. I expected it to improve my breathing, but it did not at all.” Mr. Ando could not move or walk even a couple of steps because of severe shortness of breath, but he had no one to consult before starting telenursing.
After the introduction of telenursing during the T2 and T3 phases following his discharge from the hospital, Mr. Ando’s vitality improved. He was able to maintain a stable condition with the support of the telenursing services. During this period, his attending physician noted that Mr. Ando had regained his muscle tone. This resulted in an improvement in his BMI to within the normal range. He recognized that telenursing was instrumental in improving his daily life. He said, “I was living upside down. Now, my life at home has been completely improved.”
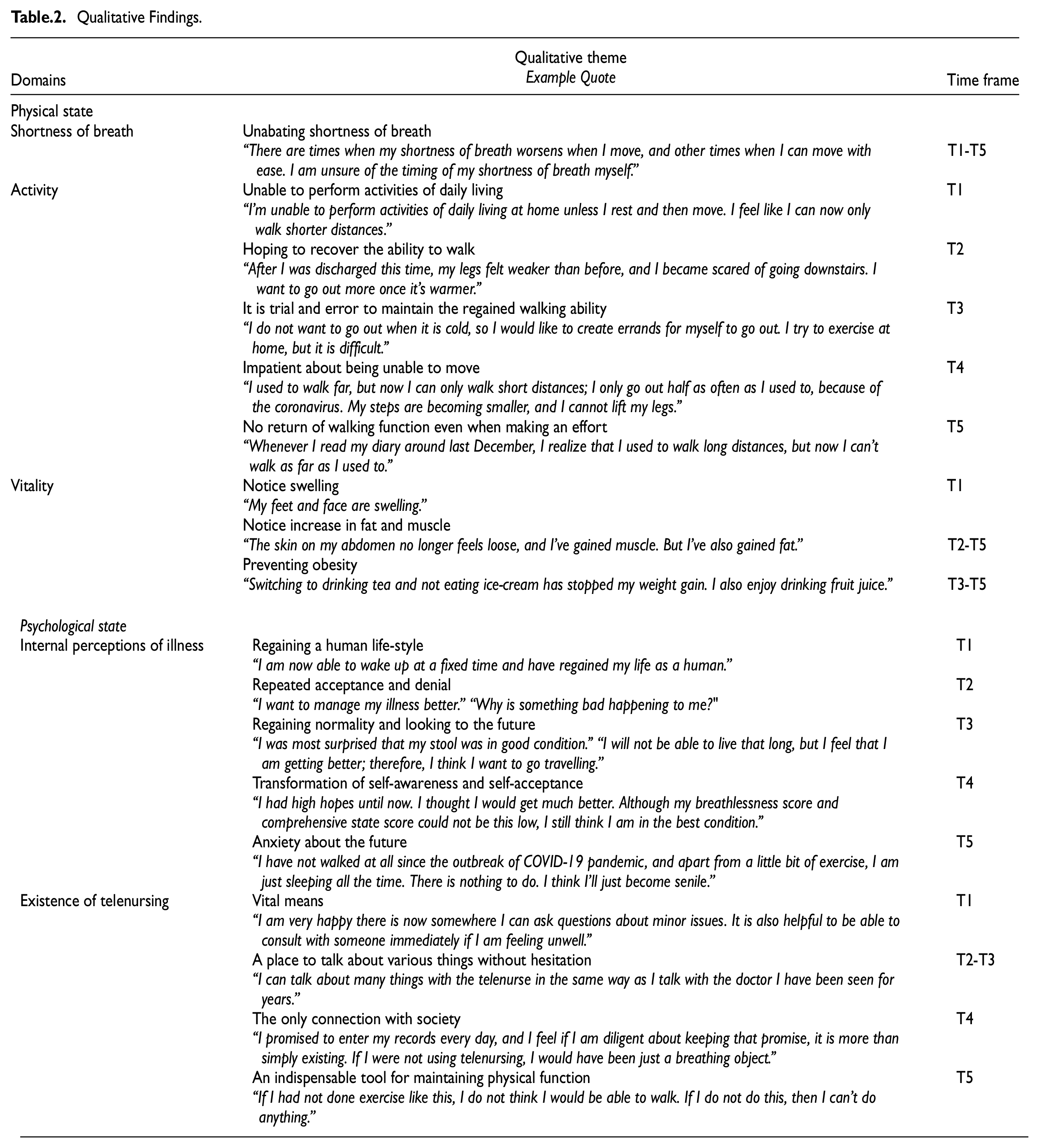
The telenurse was concerned about Mr. Ando’s weight gain, and she suspected progression swelling from fluid accumulation and heart failure. However, his weight gain actually was a sign of improvement in muscle strength. Mr. Ando had become knowledgeable enough to manage his own medication, but he was worried about taking a medicine that increased urination. The telenurse explained to Mr. Ando the necessity of continuing to take the medicine to avoid heart failure. Mr. Ando stopped outdoor walks during T4 (from March to May 2020) because of the high risk of contracting COVID-19. Knowing that physical exercise improves breathing, Mr. Ando asked whether he could perform moderate indoor exercises. In response, the telenurse sent him a physical booklet that illustrated various methods of pulmonary rehabilitation and respiratory exercises of moderate intensity. Unfortunately, Mr. Ando received the booklet only a week later as he did not check his mailbox outside the house for fear of contracting COVID-19 infection (Table 2).
Qualitative Findings.
Data Integration for Each Time Frame
T1: Introduction to Telenursing
T1 covers the first month since the beginning of telenursing (from November 2018 to December 2018). Shortly after Mr. Ando was introduced to telenursing, a telenurse recommended that he be hospitalized for exacerbation of heart failure. His shortness of breath increased to a level 2 out of 10, and the number of steps he walked also decreased despite the excellent season and weather for walking out (QUAN). His BMI increased from 17.7 to 18.3 kg/m2 within only 1 month because of the acute swelling induced by the heart failure (QUAN). During the T1 phase, telenursing became a vital means to maintain Mr. Ando’s daily routine. It facilitated ongoing consultations, which gave him a feeling of comfort. Gradually, Mr. Ando’s exacerbation of heart failure was alleviated following urgent treatment, with the overall satisfactory experience causing Mr. Ando to say, “I am now able to wake up at a fixed time and have regained my life as a human” (QUAL).
Meta-Inferences Drawn From T1
Mr. Ando’s breathing worsened. However, he felt better because of the comfort he was receiving from the telenursing. Furthermore, telenursing’s self-monitoring systems allowed him to follow a routine, making him feel like he was leading a normal life. Thus, T1 represents a period of ambivalence for Mr. Ando because his physical and mental conditions did not converge. In other words, although Mr. Ando’s absolute state of respiratory conditions was weak, his mental state was relatively positive. The support he started to receive from telenursing appeared to have contributed to achieving this positive mental state.
T2: Oscillating Between Acceptance and Denial of His Illness
For 6 months, from January to June 2019 (T2), Mr. Ando was hospitalized for 25 days because of heart failure. Despite improved heart function after receiving treatment, Mr. Ando’s shortness of breath did not fully disappear and remained at a 0.6-1.1 level (out of 10). In the rainy season during this T2 phase, the number of steps Mr. Ando walked per day decreased (QUAN). He had temporary breathlessness, and he noticed that he was getting physically weaker. However, his BMI increased steadily from 18.0 to 19.0 kg/m2 owing to his increasing appetite (QUAN). Giving recognition to telenursing, Mr. Ando stated, “I can talk about many things with the telenurse in the same way as I talk with the doctor I have seen for years” (QUAL). For Mr. Ando, telenursing had become an avenue to talk about health and various other issues without hesitation. After consulting with the telenurse about his physical conditions, including shortness of breath, increased BMI, and worsening vital signs, Mr. Ando began to change his perception toward his illness and started to actively manage and monitor his physical conditions. His willingness to move on with his life grew, and the number of steps he could take per day also steadily increased until it reached an average of 1,193 steps/day (QUAN). These physical changes gave Mr. Ando the confidence that “I can do what I want to do” (QUAL).
Although Mr. Ando expressed some positive feelings about his current situation, he also revealed negative emotions associated with his weakened physical condition compared with others around him. He said, “Every friend around me is still working. Furthermore, it is not that all I do is watch TV; I used to play golf, but whenever my golf buddies invite me over, it is getting more difficult for me to catch up with their conversation since I do not play golf anymore. I have realized that my idea of a normal physical condition is different from that of a healthy person” (QUAL). Mr. Ando’s awareness of being different from other people was increasing. One day, he said, “I want to manage my illness better.” On another day, he said, “Why is something bad happening to me?” (QUAL). Mr. Ando was oscillating between acceptance and denial of his illness. However, his physical functions improved as his activity increased.
Meta-Inferences Drawn From T2
As Mr. Ando’s physical condition and activities gradually improved, he came to accept his state of breathing. Nevertheless, he also experienced difficulty accepting the reality of his being different from his past healthy self and other healthy friends, sending him once again into denial. Thus, T2 represents a period of oscillation between Mr. Ando’s acceptance and denial of his illness.
T3: Feeling Hopeful About Life and Regaining Vitality While Facing Forced Inactivity Owing to Seasonal Changes
For 6 months, from July to December 2019 (T3), Mr. Ando’s shortness of breath improved by 0.4-0.6 points out of 10 (i.e., reduced shortness of breath; QUAN). Nevertheless, his temporary breathlessness continued. In this situation, Mr. Ando took responsibility for managing and monitoring his physical conditions, which might have prevented recurrence of heart failure and COPD. Additionally, he felt that he was leading a normal life for the first time in a long while and said, “I was most surprised that my stool was in good condition. I wore a diaper for several years because I have diarrhea five to six times a day, and I could not even walk to the nearby bathroom because of breathlessness. However, my condition has been gradually improving after being discharged from the hospital the last time and after starting telenursing, and I can maintain this condition without taking medication” (QUAL). Mr. Ando expressed satisfaction with the telenursing support that he was receiving.
Around this time, he began to express hope for his future, saying, “I will not be able to live that long, but I feel that I am getting better; therefore, I think I want to go traveling” (QUAL). After the rainy season was over, the number of steps that he could walk increased, reaching an average of 1,335 steps/day. Simultaneously, Mr. Ando made an effort to maintain his physical condition by walking regularly (QUAN). In the winter, although the low temperature prevented Mr. Ando from going outside, he was enthusiastic about exercising indoors to maintain his physical functions. During this time, Mr. Ando’s BMI increased from 19.2 to 20.5 kg/m2 (QUAN), and he was concerned about obesity. However, he felt confident in his physical strength owing to his regular walking (QUAL).
The season had changed, and so had Mr. Ando’s situation. By November, the cold temperature limited his physical activity, and the average number of steps per day decreased to 836, while his shortness of breathing remained almost unchanged (QUAN). He said, “I do not want to go out when it is cold, so I want to create errands for myself to go out. I try to exercise at home, but it is difficult” (QUAL).
Meta-Inferences Drawn From T3
Mr. Ando’s physical state gradually improved, and he began to feel that he was leading a normal life. Mr. Ando finally found hope for the future after going through countless physical and psychological ups and downs. However, despite his high motivation to increase his daily step count, the cold temperature discouraged him from walking. Thus, T3 represents a period of tension between moving forward and halting in the course of recovery.
T4: Reaching Self-Acceptance by Assigning a New Meaning to His Illness
For 5 months, from January to May 2020 (T4), Mr. Ando made an effort to walk regularly to maintain his physical condition, despite the cold temperature. However, the outbreak of the COVID-19 pandemic prevented him from going out to walk. He was afraid to go outside and said, “I try to go out on walks. Nonetheless, I am scared right now because of the coronavirus” (QUAL). After the Japanese government requested people to refrain from going out, Mr. Ando’s number of steps per day dropped steadily to an average of 548 (QUAN). Mr. Ando realized that his ability to walk was gradually deteriorating, and he could not move as he wanted for about 2 months after the outbreak of the pandemic. He said, “I used to walk far, but now I can only walk short distances; I only go out half as often as I used to because of the coronavirus. My steps are becoming smaller, and I cannot lift my legs” (QUAL).
Even though Mr. Ando’s physical activities decreased, his BMI was stable, at an average of 21 kg/m2 (QUAN), because he avoided excessive sugar intake to prevent obesity (QUAL). In this situation, he strove to prevent exacerbation of his illness by being careful about his physical condition. His temporary breathlessness continued to bother him. However, one day in March 2020, his score in the breathlessness self-rated inventory (Borg Scale) suddenly changed from 0.5 to 0, with 0 indicating absence of shortness of breath (QUAN). Mr. Ando’s perceived improvement of his condition might have resulted from his acceptance of his illness after oscillating between acceptance and denial over the previous year. He said, “I had high hopes until now. I thought I would get much better. Although my breathlessness score and comprehensive state score (visual analog scale) could not be this low, I still think I am in the best condition. That is why I decided to give a perfect score and It can be said that I have given up, but I have also come to understand myself” (QUAL). The telenurse asked him whether the COVID-19 pandemic affected him psychologically; he was not sure about it. What he was sure about was the value of telenursing. Mr. Ando stated, “The telenurse is the only connection that I have with society. I promised to enter my records every day, and I feel if I am diligent about keeping that promise, it is more than simply existing. If I were not using telenursing, I would have been just a breathing object.” It seems that for Mr. Ando telenursing had become an avenue to communicate without hesitation and served as a vital connection with others during the COVID-19 pandemic.
Meta-Inferences Drawn From T4
A few weeks after the declaration of the state of emergency, in spite of the significant deterioration in his walking ability, Mr. Ando came to accept his illness and became less concerned about the state of his shortness of breath. The telenurse’s interactions also contributed to the transformation of Mr. Ando’s view of life. Communication with the telenurse reminded Mr. Ando that he was neither alone nor simply a “breathing object.” The interactions with the telenurse helped remind Mr. Ando that he was very much a part of society. Thus, T4 represents a period of self-acceptance and transformation in the meaning Mr. Ando assigned to his illness.
T5: Starting to Feel Anxious About the Future
For 4 months, from June to October 2020 (T5), during the rainy season and the hot summer that followed, Mr. Ando’s average number of steps per day decreased to 348 (QUAN), and his level of low physical activity induced breathlessness. For that reason, the telenurse started providing rehabilitation support to Mr. Ando through a video telephone system (telerehabilitation). Mr. Ando’s lack of activity in T5 also manifested in his high BMI (QUAN). Mr. Ando mentioned that his fear of contracting the COVID-19 infection prevented his movement and he hesitated to visit the bookstore that he had frequented before the pandemic. The pandemic, rainy season, and hot summer all contributed to the decrease in the number of steps. Mr. Ando said, “I cannot even go to the bookstore right now, so I do not have a reason for stepping out. I just walk around, and I go home immediately” (QUAL). Mr. Ando was disappointed at his inability to walk because of COVID-19. The interview data of Mr. Ando imply that the pandemic deprived him of opportunities to improve his physical function through activity as well as his daily pleasure in going to the bookstore. Recollecting the previous year, when he had regained a normal life after a long time, Mr. Ando said, “Whenever I read my diary around last December, I realize that I used to walk long distances, but now I can't walk as far as I used to” (QUAL).
The deterioration in physical function due to the lack of activity made Mr. Ando anxious about his future. Mr. Ando said, I have not walked at all since the outbreak of the COVID-19 pandemic, and apart from a little bit of exercise, I am just sleeping all the time. There is nothing to do. I think I will just become senile (QUAL).
However, his feeling of breathlessness did not appear during this period (QUAN). Mr. Ando started to look into the option of joining a retirement home in the future, but he realized that he did not want to live in such a place. Mr. Ando said, “There are places where energetic people move into, but I do not feel inclined to move into a place like that yet” (QUAL). Although he could not engage in activities as he wanted due to the fear of COVID-19 infection, he continuously made an effort to address his lack of activity through telerehabilitation; thus, his average number of steps per day did not continually decrease (QUAN).
Meta-Inferences Drawn From T5
The COVID-19 pandemic accelerated the deterioration in Mr. Ando’s physical function by depriving him of opportunities to engage in physical activity. The fear of COVID-19 infection prevented Mr. Ando from even going to the bookstore in the neighborhood, which was one of the few pleasures he could still enjoy. Staying at home and sleeping all the time, Mr. Ando began to feel anxious about his future, given the decline in his physical and mental health.
Global Meta-Inferences
After drawing meta-inferences from all time points (T1-T5), we compared and contrasted them and developed global meta-inferences encompassing all five time points. Our global meta-inferences are as follows. Mr. Ando’s illness trajectory was never static. It showed continuous changes in his physical and psychological states over time. Living with breathlessness, Mr. Ando was continuously reminded of his illness’s reality and the activity limitations it imposed on him. One time, he found hope for the future through the experiences of actively controlling and managing his illness, maintaining good health and physical function, and realizing that he could lead a normal life. He was also disappointed by losing opportunities for activity, experienced a decline in bodily functions, and felt anxious about the future. Thus, in his dynamic illness trajectory, Mr. Ando repeatedly oscillated between hope and despair.
There were times when Mr. Ando was reminded of his healthy past. He felt desperate, especially when he compared himself with healthy peers. However, as much as he experienced disappointment with his life and self-rejection because of his illness, he also experienced hope for the future by improving his physical condition and focusing on what he could still manage to do. The transformation in the meaning Mr. Ando assigned to his illness and life promoted his self-acceptance. However, the COVID-19 pandemic posed a setback to his efforts to regain his life as a normal person. The pandemic also accelerated the deterioration in Mr. Ando’s physical function, making him anxious about the future as he envisioned more health problems emerging. Nevertheless, the pandemic allowed Mr. Ando to realize that he was not alone in his illness journey and that help (i.e., a telenurse) was only a screen away.
Discussion
This study elaborates on the novelty of an FLMM-CS design to show a two-step data integration approach to drawing global meta-inferences that encompass interpretation of the mixed data from all longitudinal time frames of a case study. The case study in the present article examined an illness trajectory of a participant by collecting data on daily measures of the participant’s physical state as well as his psychological state through clinical interviews in video consultations with a telenurse over a period of 24 months (before and during the COVID-19 pandemic), using an FLMM-CS design.
The different frequencies of QUAL and QUAN data collection made it difficult for us to pinpoint the appropriate timing for data integration. Therefore, we focused on typical changes in Mr. Ando’s physical and psychological states in his dynamic illness trajectory. We divided the time frame into five different phases, starting from T1 (the period of being introduced to telenursing) and ending with T5 (the period of beginning to feel anxious about the future).
Illness Trajectory
The present study contributes to the chronic illness trajectory literature pioneered by Corbin and Strauss (1991). Mr. Ando experienced multiple ups and downs in his physical and psychological states through different phases of his dynamic illness trajectory: having a low level of physical function while developing positive feelings as a result of telenursing (T1), oscillating between acceptance and denial of his illness (T2), finding hope for his life and regaining vitality but facing forced inactivity owing to seasonal changes (T3), reaching self-acceptance by assigning a transformed meaning to his illness (T4), and beginning to feel anxious about the future (T5). During the process, telenursing had an increased presence and role in Mr. Ando’s life by providing various types of support.
Our analysis of Mr. Ando’s illness trajectory revealed that the experience of living with a chronic disease is a dynamic process with multiple physical and psychological ups and downs. Comparing himself with others who are healthy or even with his past self-triggered episodes of psychological distress. Furthermore, we found that regardless of the absolute state of physical function, the participant could still feel hopeful by viewing his life from a different perspective.
A major challenge of data analysis and integration in an LMMD lies in conceptualizing time (Plano Clark et al., 2015). Since we consider the passage of time (time flow) as a trajectory, the integration of QUAL and QUAN is viewed as a conceptual cohesion (unity) within the framework of time. Therefore, we drew meta-inferences for each of the five time periods and connected them to obtain global meta-inferences encompassing the full course of time. We believe that this approach to deeply understanding the trajectory of a single case is innovative.
Promising Role of Telenursing in Light of the COVID-19 Pandemic
The present study’s results indicate the promising role of telenursing in providing informational, instrumental, and emotional support to individuals with chronic diseases by offering health advice, monitoring the person’s health, and paying attention to their thoughts and feelings. The COVID-19 pandemic highlighted the crucial role of telenursing in the participant’s life. Telenursing will be particularly beneficial for the delivery of individualized quality care, through telemonitoring and interaction over video calls (Balenton & Chiappelli, 2017). Such care allows nurses and clients to interact with each other even at a distance. We also observed that providing an opportunity for the patient to talk through telenursing might promote their well-being (Tsai et al., 2020). Furthermore, during a pandemic situation of the kind global communities are currently experiencing, the value of information technology–based telenursing becomes even more significant as individuals can use this service right from their homes.
The findings of the present study suggest that constant dialogue with a telenurse may help individuals who are chronically ill to develop a broader perspective and resilience through their illness trajectory. Simonÿ et al. (2019) reported that the considerable difficulty patients face when living with COPD hinder their prospects of overcoming the perceived lack of trust in their body during standard pulmonary rehabilitation. Providing breath management and physical recovery interventions on time is essential to allow people living with COPD to achieve vitality. Trust in telenursing would promote people’s well-being at each stage of illness. Therefore, telenursing is a promising solution to respond to the health care needs of individuals with chronic conditions. Despite these benefits, telenursing also has limitations due to the lack of physical contact with the client and potentially missing verbal cues from the client (Vijayalakshmi et al., 2020).
The Application of the Chronic Illness Trajectory as a Nursing Model
Human beings are facing unprecedented challenges because of the COVID-19 pandemic. Even as of April 2021, the number of COVID-19 cases and deaths worldwide has continued to increase. Although technology cannot solve every problem, a digital shift has rapidly occurred in governments, businesses, schools, hospitals, and many other social institutions because of the COVID-19 pandemic. Nursing is no exception, and the present study illustrates the promising role of telenursing in primary care settings both during this pandemic and beyond. The present study also illustrates the appropriateness of an FLMM-CS design for the theory of chronic illness trajectory.
Contribution to Mixed Methods Research
Introduction of FLMM-CS Design as an Example of Intersected/Scaffolded Design
In this article, we introduced an FLMM-CS design as an example of intersected/scaffolded design. Creswell and Plano Clark (2018) call such an intersected/scaffolded design a complex design. By intersecting (Plano Clark & Ivankova, 2016) or scaffolding (Fetters, 2020) different methodologies, researchers can expand the range of integrated mixed methods designs for tackling dynamic and complex issues in the real world.
When analyzing the data for the present study, we realized the benefits of intersecting/scaffolding a case study framework (Fetters et al., 2013; Guetterman & Fetters, 2018) with an LMMD (Plano Clark et al., 2015). This expanded and more complex mixed methods design that we used for the present study provided both a bird’s-eye view and a “worm’s-eye view” of the phenomenon under investigation. With the bird’s-eye view, we could see changes in the case over time. With the worm’s-eye view, we could observe details of how the case was proceeding within a particular time frame.
A Two-Step Process for Developing Global Meta-Inferences in an FLMM-CS Design
This article also details how we integrated QUAL and QUAN data collected continuously over time and developed global meta-inferences that encompassed the meta-inferences obtained from multiple phases. To our knowledge, this two-step process is a novel approach for drawing meta-inferences in an FLMM-CS design that no researcher has previously proposed.
The two-step approach to developing meta-inferences in an FLMM-CS design allowed us to understand what was happening to the participant during each time frame. Simultaneously, it also provided a big picture of the participant’s illness trajectory. Had we not used an FLMM-CS design, we could not have developed a comprehensive and complex understanding of the case over time.
Recommendation for Further Mixed Methods Study and Contribution to the COVID-19 Special Issue on Methodological Innovations
An FLMM-CS design allows authors and researchers to enhance their understanding of a phenomenon across different time frames and obtain an overall picture of the phenomenon’s trajectory under longitudinal investigation. In the present study, although the number of observations of QUAL and QUAN data was not equal, we believe that this is not problematic if the researcher carefully identifies a conceptual unity in the time frames to integrate QUAL and QUAN data. We believe that an FLMM-CS design is well suited for the continuous implementation and evaluation of many practices.
As countries continue to ask residents to limit their activities to indoor environments, individuals with chronic diseases are likely to feel more confined. Moreover, as other disasters such as a large earthquake, a strong typhoon, or heavy snow can affect individuals’ in-home care, public health assessments are needed to gain both a bird’s-eye view and a worm’s-eye view, to arrive at a rapid and comprehensive assessment of the situation (Ojima, 2020). This may prevent a patient with chronic illness from carrying negative feelings about the disease for a long time in their illness trajectory. Moreover, the present research method, which fully integrates QUAL and QUAN data over time and allows for a good grasp of the situation globally in two steps, is transferable. We found intersecting/scaffolding case study methodology and longitudinal methodology through the fully LMMD to be a compelling approach for clinical studies that follow dynamic changes in physical and psychological states within individuals over time.
Limitations
The present study’s strength lies in its unique approach to developing global meta-inferences by integrating all meta-inferences drawn from each observational period. This approach is innovative in the field of mixed methods. The use of theory in the current study was particularly helpful. However, the study also has limitations.
The procedures for developing global meta-inferences may vary depending on each study’s distinct nature. This is because each study has a unique way of dividing time based on its meaning and significance in relation to the study’s purpose, which may limit the generalizability of the findings. However, this issue may be irrelevant since our aim was to gain an in-depth understanding of the case. Furthermore, the replicability of the present FLMM-CS findings may also be a problem since determining the boundary of each stage relies on the researcher’s interpretation of the longitudinal data.
When analyzing interview data, the participants’ cultural values as well as thinking and rhetorical styles also need to be considered (Hatta et al., 2020; Schrauf, 2016). For example, the strong desire to avoid being a burden on the family, as observed in Mr. Ando’s case, is a value commonly shared by many Japanese patients (Elwyn et al., 2002; Kakai, 2002; Long & Long, 1982). Providing detailed cultural discussion may help the reader understand the context; however, due to the page limit, we could not do so here. Finally, the quality of available clinical interview data, particularly QUAL data, may be influenced by the participants’ ability and/or the willingness to articulate their thoughts and feelings.
Conclusion
This study illustrates an FLMM-CS design to explore an individual’s physical and psychological changes by collecting daily data on physical state measures and clinical interviews over time. This was done via video consultations before and during the COVID-19 pandemic through home-monitoring-based telenursing. The study also explored how technology-based telenursing helped the individual in his illness trajectory during the pandemic. We developed a joint display to draw global meta-inferences from five different time points in a longitudinal study. This two-step process began with the initial integration of daily physical and psychological telenursing data and the participant’s perception of illness. Subsequently, global meta-inferences were drawn from the continuous integration of QUAN and QUAL data in an FLMM-CS design. This design has the advantage of elucidating the individual’s dynamic illness trajectory during the COVID-19 pandemic.
Footnotes
Acknowledgements
The authors sincerely thank the participant of this study.
Author Contributions
All the authors contributed equally to this study. T.K. developed the study concept. N.N. introduced the case, and T.K., A.K., and N.N. collected data. T.K., A.K., and H.K. analyzed the data, and H.K. supervised the methodological procedures. T.K., A.K., and H.K. drafted the manuscript. All the authors read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the JSPS KAKENHI of Japan, Grant-in-Aid for Scientific Research (A);(Grant number 19H01082) and Scientific Research (B);(Grant number 16H05598).