
Abstract
Introduction
The radial forearm flap (RFF) is based on the radial artery and concomitant veins together with superficial veins of the forearm (Figure 1). In its free or pediculate, fasciocutaneous, pure fascial, including bone, muscle, nerve, or tendon forms, it is commonly applied for coverage of cutaneous defects by both hand surgeons and plastic surgeons.9,15 The technique was first described in 1981 by Yang et al 18 as a microsurgical free flap and, in 1982, by Lu et al 10 who published the first experience as a reverse-flow pediculated flap. Both publications were originally in the Chinese literature, giving rise to its pseudonym of the “Chinese flap.”

Art depicting RFF in dissection.
The main features of RFF are low thickness, absence of hair, good elasticity and flexibility, as well as long, thick and reliable pedicle, being applicable for many different reconstructions for coverage defects of the hand, in its pediculated form, and also for a number of other areas of the body in its free form. 7 However, despite excellent results in terms of coverage of defects, there are a number of major drawbacks discussed in the literature. These drawbacks include donor site morbidity, such as local intolerance to the cold, changes in sensitivity, aesthetic issues, claudification of the upper limb, as well as both motor and temperature changes.1,2,4,5,11,12,16,17
A widely discussed subject, albeit with few associated studies and publications, centers on whether sacrifice of the radial artery to perform the RFF is deleterious to the patient.3,8,14
The objective of this study was to assess, by questionnaire, the complications at the RFF donor site reported, particularly those related to sacrifice of the radial artery.
Materials and Methods
During the 2014 Symposium of the Brazilian Society of Reconstructive Microsurgery, the surgeons attending were asked to answer a questionnaire on RFF cases and complications, and to sign the attached Free and Informed Consent Form.
The study was performed according to the Guidelines of the World Medical Association’s Declaration of Helsinki and was approved by the Research Ethics Committees of the institution where the research was conducted.
The questionnaire comprised direct, objective, and discursive questions. The questionnaire contained fields identifying name, age and specialty (hand surgeon, plastic surgeon, or others). Subsequently, respondents were asked how many surgical procedures with RFF they had performed and the complications experienced, under 7 items with percentage options for each. In addition, an open field was provided allowing professionals to freely describe any other type of complication they had had not covered by the questionnaire. To conclude, information was collected regarding the performing of complementary exams for assessing the flaps. Where performed, data were collected on which exams were run, with results and whether they confirmed ischemia or other alterations (see the appendix).
For statistical analysis, the SPSS V17, Minitab 16, and Excel Office 2010 software applications were used. For the descriptive analysis, the parametric analysis of variance (ANOVA) test, the chi-square test for independence, the nonparametric test for equality of two proportions, and the confidence interval for the mean were applied.
The level of statistical significance was set at .05 (5%). All confidence intervals were based on 95% statistical confidence.
Results
Results were collected from 52 specialists, consisting of 37 (72.2%) hand surgeons, a statistically significant majority (P < .001), and 15 (28.8%) plastic surgeons. One study participant was excluded for incomplete questionnaire (failed to fill in the field for mean number of flaps performed).
The mean age of the surgeons was 41.1 ± 2.7 years. The total number of RFF performed was 1314, averaging 25.3 ± 12.4 per surgeon.
The results on intolerance to cold, changes in sensitivity, aesthetic complaints, fatigue or claudification, motor impairment, and change in temperature, together with the respective tests for equality of 2 proportions, are given in Table 1.
Results From the Questionnaire.
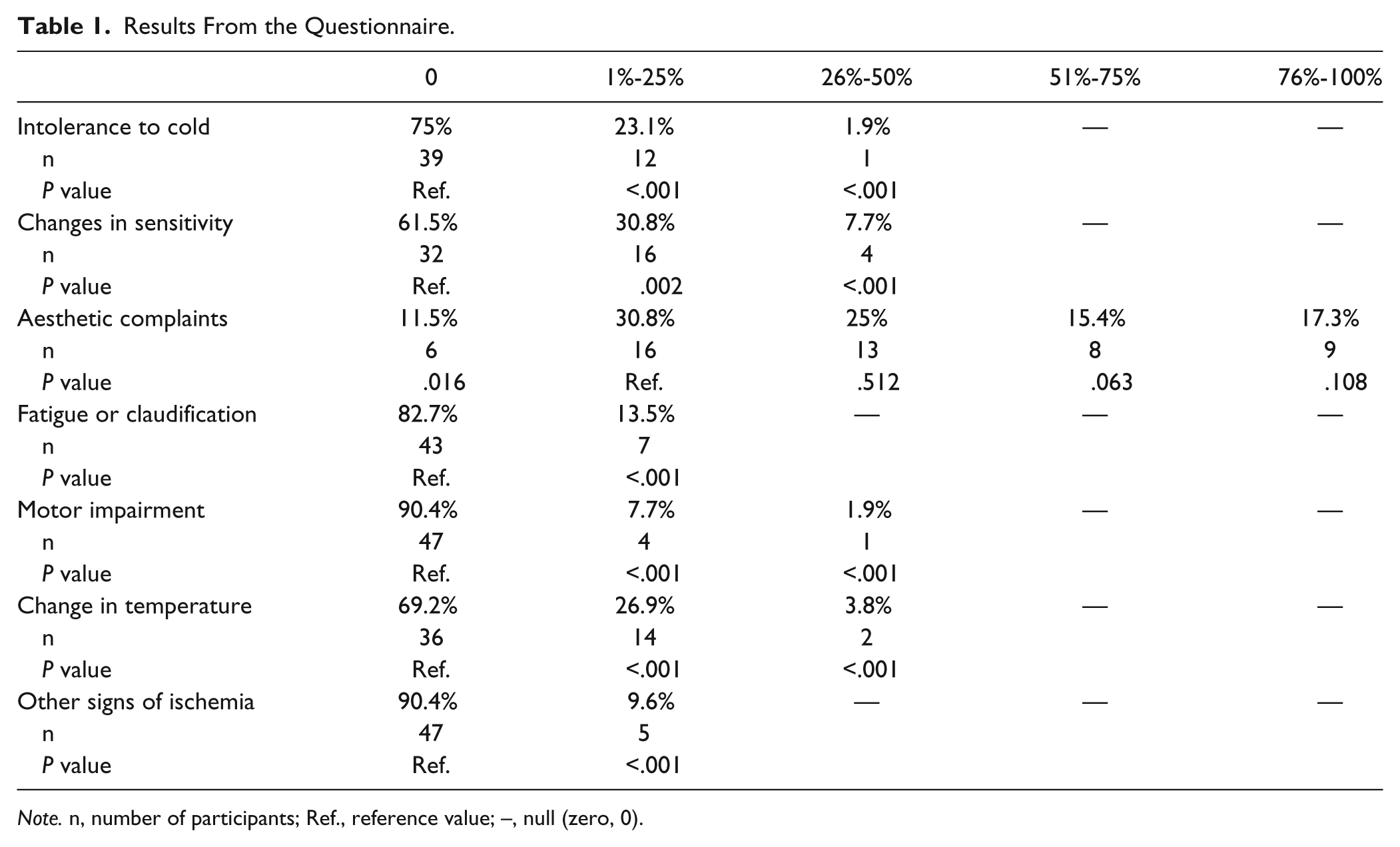
Note. n, number of participants; Ref., reference value; –, null (zero, 0).
The radial nerve was the most commonly affected, representing 70.6% of impairments, reaching statistical significance. The median (P = .006) plus ulnar (P < .001) nerves together accounted for only 29.4% (Figure 2).
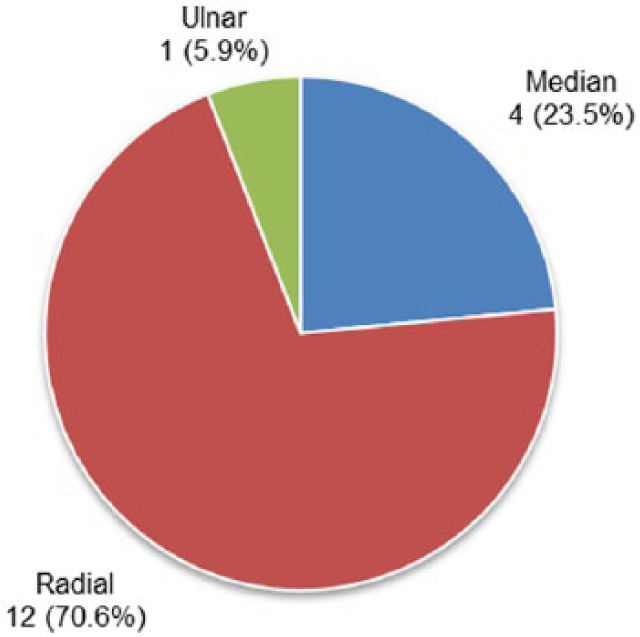
Distribution of nerve impairment.
There were 2 cases of transient venous congestion of the flap in 5 participants (9.6%) who responded positively to regarding other signs of ischemia; related complications such as mild dystrophy with reduction in local hair and nail clubbing; 1 case of epidermolysis with necrosis of the border of the flap, while 1 surgeon failed to describe the complication in question.
Of all the participants studied, 30 (57.7%) had no other postoperative complication (P = .117). Out of the 22 (42.3%) who reported other complications, there were 4 descriptions of total loss of the graft with the need for regrafting at the donor site, comprising 1 with local ulceration, 3 with dehiscence along the suture of the flap, 3 cases of flap necrosis, 3 losses of the flap, with 1 likely due to preoperative section of the palmar arch, 3 cases of partial loss of the skin graft at the donor site, 2 cases of necrosis of the border of the flap, 2 cases of infection, 1 surgeon citing 2 cases of dehiscence in the suture at the donor site, fracture of the radius (osteocutaneous RFF), pain and paresthesia of the territory of the radial sensory, and lateral cutaneous nerve of the forearm.
With regard to the opinion of respondents on the deleteriousness of sacrificing the radial artery, 39 (75%) answered negatively, that is, no deleterious effect, where response on this question was statistically significant (P < .001). Among the 13 participants (25%) who answered positively, 2 participants reported cases with intolerance to cold in lower temperature environments (winter or colder countries); 1 participant justified the positive answer commenting that “apparently not, but I do not like sacrificing a major artery of the forearm/hand”; 1 participant justified citing not the major artery but the donor site; 1 participant explained it would not be his first option owing to concerns about later complications given he would be eliminating the patient’s radial artery; 1 participant justified by temperature changes in the hand; 1 participant explained that although he had experienced few complications when performing the flap, he still considered sacrificing the radial artery and grafting the donor site a high price to pay; 1 participant answered that the literature pointed to a deleterious effect and also cited intolerance to cold; 1 participant mentioned temperature/vasomotor changes and risk of future injury to the limb; 1 participant mentioned limiting of subsequent reconstruction options, preferring the radial artery perforator flap; 1 participant wrote, “mainly owing to vascularization-related complications caused by sacrificing 1 of the forearm arteries”; and 1 participant justified saying “greater symptomatic changes in patients from countries with more temperate weather.”
None of 52 study participants performed complementary exams for detection of postoperatory ischemia and therefore did not confirm postoperative ischemia.
No statistically significant difference between the two groups (hand surgeons and plastic surgeons) was found for any of the complications (Table 2).
Relationship of Specialists With Questions From the Questionnaire.
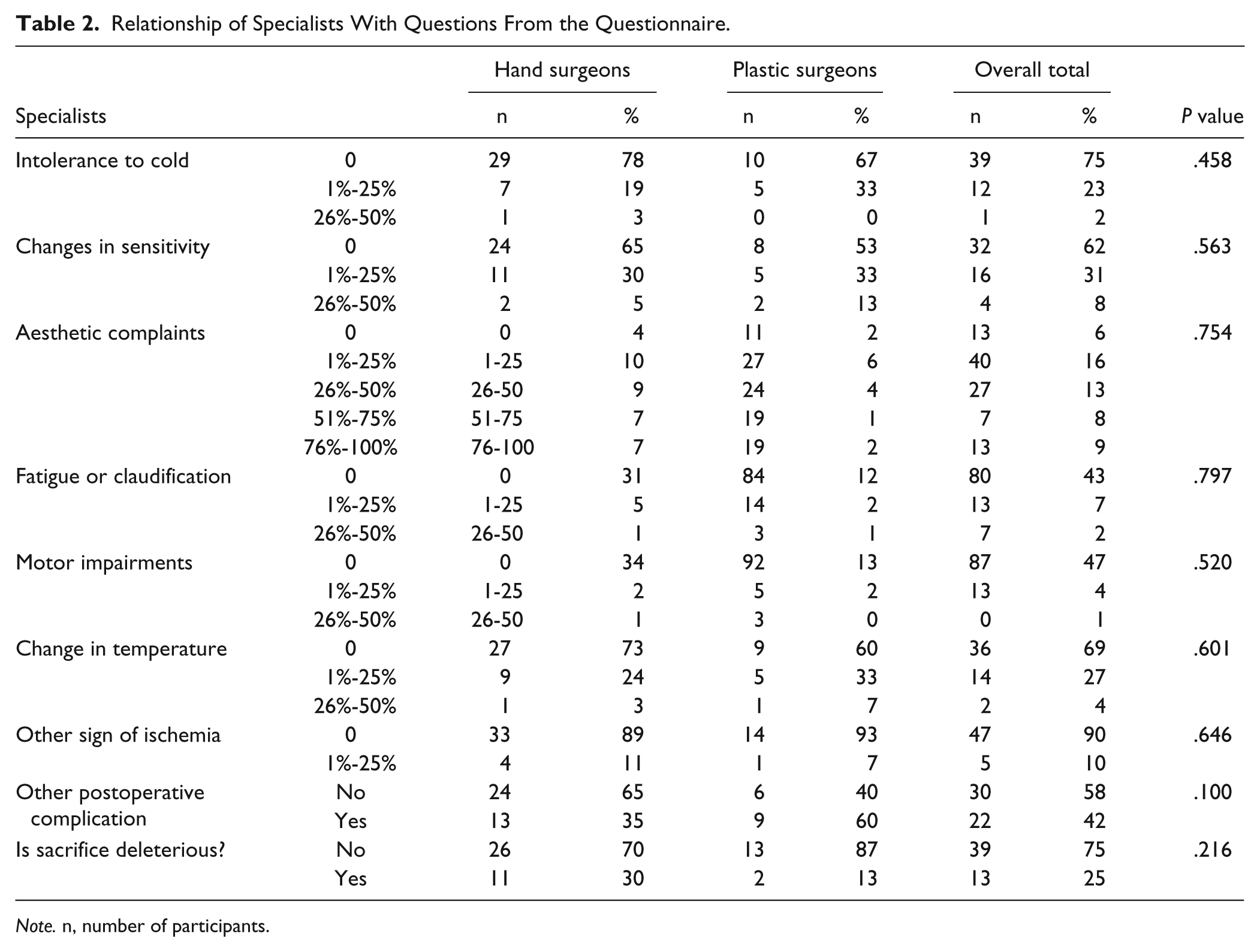
Note. n, number of participants.
No statistically significant association was found between other signs of ischemia and the remaining covariables (Table 3).
Relationship of “Other Sign of Ischemia” With Questions From the Questionnaire.
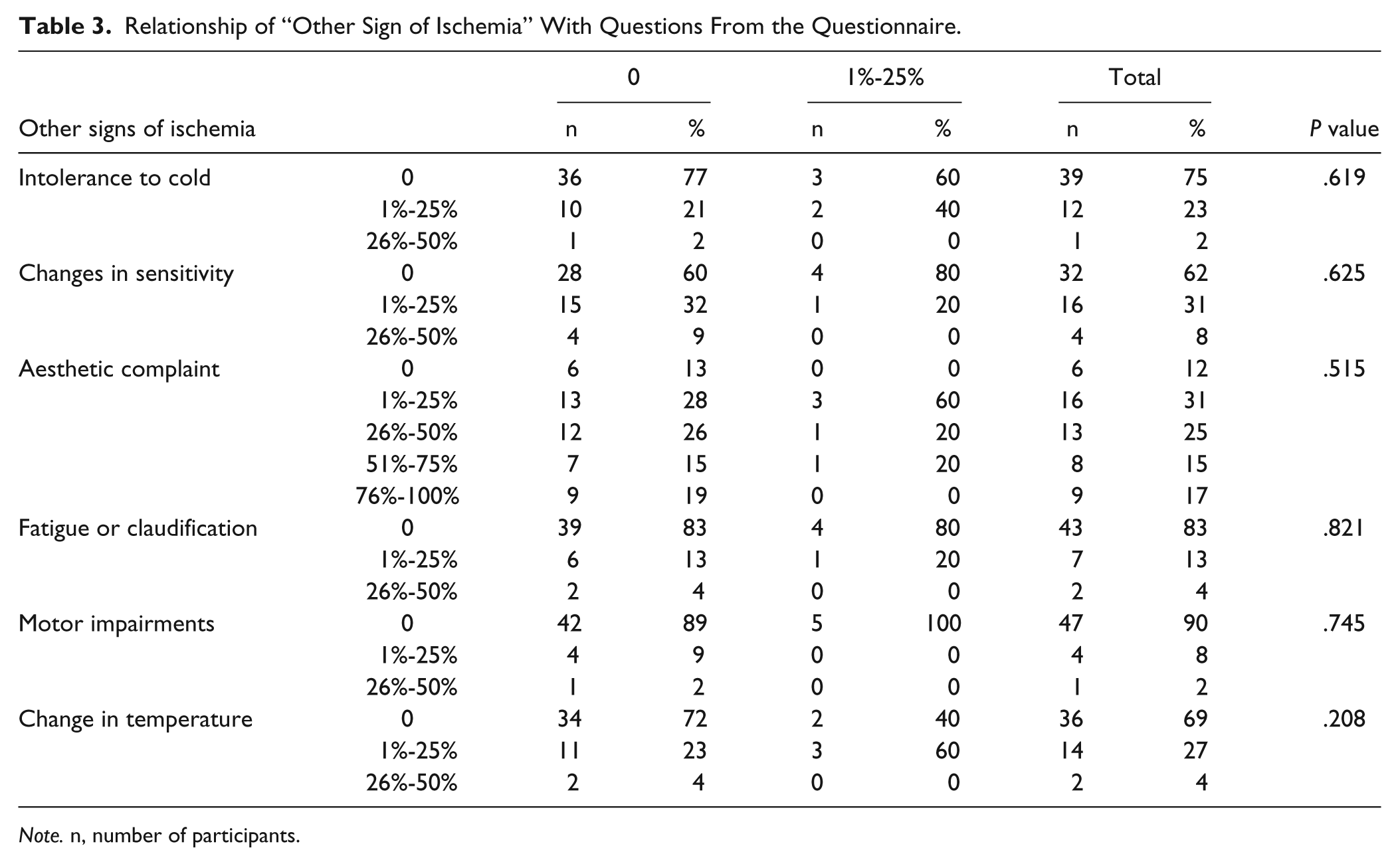
Note. n, number of participants.
The mean number of flaps in the plastic surgeons group was 41.7, proving higher than the mean of 18.6 flaps for the hand surgeons group (Table 4).
Comparison of “Number of Flaps” by Specialty.
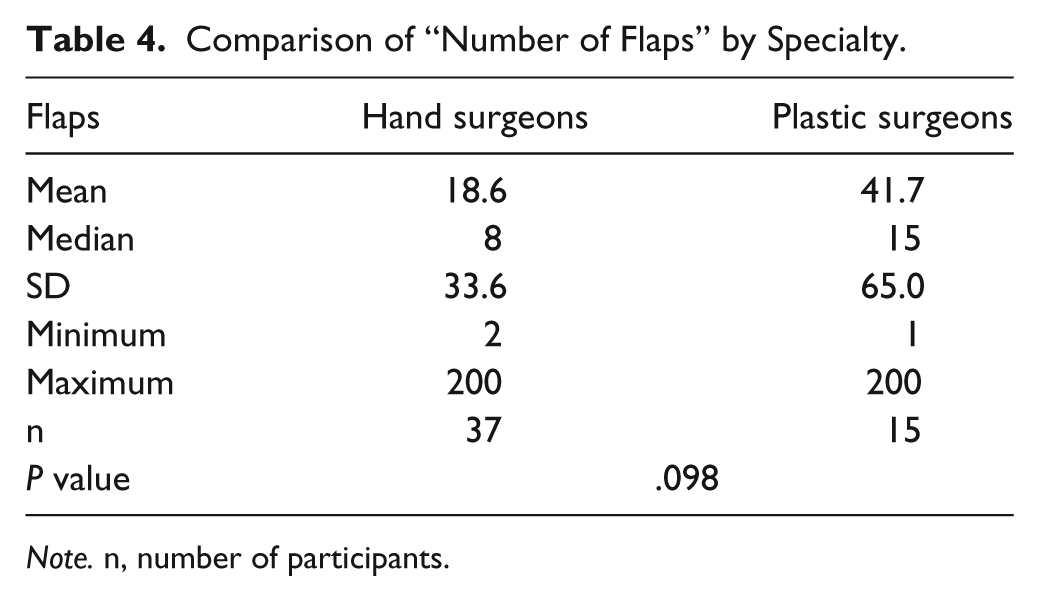
Note. n, number of participants.
Three groups were established for level of experience:
Low experience: professionals who had performed 1 to 5 flaps (15 participants);
Moderate experience: 6 to 15 flaps (20 participants); and
High experience: >15 flaps (17 participants).
No statistically significant association was found with the following variables: intolerance to cold (P = .137), changes in sensitivity (P = .360), aesthetic complaints (P = .459), fatigue or claudification (P = .707), motor impairment (P = .538), and change in temperature (P = .125), or other sign of ischemia (P = .113).
Similarly, no statistically significant difference was found among levels of experience regarding the opinion whether radial artery sacrifice was deleterious (.784).
Discussion
The versatility and effectiveness of RFF is undisputed. However, doubts exist over the deleterious effects on the patient of sacrificing the radial artery while few studies have specifically addressed this issue.3,8,14 In routine clinical practice, some professionals contraindicate RFF in some situations, wary of sacrificing the radial artery and compromising blood circulation to the hand, even though the arterial system of the limb remains intact (Figure 3).
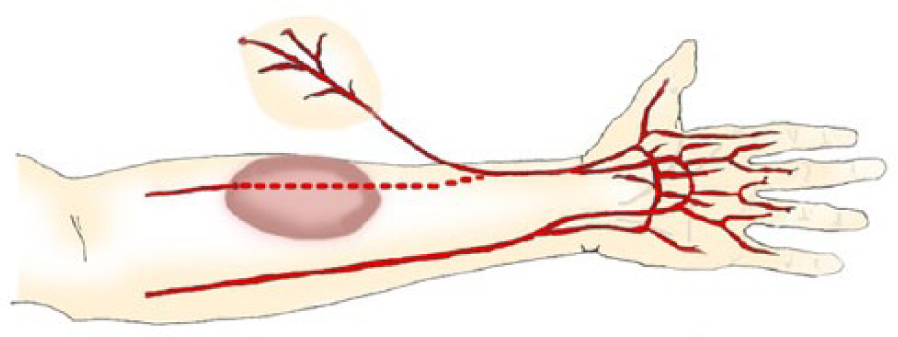
Schematic drawing of RFF depicting arterial vascular network of the forearm and hand.
These doubts are not held by reconstruction surgeons alone. Other specialists, such as heart surgeons, also use the widely adopted technique of grafting the radial artery for coronary revascularization, without causing neurological or vascular injury to the upper limb.6,8,13
Beyond performing some procedures and following evolution within a specific service, it was decided to broaden the range of opinions and enlarge the casuistic by assessing the answers of many specialists from the fields of hand surgery and plastic surgery. Data collected from these surgeons using the questionnaire were compared to determine the sequelae at the donor site and particularly whether sacrifice of the radial artery in RFF was deleterious to the patient.
The questionnaire was applied spontaneously where study participants provided approximate data. The overall number of flaps performed was considered substantial (1314), with a high average and wide variability. This can be explained by the inclusion of novice as well as experienced surgeons. Nevertheless, the finding is significant as this sample is representative of the Brazilian reality.
The complication most commonly cited by the professionals was aesthetic complaints, mentioned by 90%. Although the assessment of this variable was subjective, without the use of a suitable questionnaire for the task, this aspect should be considered when indicating RFF. All other complications occurred at low rates. On analyzing the positive responses, there was no convincing evidence that sacrifice of the radial artery was responsible for the complaints. Notably, all complications reported may have been inherent to the initial trauma process and not due to donor site morbidity per se. Some of the RFF were likely performed to provide cutaneous coverage of the severely traumatic hand, perhaps explaining some complaints such as intolerance to cold, changes in sensitivity, fatigue or claudification of the limb, motor impairment, and changes in temperature.
There is the possibility of misinterpretation of the question posed with regard to the ischemia being related only to elevation of the flap. We believe that many complaints reported pertained to the circulation of the flap as opposed to sequela at the donor site, such as transient venous congestion of the flap, partial or total necrosis of the flap, and epidermolysis. Other complaints such as loss of the skin graft at the donor site, dehiscence of the suture, and infection were also unrelated to sacrificing of the radial artery, the primary focus of the present study.
All mentions of ischemia were highly subjective and therefore the association with ischemia of the limb was not considered relevant. The opinion of the surgeons regarding the question investigated in this study was valuable. Thus, upon answering whether sacrificing the radial artery in RFF was deleterious to patients, the respondents also had the opportunity to justify the reasons for their view. The majority of the reasons given were not justifiable to the point of inferring that sacrificing the radial artery in RFF was harmful to patients, despite being grounded in the opinions given.
It is noteworthy that none of the interviewees performed complementary exams for the detection of postoperative ischemia. This further undermines and detracts from the “theory” of the much mooted dangers of sacrificing the radial artery.
Comparison of the complications reported among all the surgeons entailed subdividing the professionals to prevent number of flaps performed by surgeons from being rounded up or down during treatment of the data. The sample was therefore grouped into three levels of experience. No difference in opinion across groups was found.
Although no objective data confirming the deleterious effect of sacrificing the radial artery were found, further clinical trials or studies involving complementary exams are warranted to check whether deficits indeed occur after RFF.
The most commonly reported complication was aesthetic complaints. Although complaints at the donor site were frequently cited, no objective reports on morbidity following sacrifice of the radial artery in RFF were forthcoming.
Footnotes
Appendix
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
The study was performed according to the Guidelines of the World Medical Association’s Declaration of Helsinki and was approved by the Research Ethics Committees of the institution where the research was conducted.
Statement of Informed Consent
Informed consent was obtained when necessary.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.