
Abstract
Introduction
Approximately 18 million acute injuries occur to the upper extremities in the United States each year, accounting for 1.5% of all emergency department visits. 5 Hand fractures in particular carry a significant financial burden as they incur not only the cost of medical treatment but also that of occupational disability, particularly in patients employed in laboring occupations. 2 Open fracture variants occur in 5% of cases and can pose a unique treatment challenge. 14 Potential complications of an open fracture include infection, loss of motion, nonunion, neuropathy, contractures, osteomyelitis, amputation, and sepsis. 16
Routine administration of prophylactic antibiotics in the management of open fractures of the hand remains controversial. 7 Existing literature on open fracture infection rates and treatment guidelines have focused primarily on long bone fractures, with limited guidelines available specifically for open fractures of the hand. 16 There is also a paucity of literature examining factors such as timing to debridement and administration of antibiotics and their effect on infection rates. 13 Moreover, the optimal timing of treatment for open fractures of the hand is still unknown.
The aim of this study was to systematically review the available literature on open fractures of the hand (including phalangeal and metacarpal fractures), distal to the radius and ulna, to determine the effect of timing of debridement and antibiotic administration on infection rates.
Methods
Data Sources
A comprehensive search of the MEDLINE, EMBASE, and Cochrane computerized literature databases (from 1970 through January 2012) was performed for all studies (retrospective and prospective) that included relevant data for open fractures of the hand. The medical subject headings used were “open fracture” and “hand” or “phalanges” or “metacarpal.” Furthermore, the references of the retrieved articles (including review articles) were traced for citations missed by the electronic search.
Study Selection
Abstract titles were reviewed for relevance. If the article was deemed eligible, the abstract was retrieved and reviewed in full. Only studies in English were reviewed. Studies were included if they described (1) open fractures of the carpus, metacarpals, or phalanges; (2) a minimum of 25 subjects; (3) patients over the age of 14 years; and (4) infection outcomes. Studies were excluded if they (1) did not meet the above inclusion criteria, (2) were not performed on human subjects, (3) did not allow data from open fractures of the hand to be separated from data for open long bone fractures, and (4) did not allow outcomes from open fractures of the hand to be distinguished from closed fractures of the hand (Figure 1).
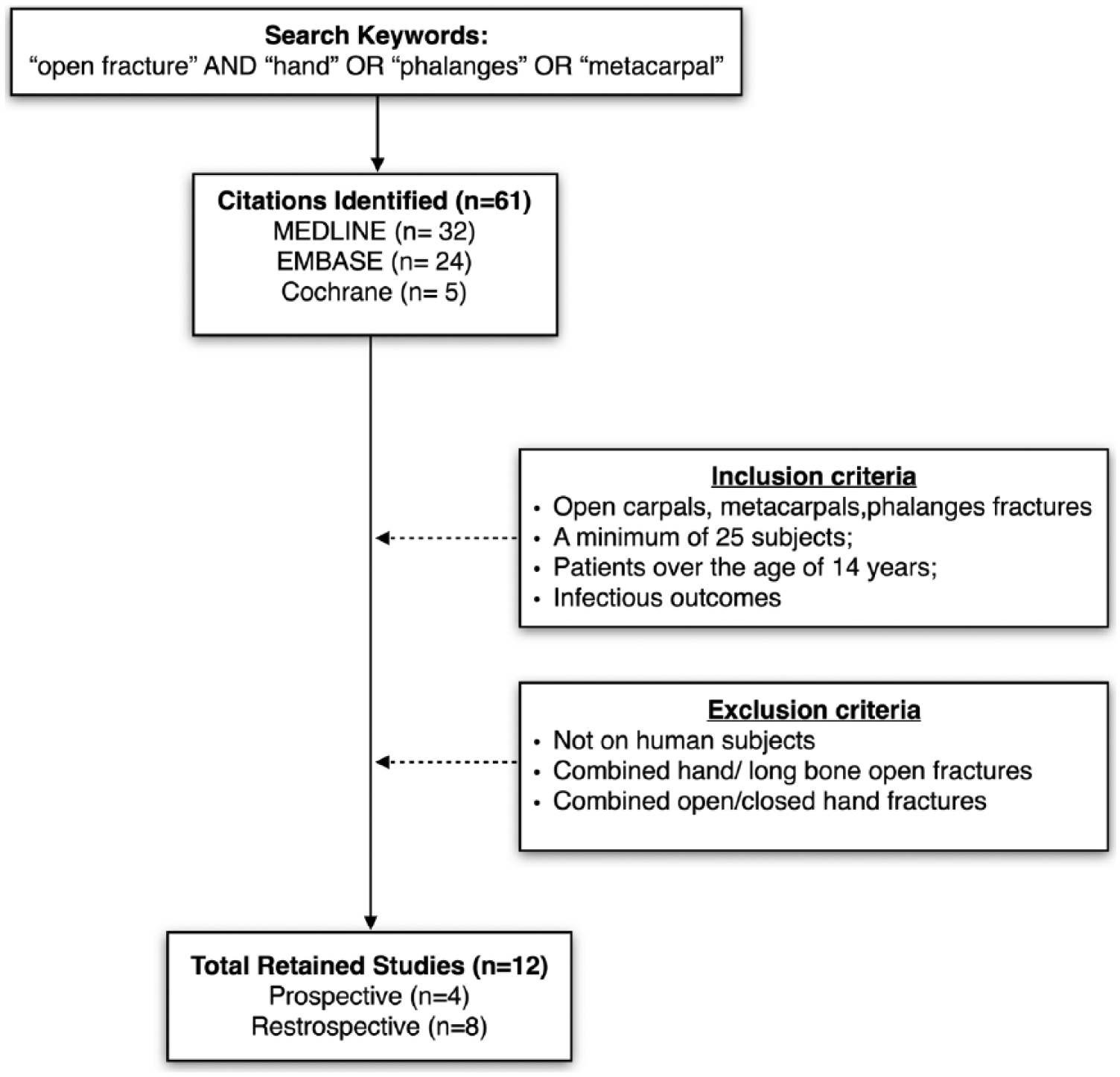
Flowchart depicting the search algorithm and the inclusion/exclusion criteria used for the systematic review.
Data Extraction
Data was extracted from each of the articles, including general information (author, year of publication, study design), period of patient enrollment, number of patients/open fractures, treatment received, antibiotic administration, timing to debridement, number and type of infections (superficial vs deep), and follow-up duration. Also recorded was the Gustilo-Anderson (GA) grade, associated injuries, and other complications.
Data Synthesis
Descriptive and quantitative data were extracted. A meta-analysis of different patient cohorts and treatment modalities was performed to compare infection rates. The overall infection rate for open fractures of the hand (regardless of treatment modalities) was calculated. Data regarding the relationship between infectious complications and administration of antibiotics was explored. Timing to debridement and its effect on infectious complications were evaluated. The odds ratio, its standard error, and 95% confidence interval were calculated.
This article adhered to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (www.prisma-statement.org).
Results
The initial search yielded 61 references. Twelve of the articles (4 prospective and 8 retrospective cohort studies) that included specific information regarding open fractures of the hand met the inclusion criteria. A total of 1669 open fractures of the hand were drawn from these studies included in the meta-analysis. There were a total of 77 infections with an overall infection rate of 4.6% (Table 1).
Studies Included in the Systematic Review That Were Used for the Meta-Analysis Along With Their Significant Finding and Relevant Notes for Each.
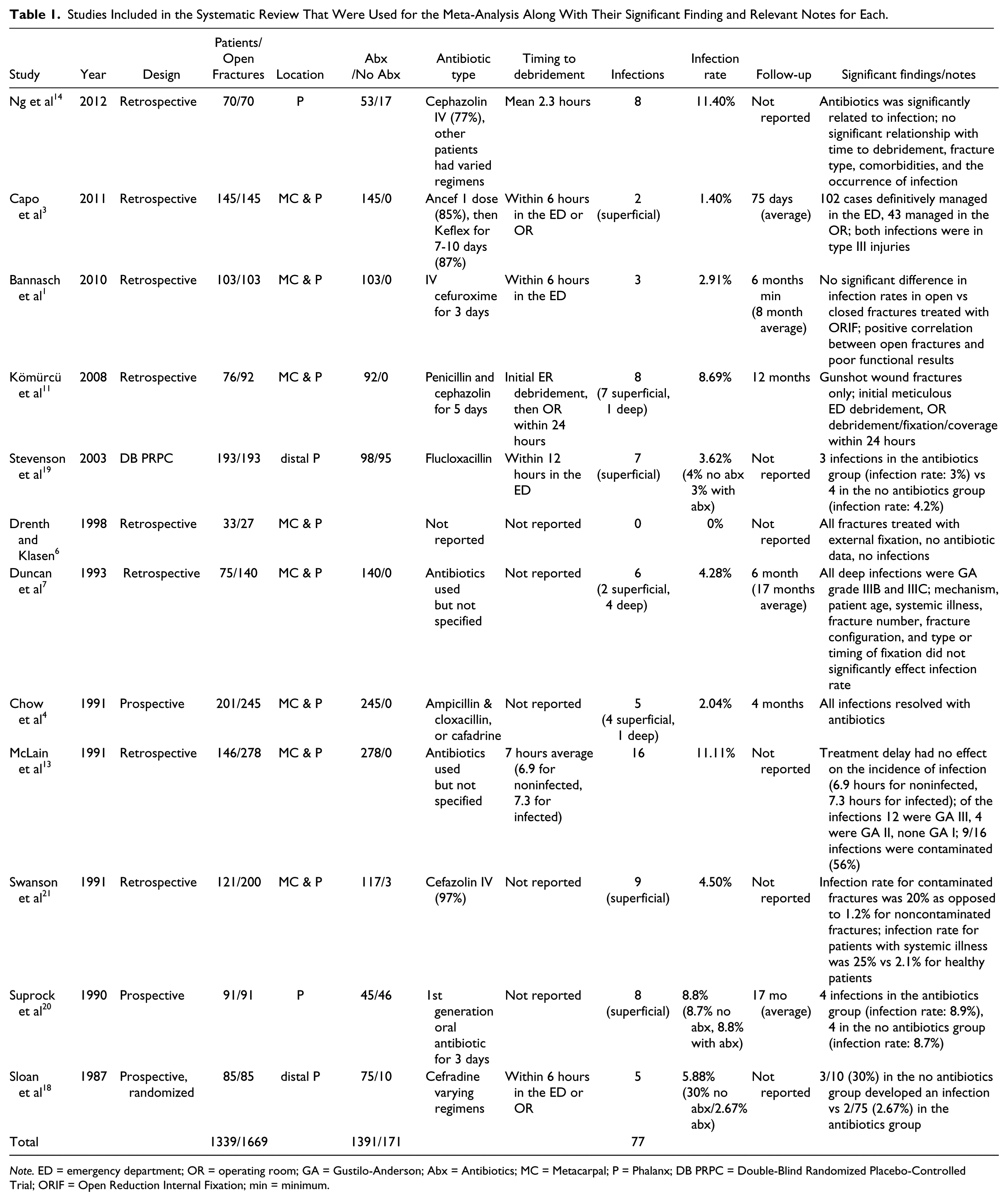
Note. ED = emergency department; OR = operating room; GA = Gustilo-Anderson; Abx = Antibiotics; MC = Metacarpal; P = Phalanx; DB PRPC = Double-Blind Randomized Placebo-Controlled Trial; ORIF = Open Reduction Internal Fixation; min = minimum.
Effect of Antibiotic Administration
Most of the studies included information regarding the administration of antibiotics for open fractures of the hand. Antibiotic type and duration varied between studies and included cafalexin, cefazolin, cefuroxime, penicillin, flucloxacillin, ampicillin, and cephradine. Duration ranged from 3 to 10 days. In 1 study 3 (145 patients/2 infections), patients received 1 dose of cefazolin followed by cafalexin for another 7 to 10 days. Two studies7,13 (221 patients/24 infections) used antibiotics but did not specify the type or duration. Four studies14,18-20 (439 patients/28 infections), randomized administration of antibiotics, and clearly defined whether the infected patients had received antibiotics or not. For each of those studies, the odd ratios for developing an infection were calculated for patients who received antibiotics over those who did not. Data from two studies reached significance defined as P < .05 with odds ratio 0.0639 (95% confidence interval [CI], 0.0091-0.4494) and 0.144 (CI, 0.0301-0.6880). The cases were then pooled together from all studies including the ones that used antibiotics for all their patients and odds ratio was recalculated to 0.4443 (CI, 0.2500-0.7897) with P = .0057 (Table 2), indicating that antibiotic use is associated with lower odds of infection.
Meta-Analysis of Infection Risk With Respect to Antibiotic Use.
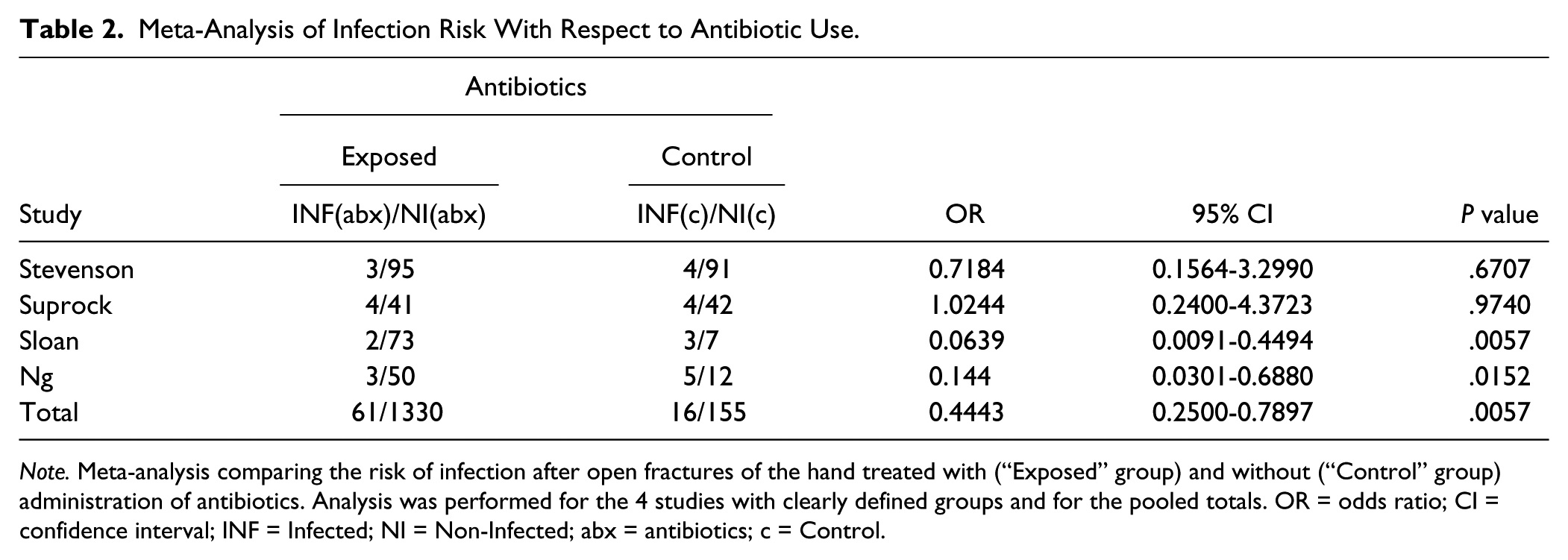
Note. Meta-analysis comparing the risk of infection after open fractures of the hand treated with (“Exposed” group) and without (“Control” group) administration of antibiotics. Analysis was performed for the 4 studies with clearly defined groups and for the pooled totals. OR = odds ratio; CI = confidence interval; INF = Infected; NI = Non-Infected; abx = antibiotics; c = Control.
Of the 1391 patients who received antibiotics in the perioperative period, there were 61 total infections (4.4% infection rate). Of the 171 patients who did not receive antibiotics perioperatively, there were 16 total infections (9.4% infection rate). Seven studies (including 1106 open fractures) provided information regarding deep vs superficial infections. Superficial infections (requiring oral antibiotics only) accounted for 86%, whereas deep infections (requiring repeat surgical irrigation and debridement) accounted for 14% (Table 3). This suggests that infections detected early often can be treated nonoperatively, and close follow-up for these fractures is warranted.
Summary of Infection Rate by Condition.
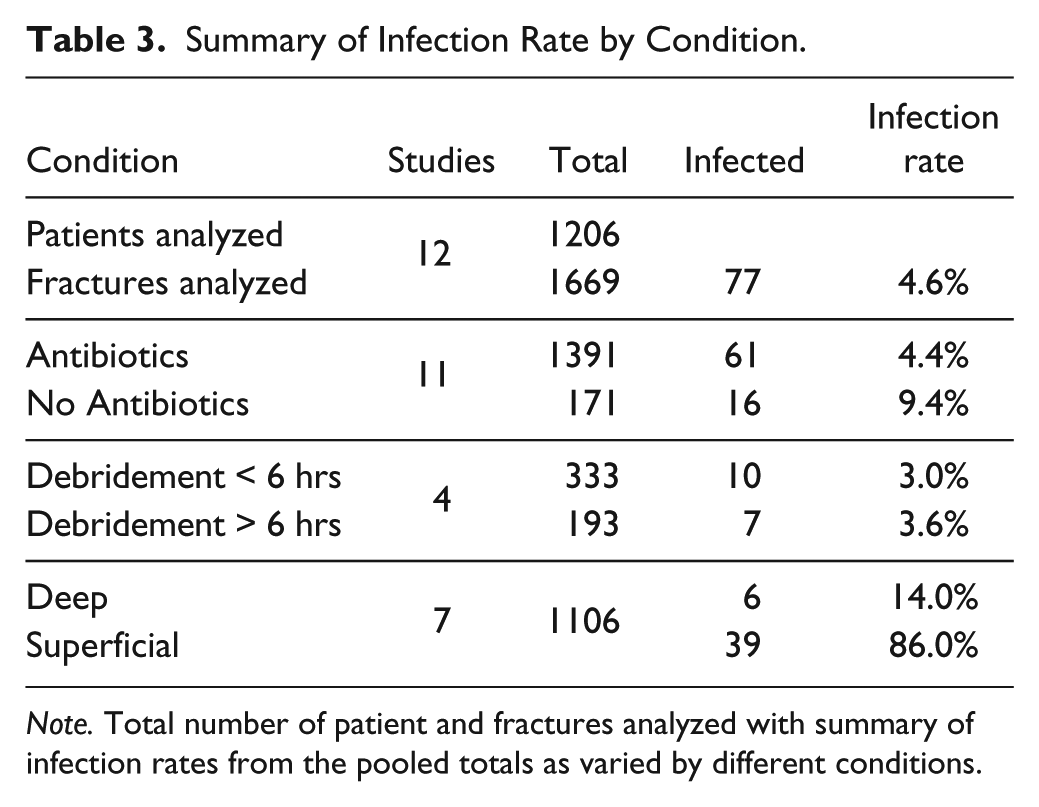
Note. Total number of patient and fractures analyzed with summary of infection rates from the pooled totals as varied by different conditions.
Effect of Early Debridement
Debridement timing and location varied between studies. Most studies reported an initial debridement in the emergency room and in a subset of those, this was followed by a formal debridement in the operating room. Two studies define the timing of debridement but do not specify whether this was performed in the emergency department or the operating room. Five studies did not include any information on timing of debridement. For the purpose of this analysis, only timing of the debridement was considered, regardless of where it was performed. Debridement within 6 hours of injury was clearly defined in 3 studies1,3,18 (including 333 fractures) with an infection rate of 3.0% (10 fractures). Debridement within 12 hours of injury (1 study with 193 fractures) resulted in a 3.6% infection rate (Table 3). Two studies looked specifically at timing to debridement, showing no correlation to the incidence of infection.13,14
Discussion
Open fractures of the hand make up 5% of all hand fractures. 14 However, there have been relatively few investigations looking into the infection rates for these types of fractures as well as the optimal treatment guidelines. Use of antibiotics is a widely accepted standard treatment in open fractures of long bones,8,15 but there is a noticeable paucity of objective studies demonstrating similar efficacy in open fractures of the hand. 20 Nonetheless, the financial burden and disability caused by infections following such injuries can be equally significant. 2
Some studies recently have questioned the necessity of antibiotic prophylaxis and open fractures of the hand.19,20 Our data however suggest that the routine use of antibiotics for open fractures of the hand results in a 4.4% infection rate as opposed to the 9.4% infection rate without antibiotic use with an odds ratio of 0.4443 (CI, 0.2500-0.7897), suggesting that antibiotic use is associated with lower odds of infection. This is in agreement with a recent study by Ng et al 14 that retrospectively reviewed 70 patients with open fractures of the hand and found that administration of intravenous antibiotics in the emergency room was the most significant factor in preventing infection. The type of antibiotics, dosing, and durations varied widely among most studies, so the optimal antibiotic regimen is still being defined. In regard to the severity of infection, 6 studies provided data on the depth of infection and the response to treatment. Superficial cellulitis accounted for 86% of the infections, and these resolved with oral antibiotics. Deep infections that required repeat irrigation and debridement accounted for the remaining 14%.
Timing to debridement has also been a long-debated issue when it comes to open fractures. The historical “six hour rule” has recently been challenged in several studies.9,10,17 Our review of the hand surgery literature found only 3 articles that clearly defined a time period comparing early vs late debridement. Debridement within 6 hours of injury was clearly defined in 2 studies (including 188 fractures) with an infection rate of 4.2%. Debridement within 12 hours of injury (1 study, 193 fractures) resulted in a 3.6% infection rate. Two studies looked specifically at timing to debridement, showing no correlation to the incidence of infection. McLain et al 13 looked specifically at treatment delay and incidence of infection. Among the 278 open hand fractures studied, treatment delay was 6.9 hours for the noninfected and 7.3 hour for the infected. Kurylo et al 12 also looked at timing to debridement in 32 patients with open distal radius including grade I, II, and III injuries, and concluded that infections in this group was not related to either the time to debridement or the initial type of fracture fixation. This is in agreement with a recent retrospective review of 296 open fractures of the radius and/or ulna performed by Zumsteg et al 22 that showed that time to antibiotics and time to operative debridement were not predictors for either rate of deep infection or nonunion in open fractures of the radius and/or ulna. In the same study however, the GA classification was strongly associated with the development of deep infection. Our pooled analysis indicates that the timing to debridement within the first 12 hours after injury does not affect the chance of developing an infection.
In regard to type of debridement, questions still remain. Many of the studies included fractures that had their initial debridement in the emergency room. Capo et al 3 looked at 145 open hand fractures, of which 102 cases were able to be definitively managed in the emergency room without an infection. Stevenson et al 19 treated all open distal phalanx fractures definitively with debridement in the emergency room and had an infection rate of 3.2%, with no infections requiring repeat surgical debridement. Subsequently, our review of the literature suggests that open fractures of the metacarpals and phalanges, without extensive contamination, can safely be treated with thorough initial debridement in the emergency room without increased risk of infection.
The degree of soft tissue injury associated with open fractures was specifically investigated in 3 studies. In regard to modified GA grade for open hand fractures, the infection rates for GA grade I and grade II fractures as opposed to GA grade III fractures were 0% vs 2.2%, 3 3.3% vs 6.3%, 7 and 6.8% vs 13.8%. 13 Based on these studies, it appears that the degree of soft tissue compromise in open fractures of the metacarpals and phalanges plays an important role in the development of subsequent complications as it has been shown for other locations such as the distal radius. Rozental et al 16 reviewed 18 patients treated at their institution for open distal radius fractures and showed that wound severity was associated with an increased number of complications (including infection), a higher number of surgical procedures, a decreased average range of motion, and fair or poor results. Taken together, this suggests that the degree of soft tissue injury and contamination does have a correlation with incidence of infection as well as other complications.
Some authors have suggested that distal phalanx fractures should be considered their own entity and should be treated differently from other open fractures of the hand entirely. Two studies included in our review included only distal phalanx fractures in their analysis. Sloan et al 18 performed a randomized prospective trial comparing patients who received no antibiotics vs 1 of 3 antibiotic regimens. They stopped the “no antibiotics” group after 3 of 10 patients became infected, and subsequently only had 2 infections for the remaining 75 patients in the “antibiotics” group. Stevenson et al 19 performed a similar randomized trial of 193 distal phalanx fractures to either receive antibiotics or receive placebo and found similar infection rates (3% with antibiotics, 4% without antibiotics). We included open distal phalanx fractures in our meta-analysis because no studies have shown a significantly lower infection rate for these fractures compared with open fractures of other bones in the hand.
There are a number of limitations to our study as it is based on a retrospective literature-based review. First, there was variability among treatment regimens. Even within individual studies, there were differences in antibiotic type and duration of administration. Furthermore, the location of the debridement (whether it was performed in the emergency room or the operating room) and timing of debridement varied significantly within, as well as between, studies. To overcome this, we categorized the time to debridement as less than 6 hours and more than 6 hours based on the “six hour rule.” Second, because the information in most studies was sparse in regard to the characteristics of their groups, we pooled all reported fractures and analyzed them together without subgroup analysis. It is possible that variation in the results can exist based on GA grade, comorbidities, age, and health status. However, our goal was to explore the overall incidence of infection in all open hand fractures and the effects of antibiotics and debridement.
Our results add to the available literature indicating that the overall infection rate for open fractures of the hand is relatively low. There is a correlation between the administration of antibiotics and infection rate and the majority of infections encountered after an open fracture of the hand can be treated successfully with antibiotics alone. The data suggest that timing of debridement in open hand fractures has not been shown to alter infection rates. Further prospective studies are needed to help establish formal guidelines in the treatment and management of open hand fractures.
Footnotes
Ethical Approval
This study was approved by our institutional review board.
Statement of Human and Animal Rights
This article does not contain any studies with human or animal subjects.
Statement of Informed Consent
This article is a systematic review of the existing literature and did not directly involve human subjects. No informed consent was necessary.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.